

Abstract
Context
Biomechanical analyses of cutting tasks have demonstrated kinematic differences associated with the noncontact knee-injury risk when the movement direction is unanticipated. Motor-motor dual tasks occur within dynamic environments and change the demand for attentional resources needed to complete athletic maneuvers, which may contribute to injury risk.
Objective
To investigate the influence of anticipation and motor-motor task performance on cutting biomechanics.
Design
Cross-sectional study.
Setting
Laboratory.
Patients or Other Participants
A total of 32 healthy, recreationally active men (age = 23.1 ± 3.6 years, height = 180.0 ± 7.0 cm, mass = 81.3 ± 17.3 kg) who self-reported regular participation in cutting sports.
Intervention(s)
Participants performed a 45° side-step cut on the dominant limb in a random order of conditions: anticipation (anticipated, unanticipated) and task (no ball throw, ball fake, ball throw).
Main Outcome Measure(s)
Triplanar trunk, hip, and knee angles were assessed throughout the stance phase using 3-dimensional motion capture. Data were analyzed using a time series of means calculated from initial contact to toe-off (0%–100%) with 90% confidence intervals. Mean differences between conditions were identified as regions of nonoverlapping confidence intervals, and those that occurred during the region of peak vertical ground reaction force (0%–25%) are presented.
Results
Regardless of anticipation, attending to a ball (ball throw) resulted in more trunk extension (range = 2.9°–3.7°) and less lateral trunk flexion toward the cutting direction (range = 5.2°–5.9°). Planning to attend to a ball (ball fake) resulted in less lateral trunk flexion toward the cutting direction (4.7°). During unanticipated cutting, more trunk rotation away from the cutting direction was observed when attending to a ball (range = 5.3°–7.1°). The interaction of anticipation and task had a similar influence on sagittal- and frontal-plane trunk position.
Conclusions
Motor-motor task performance and its interaction with anticipation induced an upright, neutral trunk position during side-step cutting, which has been associated with the risk for noncontact knee injury. Promoting task complexity during rehabilitation and injury-prevention programs may better prepare individuals to succeed when performing high-risk athletic maneuvers.
Keywords: attentional resources, dual task, kinematics, lower extremity, trunk
Key Points
Motor-motor task performance and its interaction with anticipation promoted a more upright, neutral trunk position during side-step cutting, which has been associated with the risk for noncontact knee injury.
By promoting task complexity during end-stage rehabilitation and injury-prevention programs, physically active individuals may become better prepared to succeed when performing high-risk athletic maneuvers.
The ability to safely perform repeated cutting maneuvers is critical to optimize level I and level II sports1 performance in which the act of pivoting is essential.2 Unfortunately, physically demanding tasks, such as side-step cutting, are believed to place individuals at greater risk for anterior cruciate ligament (ACL) injuries.3,4 More than two-thirds of ACL injuries have been reported to occur from noncontact mechanisms, and nearly one-third of noncontact injuries are related to cutting or landing mechanisms,5 highlighting that the injury risk is largely modifiable.6 Whereas ACL reconstruction is a mainstay of treatment for young, active individuals, it remains far from protective against osteoarthritis,7 emphasizing the continued need to optimize injury-prevention strategies that mitigate long-term disability. To do so, it is necessary to examine high-risk movement tasks that incorporate athletic demands, which may contribute to the injury risk.
The side-step cut has been studied as an athletic maneuver used to mimic the risk of sustaining a noncontact ACL injury in a controlled environment.3,5,8 Researchers3,4,9 using 3-dimensional motion-capture, high-speed 2-dimensional video, and subjective athlete recall of ACL injury have suggested that trunk and lower extremity kinematics are critical biomechanical factors that contribute to the risk for injury. Specifically, increased trunk lateral flexion, hip adduction, and knee abduction have been described as increasing ACL loading during cutting.3,5,10,11 To understand the mechanisms involved in the risk for ACL injury, investigators have widely reported on the biomechanical factors associated with injury during cutting tasks. However, the generalizability of such findings to athletic demands may be limited when the task is performed without distraction and in a known direction. By introducing environmental constraints commonly encountered by athletes, researchers can gain an improved understanding of movement behavior during increasingly complex tasks, which may provide further insight into injury risk.
During athletic events, change-of-direction maneuvers are often unanticipated due to a constantly varying environment. Authors12–15 have examined the influence of anticipation on cutting, single-legged drop landings, and walking mechanics in healthy individuals. More hip adduction, knee-abduction (valgus) moment, knee internal-rotation moment, and ACL strain have been observed in response to an unanticipated cut than to an anticipated cutting task.12,14,15 Furthermore, lateral trunk position has been associated with frontal-plane changes in hip kinematics during unanticipated cutting.14 Increased hip adduction has also been identified as a predictor of increased knee abduction in women during anticipated cutting,16 which may further influence the risk for injury when the direction of cutting is unknown. Whereas many researchers have investigated high-risk kinematics in women, much less information is available in men, a gap we aimed to address. Collectively, these data support the link between anticipation of athletic movement and risk for injury. However, this relationship may be further complicated in the presence of competing environmental stimuli that increase the demand for attentional resources.
The control of trunk movement is important for minimizing aberrant lower extremity joint loading during athletic tasks. Yet the appropriate control of human movement requires specific attentional resources that may be altered in the presence of attention-demanding conditions, such as dual tasking.17 Dual tasking requires the ability to split attention to coordinate the simultaneous performance of 2 tasks and may be classified as motor-motor, cognitive-cognitive, or cognitive-motor.18 In an athletic context, the ability to control movement during motor-motor tasks, such as focusing on an external event (eg, catching a ball) while cutting, is essential. Motor-motor tasks introduce an inherent layer of neuromuscular complexity, as evident in the biomechanical adaptations reported,19–22 although few researchers have examined such relationships during cutting. In a study of healthy basketball players, Fedie et al20 reported that dual-task (attending to a ball) cutting increased knee-valgus moment. Whereas fewer differences have been observed during walking gait and stair climbing, the influence of dual tasking on primary motor performance has been theorized to grow as the complexity of the task increases,21 which may have specific implications for sport performance.
It is plausible that athletes perform reactionary change-of-direction movements while focusing on environmental stimuli during athletic events. Whereas anticipation and motor-motor paradigms have been examined independently, to our knowledge, the interaction of these constructs, operationally defined as an additive effect, has not been explored relative to cutting.12–15,19–23 If anticipation and motor-motor task performance have an additive effect, the trunk and lower extremity biomechanics used during an athletic event may be much different than when measured in a laboratory setting using traditional, planned cutting-task paradigms. If this is the case, injury-prevention programs designed to alter modifiable biomechanical risk factors may need to include a combination of anticipation and dual-tasking components to better represent the constraints experienced during an athletic event. Therefore, the purpose of our study was to assess the independent and combined effects of anticipation and motor-motor task performance on trunk and lower extremity kinematics during cutting in male participants. We hypothesized that (1) motor-motor task performance would have a larger influence than anticipation but that (2) the additive effect of each would have the largest influence on cutting biomechanics. Specifically, we hypothesized that motor-motor task performance involving attending to a ball or planning to do so would promote a more neutral trunk position and induce high-risk movement patterns, such as increased hip adduction and knee abduction.
METHODS
We used a cross-sectional design to compare tri-planar trunk, hip, and knee angles during a 45° side-step cutting maneuver. Independent variables were anticipation (anticipated cut, unanticipated cut) and task (no ball throw, ball fake [planning to attend to a ball], ball throw [attending to a ball]). Anticipation and task conditions were performed in random order. Dependent variables were mean trunk, hip-joint, and knee-joint angles assessed throughout the stance phase.
Participants
A convenience sample, consisting of 32 healthy men (age = 23.1 ± 3.6 years, height = 180.0 ± 7.0 cm, mass = 81.3 ± 17.3 kg), was recruited from a university population. To be eligible, volunteers must have reported being physically active, as indicated by a minimum score of 6 on the Tegner Activity Scale, and participating in a cutting sport (eg, basketball, football, lacrosse, rugby, soccer, or ultimate Frisbee) at least 1 time per week. Volunteers were excluded if they reported any of the following: history of lower extremity surgery; lower extremity injury within 6 months of the study that resulted in continued pain or dysfunction; or any vestibular, balance, or connective tissue disorder. All participants provided written informed consent, and the study was approved by the University of Toledo Biomedical Institutional Review Board.
Procedures
All participants attended 1 testing session. Upon arrival, demographic information was recorded (ie, age, height, mass, limb dominance, physical activity per week, history of injury or illness). Limb dominance was determined by asking the participant which limb he would use to kick a ball. Subjective knee function was quantified using the Knee Injury and Osteoarthritis Outcome Score subscales to ensure that each participant self-reported a high level of knee function, in addition to not having a history of injury.24
Participant Familiarization and Setup
Before testing, a single researcher (T.R.F.) orally explained and physically demonstrated the testing procedures, which consisted of the approach, side-step cutting, and condition variables. Immediately afterward, participants completed a minimum of 3 practice cutting trials in each direction, performing trials until they were comfortable with the task. They were instructed to plant with the right foot when cutting to the left and with the left foot when cutting to the right. After familiarization, a single researcher (T.R.F.) applied thirty-eight 14-mm retroreflective markers (B&L Engineering, Santa Ana, CA) to the participant (acromioclavicular joints, sternal notch, C7 spinous process, right inferior angle of the scapula, iliac crests, posterior-superior iliac spines, sacrum, greater trochanters, lateral femoral epicondyles, lateral malleoli, calcanei, fifth metatarsal bases, and second metatarsal heads) using double-sided tape. Four marker clusters were secured bilaterally to the lateral thigh and shank using 2-in (5.08-cm) PowerFlex tape (Andover Healthcare, Salisbury, MD). All participants wore standardized shoes (model Gel-Contend 3 Running Shoe; ASICS, Irvine, CA) and tight-fitting elastic shorts for testing.
Experimental Setup and Cutting Conditions
Three-dimensional joint angles of the trunk, hip, and knee were collected using a 12-camera motion-capture system (model Eagle; Motion Analysis Corp, Santa Rosa, CA) sampling at 100 Hz and associated Cortex software (version 5.5.0). A cone was placed behind an unmarked 45.7- × 50.8-cm force platform (model OR605; Advanced Motion Technology Inc, Watertown, MA) to indicate where participants were to make the cut. Participants began the task 6.0 m from the force platform and were instructed to approach it as fast as possible and contact it with the foot before performing a side-step cut in either direction at approximately a 45° angle as previously described (Figure 1).25 A custom timing-gate program was used to record the approach speed between the first and the second and third timing gates and indicate the direction of the cut for the anticipation condition. The approach speed was restricted to between 4.0 and 5.5 m/s, which was identified as the range of the fastest speed that participants could successfully complete the task during pilot testing. It is important to note that all participants must have self-reported maximum effort during each cutting trial for the trial to be considered successful.
Figure 1.
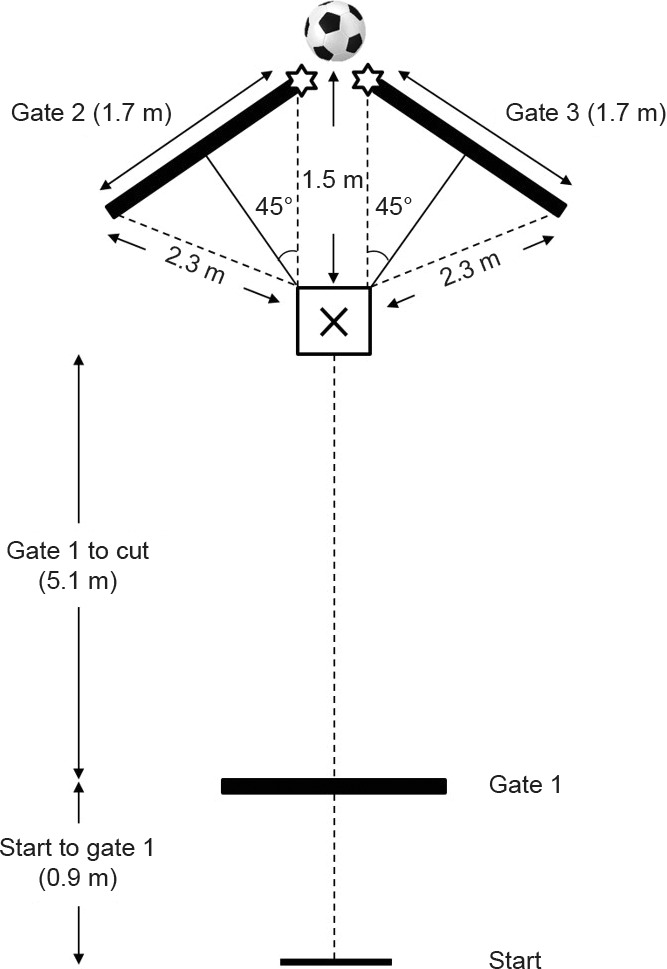
Experimental setup. Participants began at the start line, ran toward a marked region (X) as fast as possible, planted with the dominant foot, and cut in the opposite direction (side-step technique) at a 45° angle. A custom timing gate triggered a light-emitting diode (stars) to indicate the direction of cut before the trial (anticipated cut) or 300 milliseconds after gate 1 (unanticipated cut). One researcher stood beyond where the cut was made with a ball behind the back (no ball throw) or in front of the body (ball fake or ball throw).
The order of the cutting conditions was randomized via a concealed envelope by a third party before study enrollment. During the anticipated cut, a light-emitting diode was lit to indicate the direction in which the cut would be performed before the start of each trial. In contrast, a light was only triggered 300 milliseconds after the participant passed through the first timing gate during the unanticipated cut. A separate investigator (not an author) stood approximately 1.5 m beyond where the cut was made with a ball behind her back (no ball throw) or in front of her body (ball fake or ball throw). During the ball-fake condition, the investigator simply held the ball still at chest height in front of her body to give the participant a sense that the ball might be thrown. During the ball-throw condition, the investigator began in the same manner but threw the ball at chest height directly in front of the participant. The combination of anticipation and task resulted in 6 cutting conditions per limb. However, the importance, or priority, of each task condition was not specified to participants. Five successful trials were recorded and analyzed for each condition, resulting in a total of 60 trials. Participants must have demonstrated an appropriate approach speed, made full foot contact on the force platform, stayed within the appropriate cutting pathway, and performed the correct cutting task for a trial to be considered successful. Any failed trials were discarded and repeated after all planned trials. Trials in which the ball was not successfully thrown at participants' chests were discarded and repeated. To minimize the risk of fatigue, participants rested for 5 minutes after 30 trials were completed. Participants self-reported fatigue every 15 trials using a visual analog scale, indicating their level of fatigue by marking an X on a 10-cm line, ranging from no fatigue (far left) to worst fatigue (far right). After 5 successful trials of each cutting condition were completed, the participant was dismissed.
Data Reduction
All participants self-identified as right-limb dominant. In a recent systematic review, Dos'Santos et al26 reported inconclusive findings to support an influence of limb dominance on ACL injury risk based on lower extremity biomechanics. Therefore, only data recorded during the 30 trials in which participants cut to the left using the dominant right limb were included in the final analysis. Kinematic data were processed using Visual 3D software (version 6; C-Motion, Inc, Germantown, MD) and filtered using a fourth-order, low-pass Butterworth filter with a cutoff frequency of 12 Hz.27 Trunk, hip-joint, and knee-joint angles were calculated in all 3 cardinal planes during the stance phase of the cutting task, which was defined as the point at which the vertical ground reaction force exceeded 20 N (initial contact) or decreased below 20 N (toe-off). Hip-joint angles and knee-joint angles were defined as the distal segment relative to the proximal segment. Trunk angles were defined as the trunk segment relative to the laboratory coordinate system (sagittal and frontal planes) and as the trunk segment relative to the pelvis (transverse plane) to avoid the potential for misclassifying trunk rotation due to whole-body rotation.9
Statistical Analysis
The data from the 5 successful trials were first averaged for each participant and subsequently averaged for all participants. This produced means and standard deviations for each of the 101 data points across the stance phase of the cutting task. Next, 90% confidence intervals (CIs) were calculated using the mean and standard deviation of each data point, as previously described.28 The means and 90% CIs were plotted as a time series across the stance phase from initial contact to toe-off (0%–100%). This allowed us to evaluate each kinematic variable among conditions (6 total conditions). Regions in which the CIs did not overlap for more than 3 consecutive data points were considered different. Using Excel (version 2016; Microsoft Corp, Redmond, WA), we calculated mean differences and Cohen d effect sizes with 95% CIs to determine the magnitude of observed differences only within the regions previously identified as different between conditions. The 95% CIs around the mean differences between conditions were reported given the wide ranges of nonoverlapping CIs from the time-series analyses. As a secondary analysis, joint angles were compared between conditions within the first 25% of the stance phase to investigate the region of greatest loading as indicated by the vertical ground reaction force. In vivo and computational-modeling techniques have been used to demonstrate the occurrence of peak ACL force within the first 50 milliseconds of initial contact during impact activities.15,29,30 Therefore, we believed this region would adequately encompass the region of peak loading and reflect a higher risk for injury, highlighting the clinical implications of any observed differences. The approach speed, percentage of failed trials (excluding those due to investigator error), and self-reported fatigue were compared among conditions using separate 2-way analyses of variance with Bonferroni post hoc comparisons when appropriate. The level of significance was set a priori at P ≤ .05. The approach speed, percentage of failed trials, and self-reported fatigue were compared among conditions using SPSS (version 20.0; IBM Corp, Armonk, NY).
We estimated our required sample size based on a previous investigation22 of lower extremity biomechanics measured in response to a simulated defensive player during side-step cutting. Specifically, we used peak knee-abduction (valgus) angle as our primary outcome due to its association with ACL loading.31 Given that our intention was to simply compare kinematic data between 2 given conditions at a time, we based our estimate on the difference between 2 dependent means. Data from 16 healthy individuals (8 men, 8 women) demonstrated a 3.7° increase in knee-abduction angle in response to cutting in front of a simulated defender. Using the most conservative estimate of variability from these data (±5.1°), we estimated that a sample size of 30 participants would be needed to detect a difference between conditions (α = .05, 1 − β = 0.80).
RESULTS
On average, participants reported a current physical activity level of 6.8 ± 1.0 on the Tegner Activity Scale and a Knee Injury and Osteoarthritis Outcome Score of 98.1 ± 2.7, indicating a high level of subjective knee function. The average approach speed was 4.8 ± 0.3 m/s (range = 4.0–5.5 m/s). We observed a main effect of anticipation on approach speed (F1,31 = 229.79; P < .001), indicating that a faster approach was used during unanticipated cutting trials (4.94 versus 4.64 m/s; P < .001). We also noted a main effect of task (F2,62 = 3.82; P = .03), indicating that a slower approach was used during trials when participants planned to attend to a ball than those with no ball throw (4.75 versus 4.84 m/s; P = .03). We found a main effect of anticipation on the percentage of failed trials (F1,31 = 19.07; P < .001), indicating that failed trials occurred more often when participants performed unanticipated cutting trials (25.4% versus 13.3%; P < .001; Figure 2). The average self-reported fatigue level was 2.5 ± 1.1 on the visual analog scale (range, 2.1–2.8) and did not change throughout testing (F3,125 = 2.61; P = .06). Triplanar trunk, hip-joint, and knee-joint angles are presented in Figure 3, and only differences are shown in Table 1. All differences are depicted with associated CIs in Supplemental Figures 1 through 3 (available online at http://dx.doi.org/10.4085/1062-6050-569-18.S1). Differences that occurred during the first 25% of the stance phase are presented in Table 2, and mean differences are highlighted in this section. On average, peak vertical ground reaction force occurred between 18% and 20% of stance.
Figure 2.

Percentage of failed cutting trials per experimental condition. a Indicates difference (P ≤ .05).
Figure 3.

Mean triplanar knee, hip, and trunk angles plotted throughout the stance phase of a 45° side-step cutting task. Data are presented for each level of anticipation and dual tasking. Vertical lines represent 25% of the stance phase.
Table 1.
Observed Differences in Trunk Angles Between Conditions Throughout the Stance Phase of a Side-Step Cutting Maneuver
| Condition |
Plane |
Stance, %a |
Mean Difference, ° (95% Confidence Interval)b |
Effect Size (95% Confidence Interval)c |
| Task (anticipated) | ||||
| No ball throw versus ball throw | Sagittal | 0–85 | 3.7 (3.0, 4.4) | 2.7 (2.0, 3.4) |
| No ball throw versus ball throw | Frontal | 0–100 | 5.5 (4.7, 6.3) | 3.3 (2.5, 4.0) |
| No ball throw versus ball fake | Frontal | 0–100 | 4.9 (4.1, 5.8) | 2.9 (2.2, 3.5) |
| No ball throw versus ball throw | Transverse | 25–100 | 8.7 (5.9, 11.4) | 1.6 (1.0, 2.1) |
| No ball throw versus ball fake | Transverse | 88–100 | 2.7 (2.6, 2.8) | 20.2 (16.6, 23.7) |
| Ball throw versus ball fake | Transverse | 28–100 | 6.3 (3.8, 8.8) | 1.3 (0.7, 1.8) |
| Task (unanticipated) | ||||
| No ball throw versus ball throw | Sagittal | 8–72 | 2.9 (2.5, 3.3) | 3.6 (2.8, 4.4) |
| No ball throw versus ball throw | Frontal | 0–38 | 5.7 (5.1, 6.3) | 4.7 (3.8, 5.7) |
| No ball throw versus ball fake | Frontal | 0–100 | 4.4 (3.5, 5.2) | 2.6 (1.9, 3.2) |
| No ball throw versus ball throw | Transverse | 0–100 | 9.7 (5.3, 14.0) | 1.1 (0.6, 1.6) |
| No ball throw versus ball fake | Transverse | 33–100 | 4.6 (2.4, 6.8) | 1.0 (0.5, 1.6) |
| Ball throw versus ball fake | Transverse | 13–100 | 6.2 (2.8, 9.7) | 0.9 (0.4, 1.4) |
| Additive effect | ||||
| Anticipated no ball throw versus unanticipated ball throw | Sagittal | 0–59 | 4.2 (3.9, 4.4) | 8.4 (6.9, 9.9) |
| Anticipated no ball throw versus unanticipated ball fake | Frontal | 0–69 | 4.6 (3.6, 5.6) | 2.3 (1.7, 3.0) |
| Anticipated no ball throw versus unanticipated ball throw | Frontal | 0–100 | 5.4 (4.5, 6.3) | 3.0 (2.3, 3.8) |
| Anticipated ball fake versus unanticipated no ball throw | Frontal | 0–100 | 4.9 (4.0, 5.7) | 2.9 (2.2, 3.5) |
| Anticipated ball throw versus unanticipated no ball throw | Frontal | 0–100 | 5.4 (4.6, 6.3) | 3.3 (2.5, 4.0) |
| Anticipated no ball throw versus unanticipated ball throw (transverse) | Transverse | 24–100 | 9.7 (6.7, 12.7) | 1.6 (1.1, 2.2) |
| Anticipated no ball throw versus unanticipated ball fake | Transverse | 92–100 | 4.3 (4.2, 4.4) | 47.4 (39.2, 55.7) |
Percentage of stance phase from 0 (initial contact) to 100 (toe-off).
Mean differences with associated 95% confidence intervals between conditions during regions in which confidence intervals did not overlap.
Cohen d effect sizes with associated 95% confidence intervals between conditions using the pooled SD.
Table 2.
Observed Differences in Trunk Angles Between Conditions Within the First 25% of a Side-Step Cutting Maneuver
| Condition |
Plane |
Stance, % |
Mean Difference, ° (95% Confidence Interval)a |
Effect Size (95% Confidence Interval)b |
| Task (anticipated) | ||||
| No ball throw versus ball throw | Sagittal | 0–25 | 3.7 (3.6, 3.8) | 16.3 (13.5, 19.2) |
| No ball throw versus ball throw | Frontal | 0–25 | 5.2 (4.9, 5.5) | 8.1 (6.6, 9.6) |
| No ball throw versus ball fake | Frontal | 0–25 | 4.7 (4.4, 5.0) | 7.2 (5.8, 8.5) |
| Task (unanticipated) | ||||
| No ball throw versus ball throw | Sagittal | 8–25 | 2.9 (2.9, 3.0) | 30.1 (24.8, 35.3) |
| No ball throw versus ball throw | Frontal | 0–25 | 5.9 (5.6, 6.2) | 9.8 (8.0, 11.5) |
| No ball throw versus ball fake | Frontal | 0–25 | 4.7 (4.4, 5.1) | 7.6 (6.2, 8.9) |
| No ball throw versus ball throw | Transverse | 0–25 | 7.1 (6.0, 8.2) | 3.4 (2.6, 4.1) |
| Ball throw versus ball fake | Transverse | 13–25 | 5.3 (4.6, 5.9) | 4.1 (3.2, 4.9) |
| Additive effect | ||||
| Anticipated no ball throw versus unanticipated ball throw | Sagittal | 0–25 | 4.1 (4.0, 4.2) | 25.9 (21.4, 30.4) |
| Anticipated no ball throw versus unanticipated ball fake | Frontal | 0–25 | 4.3 (3.9, 4.6) | 6.3 (5.1, 7.4) |
| Anticipated no ball throw versus unanticipated ball throw (frontal) | Frontal | 0–25 | 5.4 (5.2, 5.7) | 9.9 (8.1, 11.7) |
| Anticipated ball fake versus unanticipated no ball throw | Frontal | 0–25 | 5.2 (4.9, 5.5) | 8.7 (7.1, 10.3) |
| Anticipated ball throw versus unanticipated no ball throw | Frontal | 0–25 | 5.6 (5.3, 5.9) | 9.7 (8.0, 11.5) |
Mean differences with associated 95% confidence intervals between conditions during regions in which confidence intervals did not overlap.
Cohen d effect sizes with associated 95% confidence intervals between conditions using the pooled SD.
Influence of Anticipation on Cutting
We observed no differences in trunk, hip-joint, or knee-joint angles between the anticipated and unanticipated cutting conditions for any level of task.
Influence of Motor-Motor Task on Anticipated Cutting
No differences were found in hip-joint or knee-joint angles between task levels during anticipated cutting. During the first 25% of stance, the trunk was more extended (3.7°) and less laterally flexed toward the cutting direction (5.2°) while the participants attended to a ball than for no ball throw. In addition, the trunk was less laterally flexed toward the cutting direction (4.7°) when the recruits planned to attend to a ball than for no ball throw.
Influence of Motor-Motor Task on Unanticipated Cutting
We found no differences in hip-joint or knee-joint angles between task levels during unanticipated cutting. During the first 25% of stance, the trunk was more extended (2.9°), less laterally flexed toward the cutting direction (5.9°), and more rotated away from the cutting direction (7.1°) when the participants attended to a ball than for no ball throw. In addition, the trunk was less laterally flexed toward the cutting direction (4.7°) when the individuals planned to attend to a ball than for no ball throw. Last, the trunk was more rotated away from the cutting direction (5.3°) when attending to a ball than planning to attend to a ball.
Influence of the Additive Effect on Cutting
No differences were found in hip-joint or knee-joint angles when compared between the combined conditions of anticipation and task. During the first 25% of stance, the trunk was more extended (4.1°) when attending to a ball with the cutting direction unanticipated and less laterally flexed toward the cutting direction when attending to (5.4°) or planning to attend to (4.3°) a ball than anticipated cutting with no ball throw. The trunk was less laterally flexed toward the cutting direction when attending to (5.6°) or planning to attend to (5.2°) a ball with the cutting direction anticipated than unanticipated cutting with no ball throw.
DISCUSSION
The principal finding of our study was that motor-motor task performance and the additive effect of anticipation and motor-motor task performance influenced trunk position but not hip or knee position while cutting. Regardless of anticipation, attending to a ball resulted in more trunk extension and less lateral trunk flexion toward the cutting direction (more upright and neutral). Furthermore, planning to attend to a ball resulted in less lateral trunk flexion toward the cutting direction. When the cutting direction was unanticipated, more trunk rotation away from the cutting direction was present only when participants were attending to a ball (more neutral). Collectively, these findings suggested that performing a motor-motor task by attending to an external object promoted an upright and neutral trunk position during a side-step cutting maneuver. Contrary to our hypothesis and previous findings,12,14,15 anticipation alone had no effect on trunk, hip, or knee position. However, our hypothesis that motor-motor task performance would have a greater influence on cutting biomechanics than anticipation was supported (range = 2.7°–9.7°). Whereas the additive effect of anticipation and motor-motor task performance also influenced trunk position in the sagittal and frontal planes, it did not appear to have a greater influence on the observed changes (range = 4.2°–9.7°). To our knowledge, this was the first study to combine anticipation and motor-motor task performance during an athletic maneuver, such as side-step cutting, in a controlled laboratory setting.
Trunk motion has been reported to influence lower extremity kinematics and joint loading,11,32,33 yet we did not demonstrate this relationship. More trunk flexion in the sagittal plane (mean = 47°) has been reported to cause subsequent increases in hip and knee flexion during landing.33 Also, individuals with more trunk flexion displayed less vertical ground reaction force and quadriceps electromyographic activity during landing; thus, we suggest that trunk position plays a role in lower extremity joint loading.11 Given that the changes in trunk position in our study favored a more erect posture, we would have expected decreases in hip and knee flexion as well. A possible explanation for this may be related to the amount of change that occurred. The maximum change in trunk position in our study did not exceed 5° in the sagittal plane (range = 2.9°–4.2°), 6° in the frontal plane (range = 4.4°–5.7°), or 10° in the transverse plane (range = 2.7°–9.7°). This may be attributed to the inherent difference between landing and cutting tasks: more sagittal-plane trunk displacement would be expected during a drop landing. Therefore, the differences may have been due to the physical aspect of reaching (or planning to reach) for the ball rather than a physiological or cognitive response related to dual tasking. Our observation of several differences between the ball-fake and ball-throw conditions may suggest that physically attending to a ball has a greater influence on trunk motion than planning to reach alone.
Trunk position did not influence hip or knee position in our study. However, in their investigation of landing mechanics, Sheehan et al32 indicated that landing with a more upright trunk posture (posterior center of mass relative to the base of support) was a risk factor for noncontact ACL injury. Although not directly comparable with the findings from landing studies, this factor may help to expand on the relevance of our findings during cutting. Frank et al9 advocated for trunk rotation toward the new direction of travel (away from the stance limb) to minimize the internal knee-varus moment. Relevant to our findings, previous authors23 have investigated the influence of upper limb position on knee loading during a side-step cutting maneuver. They noted that constraining the plant-side limb with either a football or lacrosse stick increased the knee-valgus moment. Given these data, one can infer that the plant-side limb inherently extends to stabilize the body during cutting. In contrast to these findings, we induced a more flexed position of the upper limb when catching a ball, which may have also altered the ability to stabilize the body during cutting. Therefore, the large-magnitude differences in trunk angle toward an upright, neutral position during the first 25% of the cutting task when loading was greatest seem to be a clinically meaningful finding. This is especially important due to the heightened risk of ACL injury during movement initiation.15,29,30 Because motor-motor task performance appeared to promote an upright and neutral trunk position, incorporating feedback to encourage greater trunk flexion and trunk rotation away from the stance limb may be warranted to reduce the injury risk during a side-step cutting task. Based on our findings, providing a reach target (eg, ball-throw or ball-fake condition) rather than altering only the individual's knowledge of the cutting direction may be an effective training strategy.
Hip and knee angles were not influenced by anticipation or motor-motor task performance in our study. Researchers20,22 have reported differences in sagittal- and frontal-plane lower extremity kinematics while dual tasking (catching a basketball or visualizing a simulated defender) during anticipated side-step cutting. Specifically, increased flexion and abduction was apparent at the knee and hip.20,22 Although changes in hip and knee kinematics have occurred in response to variable dual-tasking paradigms, the differences were small (range = 2°–6°) and may not represent clinically meaningful kinematic changes. The lack of differences in lower extremity kinematics in our study may be explained in part by the dynamic systems theory. According to this theory, the body attempts to optimize the efficiency of movement during a task.34 However, individual performance is largely influenced by the health of the person, the task being performed, and the environment in which the task is being performed. Increased task complexity coupled with a changing environment would be expected to reduce the strategies available for successful completion of a task. In our study, the lower extremity kinematics remained similar regardless of complexity, suggesting that the number of movement strategies for successfully completing the specific task is limited. Stated differently, to cut at a specific location in a 45° angle, perhaps individuals have a limited number of positions through which they can move the hip and knee to successfully complete the task. If too much deviation occurred at any joint, the trial was considered a failure according to our definition. Therefore, our participants may have used very similar movement strategies for all successful trials. Although speculative, this may begin to explain why we did not observe differences in lower extremity kinematics between conditions. In support of this theory, we observed a general increase in the number of failed trials as the complexity of the task increased (Figure 2). This finding appears to support the need for additional practice or training before performing unanticipated motor-motor tasks in an uncontrolled environment.
Clinical Implications
Current recommendations35 for lower extremity injury-prevention programs include incorporating strength training, plyometrics, balance, technique feedback, sufficient dosing, and minimal equipment requirements. However, little evidence is currently available to support including anticipation and motor-motor dual tasking in prevention programs. By promoting task complexity during end-stage rehabilitation and injury-prevention programs, athletes may become better prepared to succeed when performing high-risk movement tasks. Our findings suggested that, as the task became more complex or closer to resembling a game-like scenario, athletes may have been less likely to complete it successfully as defined by our laboratory. This idea is supported by the greater percentage of failed trials that occurred when the cutting direction was unanticipated. Whereas dual tasking resulted in similar kinematic changes regardless of anticipation, the number of failed trials appeared to increase with task complexity. Consequently, athletes may be at greatest risk for sustaining an injury when performing highly complex tasks. This appears to support the need for training in an uncontrolled, unpredictable environment, which may have implications for injury-prevention programs.
Limitations
The conclusions drawn from these results should be viewed in light of certain study limitations. First, we did not evaluate the kinematic response to each component of the motor-motor task independently (eg, cutting + no ball, cutting + ball, standing to catch a ball) and, therefore, cannot be certain of the changes due to adding another task. Although the individual components of this task inherently involved different motor commands, they represented what an individual may experience during an athletic event. Second, in the absence of known minimal clinically important differences or minimal detectable change values for trunk kinematics during cutting, the clinical effect of our findings remains in question. Third, variability in approach speed may have influenced our findings. Previous researchers have restricted speed to a greater degree, but our participants' speed was comparable with (range = 4.5–5 m/s)15 or faster than (3 m/s)12 speeds previously described. Given that athletes are more likely to perform at maximum effort than at standardized speed, we believed our range was adequate to maintain generalizability. In addition, variability could have existed in the timing and location of the ball throw among trials and participants. The individual throwing the ball was instructed to throw the ball 1 step before the participant contacted the force plate so that he had to catch it while landing on the force plate to make the cut. To help increase the consistency, we allowed for ample warm-up trials between the ball thrower and the participant so they could determine the correct timing. However, the ball throw was relatively controlled, which may not adequately reflect the variability experienced during athletic events. Fourth, it is possible that the healthy sample of college-aged men could partially explain our lack of lower extremity differences in that young women have a higher incidence of ACL injury. Future studies should be conducted to determine the influence of factors such as sex, age, skill level, and history of injury on the biomechanical response to anticipation and dual tasking. Fifth, we analyzed only successful trials using the dominant limb, which likely represented optimal movement patterns. It is possible that greater differences would have been identified if the failed trials or nondominant limb or both were analyzed. Sixth, joint moments were not included in this analysis due to technical limitations. Future evaluations of concurrent kinematic, kinetic, and electromyographic responses to dual-tasking paradigms are warranted to better understand the clinical implications of aberrant movement patterns.
CONCLUSIONS
Motor-motor task performance and its interaction with anticipation promoted a more upright, neutral trunk position during side-step cutting, which has been associated with the risk for noncontact knee injury. Current recommendations for injury prevention do not consider anticipation or dual tasking. By promoting task complexity during end-stage rehabilitation and injury-prevention programs, physically active individuals may become better prepared to succeed when performing high-risk athletic maneuvers.
Supplementary Material
ACKNOWLEDGMENTS
We thank Elizabeth Sares for her assistance in data collection.
REFERENCES
- 1.Hefti F, Muller W, Jakob RP, Staubli HU. Evaluation of knee ligament injuries with the IKDC form. Knee Surg Sports Traumatol Arthrosc. 1993;1(3–4):226–234. doi: 10.1007/BF01560215. [DOI] [PubMed] [Google Scholar]
- 2.Sheppard JM, Young WB. Agility literature review: classifications, training and testing. J Sports Sci. 2006;24(9):919–932. doi: 10.1080/02640410500457109. [DOI] [PubMed] [Google Scholar]
- 3.Boden BP, Dean GS, Feagin JA, Jr, Garrett WE., Jr Mechanisms of anterior cruciate ligament injury. Orthopedics. 2000;23(6):573–578. doi: 10.3928/0147-7447-20000601-15. [DOI] [PubMed] [Google Scholar]
- 4.Sigward SM, Powers CM. Loading characteristics of females exhibiting excessive valgus moments during cutting. Clin Biomech (Bristol Avon) 2007;22(7):827–833. doi: 10.1016/j.clinbiomech.2007.04.003. [DOI] [PubMed] [Google Scholar]
- 5.Griffin LY, Agel J, Albohm MJ, et al. Noncontact anterior cruciate ligament injuries: risk factors and prevention strategies. J Am Acad Orthop Surg. 2000;8(3):141–150. doi: 10.5435/00124635-200005000-00001. [DOI] [PubMed] [Google Scholar]
- 6.Webster KE, Hewett TE. Meta-analysis of meta-analyses of anterior cruciate ligament injury reduction training programs. J Orthop Res. 2018;36(10):2696–2708. doi: 10.1002/jor.24043. [DOI] [PubMed] [Google Scholar]
- 7.Luc B, Gribble PA, Pietrosimone BG. Osteoarthritis prevalence following anterior cruciate ligament reconstruction: a systematic review and numbers-needed-to-treat analysis. J Athl Train. 2014;49(6):806–819. doi: 10.4085/1062-6050-49.3.35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Andrews JR, McLeod WD, Ward T, Howard K. The cutting mechanism. Am J Sports Med. 1977;5(3):111–121. doi: 10.1177/036354657700500303. [DOI] [PubMed] [Google Scholar]
- 9.Frank B, Bell DR, Norcross MF, Blackburn JT, Goerger BM, Padua DA. Trunk and hip biomechanics influence anterior cruciate loading mechanisms in physically active participants. Am J Sports Med. 2013;41(11):2676–2683. doi: 10.1177/0363546513496625. [DOI] [PubMed] [Google Scholar]
- 10.Arendt E, Dick R. Knee injury patterns among men and women in collegiate basketball and soccer: NCAA data and review of literature. Am J Sports Med. 1995;23(6):694–701. doi: 10.1177/036354659502300611. [DOI] [PubMed] [Google Scholar]
- 11.Blackburn JT, Padua DA. Sagittal-plane trunk position, landing forces, and quadriceps electromyographic activity. J Athl Train. 2009;44(2):174–179. doi: 10.4085/1062-6050-44.2.174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Besier TF, Lloyd DG, Ackland TR, Cochrane JL. Anticipatory effects on knee joint loading during running and cutting maneuvers. Med Sci Sports Exerc. 2001;33(7):1176–1181. doi: 10.1097/00005768-200107000-00015. [DOI] [PubMed] [Google Scholar]
- 13.Brown TN, Palmieri-Smith RM, McLean SG. Sex and limb differences in hip and knee kinematics and kinetics during anticipated and unanticipated jump landings: implications for anterior cruciate ligament injury. Br J Sports Med. 2009;43(13):1049–1056. doi: 10.1136/bjsm.2008.055954. [DOI] [PubMed] [Google Scholar]
- 14.Houck JR, Duncan A, De Haven KE. Comparison of frontal plane trunk kinematics and hip and knee moments during anticipated and unanticipated walking and side step cutting tasks. Gait Posture. 2006;24(3):314–322. doi: 10.1016/j.gaitpost.2005.10.005. [DOI] [PubMed] [Google Scholar]
- 15.Weinhandl JT, Earl-Boehm JE, Ebersole KT, Huddleston WE, Armstrong BS, O'Connor KM. Anticipatory effects on anterior cruciate ligament loading during sidestep cutting. Clin Biomech (Bristol Avon) 2013;28(6):655–663. doi: 10.1016/j.clinbiomech.2013.06.001. [DOI] [PubMed] [Google Scholar]
- 16.Imwalle LE, Myer GD, Ford KR, Hewett TE. Relationship between hip and knee kinematics in athletic women during cutting maneuvers: a possible link to noncontact anterior cruciate ligament injury and prevention. J Strength Cond Res. 2009;23(8):2223–2230. doi: 10.1519/JSC.0b013e3181bc1a02. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Yogev-Seligmann G, Hausdorff JM, Giladi N. The role of executive function and attention in gait. Mov Disord. 2008;23(3):329–342. doi: 10.1002/mds.21720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Saxena S, Cinar E, Majnemer A, Gagnon I. Does dual tasking ability change with age across childhood and adolescence? A systematic scoping review. Int J Dev Neurosci. 2017;58:35–49. doi: 10.1016/j.ijdevneu.2017.01.012. [DOI] [PubMed] [Google Scholar]
- 19.Asai T, Misu S, Doi T, Yamada M, Ando H. Effects of dual-tasking on control of trunk movement during gait: respective effect of manual- and cognitive-task. Gait Posture. 2014;39(1):54–59. doi: 10.1016/j.gaitpost.2013.05.025. [DOI] [PubMed] [Google Scholar]
- 20.Fedie R, Carlstedt K, Willson JD, Kernozek TW. Effect of attending to a ball during a side-cut maneuver on lower extremity biomechanics in male and female athletes. Sports Biomech. 2010;9(3):165–177. doi: 10.1080/14763141.2010.502241. [DOI] [PubMed] [Google Scholar]
- 21.Vallabhajosula S, Tan CW, Mukherjee M, Davidson AJ, Stergiou N. Biomechanical analyses of stair-climbing while dual-tasking. J Biomech. 2015;48(6):921–929. doi: 10.1016/j.jbiomech.2015.02.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.McLean SG, Lipfert SW, van den Bogert AJ. Effect of gender and defensive opponent on the biomechanics of sidestep cutting. Med Sci Sports Exerc. 2004;36(6):1008–1016. doi: 10.1249/01.mss.0000128180.51443.83. [DOI] [PubMed] [Google Scholar]
- 23.Chaudhari AM, Hearn BK, Andriacchi TP. Sport-dependent variations in arm position during single-limb landing influence knee loading: implications for anterior cruciate ligament injury. Am J Sports Med. 2005;33(6):824–830. doi: 10.1177/0363546504270455. [DOI] [PubMed] [Google Scholar]
- 24.Roos EM, Roos HP, Lohmander LS, Ekdahl C, Beynnon BD. Knee Injury and Osteoarthritis Outcome Score (KOOS)—development of a self-administered outcome measure. J Orthop Sports Phys Ther. 1998;28(2):88–96. doi: 10.2519/jospt.1998.28.2.88. [DOI] [PubMed] [Google Scholar]
- 25.Cortes N, Onate J, Van Lunen B. Pivot task increases knee frontal plane loading compared with sidestep and drop-jump. J Sports Sci. 2011;29(1):83–92. doi: 10.1080/02640414.2010.523087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Dos'Santos T, Bishop C, Thomas C, Comfort P, Jones PA. The effect of limb dominance on change of direction biomechanics: a systematic review of its importance for injury risk. Phys Ther Sport. 2019;37:179–189. doi: 10.1016/j.ptsp.2019.04.005. [DOI] [PubMed] [Google Scholar]
- 27.Ericksen HM, Thomas AC, Gribble PA, Armstrong C, Rice M, Pietrosimone B. Jump-landing biomechanics following a 4-week real-time feedback intervention and retention. Clin Biomech (Bristol Avon) 2016;32:85–91. doi: 10.1016/j.clinbiomech.2016.01.005. [DOI] [PubMed] [Google Scholar]
- 28.Donovan L, Hart JM, Saliba S, et al. Effects of ankle destabilization devices and rehabilitation on gait biomechanics in chronic ankle instability patients: a randomized controlled trial. Phys Ther Sport. 2016;21:46–56. doi: 10.1016/j.ptsp.2016.02.006. [DOI] [PubMed] [Google Scholar]
- 29.Kernozek TW, Ragan RJ. Estimation of anterior cruciate ligament tension from inverse dynamics data and electromyography in females during drop landing. Clin Biomech (Bristol Avon) 2008;23(10):1279–1286. doi: 10.1016/j.clinbiomech.2008.08.001. [DOI] [PubMed] [Google Scholar]
- 30.Laughlin WA, Weinhandl JT, Kernozek TW, Cobb SC, Keenan KG, O'Connor KM. The effects of single-leg landing technique on ACL loading. J Biomech. 2011;44(10):1845–1851. doi: 10.1016/j.jbiomech.2011.04.010. [DOI] [PubMed] [Google Scholar]
- 31.Kiapour AM, Demetropoulos CK, Kiapour A, et al. Strain response of the anterior cruciate ligament to uniplanar and multiplanar loads during simulated landings: implications for injury mechanism. Am J Sports Med. 2016;44(8):2087–2096. doi: 10.1177/0363546516640499. [DOI] [PubMed] [Google Scholar]
- 32.Sheehan FT, Sipprell WH, Boden BP. Dynamic sagittal-plane trunk control during anterior cruciate ligament injury. Am J Sports Med. 2012;40(5):1068–1074. doi: 10.1177/0363546512437850. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Blackburn JT, Padua DA. Influence of trunk flexion on hip and knee joint kinematics during a controlled drop landing. Clin Biomech (Bristol Avon) 2008;23(3):313–319. doi: 10.1016/j.clinbiomech.2007.10.003. [DOI] [PubMed] [Google Scholar]
- 34.Davids K, Glazier P, Araujo D, Bartlett R. Movement systems as dynamical systems: the functional role of variability and its implications for sports medicine. Sports Med. 2003;33(4):245–260. doi: 10.2165/00007256-200333040-00001. [DOI] [PubMed] [Google Scholar]
- 35.Padua DA, DiStefano LJ, Hewett TE, et al. National Athletic Trainers' Association position statement: prevention of anterior cruciate ligament injury. J Athl Train. 2018;53(1):5–19. doi: 10.4085/1062-6050-99-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.