

Abstract
Background
Nivolumab is Food and Drug Administration approved in sorafenib-experienced, advanced hepatocellular carcinoma (HCC). Post-registration data of treatment in a real-world setting is lacking.
Patients and methods
We performed an international, multicenter observational study to confirm safety and efficacy of nivolumab in 233 patients treated outside clinical trials from eight centers in North America, Europe and Asia.
Results
Patients received nivolumab for Barcelona Clinic Liver Cancer stage C (n=191, 92.0%) and Child-Pugh (CP) A (n=158, 67.8%) or B (n=75, 32.2%) HCC as first (n=85, 36.5%) or second to fourth systemic therapy line (n=148, 63.5%). Objective response rate (ORR) was 22.4% and disease control rate was 52.1%. Median overall survival (OS) was 12.2 months (95% CI 8.4 to 16.0) and median progression-free survival was 10.1 months (95% CI 6.1 to 14.2). Treatment-related adverse events of grade >2 occurred in 26 patients (11.2%). Efficacy and safety were similar across CP classes and therapy line. OS was shorter in CP-B than A (7.3 months vs 16.3 months, p<0.001) and in post-first line use (10.4 months vs 16.3 months, p=0.05). Achievement of an objective response predicted for improved OS (25.4 months vs 13.2 months, p<0.001).
Conclusions
This study confirms safety and efficacy of nivolumab in advanced HCC across various lines of therapy and degrees of liver dysfunction. Despite equal ORR and toxicity to nivolumab, patients with CP-B functional class have shorter survival than the patients with CP-A.
Keywords: liver neoplasms; programmed cell death 1 receptor; immunotherapy; antibodies, neoplasm
Background
Hepatocellular carcinoma (HCC) is a malignancy characterized by high lethality and limited treatment options.1 Curative approaches, such as liver resection, ablation, or transplantation, can only be offered to patients diagnosed with early-stage disease.2 3 The majority of cases are diagnosed with intermediate or advanced Barcelona Clinic Liver Cancer (BCLC) HCC, for which loco-regional and systemic therapies are standard of care and treatment intent is palliative.4–6 The provision of systemic treatment has traditionally been complicated by the intrinsic chemoresistance of HCC7 and the presence of concomitant liver dysfunction,8 factors that have contributed to late-stage attrition in drug development. Current options for patients not suitable for transplantation, resection, or loco-regional therapies include the multitargeted tyrosine kinase inhibitors (TKIs) sorafenib and lenvatinib,9 10 both approved as frontline therapy for advanced HCC, followed by second-line options such as regorafenib, cabozantinib,11 12 and ramucirumab.13 Despite the rapid expansion of treatment options, achievement of long-term survivorship in patients with advanced HCC is limited by the occurrence of therapeutic resistance.14
The significant role of innate and adaptive immunity in influencing the pathogenesis and progression of HCC has made it an appealing target for antibody therapy against immune coinhibitory signals in the tumor microenvironment.15–17 Monoclonal antibodies against programmed cell death protein 1 (PD-1) or its ligand 1 (PD-L1) have recently become standard of care for a widening range of malignancies, including non-small cell lung cancer, melanoma, urothelial, renal cell cancers and many others.18 Therapeutic blockade of PD-1 or PD-L1 enhances the effector function of tumor-specific CD8 T-cells to drive tumor rejection.19 In HCC, the expression of PD-1/PD-L1 is associated with increased risk of recurrence and shortened survival rates,20 21 suggesting a rationale for inhibition.15
Evidence to support nivolumab use in HCC stems from CheckMate-040,22 a single-arm, open-label phase I/II study that has provided evidence of safety and antitumor efficacy in advanced disease. Although statistical significance was not achieved for the primary endpoint of overall survival (OS) in CheckMate-459, the follow-on phase III study of nivolumab versus sorafenib as first-line treatment in advanced HCC,23 nivolumab appears to benefit a proportion of patients, especially in the context of a radiological response—particularly if complete remission is achieved. In absence of predictive biomarkers of benefit to PD-1 monotherapy, the demonstration of radiological evidence of antitumor efficacy in approximately 20% of patients with unselected HCC, together with a favorable safety profile, led nivolumab to be the first PD-1 inhibitor to receive conditional approval by the US Food and Drug Administration (FDA) in 2017 for the treatment of patients with unresectable HCC and Child-Pugh (CP) A class after prior TKI exposure.
Post-registration studies to confirm safety and efficacy of nivolumab therapy in advanced HCC are lacking. “Real world” studies represent an invaluable source of confirmation to level I evidence and are increasingly recommended by regulatory authorities to ensure novel therapies are demonstrated to be deliverable in routine practice, outside stringent criteria dictated by trial protocols. Obtaining a reliable portrait of the prescribing strategies and clinical outcomes surrounding nivolumab therapy is a point of greater consequence given the competing indication for molecularly targeted therapies with regorafenib, cabozantinib, and ramucirumab in previously treated advanced HCC,24 where dual inhibition of PD-1 and cytotoxic T cell antigen-4 (CTLA-4) with ipilimumab and nivolumab has recently been approved as second-line immunotherapeutic option.25 In addition, the failure to demonstrate a significant survival benefit for PD-1-targeted monotherapy as a first and second-line systemic therapy options,23 26 jointly with demonstration of synergistic efficacy by combination of atezolizumab and bevacizumab in patients with treatment-naïve unresectable HCC27 urges clinicians and researchers to rethink the therapeutic landscape of HCC in routine practice.
To address the current gap in knowledge, we conducted a retrospective multicenter study to document safety and efficacy of nivolumab monotherapy in a large, international cohort of patients treated outside clinical studies, with the attempt of establishing basic information on patient outcomes and prognostic outlook that can be used as a point of reference for future clinical studies.
Methods
Study design and participants
We performed a multicenter retrospective study in patients with advanced HCC to evaluate the safety and efficacy of nivolumab monotherapy prescribed outside clinical studies. Patients receiving immunotherapy were recruited from eight tertiary referral centers for the care of HCC in the USA (n=226), Asia (n=47), and Europe (n=68) between 2017 and 2019. Eligible patients were at least 18 years old, had HCC confirmed histologically or radiologically according to the European Association for the Study of the Liver/European Organisation for Research and Treatment of Cancer guidelines,4 and were considered suitable for nivolumab as their disease was not amenable to curative or loco-regional therapy.
Treatment administration and outcome measures
Nivolumab was administered intravenously at the dose of 3 mg/kg of body weight every 2 weeks. Dose modifications were made based on toxicity in accordance to the summary of product characteristics (SPC) for nivolumab. Treatment was continued until disease progression or unacceptable toxicity occurred. Patient’s demographics and clinical data were collected retrospectively and prospectively curated and updated at each participating center.
Patients were followed up for survival and safety at every cycle. Evaluation of response followed the Response Evaluation Criteria in Solid Tumours (RECIST) criteria (version 1.1) on CT or MRI, as part of periodic restaging on a 9–12 weekly basis. The National Cancer Institute Common Terminology Criteria for Adverse Events version 5.0 were used to grade side effects at every contact with the patient and based on comprehensive review of medical notes, laboratory or imaging results, or records of hospitalization. Attribution of causality to nivolumab was based on the assessment of the treating physician and validated by the designated principal investigator at each site based on the nivolumab SPC.
Duration of treatment was defined as time from the date of the first dose of nivolumab to the date of the last dose. We defined OS as the time from the date of the first dose of nivolumab to the date of death. We defined progression-free survival (PFS) as the time from the date of the first dose of nivolumab to the date of death or the date of radiological evidence of tumor progression.
Statistical analysis
Demographic data were summarized using descriptive statistics. Nominal data were compared using Fisher’s exact test or χ2 test as appropriate. OS and PFS curves were calculated using the Kaplan-Meier method, and these were compared with the log-rank test. OS and PFS were compared with regards to clinically relevant variables: alpha-fetoprotein (AFP) >400 IU/mL status, BCLC staging (A-B vs C-D), presence of cirrhosis (defined as clinical/radiological diagnosis), CP class, Eastern Cooperative Oncology Group (ECOG) performance status (0 vs 1–3), etiology of chronic liver disease, extrahepatic spread (EHS), line of therapy (first line (1L) versus >1L), portal vein thrombosis (PVT) and use of corticosteroids during immunotherapy. Candidate predictors of OS and PFS were analyzed by univariate and multivariate Cox regression analysis (backward regression model) with a threshold for backward elimination of p>0.10 at each step. The influence of each factor on OS/PFS was presented as HR with corresponding p values.
All statistical analyzes were performed using SPSS V.25.0 (IBM) with all estimates being reported with 95% CIs and a two-tailed level of significance of p≤0.05.
Results
Patient disposition
Our initial study population was composed up of 341 patients, of which 108 were excluded in order to focus on patients receiving nivolumab monotherapy (figure 1). The final cohort consisted of 233 eligible patients (184 men, 79.0%) of median age 64.0 (IQR 56–69) (table 1). Treatment was administered for a mean duration of 4.0 months (IQR 1.9–9.0), with a median duration of follow-up of 8.0 months (IQR 3.8–15.0). Median interval between initial diagnosis of HCC and nivolumab initiation was 14 months (IQR 4.0–38.0).
Figure 1.
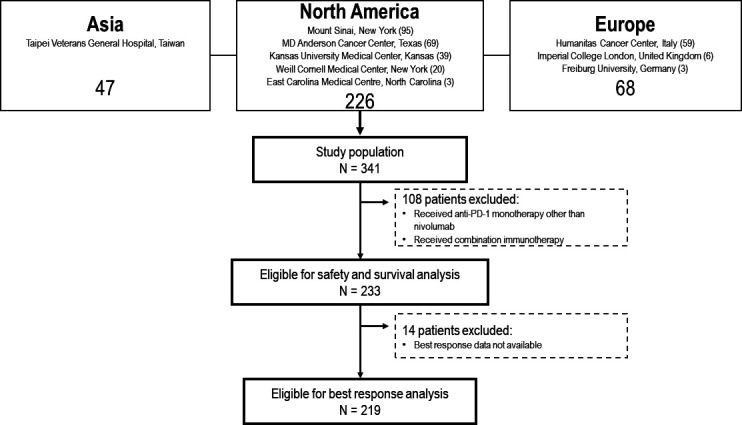
Flow chart illustrating patient disposition.
Table 1.
Baseline characteristics of hepatocellular carcinoma patients treated with nivolumab
| Baseline characteristic | N (%) |
| Total | 233 (100) |
| Age in years, median (IQR) | 64 (56–69) |
| Gender | |
| Male | 184 (79.0) |
| Female | 49 (21.0) |
| Cirrhosis | |
| Present | 176 (75.5) |
| Absent | 57 (24.5) |
| Etiology of chronic liver disease | |
| HCV | 95 (40.8) |
| HBV | 83 (35.6) |
| Alcohol | 29 (12.4) |
| NASH | 24 (10.3) |
| Other | 10 (4.3) |
| Child-Pugh class | |
| A | 158 (67.8) |
| B | 75 (32.2) |
| Albumin (g/L), median (IQR) | 35 (30–39) |
| Bilirubin (mmol/L), median (IQR) | 15 (10–24) |
| ALT (IU/L), median (IQR) | 47 (30–78) |
| ALP (IU/L), median (IQR) | 147.5 (93.3–228.8) |
| Platelet count, median (IQR) (n=139) | 142 (96.5–212.5) |
| Barcelona clinic liver cancer stage | |
| A | 4 (1.7) |
| B | 23 (9.9) |
| C | 204 (87.8) |
| D | 2 (0.6) |
| ECOG performance status | |
| 0 | 44 (28.0) |
| 1 | 99 (63.1) |
| 2 | 11 (7.0) |
| 3 | 2 (1.3) |
| Portal vein thrombosis | |
| Present | 59 (37.6) |
| Absent | 98 (62.4) |
| Extrahepatic spread | |
| Present | 66 (42.0) |
| Absent | 91 (58.0) |
| Prior therapy | |
| Surgery | 65 (27.9) |
| RFA | 41 (17.6) |
| TACE | 109 (46.8) |
| TARE | 66 (28.3) |
| EBRT | 23 (9.9) |
| Systemic therapy line | |
| 1 | 85 (36.5) |
| 2 | 130 (55.8) |
| 3 | 15 (6.4) |
| 4 | 3 (1.3) |
| Alfa-fetoprotein | |
| >400 IU/mL | 132 (56.7) |
| <400 IU/mL | 93 (39.9) |
| Maximum diameter of largest lesion (cm), median (IQR) (n=137) | 5.5 (2.8–8.9) |
ALP, alkaline phosphatase; ALT, alanine transaminase; EBRT, external beam radiotherapy; ECOG, Eastern Cooperative Oncology Group; HBV, hepatitis B virus; HCV, hepatitis C virus; NASH, non-alcoholic steatohepatitis; RFA, radio-frequency ablation; TACE, trans-arterial chemoembolization; TARE, trans-arterial radioembolization.
Most patients (n=204, 87.8%) were of stage BCLC C, with 4 classified as stage A (1.7%), 23 as stage B (9.9%), and only 2 as D (0.6%) due to performance status (PS) of 3. Severity of liver disease was CP class A in 158 patients (67.8%) and class B in the remaining 75 (32.2%). ECOG PS was available for 157 of our patients, with the majority having a score of 0 (n=44, 28.0%) or 1 (n=99, 63.1%). Median duration of treatment was not significantly different between CP-A and CP-B (p=0.08) or BCLC stage (p=0.51).
HCC was associated with radiologically/clinically documented cirrhosis in 176 patients (75.5%). The underlying etiologies of liver disease in order of descending frequency were hepatitis C (95/233, 40.8%), hepatitis B infection (83/233, 35.6%), alcoholic liver disease (29/233, 12.4%), and non-alcoholic fatty liver disease (24/233, 10.3%), with 10 patients (4.3%) suffering from liver disease secondary to other causes, such as hemochromatosis and Wilson’s disease. PVT was documented in 59 patients (37.6%) and EHS in 66 out of 157 patients (42.0%). Additional information on the biochemical and radiological profile of our cohort is provided in table 1.
With regards to prior anticancer therapy, 65 patients (27.9%) had relapsed following surgery, 109 (46.8%) had progressed after trans-arterial chemoembolization, 66 (28.3%) post-Yttrium-90 radioembolization, 41 (17.6%) had prior radiofrequency ablation, whereas 23 (9.9%) had received external beam radiotherapy. No patients received prior liver transplantation. Nivolumab was the first-line systemic therapy for 85 patients (36.5%), while it was second line for 130 (55.8%), third line for 15 (6.4%), and fourth line for 3 (1.3%). Among patients pretreated with systemic therapy (n=148), 142 had received sorafenib (95.9%). Within the cohort of patients for which post-immune-checkpoint inhibitor (ICI) treatment information was available (n=140), there was no difference in the proportion of patients who received active anticancer treatment post-ICI among those who received nivolumab as 1 L (9/27, 33.3%) as opposed to later lines (33/113, 29.2%) (p=0.67). There were no statistically significant differences between patients receiving nivolumab as 1 L or >1 L in terms of CP class, BCLC grade, PVT, EHS, and AFP >400 IU/mL (online supplementary table 2).
jitc-2020-001033supp001.pdf (99.3KB, pdf)
Efficacy of nivolumab
In total, 219 patients were evaluable for radiological response to treatment by RECIST 1.1 criteria (94.0%). Best response to nivolumab included complete response (CR) in 18 patients (8.2%), partial response (PR) in 31 (14.2%), and stable disease (SD) in 65 (29.7%). Primary disease progression (PD) was observed in 104 patients (47.9%). The objective response rate (ORR) was 22.4% and the disease control rate (DCR) was 52.1%. The treatment duration for patients who achieved different best responses were significantly different, with those who achieved a CR being treated for a mean duration of 15.6 months (95% CI 12.0 to 19.3), compared to 11.6 months (95% CI 9.2 to 14.1), for PR, 7.8 months for SD (95% CI 6.6 to 9.3), and 3.0 months for PD (95% CI 2.4 to 3.6, p<0.001). There was no significant difference in the proportion of best responses observed when the cohort was analyzed by BCLC stage (p=0.22), cirrhosis status (p=0.17), CP class (p=0.26, figure 2A), ECOG PS (p=0.51), EHS (p=0.29), line of treatment (p=0.49, figure 2B), and PVT (p=0.77).
Figure 2.

The relationship between best radiological response to nivolumab and liver functional reserve by Child-Pugh class (CP, A) and line of therapy (B). CR, complete response; PD, primary disease; PR, partial response; SD, stable disease.
The median OS in our cohort was 12.2 months (95% CI 8.4 to 16.0) (figure 3A). The 6-month and 1-year OS rates were 57.5% and 32.6%, respectively. Median OS was 30.6 months (95% CI 26.5 to 34.7) for patients who achieved CR, 18.7 months (95% CI 13.7 to 23.7) for PR, 16.3 months (95% CI 12.8 to 19.7) for SD, and 6.0 months (95% CI 4.0 to 8.0) for PD (figure 3B).
Figure 3.

Kaplan-Meier curves describing the overall survival of the whole patient cohort (A) stratified by best radiological response (B) and Child-Pugh (CP) class (C). (D) Patients’ progression-free survival stratified by best radiological response (E). CR, complete response; PD, primary disease; PR, partial response; SD, stable disease.
Univariate predictors (table 2) of OS included CP class (CP-B/A 7.3 months/16.3 months, HR=1.95, 95% CI 1.35 to 2.81, p<0.001, figure 3C), objective response as per RECIST criteria (CR+PR/SD+PD, 25.4 months/13.2 months, HR=0.26, 95% CI 0.18 to 0.39, p<0.001), ECOG PS (0/1–3, 15.3 months/8.5 months, HR=0.47, 95% CI 0.22 to 0.99, p=0.05), line of therapy (1 L/>1 L 16.3 months/10.4 months, HR=0.68, 95% CI 0.47 to 1.00, p=0.05), and PVT (present/absent 10.4 months/13.8 months, HR=1.82, 95% CI 1.13 to 2.94, p=0.02).
Table 2.
Univariate and multivariate analysis of overall survival in patients with hepatocellular carcinoma treated with nivolumab
| Variable | Univariable HR (95% CI) |
P value | Multivariable HR (95% CI) |
P value |
| Baseline AFP, >400/<400 ng/mL |
1.38 (0.96 to 2.00) | 0.09 | ||
| BCLC stage, C+D/A+B |
1.51 (0.94 to 2.44) | 0.09 | ||
| Child-Pugh, B/A |
1.95 (1.35 to 2.81) | <0.001* | 2.30 (1.40 to 3.73) | 0.001* |
| Cirrhosis, present/absent | 1.01 (0.66 to 1.54) | 0.97 | ||
| Concomitant steroid use, present/absent | 0.95 (0.65 to 1.39) | 0.95 | ||
| Objective response CR+PR/SD+PD |
0.26 (0.18 to 0.39) | <0.001* | 0.25 (0.12 to 0.54) | <0.001* |
| ECOG-PS, 0/1–3 |
0.47 (0.22 to 0.99) | 0.05* | ||
| Extrahepatic spread, present/absent | 0.92 (0.57 to 1.48) | 0.73 | ||
| Immunotherapy line, 1st/2nd–4th |
0.68 (0.47 to 1.00) | 0.05* | ||
| PVT, present/absent | 1.82 (1.13 to 2.94) | 0.02* | 1.87 (1.15 to 3.05) | 0.01* |
*marks statistical significance
AFP, alpha-fetoprotein; BCLC, Barcelona Clinic Liver Cancer; CR, complete response; ECOG, Eastern Cooperative Oncology Group; PD, primary disease; PR, partial response; PS, performance status; PVT, portal vein thrombosis; SD, stable disease.
Within CP classes, we observed no significant difference in median OS (mOS) between CP-A5 (19.2 months, 95% CI 10.8 to 27.6) and CP-A6 (16.1 months, 95% CI 9.5 to 22.7) (p=0.25), or between CP-B7 (7.2 months, 95% CI 2.3 to 12.1), CP-B8 (8.2 months, 95% CI 6.3 to 10.1), and CP-B9 (4.1 months, 95% CI 0.5 to 7.8) (p=0.46). OS was not influenced by AFP concentration >400 IU/mL (p=0.09), BCLC stage (p=0.09) (figure 2C), cirrhosis status (p=0.97), concomitant steroid use (p=0.8) or EHS (p=0.73). Multivariable predictors of OS included CP class (HR=2.30, 95% CI 1.40 to 3.73, p=0.002), objective response (HR=0.25, 95% CI 0.12 to 0.54, p<0.001), and PVT status (HR=1.87, 95% CI 1.15 to 3.05, p=0.004).
The median PFS was 10.1 months (95% CI 6.1 to 14.2) (figure 3D) and was predicted by BCLC stage (C+D/A+B 8.2 months/19.0 months, HR=2.82, 95% CI 1.46 to 5.44, p=0.002), objective response (CR+PR/SD+PD, 22.7 months/9.7 months, HR=0.26, 95% CI 0.18 to 0.39, p<0.001, figure 3E), and line of therapy (1 L/>1 L 18.2 months/8.2 months, HR=0.60, 95% CI 0.39 to 0.93, p=0.02). PFS was not influenced by presence of cirrhosis (p=0.97), AFP concentration >400 IU/mL (p=0.22), CP class (p=0.86), ECOG PS (p=0.25), concomitant steroid use (p=0.95), EHS (p=0.89), and PVT (p=0.80) (online supplementary table 1). Multivariable predictors of PFS included BCLC stage (HR=2.58, 95% CI 1.33 to 5.01, p=0.005), immunotherapy line (HR=0.60, 95% CI 0.38 to 0.93, p=0.023), and objective response (HR=0.20, 95% CI 0.11 to 0.37, p<0.001).
Safety of nivolumab
Treatment-related adverse events (trAEs) were monitored for all patients (n=233). Treatment-related toxicity of any grade was reported in 62 patients (26.6%), with 11 (4.7%) being grade 2 and 15 (6.4%) being grade 3 or above, and 30 requiring corticosteroids in the opinion of treating physicians (12.9%). The types of trAE in order of descending frequency were fatigue (46.8%, as a percentage of all trAEs), dermatological toxicity (33.9%), hepatic toxicity (27.4%), gastrointestinal toxicity (colitis/diarrhea) (16.1%), endocrine toxicity (14.6%), pulmonary toxicity (11.3%), and musculoskeletal toxicity (1.6%). Incidence of trAE of grade ≥2 was compared with regards to baseline clinico-pathological features of HCC. Incidence of grade >2 trAE was not significantly different based on presence of cirrhosis (p=0.20), and etiology of chronic liver disease (viral vs non-viral, p=0.07) (figure 4A), CP class (p=0.61) (figure 4B), BCLC stage (p=0.37), or treatment line (p=0.21). Treatment was discontinued due to unacceptable toxicity in eight patients (3.4%). Toxicity leading to discontinuation was dermatological (n=3), hepatological (n=2), endocrine (n=2), pulmonary (n=2), gastrointestinal (n=1), or rheumatological (n=1) in nature, or fatigue (n=2). Treatment-related hepatic toxicity of any grade had no relationship with prior treatment with radioembolization (p=0.17). A combination of different types of toxicity was present in 5 out of the 8 patients who discontinued treatment for this reason, and was of grade ≥2 severity in 5 out of 8.
Figure 4.

The distribution of treatment-related adverse events (trAEs) of any grade in relation to etiology of chronic liver disease (viral vs non-viral, A) and Child-Pugh (CP) class (B).
Discussion
The rising incidence and high mortality from HCC make this oncological diagnosis an area of high unmet need. Immune-based therapies targeting the PD-1 axis have shown initial evidence of oncological efficacy in HCC and a favorable therapeutic index. While it is undoubted that a fraction of patients will derive durable benefit from PD-1 inhibitors, deciphering the clinical value of PD-1 monotherapy has been challenging in clinical studies because of the lack of predictive markers and the influence of post-progression therapy on OS.23 26 In a rapidly evolving therapeutic landscape, where the atezolizumab/bevacizumab combination has demonstrated superiority to sorafenib in treatment-naïve patients27 and combination therapy with pembrolizumab and lenvatinib is showing promise,28 post-registration evidence of safety and efficacy of nivolumab in advanced HCC is needed to appreciate the clinical role of this therapeutic option outside clinical trials.
Capitalizing on an international collaborative network of investigators involved in the multidisciplinary management of HCC, we report the results of the largest real-world dataset to include patients who received nivolumab outside common clinical trial eligibility criteria including 32.2% with CP-B functional class and 44.2% outside second-line prescribing.
In our study, we reproduce the antitumor efficacy of nivolumab with ORR of 22.4% and DCR of 52.1%, estimates that are comparable to those reported in the dose expansion cohort of CheckMate-040 (ORR 20%, DCR 58%),22 as well as in a smaller retrospective study by Scheiner et al (ORR 15%, DCR 44%).29 When accounting for the heterogeneity in treatment line and liver functional reserve described in our cohort, the reported mOS of 12.2 months of our study appears consistent with that of sorafenib-experienced trial participants (13.2 months)22 and compares positively with first-line nivolumab experience in CheckMate-459 (mOS 16.4 months)23 and observational evidence (Scheiner et al, mOS 9.0).29
We have demonstrated that patients achieving a radiologically measurable tumor response are the ones with longer OS following nivolumab therapy, with greatest benefit observed in patients with a documented CR, whose median OS was in excess of 30 months. In absence of molecular predictors, achievement of radiological response following nivolumab can help clinicians to identify patients who are likely to derive long-term benefit from single-agent anti-PD-1 therapy. To our knowledge, this is the first observational study to validate such important prognostic role in patients treated with PD-1 inhibitors outside clinical trials: previous studies were underpowered to evaluate this aspect, having accrued no complete responders29 or having included patients treated with immunotherapy combinations.30
In this study, responses to nivolumab were consistent across patients’ subgroups, being independent of viral etiology, baseline BCLC stage and CP class. However, the OS of patients classifying within CP-B class was 9 months shorter than CP-A (median: 7.3 months vs 16.3 months), underscoring the prognostic impact of liver functional reserve prior to immunotherapy.
CP-B patients derive small benefit from sorafenib31 and more advanced liver dysfunction is postulated to gear the liver microenvironment towards more profound immune-suppression,32 implying reduced responsiveness to ICI. In contrast to this hypothesis, our data suggest equal probability of response to PD-1 inhibitors and acceptable safety in CP-B patients, in keeping with published evidence from smaller studies.33
While requiring prospective confirmation, our results stand as a valuable point of reference for future prospective evaluation of nivolumab in CP-B patients. Preliminary data from cohort 5 of CheckMate-040, which is currently exploring efficacy and safety of nivolumab in a restricted group of CP B7-8 patients without encephalopathy or ascites,34 reassuringly confirm our findings with a median OS of 7.6 months and a comparable ORR, DCR and proportion of trAEs.
Our study is also the first to document outcomes of a subset of patients who received nivolumab as off-label therapy for HCC beyond FDA-approved second-line use. Recommendation for nivolumab therapy in these patients followed individualized discussion within the treating multidisciplinary team and agreement of funding within respective treating institutions. The accrual of a wide proportion of patients treated with nivolumab from first to fourth line allowed us to perform a detailed analysis of its efficacy across line of therapy including first-line use, where median OS of 16.3 months overlays with CheckMate-459 data.23 Despite comparable ORR and DCR, we found that earlier provision of immunotherapy was associated with improved OS and PFS compared with later-line use. While of interest, these results are not meant to inform changes in practice, especially after the documented failure of nivolumab to improve OS in first-line advanced HCC.23 Despite equal proportion of post-progression therapy, patients receiving nivolumab as first-line systemic therapy in our study had shorter interval from original HCC diagnosis, a key factor to explain the significantly longer OS and PFS in this group compared with more heavily pretreated patients.
Perhaps unsurprisingly, we found a higher degree of heterogeneity in the assessment of PFS (median 10.1 months) which is closer to the estimate of 9.0 months published in CheckMate-04022 compared with CheckMate-459 (3.7 months)23 and the Scheiner study (4.3 months).29 Differences in PFS between observational versus interventional studies are not uncommon and attributable not only to patient heterogeneity but also to inherent differences in investigator-based versus central assessment of progression as well as in the variable frequency of re-staging that is typical of routine practice. In our study, we lack assessment of response by immune-related RECIST criteria which, unlike investigator-led adjudication of progression outcomes on the basis of RECIST version 1.1 criteria, would have facilitated identification of pseudo-progression events in our patient cohort.35
In addition to efficacy estimates, our study provides important confirmatory evidence of the safety of nivolumab in routine practice. We observed no unexpected safety signals from routine nivolumab use nor treatment-related deaths. The overall trAE rate of 26.6% and grade >3 trAE rate of 6.4% compare favorably with the proportion of grade >3 trAE observed in CheckMate-040 (19.0%),22 CheckMate-459 (22%),23 and Scheiner et al (15%).29 The rate of discontinuation due to unacceptable toxicity was also low and comparable to previous studies. Importantly, we documented no significant differences in trAE rates between CP class A and B. This is reassuring given concerns raised by a retrospective case series (n=18) that reported an all-grade trAE rate of 94% and a rate of grade ≥3 trAE of 28% in CP-B patients receiving nivolumab.33
The retrospective nature of our work stands as an important limitation of our study. However, the geographic diversity of our cohort, with patients from the USA, Europe, and Asia, significantly expands on previous studies of real-world cohorts from Germany, Austria (n=34)29 and the USA (n=18).33 The demographics of our cohort were comparable with previous studies with regards to commonly reported parameters, including age, etiology of liver disease and stage.22 23 29
Our cohort size (n=233) positively compares to that of phase II (n=214) and III (n=371) studies in this indication,22 23 with the important distinctive feature of having included patients subgroups for whom little prospective data on safety and efficacy exist (ie, CP-B or heavily pretreated patients).
Conclusion
Our study confirms that PD-1-targeted immunotherapy with nivolumab is a deliverable treatment option in a real-world patient cohort including patients with varying degrees of liver dysfunction and prior-treatment. Measures of efficacy and safety of nivolumab therapy were comparable to clinical trial data and longer survival was observed in patients achieving radiological response to treatment.
As combination immunotherapy expands across the treatment landscape of advanced HCC,27 28 the favorable response and toxicity observed in CP-B patients supports the case to investigate the use of nivolumab in this treatment-deprived patient population who is currently ineligible to molecularly targeted therapies and might be more at risk of vascular events from combination of ICI with anti-angiogenics.
Acknowledgments
The authors would like to acknowledge the infrastructure support provided by Imperial BRC Experimental Cancer Medicine Centre, Cancer Research UK Imperial Centre, and the Imperial College Healthcare NHS Trust Tissue Bank.
Footnotes
Twitter: @uqbakhan
Contributors: Study concept and design: PF, DP. Acquisition of data: AK, YW, AS, DS, TJ, SD, ARN, MM, MN, UK, CJL, AB, BY, SP, NN, DB, FB, HH, TP, YIA, NP, Y-HH, LR, CA, TM, DP. Analysis and interpretation of data: PF, DP. Drafting of the manuscript: PF, DP. Critical revision of the manuscript for important intellectual content: all the authors. Statistical analysis: PF. Obtained funding: DP. Study supervision: DP.
Funding: DJP is supported by grant funding from the Wellcome Trust Strategic Fund (PS3416).
Competing interests: DP received lecture fees from ViiV Healthcare, Bayer Healthcare and travel expenses from BMS and Bayer Healthcare; consulting fees for Mina Therapeutics, EISAI, Roche, Astra Zeneca; received research funding (to institution) from MSD, BMS. DB has received lecture and speaker fees from Bayer Healthcare and the Falk Foundation Germany. LR received lecture fees from AbbVie, Amgen, Eisai, Gilead, Incyte, Ipsen, Lilly, Roche, Sanofi; advisory board/consulting fees from Amgen, ArQule, AstraZeneca, Basilea, Bayer, Celgene, Eisai, Exelixis, Hengrui, Incyte, Ipsen, Lilly, MSD, Nerviano Medical Sciences, Roche, Sanofi; travel expenses from Ipsen; received research funding (to institution) from Agios, ARMO BioSciences, AstraZeneca, BeiGene, Eisai, Exelixis, Fibrogen, Incyte, Ipsen, Lilly, MSD, Roche. NP received lecture fees from AbbVie and Gilead; travel expenses from ArQule. YHH has received advisory board/consulting fees for BMS, MSD, Bayer Healthcare, IPSEN, EISAI, Gilead and Lilly. AS received research funding (to institution) from AstraZeneca, Exelixis, BMS and Clovis; advisory board/consulting fees from BMS, AstraZeneca, and Exelixis.
Patient consent for publication: Not required.
Ethics approval: This project received authorization for the retrospective use of patient data from the Imperial College Tissue Bank (Reference Number R16008). The study was conducted in accordance with the principles stipulated in the Declaration of Helsinki and following Good Clinical Practice standards. The date of ethical approval was March 20, 2018. Written consent was waived due to the retrospective nature of the study.
Provenance and peer review: Not commissioned; externally peer reviewed.
Data availability statement: Data are available upon reasonable request. Data (eg deidentified retrospective patient data) are available upon reasonable request.
Author note: Guarantor of the article: Dr David J. Pinato, Imperial Centre for Translational and Experimental Medicine (ICTEM), 72 Du Cane Road, White City, London W12 0NN, +44 (0)20 7594 2799, david.pinato@imperial.ac.uk.
References
- 1.Bertuccio P, Turati F, Carioli G, et al. . Global trends and predictions in hepatocellular carcinoma mortality. J Hepatol 2017;67:302–9. 10.1016/j.jhep.2017.03.011 [DOI] [PubMed] [Google Scholar]
- 2.Yegin EG, Oymaci E, Karatay E, et al. . Progress in surgical and nonsurgical approaches for hepatocellular carcinoma treatment. Hepatobiliary Pancreat Dis Int 2016;15:234–56. 10.1016/S1499-3872(16)60097-8 [DOI] [PubMed] [Google Scholar]
- 3.Mazzaferro V, Sposito C, Zhou J, et al. . Metroticket 2.0 model for analysis of competing risks of death after liver transplantation for hepatocellular carcinoma. Gastroenterology 2018;154:128–39. 10.1053/j.gastro.2017.09.025 [DOI] [PubMed] [Google Scholar]
- 4.European Association for the Study of the Liver. Electronic address: easloffice@easloffice.eu, European Association for the Study of the Liver . EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol 2018;69:182–236. 10.1016/j.jhep.2018.03.019 [DOI] [PubMed] [Google Scholar]
- 5.Vogel A, Cervantes A, Chau I, et al. . Hepatocellular carcinoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol 2018;29:iv238–55. 10.1093/annonc/mdy308 [DOI] [PubMed] [Google Scholar]
- 6.Pinter M, Peck-Radosavljevic M. Review article: systemic treatment of hepatocellular carcinoma. Aliment Pharmacol Ther 2018;48:598–609. 10.1111/apt.14913 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Lohitesh K, Chowdhury R, Mukherjee S. Resistance a major hindrance to chemotherapy in hepatocellular carcinoma: an insight. Cancer Cell Int 2018;18:44. 10.1186/s12935-018-0538-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Thomas M. Molecular targeted therapy for hepatocellular carcinoma. J Gastroenterol 2009;44(Suppl 19):136–41. 10.1007/s00535-008-2252-z [DOI] [PubMed] [Google Scholar]
- 9.Llovet JM, Ricci S, Mazzaferro V, et al. . Sorafenib in advanced hepatocellular carcinoma. N Engl J Med 2008;359:378–90. 10.1056/NEJMoa0708857 [DOI] [PubMed] [Google Scholar]
- 10.Kudo M, Finn RS, Qin S, et al. . Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet 2018;391:1163–73. 10.1016/S0140-6736(18)30207-1 [DOI] [PubMed] [Google Scholar]
- 11.Bruix J, Qin S, Merle P, et al. . Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2017;389:56–66. 10.1016/S0140-6736(16)32453-9 [DOI] [PubMed] [Google Scholar]
- 12.Abou-Alfa GK, Meyer T, Cheng A-L, et al. . Cabozantinib in patients with advanced and progressing hepatocellular carcinoma. N Engl J Med 2018;379:54–63. 10.1056/NEJMoa1717002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Zhu AX, Kang Y-K, Yen C-J, et al. . Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased α-fetoprotein concentrations (REACH-2): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol 2019;20:282–96. 10.1016/S1470-2045(18)30937-9 [DOI] [PubMed] [Google Scholar]
- 14.Guo J, Li L, Guo B, et al. . Mechanisms of resistance to chemotherapy and radiotherapy in hepatocellular carcinoma. Transl Cancer Res 2018;7:765–81. 10.21037/tcr.2018.05.20 [DOI] [Google Scholar]
- 15.Pinato DJ, Guerra N, Fessas P, et al. . Immune-based therapies for hepatocellular carcinoma. Oncogene 2020;39:3620–37. 10.1038/s41388-020-1249-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Greten TF, Wang XW, Korangy F. Current concepts of immune based treatments for patients with HCC: from basic science to novel treatment approaches. Gut 2015;64:842–8. 10.1136/gutjnl-2014-307990 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hato T, Goyal L, Greten TF, et al. . Immune checkpoint blockade in hepatocellular carcinoma: current progress and future directions. Hepatology 2014;60:1776–82. 10.1002/hep.27246 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Smyth MJ, Ngiow SF, Ribas A, et al. . Combination cancer immunotherapies tailored to the tumour microenvironment. Nat Rev Clin Oncol 2016;13:143–58. 10.1038/nrclinonc.2015.209 [DOI] [PubMed] [Google Scholar]
- 19.Ahn E, Araki K, Hashimoto M, et al. . Role of PD-1 during effector CD8 T cell differentiation. Proc Natl Acad Sci U S A 2018;115:4749–54. 10.1073/pnas.1718217115 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Gao Q, Wang X-Y, Qiu S-J, et al. . Overexpression of PD-L1 significantly associates with tumor aggressiveness and postoperative recurrence in human hepatocellular carcinoma. Clin Cancer Res 2009;15:971–9. 10.1158/1078-0432.CCR-08-1608 [DOI] [PubMed] [Google Scholar]
- 21.Shi F, Shi M, Zeng Z, et al. . PD-1 and PD-L1 upregulation promotes CD8(+) T-cell apoptosis and postoperative recurrence in hepatocellular carcinoma patients. Int J Cancer 2011;128:887–96. 10.1002/ijc.25397 [DOI] [PubMed] [Google Scholar]
- 22.El-Khoueiry AB, Sangro B, Yau T, et al. . Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): an open-label, non-comparative, phase 1/2 dose escalation and expansion trial. Lancet 2017;389:2492–502. 10.1016/S0140-6736(17)31046-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Yau T, Park JW, Finn RS, et al. . CheckMate 459: a randomized, multi-center phase III study of nivolumab (NIVO) vs sorafenib (SOR) as first-line (1L) treatment in patients (PTS) with advanced hepatocellular carcinoma (aHCC). Ann Oncol 2019;30:v874–5. 10.1093/annonc/mdz394.029 [DOI] [Google Scholar]
- 24.Kudo M. Targeted and immune therapies for hepatocellular carcinoma: predictions for 2019 and beyond. World J Gastroenterol 2019;25:789–807. 10.3748/wjg.v25.i7.789 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Yau T, Kang Y-K, Kim T-Y, et al. . Nivolumab (NIVO) + ipilimumab (IPI) combination therapy in patients (pts) with advanced hepatocellular carcinoma (aHCC): results from CheckMate 040. J Clin Oncol 2019;37:4012 10.1200/JCO.2019.37.15_suppl.4012 [DOI] [Google Scholar]
- 26.Finn RS, Ryoo B-Y, Merle P, et al. . Pembrolizumab as second-line therapy in patients with advanced hepatocellular carcinoma in KEYNOTE-240: a randomized, double-blind, phase III trial. J Clin Oncol 2020;38:193–202. 10.1200/JCO.19.01307 [DOI] [PubMed] [Google Scholar]
- 27.Finn RS, Qin S, Ikeda M, et al. . Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med 2020;382:1894–905. 10.1056/NEJMoa1915745 [DOI] [PubMed] [Google Scholar]
- 28.Llovet J, Shepard KV, Finn RS, et al. . A phase Ib trial of lenvatinib (LEN) plus pembrolizumab (PEMBRO) in unresectable hepatocellular carcinoma (uHCC): updated results. Ann Oncol 2019;30:v286–7. 10.1093/annonc/mdz247.073 [DOI] [Google Scholar]
- 29.Scheiner B, Kirstein MM, Hucke F, et al. . Programmed cell death protein-1 (PD-1)-targeted immunotherapy in advanced hepatocellular carcinoma: efficacy and safety data from an international multicentre real-world cohort. Aliment Pharmacol Ther 2019;49:1323–33. 10.1111/apt.15245 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Lee P-C, Chao Y, Chen M-H, et al. . Predictors of response and survival in immune checkpoint inhibitor-treated unresectable hepatocellular carcinoma. Cancers 2020;12:182. 10.3390/cancers12010182 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Pressiani T, Boni C, Rimassa L, et al. . Sorafenib in patients with Child-Pugh class A and B advanced hepatocellular carcinoma: a prospective feasibility analysis. Ann Oncol 2013;24:406–11. 10.1093/annonc/mds343 [DOI] [PubMed] [Google Scholar]
- 32.Albillos A, Lario M, Álvarez-Mon M. Cirrhosis-associated immune dysfunction: distinctive features and clinical relevance. J Hepatol 2014;61:1385–96. 10.1016/j.jhep.2014.08.010 [DOI] [PubMed] [Google Scholar]
- 33.Kambhampati S, Bauer KE, Bracci PM, et al. . Nivolumab in patients with advanced hepatocellular carcinoma and Child-Pugh class B cirrhosis: safety and clinical outcomes in a retrospective case series. Cancer 2019;125:3234–41. 10.1002/cncr.32206 [DOI] [PubMed] [Google Scholar]
- 34.Kudo M, Matilla A, Santoro A, et al. . Checkmate-040: nivolumab (NIVO) in patients (pts) with advanced hepatocellular carcinoma (aHCC) and Child-Pugh B (CPB) status. J Clin Oncol 2019;37:327 10.1200/JCO.2019.37.4_suppl.327 [DOI] [Google Scholar]
- 35.Seymour L, Bogaerts J, Perrone A, et al. . iRECIST: guidelines for response criteria for use in trials testing immunotherapeutics. Lancet Oncol 2017;18:e143–52. 10.1016/S1470-2045(17)30074-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
jitc-2020-001033supp001.pdf (99.3KB, pdf)