

The presence of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in fecal material has raised the possibility of viral transmission via a fecal–oral route. This study investigated whether SARS-CoV-2 transmission via fecal aerosols in the drainage pipe system may have been the cause of COVID-19 infection in a cluster of 3 families living in a high-rise building in China.
Visual Abstract. Fecal Aerosol Transmission of SARS-CoV-2.
The presence of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in fecal material has raised the possibility of viral transmission via a fecal–oral route. This study investigated whether SARS-CoV-2 transmission via fecal aerosols in the drainage pipe system may have been the cause of COVID-19 infection in a cluster of 3 families living in a high-rise building in China.
Abstract
Background:
The role of fecal aerosols in the transmission of severe acute respiratory syndrome coronavirus 2 has been suspected.
Objective:
To investigate the temporal and spatial distributions of 3 infected families in a high-rise apartment building and examine the associated environment variables to verify the role of fecal aerosols.
Design:
Epidemiologic survey and quantitative reverse transcriptase polymerase chain reaction analyses on throat swabs from the participants; 237 surface and air samples from 11 of the 83 flats in the building, public areas, and building drainage systems; and tracer gas released into bathrooms as a surrogate for virus-laden aerosols in the drainage system.
Setting:
A high-rise apartment building in Guangzhou, China.
Participants:
9 infected patients, 193 other residents of the building, and 24 members of the building's management staff.
Measurements:
Locations of infected flats and positive environmental samples, and spread of virus-laden aerosols.
Results:
9 infected patients in 3 families were identified. The first family had a history of travel to the coronavirus disease 2019 (COVID-19) epicenter Wuhan, whereas the other 2 families had no travel history and a later onset of symptoms. No evidence was found for transmission via the elevator or elsewhere. The families lived in 3 vertically aligned flats connected by drainage pipes in the master bathrooms. Both the observed infections and the locations of positive environmental samples are consistent with the vertical spread of virus-laden aerosols via these stacks and vents.
Limitation:
Inability to determine whether the water seals were dried out in the flats of the infected families.
Conclusion:
On the basis of circumstantial evidence, fecal aerosol transmission may have caused the community outbreak of COVID-19 in this high-rise building.
Primary Funding Source:
Key-Area Research and Development Program of Guangdong Province and the Research Grants Council of Hong Kong.
Most authorities state that severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is transmitted mainly by close contact and fomites (1–3). These assertions are probably supported by the observed data (4–6). After the detection of viral RNA and isolation of viable viruses from human feces (7–9), the fecal–oral route of transmission has been suspected (10, 11). Zhang and colleagues (12) reported the presence of SARS-CoV-2 in anal swabs, noting that in the later stage of infection, positive anal swab samples were more frequent than positive oral swab samples. Ong and colleagues (13) found positive test results from wipe samples from surfaces of bathrooms used by patients with SARS-CoV-2 infection. Virus-laden aerosols were detected in a recent air sampling study in a mobile toilet room used by patients at Fangcang Hospital (14). McDermott and colleagues (15) examined whether fecal bioaerosols are a route of transmission for SARS-CoV-2 in hospitals.
Here, we report an outbreak of 9 confirmed cases of coronavirus disease 2019 (COVID-19) between 26 January 2020 and 13 February 2020 in 3 vertically aligned flats in a high-rise building (block X) in Guangzhou, China, during a period of social distancing. Block X is 1 of 30 high-rise housing blocks in a 6-year-old private housing estate; it has 29 floors. There are 3 apartment units, designated as flats -01, -02, and -03, on each of floors 2 through 28 (Figure 1) and 2 flats on the 29th floor, for a total of 83 flats in the building. Dried floor drains have been a common hygiene issue that has led to vertical transmission of SARS-CoV-1 and SARS-CoV-2 in similar high-rise apartment buildings in southern China (16–19). In 2003, fecal aerosols were found to transmit SARS-CoV-1 to more than 300 residents in the Amoy Gardens outbreak (17). We took environmental samples and measured the drainage airflow dispersion of a tracer gas in block X to investigate the potential for a fecal aerosol transmission route of SARS-CoV-2.
Figure 1. The block X outbreak and suggested transmission route.
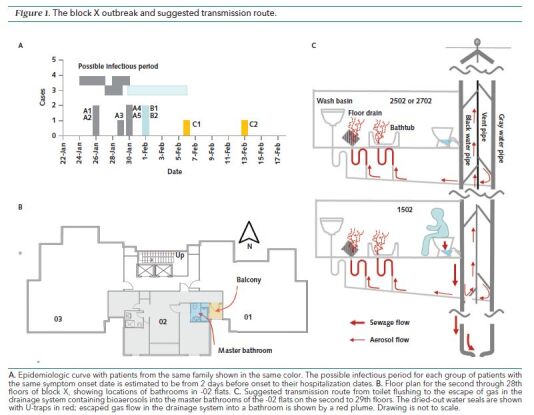
A. Epidemiologic curve with patients from the same family shown in the same color. The possible infectious period for each group of patients with the same symptom onset date is estimated to be from 2 days before onset to their hospitalization dates. B. Floor plan for the second through 28th floors of block X, showing locations of bathrooms in -02 flats. C. Suggested transmission route from toilet flushing to the escape of gas in the drainage system containing bioaerosols into the master bathrooms of the -02 flats on the second to 29th floors. The dried-out water seals are shown with U-traps in red; escaped gas flow in the drainage system into a bathroom is shown by a red plume. Drawing is not to scale.
Methods
We first obtained the dates of symptom onset of the 9 residents with SARS-CoV-2 infection and the locations of their flats within block X. The symptom onset date was defined as the day when the first symptom (fever or cough) was noticed by the patient. All infections were confirmed to be COVID-19 on the basis of throat swab and RNA test results. We collected demographic data, travel history, exposure history, and other symptoms experienced by the infected persons. We also collected a detailed site plan, floor plans, details of the drainage system on the basis of on-site measurement and design drawings, and hourly weather data from weather stations close to the site during the suspected infectious period (24 January through 6 February 2020). Closed-circuit television camera records from the 2 public elevators in block X were reviewed to obtain the elevator usage pattern for 25 January through 30 January.
Extended close-contact tracing and environmental detection were conducted from 9 February through 19 February. Throat swab specimens were collected from 193 residents and 24 management staff in block X. From 11 February through 19 February, 237 surface and air samples were taken from the building. Viral RNA was extracted from the samples by using PureLink Viral RNA/DNA kits (Invitrogen), and quantitative reverse transcriptase polymerase chain reaction assays were performed with a China Food and Drug Administration–approved commercial kit specific for SARS-CoV-2 detection (GeneoDX Biotech). The specimens were considered positive if the cycle threshold value was 37.0 or less.
Airflow and dispersion tests were performed on 21 February by using ethane as a tracer gas surrogate for virus-laden droplets in gas in the drainage system. Tracer gas has been shown to be an effective surrogate for modeling the spread of fine droplets or droplet nuclei (20). About 3.0 L/min of ethane was released into the drainage stack of the master bathroom in flat 1502 to model the virus-laden droplets generated during the hydraulic interactions of toilet wastewater and the stack. The tracer gas concentrations were monitored in other master bathrooms by using a 24-channel multipoint sampler and a photoacoustic gas monitor (Innova 1412i and 1409; LumaSense Technologies). In addition, computational fluid dynamics simulations were performed by using commercial Ansys Fluent 16.0 software to estimate the air pressure in the bathrooms. On the basis of findings from the 2003 Amoy Garden SARS outbreak (17), we expected that some floor drain water seals would be dry because residents do not often fill them with water. We also conducted a telephone survey of bathtub use habits in the -02 flats and found that some bathtubs must also have dried-out water seals. We then compared the infection distribution pattern and the measured tracer gas concentrations through the dried-out floor and bathtub drains in vertically aligned -02 apartments (Figure 1).
Role of the Funding Source
The funding source had no role in the design, conduct, and analysis of the study or the decision to submit the manuscript for publication.
Results
The estate comprises 3336 flats with a total of 5800 residents in 30 high-rise housing blocks. The chronologic sequence of events and our subsequent investigations, as well as the epidemic curve for Guangzhou city, are summarized in Supplement Figures 1 and 2. During the suspected infectious period (24 January through 6 February 2020), the prevailing wind was mostly northerly, with an average speed of 1.5 m/s (Supplement Figure 3). At the time of infection, block X had 202 residents in 57 families and 26 flats were unoccupied (see Supplement Table 1 for more details). Public elevator lobbies and a corridor connect the flats on each floor. Each of the -02 flats has 2 bathrooms.
Locations of the infected and noninfected families and the environmental samples are summarized in the Table (for further details see Supplement Figure 1 and Supplement Tables 2 to 4). The epidemic curve for block X is shown in Figure 1, A. The infected families were all from vertically aligned -02 flats (numbers 1502, 2502, and 2702). Family A in flat 1502 was first to be infected, with 2 elders showing fever and cough symptoms on 26 January, followed by 3 younger family members with symptom onset on 29 January or 30 January. Four members of family A had traveled to the epicenter, Wuhan, 14 days before their first onset date, and the fifth member had traveled to Jiangxi. They returned to Guangzhou together on 24 January. Family B (flat 2502) and family C (flat 2702) were both middle-aged couples, and they all slept in their master bedrooms. Family B had their symptom onset on 1 February. They are most likely to have been infected by family A, whereas various possibilities exist for family C, such as person C1 being infected by a member of family A or B and person C2 being infected by C1.
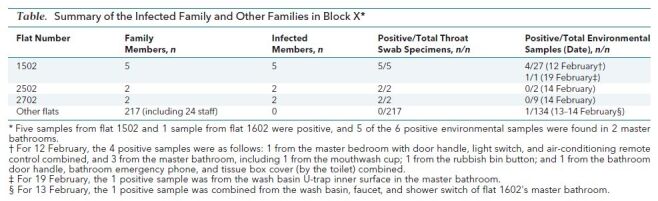
Table. Summary of the Infected Family and Other Families in Block X*.
According to the epidemic investigations by the Center for Disease Control and Prevention, families B and C had no travel history or close contact with any other confirmed cases, including family A members. In 2020, the Chinese New Year holiday was from 24 January to 30 January, and families B and C had stayed at home for most of that period. The 3 families did not know one another, and they had not shared use of the elevators during the possible infectious period. Moreover, 3 other block X residents had shared the elevators with at least 1 family A member, but none had become infected. Residents who used the elevator after members of family A might also have been exposed via fomites or recirculated air inside the elevator, but the exposure risks for the infected and noninfected families were not substantially different. For example, the 30-minute use exposure for family B, family C, and 54 other families were 3.0, 16.0, and 5.4 person-times per family, respectively (Supplement Table 6). In addition, family A members wore masks on most occasions while using the elevators, and viral RNA was not detected from the elevator button or air supply inlets.
Throat swab specimens from 217 other persons (residents and staff) in block X taken between 9 February and 11 February were all negative. Five environmental samples from flat 1502 and 1 sample from flat 1602 (unoccupied for more than 3 months before the outbreak) were positive (Table) among a total of 166 environmental and 7 air samples collected from 11 -02 flats and public areas from 11 February through 14 February. Sixty surface and 4 air samples taken from other public areas of block X, elevators, ventilation grills, and vent outlets on the roof all tested negative. The detection of all positive samples from areas in master bathrooms, except 1 positive sample in the 1502 master bedroom, suggests that the master bathrooms were the probable source and exposure venues.
A 2-pipe system is used for drainage in block X, with 2 sets of individual black water stacks, gray water stacks, and a vent in each of the master and guest bathrooms. This means that the vertically aligned master bathrooms in -02 flats are connected by the drainage stacks and vent. There is a bathtub in the master bathroom of each apartment but not in the guest bathroom. In the master bathroom, U-traps act as water seals for the wash basin, floor drain, toilet, and bathtub. Water seals in U-traps are generally 75 mm in depth and are expected to dry out in 30 days or sooner in dry conditions if no water is added. A telephone survey (Supplement Table 5) revealed that families in 11 of 16 -02 flats, including the infected families in 2502 and 2702, do not habitually use the bathtubs in their master bathrooms, which suggests that these bathtubs must also have had dried-out water seals. It is unfortunate that we were not able to determine whether the water seals were indeed dried out in 2502 and 2702, because an immediate disinfection campaign after the cases were discovered destroyed any evidence in those flats.
To examine the possibility that bioaerosols entered the bathrooms from drainage stacks, we continuously released tracer gas into the black water pipe through the toilet in flat 1502 for 30 minutes at 1:00 p.m. on 21 February while block X was still in quarantine. The doors and windows of the master bathrooms in 1502, 1602, 2102, 2502, and 2702 were kept open. Substantial tracer gas concentrations were detected in all the flats we monitored: 1602 (bathtub drain and floor drain, 559 and 94 ppm), 2102 (11 and 10 ppm), 2502 (27 and 20 ppm), and 2702 (597 and 587 ppm). Leaked tracer gas also was detected in flat 802 (floor drain, 1119 ppm) in a separate test when the water seals of the upper flats were present. These results demonstrate that the drainage pipes in block X might serve as a transport route for bioaerosols between the flats. The variation in monitored concentrations is probably a result of differences in the air pressures influenced by wind and flat location, as well as pipe–drain geometry. Supplement Figure 4 shows the vertical variation of negative pressure outside the -02 flat master bathrooms due to wind. Each household decorated its own bathrooms, and variation in the connecting pipes and water seal traps may have led to different pressure losses for the gas escape flow in the drainage system.
Discussion
Our epidemiologic and environmental data indicate that the infection source for patients in flat 2502 and possibly those in 2702 was probably the master bathroom of flat 1502, and virus-containing fecal aerosols were probably produced in the associated vertical stack during toilet flushing after use by the index patients. Yu and colleagues (17) found that large amounts of bioaerosols were generated in a similar high-rise vertical drainage stack as a result of hydraulic interactions after the index patient flushed a toilet in the 2003 Amoy Garden SARS outbreak, although the number, size, and virus concentration in these bioaerosols remain unknown. Toilet wastewater may contain feces, urine, and exhaled mucus from the index patients; 2.0% to 49.5% of patients with COVID-19 have had diarrhea (11), and viral RNA has been detected in stool samples from patients (7, 8). The presence of SARS-CoV-2 in anal swab samples was also reported by Zhang and colleagues (12), who also found that more anal swab than oral swab specimens were positive in later stages of infection. In addition, SARS-CoV-2 was isolated from a stool specimen by researchers in China (9), confirming the presence of viable virus in the feces of patients with COVID-19 and its potential infectivity. High sequence similarity between SARS-CoV-2 and SARS-CoV-1 has been reported. A high viral load also has been detected in stool samples from patients with SARS (21).
The 3 young members of family A, who slept in the master bedroom, are suspected to be the index patients for family B, person C1, and possibly person C2. When an index patient used and flushed the toilet in the master bathroom of flat 1502, the dried-out floor or bathtub drain in the same bathroom may have enabled virus-laden bioaerosols to leak back into the room (Figure 1, C) as well as to other rooms connected to the drainage system. Such a possibility is supported by 1 positive surface sample from the master bathroom of flat 1602, and partly supported by the 4 positive surface samples from the master bathroom in 1502 and possibly also the 1 positive surface sample from the same flat's master bedroom. These positive samples were collected from frequently touched surfaces and the inner surface of the wash basin's U-trap, as listed in Supplement Table 4. The positive samples from flat 1502 also suggest that the hands of the index patients may have been contaminated while using the toilet, but we cannot rule out the possibility of touching deposited aerosols that re-entered the bathroom from the dried-out drain. Furthermore, all surface samples from other public areas were negative.
The same suck-in phenomenon may have occurred in other master bathrooms in the -02 flats. If another resident, for example from flat 2502 or 2702, happened to be in their bathroom at the same time the index patient's toilet was flushed, they may have inhaled some of the sucked-in bioaerosols. The exact timing of toilet use by an index patient is unknown, but the likelihood that 2 of the -02 families used their master bathrooms at the same time is intuitively low. However, bioaerosols of sufficiently small size are likely to be airborne in drainage pipes and vents for hours, and they can be sucked into a bathroom continuously when relevant conditions are met, as described later. The transient movement of bioaerosols in the drainage stacks and vents may be the result of a buoyancy (chimney) effect, falling wastewater, or both. The buoyancy effect may occur when the temperature and humidity differ between the air in the drainage pipes and the air in the bathrooms. The stack and vent for the master bathroom are located indoors in a service conduit in block X; even a small difference in air temperature and humidity would cause a substantial stack effect because the “chimneys” (that is, the vent and stack pipes) are nearly 90 m tall (Figure 2). However, the exact location of the neutral level is unknown, although it probably is located below mid-height, because leaked-out gases were also detected in flats below 1502. Neutral level is where the pressures in the room and in the chimney are equal (22).
Figure 2. Illustration of the buoyancy (chimney) effect, with inflows into the vent at lower stories and outflows into the bathrooms at upper stories when the source bathroom is above (left) and below (right) the neutral level.
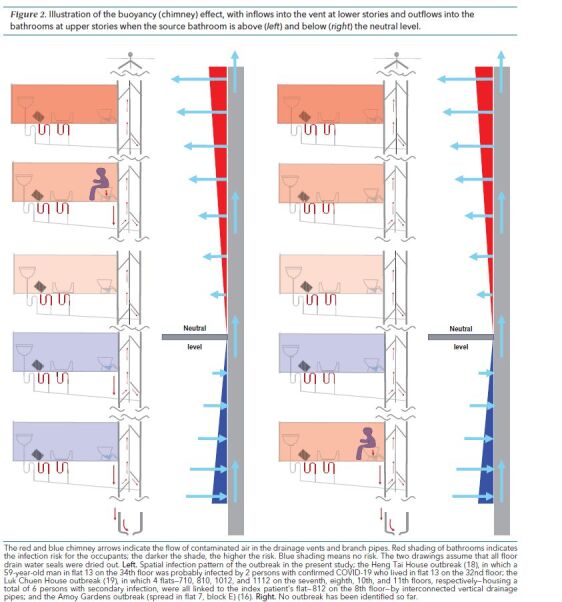
The red and blue chimney arrows indicate the flow of contaminated air in the drainage vents and branch pipes. Red shading of bathrooms indicates the infection risk for the occupants; the darker the shade, the higher the risk. Blue shading means no risk. The two drawings assume that all floor drain water seals were dried out. Left. Spatial infection pattern of the outbreak in the present study; the Heng Tai House outbreak (18), in which a 59-year-old man in flat 13 on the 34th floor was probably infected by 2 persons with confirmed COVID-19 who lived in flat 13 on the 32nd floor; the Luk Chuen House outbreak (19), in which 4 flats—710, 810, 1012, and 1112 on the seventh, eighth, 10th, and 11th floors, respectively—housing a total of 6 persons with secondary infection, were all linked to the index patient's flat—812 on the 8th floor—by interconnected vertical drainage pipes; and the Amoy Gardens outbreak (spread in flat 7, block E) (16). Right. No outbreak has been identified so far.
In addition to the buoyancy effect, the suction flow rate for each flat depends on the negative pressure in its bathroom. Negative pressure may be caused by the use of an exhaust fan or by a northerly wind that creates a wake flow when the bathroom has a window onto a balcony. According to the phone survey (Supplement Table 5), only the occupants in flats 2502 and 2702 never open the window of their master bathrooms, and the use of an exhaust fan might create a negative pressure and impose a higher fecal aerosol infiltration risk compared with the master bathrooms in other flats. Computational fluid dynamics simulations showed that the negative pressure in the flats may be as high as 16.8 Pa (Supplement Figure 4). Most upper -02 flats with dried-out traps probably have a similar risk for infection if the wind or fan pressures are similar when the buoyancy (chimney) effect is absent. When this sucked-in effect is combined with the stack (chimney) effect, the uppermost floors are the most “polluted,” which explains the higher concentration measured on those floors. The positive sample in unoccupied flat 1602 suggests that the wind generated its negative pressure, because its exhaust fans were probably not turned on at the time. It is possible that bioaerosols sucked into the bathroom would deposit on some surfaces and subsequently be touched by residents and spread to other surfaces (23).
The bioaerosolization of wastewater mixed with urine, feces, and exhaled mucus originating from index patients is suggested to be the source of infectious bioaerosols in this outbreak. The production of fecal aerosols in the drainage pipe is supported by a positive sample from inside the wash basin U-trap in the master bathroom that was detected as late as 19 February. These bioaerosols probably entered some master bathrooms through dried-out floor or bathtub drains. The bioaerosols were generated during toilet flushing and then spread via the drainage stacks and vents with minimum dilution. This behavior differs from that of expired jets or puffs in open space, where the concentration of virus-containing droplets rapidly decreases as the distance from infected persons increases, because of jets or puffs mixing with room air. Thus, the concentration of virus in drainage pipes can remain very high even after the virus travels a long distance. These bioaerosols might be inhaled directly by a bathroom's occupants or be deposited on room surfaces, which might later be touched by occupants. With positive surface samples in the 2 master bathrooms (1502 and 1602), a possibility exists of surface contamination by aerosols and subsequent mucous membrane infection, rather than inhalation. Either inhalation or fomite transmission of these fecal aerosols constitutes the route for the respiratory infection. An investigation of the 2003 Amoy Gardens SARS outbreak in Hong Kong (17) also suggested that SARS-CoV is likely to transmit in the form of virus-laden fecal aerosols through exhaust air or vent pipes. A fecal–respiratory route was also suggested for the 2003 Amoy Gardens SARS outbreak (16). Those findings indirectly support the conclusions of our study. Two other COVID-19 outbreaks involving vertically aligned flats also occurred in Hong Kong. In the first case, in Heng Tai House at Fu Heng Estate (18), a 59-year-old man in flat 13 on the 34th floor was probably infected by 2 persons with confirmed COVID-19 living in flat 13 on the 32nd floor. In the second outbreak, in Luk Chuen House at Lek Yuen Estate (19), 4 flats in which the residents were infected—710, 810, 1012, and 1112 on the seventh, eighth, 10th, and 11th floors, respectively—were linked to the index patient's flat—812 on the eighth floor—by interconnected vertical drainage pipes; this case involved 6 patients with secondary infection. However, in all these outbreaks, including the one studied here, we do not have direct evidence for the presence of virus-laden bioaerosol of fecal origin in the drainage pipe system, except for the positive surface samples in the bathrooms.
Thus, the COVID-19 outbreak in block X may have been caused by fecal aerosol transmission, on the basis of circumstantial evidence. To prevent such transmission, bioaerosols can be controlled at the source by avoiding any potential gas leaks from the drainage system to indoor spaces. For example, to block fecal aerosol transmission, drainage traps, such as U-shaped water traps, should not be allowed to dry out. Adequate hygiene in sanitary drainage is known to prevent the transmission of diarrheal diseases by the fecal–oral route. Our study also indirectly suggests the importance of bathroom ventilation and hygiene, because toilet flushing may generate fecal aerosols (24). Further studies are warranted to examine the role of fecal aerosols in the spread of SARS-CoV-2.
Supplementary Material
Footnotes
This article was published at Annals.org on 1 September 2020
* Min Kang, Yuguo Li, Jianfeng He, Jianjian Wei, Jun Yuan and Nanshan Zhong contributed equally to this article.
References
- 1. World Health Organization. Infection prevention and control during health care when novel coronavirus (nCoV) infection is suspected. Accessed at www.who.int/publications/i/item/infection-prevention-and-control-during-health-care-when-novel-coronavirus-(ncov)-infection-is-suspected-20200125 on 11 August 2020.
- 2. National Health Commission. New Coronavirus Pneumonia Prevention and Control Plan. 5th ed. Accessed at www.nhc.gov.cn on 27 February 2020.
- 3. Centers for Disease Control and Prevention. How 2019-nCoV Spreads. Accessed at www.cdc.gov/coronavirus/2019-ncov/about/transmission.html on 3 May 2020.
- 4. Chan JF, Yuan S, Kok KH, et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster. Lancet. 2020;395:514-523. [PMID: 31986261] doi:10.1016/S0140-6736(20)30154-9 [DOI] [PMC free article] [PubMed]
- 5. Phan LT, Nguyen TV, Luong QC, et al. Importation and human-to-human transmission of a novel coronavirus in Vietnam [Letter]. N Engl J Med. 2020;382:872-874. [PMID: 31991079] doi:10.1056/NEJMc2001272 [DOI] [PMC free article] [PubMed]
- 6. Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med. 2020;382:1199-1207. [PMID: 31995857] doi:10.1056/NEJMoa2001316 [DOI] [PMC free article] [PubMed]
- 7. Holshue ML, DeBolt C, Lindquist S, et al; Washington State 2019-nCoV Case Investigation Team. First case of 2019 novel coronavirus in the United States. N Engl J Med. 2020;382:929-936. [PMID: 32004427] doi:10.1056/NEJMoa2001191 [DOI] [PMC free article] [PubMed]
- 8. Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020. [PMID: 32031570] doi:10.1001/jama.2020.1585 [DOI] [PMC free article] [PubMed]
- 9. Yong Z, Cao C, Zhu S et al. Isolation of 2019-nCoV from a stool specimen of a laboratory-confirmed case of the coronavirus disease 2019 (COVID-19). China CDC Weekly 2020;2(8):123-4. [PMC free article] [PubMed]
- 10. Zhang H, Kang ZJ, Gong HY et al. Digestive system is a potential route of COVID-19: an analysis of single-cell coexpression pattern of key proteins in viral entry process. Gut 2020;69:1010-1018. doi:10.1136/gutjnl-2020-320953
- 11. Tian Y, Rong L, Nian W, et al. Review article: gastrointestinal features in COVID-19 and the possibility of faecal transmission. Aliment Pharmacol Ther. 2020;51:843-851. [PMID: 32222988] doi:10.1111/apt.1573111 [DOI] [PMC free article] [PubMed]
- 12. Zhang W, Du RH, Li B, et al. Molecular and serological investigation of 2019-nCoV infected patients: implication of multiple shedding routes. Emerg Microbes Infect. 2020;9:386-389. [PMID: 32065057] doi:10.1080/22221751.2020.1729071 [DOI] [PMC free article] [PubMed]
- 13. Ong SWX, Tan YK, Chia PY, et al. Air, surface environmental, and personal protective equipment contamination by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) from a symptomatic patient. JAMA. 2020. [PMID: 32129805] doi:10.1001/jama.2020.3227 [DOI] [PMC free article] [PubMed]
- 14. Liu Y, Ning Z, Chen Y, et al. Aerodynamic analysis of SARS-CoV-2 in two Wuhan hospitals. Nature. 2020;582:557-560. [PMID: 32340022] doi:10.1038/s41586-020-2271-3 [DOI] [PubMed]
- 15. McDermott CV, Alicic RZ, Harden N, et al. Put a lid on it: are faecal bio-aerosols a route of transmission for SARS-CoV-2? J Hosp Infect. 2020. [PMID: 32315667] doi:10.1016/j.jhin.2020.04.024 [DOI] [PMC free article] [PubMed]
- 16. Li Y, Qian H, Yu ITS, Wong TW. Probable roles of bio-aerosol dispersion in the SARS outbreak in Amoy Gardens, Hong Kong. In: Sleigh AC, Leng CH, Yeoh BSA, et al, eds. Population Dynamics and Infectious Diseases in Asia. World Scientific; 2007.
- 17. Yu IT, Li Y, Wong TW, et al. Evidence of airborne transmission of the severe acute respiratory syndrome virus. N Engl J Med. 2004;350:1731-9. [PMID: 15102999] [DOI] [PubMed]
- 18. Leung K, Leung C, Ho-him C. Coronavirus: at least 10 households evacuated from Hong Kong public housing block in Tai Po over multiple infections. Accessed at www.scmp.com/news/hong-kong/health-environment/article/3075228/coronavirus-another-public-housing-estate-hong on 15 April 2020.
- 19. Tsang D, Ho-him C. Coronavirus: Hongkonger living in public housing at centre of infection cluster confirmed as infected. Accessed at https://www.scmp.com/news/hong-kong/health-environment/article/3088925/coronavirus-man-living-hong-kong-public-housing on 11 July 2020.
- 20. Bivolarova M, Ondrácek J, Melikov A, et al. A comparison between tracer gas and aerosol particles distribution indoors: the impact of ventilation rate, interaction of airflows, and presence of objects. Indoor Air. 2017;27:1201-1212. [PMID: 28378912] doi:10.1111/ina.12388 [DOI] [PubMed]
- 21. Peiris JS, Chu CM, Cheng VC, et al; HKU/UCH SARS Study Group. Clinical progression and viral load in a community outbreak of coronavirus-associated SARS pneumonia: a prospective study. Lancet. 2003;361:1767-72. [PMID: 12781535] [DOI] [PMC free article] [PubMed]
- 22. Li Y, Delsante A, Symons J. Prediction of natural ventilation in buildings with large openings. Building and Environment 2000;35:191-206. doi:10.1016/S0360-1323(99)00011-6
- 23. Lei H, Li Y, Xiao S, et al. Routes of transmission of influenza A H1N1, SARS CoV, and norovirus in air cabin: comparative analyses. Indoor Air. 2018;28:394-403. [PMID: 29244221] doi:10.1111/ina.12445 [DOI] [PMC free article] [PubMed]
- 24. Gerba CP, Wallis C, Melnick JL. Microbiological hazards of household toilets: droplet production and the fate of residual organisms. Appl Microbiol. 1975;30:229-37. [PMID: 169732] [DOI] [PMC free article] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.