

Abstract
Objective
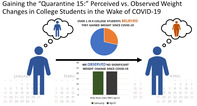
Amidst restrictions to reduce the spread of COVID‐19, jokes have surfaced regarding weight gain during the pandemic. The current study documents perceived changes since COVID‐19 and compares these to observed longitudinal changes in reported weight, BMI, and how college students described their weight from January to April 2020.
Method
Undergraduates (N = 90; 88% female) completed on‐line assessments before and after students were required to leave campus due to COVID‐19. Time 1 and Time 2 surveys collected demographic information, height, weight, and a Likert‐scale rating to describe perceived weight, ranging from 1 = very underweight to 5 = very overweight (weight description). Time 2 surveys added questions for perceived changes since COVID‐19 in body weight, eating, physical activity, various forms of screen time, and concerns about weight, shape, and eating.
Results
Time 2 surveys indicated perceived increases in body weight, eating, and screen time, and decreases in physical activity along with increased concerns about weight, shape and eating since COVID‐19. Longitudinal data indicated no significant change in weight, body mass index (BMI), or BMI category, but how participants described their weight changed significantly from January to April 2020. Compared to longitudinal changes in BMI category, students' weight description was significantly more likely to fall into a higher category from Time 1 to Time 2.
Discussion
Shifts in how body weight is experienced in the wake of COVID‐19 that do not align with observed changes in reported weight may reflect cognitive distortions that could increase risk for disordered eating in some individuals.
Keywords: body mass index, COVID‐19, eating concerns, weight concerns, weight gain
1. INTRODUCTION
COVID‐19 has severely disrupted daily life around the globe. In the United States, many universities abruptly shifted to on‐line instruction during March 2020 and required students to leave campus to reduce the risk of infection. For many students, this meant returning home to live with families and adapting to various stages of community restrictions to “flatten the curve.” A return to home, adhering to calls for social distancing, and the closing of bars, restaurants, retail stores, movie theaters, gyms, and more, dramatically altered college students' home, school, work, and social lives.
Because grocery shopping was deemed “essential” in almost all communities, food and eating remained one of the few pleasurable activities that most people could pursue along with watching television, gaming, and social media use. A combination of increased food intake and decreased physical activity could contribute to weight gain. Reflecting this, on‐line jokes and memes referred to “the Quarantine 15” (a word play on “the Freshman 15”) or to gaining “the COVID 19” to capture the zeitgeist that people gained weight in response to this pandemic (Elizabeth, 2020; Kibble, 2020). Although meant in jest, such jokes may increase pressures among those vulnerable to eating disorders to engage in disordered eating behaviors. To our knowledge, no study has examined perceived versus observed changes in body weight related to COVID‐19. Instead, articles have warned about the risks of weight gain due to COVID‐19 restrictions without data (Bhutani & Cooper, 2020; Lippi, Henry, Bovo, & Sanchis‐Gomar, 2020) or have relied on retrospective reports about weight changes perceived by participants during lockdown (Scarmozzino & Visioli, 2020; Zeigler et al., 2020). The current study measured college students' subjective experiences of how weight changed since COVID‐19 using surveys distributed in April 2020, during COVID‐19 lockdowns, and compared this to observed changes in reported weight using longitudinal assessments conducted in January 2020 (Time 1) and April 2020 (Time 2). Additional measures assessed body image at Time 1, and perceived changes in eating, physical activity, watching TV/movies, social media use, gaming and concerns about weight and shape and eating at Time 2.
2. METHODS
2.1. Participants
Participants were recruited from a southeastern public university to complete an on‐line assessment during April 15–24, 2020 (Time 2) that had been used as an on‐line screen for psychology course credit during January 8–24, 2020 (Time 1). Students experienced significant disruption in their college education between Time 1 and Time 2 assessments due to COVID‐19. In January, the university was following normal operating procedures, no cases of COVID‐19 had been identified in the state, and COVID‐19 had not yet reached the status of a pandemic. 1 On April 15, the first day Time 2 surveys were available, the university had transitioned to on‐line instruction, banned students from campus, and had no firm plans regarding on‐campus instruction for Fall 2020. Of the 797 participants who completed surveys at Time 1, 102 (13%) completed surveys at Time 2.
To maximize data quality, only participants who provided reliable reports of their height from Time 1 to Time 2 were included in analyses. This was defined as height within 1 in. between reports to allow for growth and rounding. This resulted in a final sample of N = 90 participants (n = 79 female) for analyses. No significant differences were observed for demographic, height, or weight‐related variables between those included versus excluded from analyses due to unreliable reporting or the combination of unreliable reporting and nonparticipation at follow‐up (all p‐values >.10). Racial/ethnic identity was 22% Latino, 78% White, 12% Black or African American, 4% Asian, 1% American Indian/Alaskan Native, and 3% “Other” (totals >100% because ethnicity and race were obtained through separate items). Among participants, 89% described themselves as heterosexual, and mean (SD) age was 19.45 (1.26) years at baseline and 19.71 (1.24) years at follow‐up, reflecting the 3 months between Time 1 and Time 2 surveys. Both the original assessment and the follow‐up study were approved by the university's IRB, and all participants provided informed consent prior to completing assessments at each time because the original screen was not administered in the context of a longitudinal study.
2.2. Measures
Time 1 surveys included questions from 14 labs from the Clinical, Social, Cognitive, and Neuroscience areas of the Department of Psychology to screen eligibility for studies. All items from Time 1 surveys were re‐administered in the same order at Time 2 to minimize method variance. To minimize participant burden, each lab was limited to 25 items, and the number of items per lab ranged from 1 to 22 questions, with both a mean and modal number of 13 items per lab. Additional items to assess the impact of COVID‐19 on participants' lives were added to the Time 2 measure. The survey required a mean (SD) of 35.08 (22.11) minutes at Time 1 and 38.98 (25.28) minutes at Time 2 to complete, with no significant difference in duration (t[86] = 1.14, p = .26; d = .16). Questions included single‐item assessments of specific inclusion/exclusion criteria (e.g., for fMRI research, “Do you: Have any metal in your head (other than your mouth) such as shrapnel, surgical clips, or metal plates?”) and item subsets from larger scales of psychological constructs (e.g., the first two items from the Patient Health Questionnaire‐9 assessment of depression). The left column of Supplemental Table S1 presents the constructs measured across these item subsets.
2.3. Time 1 measures of body image
Among baseline screening measures, two items from the Body subscale of the Body, Eating, and Exercise Comparison Orientation Measure (α = .91; Fitzsimmons‐Craft, Bardone‐Cone, & Harney, 2012), and four items from the Eating Disorder Diagnostic Scale focusing on weight and shape concerns (α = .85; Stice, Telch, & Rizvi, 2000) were included as Time 1 measures of body image in the current study due to their relevance and evidence of internal consistency despite their abbreviated nature. Three items from the Fear of Fat scale (Goldfarb, Dykens, & Gerrard, 1985) did not demonstrate adequate internal consistency for inclusion (α = .58).
2.4. Longitudinal variables assessed at time 1 and time 2
2.4.1. Weight and body mass index (BMI)
Both surveys included items assessing height in inches and weight in pounds, which were used to calculate BMI. Prior work supports the reliability and validity of self‐reported height and weight, with absolute errors from objectively measured values ranging from 1.00 to 3.54% in college men and women (Imrhan, Imrhan, & Hart, 1996). A meta‐analysis of longitudinal studies measuring weight change in college students found no significant difference between estimates based on self‐report versus objectively measured weight, with mean weight change differing by 0.005 kg/month (or 0.01 lb/month) (Fedewa, Das, Evans, & Dishman, 2014). In addition to examining weight and BMI as continuous variables, the Centers for Disease Control and Prevention (CDC) on‐line calculators were used to transform BMI values into the following categories: underweight, normal weight, overweight, and very overweight (Centers for Disease Control and Prevention, 2020a, 2020b). Because the CDC does not distinguish between underweight and very underweight, the DSM‐5 guideline for moderate severity for anorexia nervosa (BMI <17.5 kg/m2) defined “very underweight” (American Psychiatric Association, 2013).
2.4.2. Weight description
At both Time 1 and Time 2, participants also were asked to “Select the option that best describes your weight:” with response options of “1 = Very underweight,” “2 = Underweight,” “3 = Normal weight,” “4 = Overweight,” and “5 = Very overweight.” Prior research supports the concurrent and predictive validity of this single‐item assessment of weight description 2 as a measure of body image that demonstrates prospective associations with increased eating pathology and eating disorders (Atlantis & Ball, 2008; Brown, Forney, Klein, Grillot, & Keel, 2020; Keel & Heatherton, 2010).
2.5. Time 2 measures
Time 2 surveys added several items reflecting participants' subjective experience of changes that had occurred since COVID‐19. Participants were asked, “Since the COVID‐19 pandemic, please rate each of the following:” ranging from “1 = Much less/lower than before,” “2 = Less than before,” “3 = Somewhat less than before,” “4 = No change from before,” “5 = Somewhat more than before,” “6 = More than before,” and “7 = Much more than before.” Responses for the following items are included in the current report: “Body weight,” “Eating,” “Physical activity,” “Concerns about weight and shape,” “Concerns about eating,” “Time on social media (Instagram, Snapchat, Facebook),” and “Time on gaming.”
Because participants relocated to various parts of the state and country, we also included an item to measure COVID‐19 restrictions: “Right now, the status of COVID‐19 restrictions for my community is (choose one): 1 = No restrictions, just advice on hand washing and social distancing, 2 = Stay at home orders for those over 65 years and with existing conditions, 3 = Stay at home orders for everyone, 4 = Shelter at home orders for those over 65 years and with existing conditions, 5 = Shelter at home orders for everyone.” The majority of participants (n = 82) endorsed orders to remain home, and we recoded this variable to distinguish between these participants and the small number (n = 8) who were not restricted to their homes due to COVID‐19.
2.6. Analyses
Due to the low participation rate at follow‐up, we examined evidence of biased attrition on demographic variables, variables included in our study, and across all psychological measures included in the mass screen using χ 2, t‐tests, and a MANOVA followed by posthoc t‐tests, as appropriate. Complete results are reported in a supplemental table (see Table S1).
Examination of study variables indicated skewness between −1 and 1 and kurtosis between −2 and 2, supporting the use of parametric tests. Descriptive statistics captured perceived changes due to COVID‐19, and one sample t‐tests were used to compare whether sample means differed significantly from a null hypothesis of “no change” (a rating of 4 on this measure). These analyses permitted us to determine whether participants' subjective experiences of changes since COVID‐19 matched widely circulating concerns about weight gain. Because ratings on these items represented an ordinal versus continuous variable, we conducted a second set of nonparametric analyses to further probe these findings.
Paired t‐tests were used to examine changes observed from Time 1 to Time 2 on means for reported weight, BMI, and weight description, and correlations were used to determine associations between observed longitudinal changes (Time 2–Time 1 variables), baseline measures of body image (Time 1 variables), and subjectively perceived changes since COVID‐19 (Time 2 variables). Both BMI and weight description were analyzed as continuous variables to maintain consistency with prior analyses establishing their predictive associations with eating pathology and eating disorders (Brown et al., 2020; Keel & Heatherton, 2010). Given that weight description represented an ordinal rather than continuous variable and the ability to convert BMI into an ordinal variable using CDC guidelines, we also conducted nonparametric analyses of these variables. Additional exploratory analyses examined whether gender or COVID‐19 restrictions were associated with any variable. All analyses were conducted in SPSS Version 23 and used two‐tailed p < .05 as the threshold for statistical significance.
3. RESULTS
3.1. Attrition analyses
Completion of surveys at Time 2 was not significantly associated with gender, ethnicity, race, age, sexual orientation, height, weight, BMI, or weight description at Time 1 (all p‐values > .10; see Table S1). Thus, study variables demonstrated no evidence of biased attrition at Time 2. In addition, comparison between those who did and did not complete Time 2 surveys supported no significant differences across the range of baseline measures included in the mass screen (F(21, 590) = 1.36, p = .13, ηp 2 = .046). Posthoc analyses that did not control for family‐wise error rate indicated that 2 of the 30 baseline variables differed significantly between nonparticipants and participants. Those who completed Time 2 surveys endorsed lower concern over mistakes and lower lifetime suicidal ideation compared to nonparticipants. Effect sizes were small for all comparisons but approached a medium effect size for the difference in concern over mistakes (see Table S1).
3.2. Perceived changes following COVID‐19
Table 1 presents perceived changes since COVID‐19 in body weight, eating, physical activity, various forms of screen time, and concerns about weight/shape and eating reported at Time 2. Participants' mean scores differed significantly from a rating of “4” (no change) on all variables in parametric analyses. Differences indicated a tendency to feel they had gained weight and were eating more, less physically active, spending more time watching TV/movies, on social media, and gaming, and that they were more concerned about weight and shape and eating, since COVID‐19. Effect sizes were small for body weight and gaming, moderate for eating, and large for the remaining variables—with the largest effect size for increased time on social media. Mirroring results from parametric analyses, a Wilcoxon Signed Rank Test indicated that the median value for each response differed significantly from “4” (no change) for each question, except for time spent gaming (see Table 1).
TABLE 1.
Perceived changes since COVID‐19 based on retrospective report
| Body weight | Eating | Physical activity | Watching TV/movies | Time on social media (Instagram Snapchat Facebook) | Time on gaming | Concerns about weight and shape | Concerns about eating | |
|---|---|---|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |
| 1 = much less than before | 0 (0) | 3 (3.4) | 18 (20.5) | 1 (1.1) | 0 (0) | 5 (5.7) | 1 (1.1) | 1 (1.1) |
| 2 = less than before | 3 (3.4) | 2 (2.3) | 23 (26.1) | 0 (0) | 1 (1.1) | 3 (3.4) | 0 (0) | 1 (1.1) |
| 3 = somewhat less than before | 11 (12.5) | 15 (17.0) | 13 (14.8) | 5 (5.7) | 1 (13.3) | 1 (1.1) | 1 (1.1) | 0 (0) |
| 4 = no change from before | 49 (55.7) | 19 (21.6) | 12 (13.6) | 16 (18.2) | 12 (13.6) | 53 (58.9) | 28 (31.8) | 32 (36.8) |
| 5 = somewhat more than before | 16 (18.2) | 32 (36.4) | 15 (17.0) | 23 (26.1) | 23 (26.1) | 9 (10.2) | 33 (37.5) | 36 (41.4) |
| 6 = more than before | 6 (6.8) | 14 (15.9) | 4 (4.5) | 22 (25.0) | 33 (37.5) | 10 (11.4) | 14 (15.9) | 7 (8.0) |
| 7 = much more than before | 3 (3.4) | 3 (3.4) | 3 (3.4) | 21 (23.9) | 18 (20.5) | 7 (8.0) | 11 (12.5) | 10 (11.5) |
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | |
|---|---|---|---|---|---|---|---|---|
| 4.23 (.99) | 4.47 (1.30) | 3.08 (1.70) | 5.39 (1.29) | 5.59 (1.07) | 4.32 (1.36) | 5.02 (1.10) | 4.86 (1.09) | |
| t(87) | 2.18* | 3.39** | −5.08*** | 10.11*** | 13.94*** | 2.21* | 8.70*** | 8.10*** |
| d | 0.23 | 0.54 | −0.63 | 1.08 | 1.49 | 0.16 | 0.93 | 0.79 |
| One‐sample Wilcoxon signed rank test p‐value | .04 | .001 | <.001 | <.001 | <.001 | .07 | <.001 | <.001 |
Note: Concerns about eating df = 86.
p < .05.
p < .01.
p < .001.
In contrast to these perceptions, paired t‐tests indicated no significant change in weight reported at Time 1 (mean (SD) = 140.81 (28.92) pounds) and weight reported at Time 2 (141.17 (27.50) pounds; t(89) = .57, p = .57; d = 0.01) or BMI from Time 1 (mean (SD) = 22.93 (4.02) kg/m2) to Time 2 (22.91 (3.70) kg/m2; t(89) = −0.13, p = .89; d = −0.005). Despite no statistically or clinically significant change in reported weight or BMI, there was a significant increase in the mean value for weight description from Time 1 (3.06 [.57]) to Time 2 (3.13 (.52); t(89) = 2.15, p = .03; d = .13).
Results using nonparametric analyses paralleled findings from parametric analyses. There was no significant change across BMI categories (Related‐Samples Wilcoxon Signed Rank Test p = .26) but a significant change across weight description categories from Time 1 to Time 2 (p = .04). Figure 1 depicts stability versus change in BMI category (left) versus weight description category (right). Values above the diagonal reflect an increase from Time 1 to Time 2. Values below the diagonal represent a decrease from Time 1 to Time 2, and values on the diagonal reflect stability. A Related‐Samples McNemar Test indicated that the percentage who described their weight as falling into a higher category from Time 1 to Time 2 (10%) was significantly greater than the percentage who increased in BMI category (2%) (p = .04). Furthermore, there was no significant association between an increase in BMI category and an increase in weight description category (Fisher's Exact Test p = .19).
FIGURE 1.
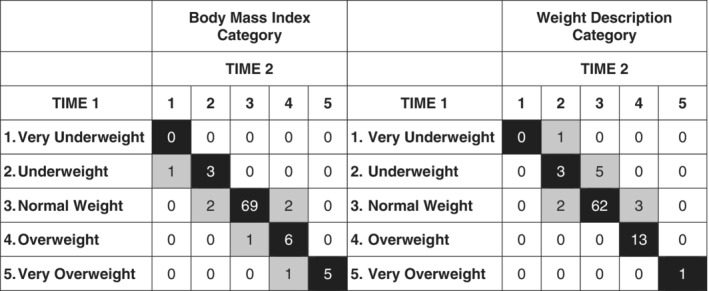
Longitudinal changes in BMI category (left) and weight description category (right) from Time 1 to Time 2. Values on the diagonal (in black) represent stability in BMI category (left) and description of weight category (right) from Time 1 to Time 2. Values above the diagonal represent an increase from a lower to a higher category from Time 1 to Time 2. Values below the diagonal represent a decrease from a higher to a lower category from Time 1 to Time 2
Table 2 presents correlations between baseline measures of body image concerns, longitudinal changes from Time 1 to Time 2, and perceived changes since COVID‐19. Baseline body image concerns were significantly associated with one another. In addition, higher weight and shape concerns at Time 1 predicted significant decreases in weight and BMI from Time 1 to Time 2 but were unassociated with change in weight description or perceived changes in body weight, eating, or physical activity since COVID‐19. Higher baseline body image concerns were significantly associated with perceived increases in weight/shape and eating concerns following COVID‐19. Higher baseline weight and shape concerns were associated with a perceived decrease in gaming. Higher baseline social comparisons on weight were associated with greater perceived increases in social media use.
TABLE 2.
Associations between baseline body image, longitudinal changes in weight, BMI, and weight description, and perceived changes since COVID‐19
| 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. T1 weight/shape concern | .69*** | −.26* | −.21* | .01 | .02 | −.12 | −.05 | .07 | .20 | −.22* | .29** | .28** |
| 2. T1 weight comparison | ‐ | −.16 | −.08 | .16 | −.04 | −.13 | .05 | −.02 | .23* | −.15 | .27* | .26* |
| 3. T2 − T1 weight | ‐ | .93*** | .14 | .23* | .07 | .19 | −.14 | .02 | −.07 | .20 | .24* | |
| 4. T2 − T1 BMI | ‐ | .12 | .24* | .03 | .21 | −.14 | −.09 | −.13 | .26* | .33** | ||
| 5. T2 − T1 weight description | ‐ | .22* | .02 | .09 | −.04 | .15 | .09 | −.10 | −.03 | |||
| 6. T2 COVID‐19 body weight | ‐ | .38*** | −.26* | .16 | .01 | −.02 | .24* | .26* | ||||
| 7. T2 COVID‐19 eating | ‐ | .04 | .22* | .03 | .05 | .19 | .12 | |||||
| 8. T2 COVID‐19 physical activity | ‐ | −.01 | −.08 | −.18 | .02 | −.14 | ||||||
| 9. T2 COVID‐19 TV/movies | ‐ | .29** | .26* | .07 | .04 | |||||||
| 10. T2 COVID‐19 social media | ‐ | .13 | .13 | .10 | ||||||||
| 11. T2 COVID‐19 gaming | ‐ | −.11 | −.16 | |||||||||
| 12. T2 COVID‐19 weight concern | ‐ | .80*** | ||||||||||
| 13. T2 COVID‐19 eating concern | ‐ |
Note: T1: Time 1, T2: Time 2, COVID‐19 identifies variables included in Table 1 regarding subjectively experienced changes since COVID‐19.
Note: *p < .05; **p < .01; p < .001.
Greater longitudinal increases in reported weight and BMI from Time 1 to Time 2 were significantly associated with one another and with perceiving greater increases in body weight and increased eating concerns since COVID‐19. A greater longitudinal increase in BMI was also significantly associated with perceived increases in weight and shape and eating concerns since COVID‐19. A greater longitudinal increase in how weight was described was significantly associated with perceiving a greater increase in body weight since COVID‐19.
Across perceived changes since COVID‐19, increased body weight was associated with increased eating, decreased physical activity, increased weight/shape and eating concerns. Increased eating was also significantly associated more time watching TV/movies. More time spent watching TV/movies was associated with more time on social media and gaming. Finally, increased weight/shape concerns were significantly associated with increased eating concerns.
We conducted exploratory analyses to determine whether study variables (see list in Table 2) differed between women and men or based on COVID‐19 restrictions. At Time 1, women endorsed significantly higher weight/shape concerns compared to men (8.59 (3.31) vs. 5.82 (1.78); t(21.31) = 4.25, p < .001; d = 1.04). At Time 2, women endorsed greater perceived increases in social media use compared to men (5.69 (.98) vs. 4.91 (1.45); t(86) = 2.32, p = .02; d = 0.63; χ 2(5) = 15.84, p = .007; Cramer's V = .42), and men endorsed greater increases in gaming compared to women following COVID‐19 (5.18 (1.54) vs. 4.19 (1.30); t(86) = 2.31, p = .02; d = 0.69; χ 2(6) = 20.09, p = .003, Cramer's V = .48). No other variables differed significantly between genders, likely reflecting the small number (n = 11) of men in the sample. Similarly, no significant differences emerged due to COVID‐19 restrictions, likely reflecting the very small number of participants (n = 8) who were not restricted to their homes.
4. DISCUSSION
The notion that people are gaining weight as a consequence of COVID‐19 was reflected in this sample's perceptions of changes in their weight since COVID‐19. Over a quarter of college students (28.4%) perceived themselves as having gained weight since the onset of the pandemic. These perceptions replicate findings from other retrospective studies of perceived weight change following COVID‐19 (Scarmozzino & Visioli, 2020; Zeigler et al., 2020). These perceptions were related to increased concerns about weight and shape and eating – which over 60% of participants described as elevated since COVID‐19. Although the perception that weight increased after COVID‐19 was related to longitudinal changes in weight and BMI from January to April of 2020, the effect sizes for these associations were small, and the mean change in reported weight was very small. Mirroring this, longitudinal changes in weight description category exceeded changes in BMI category from Time 1 to Time 2. At Time 2, 10% of students (1 in 10) described their weight using a higher category than they used at Time 1, but only 2% (1 in 50) reported increases in weight that resulted in an increase in their BMI category. Thus, COVID‐19 appears to be impacting college students' perceptions of their weight more than their weight, suggesting an increase in cognitive distortions related to risk for eating disorders (Brown et al., 2020; Keel & Heatherton, 2010).
Over the 3‐month follow‐up, mean weight increased by 0.36 lbs. across participants. A meta‐analysis of longitudinal studies examining weight change in college students reported an overall effect of 1.55 kg over 10 months, which translates into 0.34 lb/month (Fedewa et al., 2014). The smaller change observed in the current study could reflect normal variation around this mean effect. It could reflect that factors contributing to weight gain in college were eliminated when students were forced off campus. Or it could reflect biased attrition if those who gained more weight were less likely to complete assessments at Time 2. Given that we found perceived increases in body weight and concerns about weight and shape among those who demonstrated relative stability in weight over time, findings may underestimate concerns brought on by COVID‐19 among those at greater risk for weight gain.
Findings converge with well‐established data from the body image literature in which perceptions about weight are influenced by cognitive and emotional factors as well as body weight (Cash & Deagle, 1997; Haynes, Kersbergen, Sutin, Daly, & Robinson, 2018). The positive correlation between perception that weight had increased since COVID‐19 and increases in reported weight and BMI from Time 1 to Time 2 reinforces that subjectively experienced changes partially reflect reported weight. However, the effect sizes for these associations were small, indicating that other factors impacted college students' perceptions of their weight. Widespread and understandable increases in anxiety, distress, isolation, and frustration likely contribute to a tendency to view one's self more negatively (McGinty, Presskreischer, Han, & Barry, 2020). In our weight‐obsessed culture, this may translate into increased likelihood of viewing the body as being heavier during this pandemic even if body weight has not changed meaningfully. Such concerns about weight may be particularly heightened by repeated warnings that the likelihood of hospitalization and death are elevated for those whose weight falls above the threshold for obesity (Centers for Disease Control and Prevention, 2020c).
In contrast to the overall pattern of weight stability in the full sample, greater weight and shape concerns at Time 1 significantly predicted weight loss in our sample. The absence of significant associations between baseline body image concerns and subjectively experienced changes in weight, eating, or physical activity may reflect a misperception of stability among those who lost weight. These kinds of misperceptions characterize eating pathology (American Psychiatric Association, 2013). Higher Time 1 body image concerns correlated with greater perceived increases in weight/shape and eating concerns at Time 2, and greater Time 1 body comparison orientation was also associated with perceived increases in social media use. These findings suggest that COVID‐19 may have particularly deleterious effects on those at highest risk for eating disorders due to pre‐existing body image concerns.
Given uncertainty about when the COVID‐19 crisis will pass and what we will find on the other side, the pandemic's impact on mental health may be profound. In prior work (Brown et al., 2020; Keel & Heatherton, 2010), we have demonstrated the unique contribution of weight description as a prospective risk factor for increased eating disorder symptoms and eating disorder maintenance. An increase on this risk factor in 10% of the sample over such a short period of time is a concern. Now is the time to intervene to prevent worsening of eating pathology. College students may benefit from understanding that concerns about weight gain may reflect the increased importance of food in our lives more than increases in body weight. People may be more aware of what they are eating and drinking without consuming more calories given reduced access to eating at restaurants and alcohol at bars during April 2020.
Although this study focused on college students, findings may have relevance to those with eating disorders given that college students are in the age group at greatest risk for eating disorders (Hudson, Hiripi, Pope & Kessler, 2007; Udo & Grilo, 2018). In working with individuals with eating disorders, clinicians may need to focus on negative self‐appraisal and work carefully with clients to evaluate whether perceived changes in weight reflect a cognitive distortion or a reality. In cognitive‐behavioral therapy, weekly weighing represents a form of exposure therapy to reduce anxiety about the effects of normalizing eating on weight (Waller & Mountford, 2015). Now that many patients are accessing care through telehealth, clinicians may consider asking patients to weigh themselves at home “once a week, no more and no less” to counteract possible distortions that trigger restricted food intake, unhealthy exercise, and purging. These weighings may be particularly valuable to identify weight loss among patients who experience their weight as stable. To manage risk that weekly prescribed weighings could transform into compulsive checking, family members may be enlisted to help limit access to a bathroom scale by keeping it in a bedroom closet.
This study had strengths and weaknesses that may impact interpretation of findings. A key strength was the ability to capture longitudinal data on reported weight and weight description using consistent methods from January to April 2020. This permitted us to compare changes from Time 1 to Time 2 with subjectively experienced changes following COVID‐19. Evidence supporting the reliability and validity of self‐reported weight in prior studies of weight trajectory in college students (Fedewa et al., 2014) increases confidence in findings. Importantly, under restrictions limiting face‐to‐face human subjects research, on‐line assessment represented the only ethical and feasible approach for data collection in college students in April 2020. In addition, we sought to maximize data quality by restricting analyses to those who provided consistent reports on height, a variable that should not have changed dramatically over the three‐month follow‐up and appeared immediately before the question on weight, which appeared immediately before the question on weight description.
Despite the strength of a longitudinal design, only 13% of students who completed Time 1 assessments completed Time 2 assessments. This represents a weakness that requires further consideration when interpreting results. Several factors may have uniquely contributed to low participation. At Time 1, participants were not enrolled in a longitudinal study and made no commitment to complete follow‐up assessments. Instead, participants received course credit for completing a mass screen that prescreened for them additional studies for which they received credit. By April 15, students were entering the last 2 weeks of the semester, and many did not need the credits offered for completing Time 2 assessment. This decreased the value of the incentive at Time 2, which could contribute to low participation at Time 2. Time 2 assessments also occurred as students were finishing the semester during a pandemic using on‐line instruction, and the volume of university e‐mails to students increased dramatically. An e‐mail inviting them to complete Time 2 surveys may have been overlooked. Supporting these interpretations of missing data, analyses indicated no biased attrition for study variables and minimal evidence of biased attrition for any of the Time 1 variables. There was some indication that those who completed Time 2 surveys experienced lower concern over mistakes and less history of suicidality at Time 1 compared to nonparticipants, suggesting the possibility that participation was related to higher functioning. These differences may reflect chance findings given the large number of comparisons, the nonsignificant MANOVA, and that visual inspection of mean values across scales did not support systematic bias (e.g., participants also had nonsignificantly higher behavioral inhibition but lower social anxiety at baseline). That said, we cannot rule out the possibility that outcome data at follow‐up were missing due to differences we were unable to observe at Time 2 (that is, that data were missing not at random; MNAR). Although multiple imputation and other methods correct for biased attrition when data are missing at random (MAR), we had no evidence that study variables were MAR. Under these conditions, Jakobsen, Gluud, Wetterslev, and Winkel (2017) recommend analyzing observed values and acknowledging possible bias. If follow‐up data were biased toward those with better outcomes, then evidence of increased eating disorder risk may underestimate the true effect of COVID‐19.
Although the sample size was large enough to adequately power analyses of key questions, we were underpowered to evaluate possible gender differences. Similarly, although the sample size was relatively diverse with regard to ethnicity and race, we were unable to examine how race or ethnicity might impact study variables, and findings may not generalize beyond college samples. Finally, we were limited to evaluating questions that had been asked at Time 1. Based on data available in this sample, risk factors for eating disorders may be on the rise in college students, and efforts to combat these changes are needed in the wake of COVID‐19.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.
Supporting information
Table S1 Missing data analyses.
ACKNOWLEDGMENT
This work was supported by a Collaborative Collision Grant from the Florida State University Council on Research and Creativity.
Keel PK, Gomez MM, Harris L, Kennedy GA, Ribeiro J, Joiner TE. Gaining “The Quarantine 15:” Perceived versus observed weight changes in college students in the wake of COVID‐19. Int J Eat Disord. 2020;53:1801–1808. 10.1002/eat.23375
Action Editor: Ruth Weissman
Funding information Collaborative Collision Grant from the Florida State University Council on Research and Creativity
Endnotes
The first cases in Florida were confirmed on March 1, 2020 (Cutway, 2020). The World Health Organization identified COVID‐19 as a pandemic on March 11, and on this same day, the university announced that all classes would move to on‐line instruction for 2 weeks after spring break. However, on March 17, during spring break, the university announced that remote instruction would continue to the end of the semester, that students who had left campus during spring break would not be permitted to return to collect their belongings, and that on‐campus graduation ceremonies would not be held.
In our prior articles, we have named this variable “weight perception;” however, for the current report, we found it difficult to write clearly about changes in weight perception versus perceived changes in weight. Therefore, we are opted for “weight description” in the current manuscript.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request.
REFERENCES
- American Psychiatric Association . (2013). Diagnostic and statistical manual of mental disorders fifth edition (DSM‐5). Arlington, VA: American Psychiatric Association. [Google Scholar]
- Atlantis, E. , & Ball, K. (2008). Association between weight perception and psychological distress. International Journal of Obesity, 32, 715–721. 10.1038/sj.ijo.0803762 [DOI] [PubMed] [Google Scholar]
- Bhutani, S. , & Cooper, J. A. (2020). COVID‐19 related home confinement in adults: Weight gain risks and opportunities. Obesity. 10.1002/oby.22904 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown, T. A. , Forney, K. J. , Klein, K. M. , Grillot, C. , & Keel, P. K. (2020). A 30‐year longitudinal study of body weight, dieting, and eating pathology across women and men from late adolescence to later mid‐life. Journal of Abnormal Psychology, 129(4), 376–386. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cash, T. F. , & Deagle, E. A. (1997). The nature and extent of body‐image disturbances in anorexia nervosa and bulimia nervosa: A meta‐analysis. The International Journal of Eating Disorders, 22(2), 107–125. [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention (2020a). Adult BMI calculator. Available from https://www.cdc.gov/healthyweight/assessing/bmi/adult_bmi/english_bmi_calculator/bmi_calculator.html.
- Centers for Disease Control and Prevention (2020b). Child & Teen BMI calculator. Available from https://www.cdc.gov/healthyweight/bmi/calculator.html
- Centers for Disease Control and Prevention (2020c). Coronavirus disease 2019 (COVID‐19) people who are at higher risk for severe illness. Available from https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-at-higher-risk.html. [PubMed]
- Cutway, A. (2020). Timeline: The spread of coronavirus in Florida. Available from clickorlando.com/news/local/2020/03/20/timeline-the-spread-of-coronavirus-in-florida.
- Elizabeth, D. (2020). Can I socially distance myself from these terrible jokes about gaining weight while quarantined? They can be pretty triggering for those with eating disorders. Available from https://www.allure.com/story/covid-19-weight-gain-jokes-eating-disorders.
- Fedewa, M. V. , Das, B. M. , Evans, E. M. , & Dishman, R. K. (2014). Change in weight and adiposity in college students: A systematic review and meta‐analysis. American Journal of Preventative Medicine, 47, 641–652. 10.1016/j.amepre.2014.07.035 [DOI] [PubMed] [Google Scholar]
- Fitzsimmons‐Craft, E. E. , Bardone‐Cone, A. M. , & Harney, M. B. (2012). Development and validation of the body, eating, and exercise comparison orientation measure (BEECOM) among college women. Body Image, 9(4), 476–487. [DOI] [PubMed] [Google Scholar]
- Goldfarb, L. A. , Dykens, E. M. , & Gerrard, M. (1985). The Goldfarb fear of fat scale. Journal of Personality Assessment, 49(3), 329–332. [DOI] [PubMed] [Google Scholar]
- Haynes, A. , Kersbergen, I. , Sutin, A. , Daly, M. , & Robinson, E. (2018). A systematic review of the relationship between weight status perceptions and weight loss attempts, strategies, behaviours and outcomes. Obesity Reviews, 19(3), 347–363. 10.1111/obr.12634 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hudson, J. I., Hiripi, E., Pope, H. G., & Kessler, R. C. (2007). The Prevalence and Correlates of Eating Disorders in the National Comorbidity Survey Replication. Biological Psychiatry, 61(3), 348–358. 10.1016/j.biopsych.2006.03.040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Imrhan, S. N. , Imrhan, V. , & Hart, C. (1996). Can self‐estimates of body weight and height be used in place of measurements for college students? Ergonomics, 39(12), 1445–1453. [Google Scholar]
- Jakobsen, J. C. , Gluud, C. , Wetterslev, J. , & Winkel, P. (2017). When and how should multiple imputation be used for handling missing data in randomised clinical trials – A practical guide with flowcharts. BMC Medical Research Methodolology, 17, 162. 10.1186/s12874-017-0442-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keel, P. K. , & Heatherton, T. F. (2010). Weight suppression predicts maintenance and onset of bulimic syndromes at 10‐year follow‐up. Journal of Abnormal Psychology, 119(2), 268–275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kibble, K. (2020). The 'Quarantine 15' is something people joke about, but as a woman with an eating disorder, I'm panicking. Available from https://www.health.com/condition/infectious-diseases/coronavirus/quarantine-15.
- Lippi, G. , Henry, B. M. , Bovo, C. , & Sanchis‐Gomar, F. (2020). Health risks and potential remedies during prolonged lockdowns for coronavirus disease 2019 (COVID‐19). Diagnosis, 7, 85–90. 10.1515/dx-2020-0041 [DOI] [PubMed] [Google Scholar]
- McGinty, E. E. , Presskreischer, R. , Han, H. , & Barry, C. L. (2020). Psychological distress and loneliness reported by US adults in 2018 and April 2020. JAMA, 324, 2020. 10.1001/jama.2020.9740 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scarmozzino, F. , & Visioli, F. (2020). Covid‐19 and the subsequent lockdown modified dietary habits of almost half the population in an Italian sample. Food, 9(5), 675. 10.3390/foods9050675 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stice, E. , Telch, C. F. , & Rizvi, S. L. (2000). Development and validation of the eating disorder diagnostic scale: A brief self‐report measure of anorexia, bulimia, and binge‐eating disorder. Psychological Assessment, 12(2), 123–131. [DOI] [PubMed] [Google Scholar]
- Udo, T. , & Grilo, C. M. (2018). Prevalence and correlates of DSM‐5‐defined eating disorders in a nationally representative sample of U.S. adults. Biological Psychiatry, 84(5), 345–354. 10.1016/j.biopsych.2018.03.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Waller, G. , & Mountford, V. A. (2015). Weighing patients within cognitive‐behavioural therapy for eating disorders: How, when and why. Behaviour Research and Therapy, 70, 1–10. doi. 10.1016/j.brat.2015.04.004 [DOI] [PubMed] [Google Scholar]
- Zeigler, Z. , Forbes, B. , Lopez, B. , Pedersen, G. , Welty, J. , Deyo, A. , & Kerekes, M. (2020). Self‐quarantine and weight gain related risk factors during the COVID‐19 pandemic. Obesity Research Clinical Practice, 14, 210–216. 10.1016/j.orcp.2020.05.004 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1 Missing data analyses.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.