

Supplemental Digital Content is Available in the Text.
Latinx-Americans showed greater temporal summation, adversity, and adversity correlates relative to non-Hispanic Whites. Discrimination and lifespan social status change inversely related to summation for Latinx-Americans.
Keywords: Temporal summation, Ethnic differences, Latinx, Ethnic discrimination, Adverse life experiences, Pain
Abstract
Introduction:
Adverse life experiences disproportionately impact Latinx-Americans and are related to greater chronic pain rates. However, little is known about how adversities interact with central pain mechanisms for the development of later pain among Latinx-Americans.
Objectives:
The current study examined the relationship between adverse life experiences (eg, trauma and ethnic discrimination) and correlates (eg, social status) with mechanical temporal summation of pain (a proxy measure of central sensitization) between pain-free U.S. native Latinx (n = 65) and non-Hispanic White (NHW) (n = 51) adults.
Methods:
Participants completed self-report adverse life experience and correlational measures regarding childhood and adulthood and a mechanical temporal summation protocol.
Results:
Relative to NHWs, Latinx-Americans reported experiencing significantly greater trauma, discrimination, and lower social status during childhood and adulthood, along with greater temporal summation. Contrary to hypotheses, recent and lifetime experiences of ethnic discrimination significantly correlated with less temporal summation among Latinx-Americans. Decreases in objective and subjective social status across the lifespan (childhood to present day) correlated with greater temporal summation for Latinx-Americans. However, r-to-z transformation analyses confirmed that significant adversity and social status correlations observed among the Latinx group did not significantly differ from NHW participants.
Conclusions:
The present findings highlight the complex association between adverse experiences, adverse experience risk factors, and pain for Latinx-Americans. Given the disproportion of experienced pain and adversity among Latinx-Americans, the current findings suggest that a better understanding of the unique adversities for this sample may help elucidate the mechanisms underlying the relationship between adversities, adversity correlates, and pain risk for Latinx-Americans.
1. Introduction
Latinx-Americans—Americans of Latin-American origin or descent—disproportionately experience disparities for many health conditions,16,37,59 including pain.10,15,17,29,31,35,58,62,68 Disrupted endogenous pain mechanisms, such as enhanced central sensitization, underlie greater risk for chronic pain. Central sensitization is a phenomenon characterized by an amplification of neural signaling within the central nervous system that elicits pain hypersensitivity.5,7,64,65,77,84,88,89 A noninvasive proxy measure of central sensitization in humans is temporal summation of pain, a progressive increase in pain intensity ratings to repetitive noxious stimuli.27 Temporal summation of pain is heightened in individuals with chronic pain,65,78 providing a potential mechanism underlying the risk for clinical pain development and persistence. Other people of color, such as African Americans with clinical pain (ie, acute and chronic pain) show enhanced temporal summation relative to non-Hispanic White (NHW) counterparts.20,38,70 Pain-free African Americans show enhanced summation relative to NHWs,13,55 suggesting that the risk for greater pain severity may manifest before clinical pain development. If heightened temporal summation occurs in the current study among pain-free Latinx-Americans relative to NHWs, this may suggest that amplified central pain processing could be crucial to explaining the greater chronic pain severity seen in Latinx-Americans with clinical pain relative to NHWs.10,15,31,35,58,62,68 However, the psychosocial factors that may act on endogenous pain summation mechanisms to contribute to pain disparities are relatively unknown.
One psychosocial factor that may drive enhanced central sensitization is exposure to adverse life experiences. Many studies find that exposure to traumatic events (eg, physical, sexual, and emotional)—an adverse life experience—are related to pain development9,42,43,74,79,82 and exacerbation.3,90–93 Moreover, studies find greater adversity and trauma positively predict enhanced central sensitization markers.90,91,93 Considering Latinx-Americans disproportionately experience childhood trauma relative to NHWs,50,72 traumatic experiences may relate not only with the greater pain observed among Latinx-Americans,10,15,17,29,31,35,58,62,68 but also with enhanced central sensitization markers that underlie greater risk for chronic pain.
Latinx-Americans also experience unique, pervasive adverse life experiences that may relate with pain disparities, such as racial/ethnic discrimination.14,39,86 Ethnic discrimination among Latinx-Americans in the United States is a common phenomenon: 62% of U.S.-born Latinx-Americans report experiencing discrimination or being mistreated because of their ethnicity.47 Latinx-Americans not only experience discrimination more than NHWs, they likewise appraise it as more stressful.49 Studies show that perceived racial/ethnic discrimination predicts greater clinical pain severity and laboratory pain sensitivity for African Americans.14,25,54,86 Perceived racial discrimination likewise predicts greater laboratory pain sensitivity for African Americans but not NHWs.39 Moreover, 2 recent studies find that discrimination predicts greater clinical pain severity among Latinx-Americans.6,23 Taken together, these studies implicate perceived racial/ethnic discrimination as a risk factor for greater central sensitization and clinical pain experiences in minoritized people of color. However, the relationship between ethnic discrimination and temporal summation of pain in Latinx-Americans remains unexplored.
A correlate of adverse life experiences related to Latinx-American pain disparities that likewise warrants attention is social status. Social status is the relative rank an individual holds in a social hierarchy. Low social status relates to poorer physical health,1,2,21,94 including for Latinx-Americans.34,36,73 For pain, objective8,28,30,32,40,44,48,57,62,81 and subjective social status markers87 relate with greater chronic pain rates and severity, along with worse pain outcomes.8,28,30,44,57,62,81 Poverty status likewise inversely correlates with temporal summation among middle-to-older aged adults with knee osteoarthritis.38 Although an earlier study found that the Latinx-American subgroup with the lowest social status was at the greatest risk for reporting chronic abdominal pain,53 the relationship between social status and temporal summation of pain in Latinx-Americans is unknown. The relationship between social status and temporal summation may help explain clinical pain disparities for demographic groups who disproportionately fall into lower socioeconomic strata, such as Latinx-Americans.33,62
This study therefore examined ethnic differences in temporal summation among pain-free Latinx-American and NHW Americans. The study also examined the relationship between adverse experiences and temporal summation between these 2 groups to examine whether adverse experiences correlate with temporal pain summation. We predicted Latinx-Americans would report greater levels of trauma and ethnic discrimination along with lower social status relative to NHWs. Moreover, we also hypothesized that Latinx-Americans would show heightened temporal summation compared to NHWs. Finally, we hypothesized that trauma, discrimination, and social status would correlate with temporal summation across ethnicities, but particularly among Latinx-Americans.
2. Methods
The institutional review board at Texas A&M University approved this study. All participants provided informed consent and participated between January 2018 and May 2019.
2.1. Participants
Participants self-reported their ethnicity as either “non-Hispanic White” or “Hispanic/Latino.” To control for nativity/migration status, only participants reporting being born and raised in the United States were invited.46 To establish if enhanced sensitization occurs before the clinical pain onset, pain-free undergraduate students between the ages of 18 and 40 without chronic health conditions completed the study. Participants stemmed from a psychology course and received course credit for their participation. To control for other confounds beyond the study's objectives that could affect laboratory pain sensitivity, exclusionary criteria included: (1) current use of any prescription drugs (except for hormonal contraceptives), (2) history of fainting spells, (3) any skin condition/numbness on the hands or forearms, (4) history of neurological disorders, (5) current chronic pain or health condition, and (6) use of allergy or pain medication within 24 hours before the experiment.
2.2. Sample size calculation
Based on findings from a meta-analysis examining racial and ethnic differences in experimental pain sensitivity, an a priori power analysis determined the sample size required per ethnicity to reveal significant differences in pain sensitivity.45 In estimating with a medium effect (f = 0.25), 80% power, α = 0.05, with 2 groups and 2 pain measurements (ie, average 180 g, average 300 g) for a between-factors effect, the required sample size is 98 total.
2.3. General overview of procedures
The current study derived data from a larger study examining Latinx-American laboratory pain and emotion sensitivity comprising 134 participants. However, only 116 participants completed temporal summation procedures due to early study terminations from exclusionary criteria, withdrawal, time constraints, or technical difficulties. The approximately 4-hour parent study occurred during a single session within a temperature-controlled, sound-attenuated room. Participants were prescreened for inclusion/exclusion criteria before being invited to the laboratory, and again on the day of testing. If eligible, participants then filled out several questionnaires to assess background characteristics. After being affixed with psychophysiological leads, participants completed emotional and physical (eg, mechanical and thermal) processing tasks. Each task occurred with at least a 2-minute enforced rest between tasks to reduce carryover effects. Before the Mechanical Temporal Summation Task, participants completed 2 heat sensory tests on the contralateral, nondominant side of their body.
A single experimenter with approximately 8 years' experience administering laboratory pain tests (Rassu) conducted the study. Participants were alone in the experiment room while answering questionnaires to minimize observer effects.
2.4. Measures
2.4.1. Trauma
The Early Traumatic Inventory Self-Report (ETISR) assessed traumatic life events before 18 years of age. The ETISR is a 27-item questionnaire that summed responses to assess traumatic life events in 4 domains (general, physical, emotional, and sexual trauma), along with disturbance and dissociative symptoms in response to the most distressing event.11
2.4.2. Ethnic discrimination
The General Ethnic Discrimination Scale (GEDS) assessed appraised stress severity (“not at all stressful” to “extremely stressful”) and frequency (“never” to “almost all the time”) of 17 perceived discriminatory events (eg, How often have you been treated unfairly by strangers because of your race/ethnic group?) during the past 2 years (recent) and their entire life (lifetime).49 Evidence suggests scales modeled the perceived ethnic discrimination construct equally well across racial/ethnic groups, including Latinx-Americans.49
2.4.3. Social status
We assessed both objective (ie, parental education level and family household income) and subjective social status. In some instances, subjective social status is a unique21 and better2,76 health status predictor relative to objective status. The current study classified social status as childhood and present day. The U.S. version of the MacArthur Scale of Subjective Social Status was used to measure subjective social status.1 To measure childhood subjective social status, participants recorded their parent's social status during childhood (ie, 0–12 years old) relative to the greater U.S. on an illustrated nine-step ladder in which the top rung represents those with the most education, money, and respected jobs (highest status), whereas the bottom rung of the ladder represents those with the least education, money, and respected jobs (lowest status). Participants likewise recorded their own personal, present day subjective social status using the same measure. Evidence suggests that subjective social status significantly correlates with objective indicators of socioeconomic status such as education history, income, and employment status.2 Furthermore, subjective social status ladders have been used in several studies with ethnically diverse participants, including Latinx-Americans.61,95
We also calculated change in objective (Δ Objective Social Status = present family household income minus childhood family household income) and subjective social status across the lifespan (Δ Subject Social Status = present personal subjective social status minus childhood parental social status), with more positive values indicating greater increases in social status across the lifespan. Change in social status across the lifespan represents a shift from one level of social status to another within a given social hierarchy.71 Comparing participants' social status with their parents is a common method for determining social mobility, or change in social status across the lifespan.41,48,52,75
2.5. Mechanical temporal summation procedure
A Mechanical Temporal Summation Task assessed summation of pain ratings to a presented series of mechanical stimuli (Fig. 1). Temporal summation refers to increased perceived pain from either C- or Aδ-fiber stimulation by repetitive, constant-intensity, noxious stimuli delivered at frequencies greater than 0.33 Hz.63 Using 180 and 300 g calibrated nylon monofilaments designed to deliver a consistent gram force upon the filament's bend, participants were assessed on 3 locations across the participants' dominant side: the dorsal surface of the third digit's intermediate phalanx, the dorsal surface of the second digit's metacarpal, and the upper trapezius muscle (for details, see Fig. 1). Given the high intercorrelation across the temporal summation indices, total temporal summation was then calculated by subtracting average initial pain intensity ratings across the 3 sites from average peak pain intensity ratings across the same sites.12,13,38 The order of testing across the 3 anatomical sites were randomized per individual. Before pain assessment, participants completed pain rating training until confident with their own ability.
Figure 1.
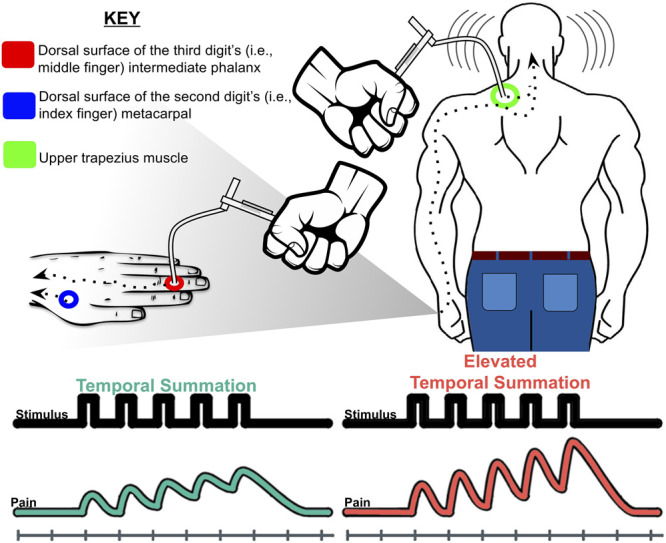
Mechanical temporal summation of pain procedure described in the current study. Participants were first assessed for initial pain after receiving a single contact and verbally rating the intensity of the pain from the single contact on a scale ranging from 0 (“no pain”) to 100 (“the most intense pain imaginable”). Participants then received a series of 10 additional contacts at a rate of one contact per second at the same body site. Upon completing 10 contacts, participants rated the peak or greatest pain intensity experienced during the 10 contacts. This single and 10 contact procedures occurred twice on each anatomical site for both the 180 and 300 g monofilaments. Temporal summation at each site was first calculated by averaging the initial and peak pain responses across the 2 trials at each site then subtracting pain intensity ratings of the single contact from the peak pain intensity.
2.6. Potential covariates
The current study focused on the relationship between adversities, adversity correlates, and temporal summation of pain. However, negative mood is likely related to adversities, adversity correlates, and pain. To ensure there were no confounding effects, we included sex, depression, and perceived stress as potential covariates. The Center for Epidemiological Studies Depression 20-item assessed depressive symptoms within the previous week.67 Higher Center for Epidemiological Studies Depression scores indicate more severe depressive symptomology, with a 20 cutoff score reflecting an adequate tradeoff between sensitivity and specificity for clinical depression risk.85 The Perceived Stress Scale 10-item assessed perceived stress within the previous 2 weeks.19 Although the Perceived Stress Scale is not a diagnostic instrument, thus absent of cutoff scores, higher scores indicate greater perceived stress. However, controlling for the 3 variables did not change the effect size, direction, or significance of relationships between temporal summation of pain and either the adversity or adversity correlate variables.
2.7. Data analysis
When values were missing because of lack of response or equipment malfunction, pairwise deletion was used to exclude participants from those particular analyses.4 Differences in continuous variables were examined with t or F tests, whereas categorical data used χ2 analyses. Significance was set at α < 0.05 (2-tailed). Partial eta squared () was the effect size metric for F tests, with 0.009, 0.0588, and 0.1379 corresponding to small, medium, and large effect sizes, respectively.18,69 Phi φ and Cramer's V were used as a measures of effect size for χ2. Cohen's d was the effect size metric for t tests.18 SPSS 23.0 (IBM, Armonk, NY) was used for all analyses.
2.7.1. Primary analyses
A series of one-way analyses of variance and χ2 analyses were used to examine ethnic differences between adversities and adversity correlates. To determine whether temporal summation occurred at each site for the 180 and 300 g filaments, we used paired t tests to compare the average pain rating after a single contact to the average maximal pain rating after 10 contacts, collapsed across ethnicity. Then, a two-way ethnicity (between: NHW, Latinx) X total body temporal summation across monofilament weights (within: 180, 300 g) repeated-measures analysis of variance evaluated ethnic differences in temporal summation (average total body peak pain minus average initial total body pain difference scores). Because transformations could not correct normality violations, nonparametric Spearman correlations analyzed the relationships between demographics, self-report measures, and total body average temporal summation of pain, separated by ethnicity groups. We then compared significant correlation coefficients for temporal summation across ethnicities using r-to-z transformations.
3. Results
3.1. Background characteristics
Table 1 displays adversities and adversity correlate comparisons between Latinx-Americans and NHWs. Participants did not differ in sex, age, depressive symptoms, or perceived stress. Latinx-Americans reported greater frequency and stress appraisal of lifetime and recent ethnic discrimination. Latinx-Americans also reported greater experiences of total trauma and trauma symptoms, along with greater emotional and sexual traumatic experiences. Several participants across ethnicities reported not knowing their current or childhood family income (Table 1). Latinx-Americans reported lower household income at both time periods, along with lower parental education and childhood subjective social status relative to NHWs. There was no ethnic difference in current subjective social status. Finally, Latinx-Americans reported greater increases in subjective social status from childhood to present day relative to NHWs, suggesting subjective social status grew to a greater degree over the lifespan for Latinx-Americans. However, there was no difference for change in objective social status (ie, household family income) from childhood to present day between ethnicity groups.
Table 1.
Background characteristics by ethnicity.
| Continuous | Non-Hispanic White | Latinx-American | F | P | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Cronbach α | N | Mean | SD | Cronbach α | N | Mean | SD | ||||
| Demographic | |||||||||||
| Age | 51 | 19.12 | 0.13 | 65 | 18.86 | 0.11 | 2.30 | 0.132 | 0.020 | ||
| Mood | |||||||||||
| Depressive symptoms (CES-D; 0–60) | 0.87 | 51 | 13.98 | 8.70 | 0.85 | 65 | 15.37 | 8.23 | 0.77 | 0.381 | 0.007 |
| Perceived stress (PSS; 0–40) | 0.85 | 51 | 17.96 | 5.86 | 0.87 | 65 | 18.34 | 6.75 | 0.10 | 0.752 | 0.001 |
| Trauma frequency (ETISR) | |||||||||||
| Total (0–27)* | 0.71 | 51 | 5.41 | 3.37 | 0.83 | 64 | 7.19 | 4.81 | 4.99 | 0.027 | 0.042 |
| General (0–11) | 0.57 | 51 | 2.33 | 1.85 | 0.51 | 64 | 2.70 | 1.89 | 1.11 | 0.295 | 0.010 |
| Physical (0–5) | 0.78 | 51 | 2.08 | 1.70 | 0.77 | 64 | 2.23 | 1.71 | 0.24 | 0.626 | 0.002 |
| Emotional (0–5)* | 0.77 | 51 | 0.82 | 1.31 | 0.85 | 64 | 1.58 | 1.80 | 6.32 | 0.013 | 0.053 |
| Sexual (0–6)* | 0.68 | 51 | 0.18 | 0.59 | 0.82 | 64 | 0.67 | 1.36 | 5.90 | 0.017 | 0.050 |
| Ethnic discrimination (GEDS) | |||||||||||
| Lifetime (17–102)‡ | 0.89 | 51 | 22.39 | 5.75 | 0.93 | 65 | 29.23 | 11.60 | 14.84 | <0.001 | 0.115 |
| Recent (17–102)‡ | 0.83 | 51 | 21.41 | 4.84 | 0.90 | 65 | 26.97 | 9.64 | 14.13 | <0.001 | 0.110 |
| Appraisal (17–102)‡ | 0.91 | 51 | 20.57 | 8.44 | 0.95 | 65 | 32.65 | 17.87 | 19.81 | <0.001 | 0.148 |
| Categorical | Non-Hispanic White | Latinx-American | χ2 | P | φ, Cramer's V | ||
|---|---|---|---|---|---|---|---|
| N | Median or % | N | Median or % | ||||
| Demographic | |||||||
| Gender (female) | 51 | 45% | 65 | 63% | 3.74 | 0.053 | 0.179 |
| Mood | |||||||
| Depressive symptoms >20 (CES-D; clinical depression) | 51 | 27% | 65 | 32% | 0.32 | 0.572 | 0.053 |
| Trauma symptoms (ETISR) | |||||||
| Disturbance (yes)* | 51 | 27% | 64 | 45% | 3.87 | 0.049 | 0.183 |
| Dissociative (yes)* | 51 | 12% | 64 | 27% | 3.88 | 0.049 | 0.184 |
| Objective social status | |||||||
| Current household income (1–9)‡ | 43 | 9 | 60 | 7 | 32.61 | <0.001 | 0.563 |
| Childhood household income (1–9)† | 41 | 9 | 55 | 7 | 25.24 | 0.001 | 0.513 |
| Father's education (1–9)† | 51 | 7 | 64 | 5 | 27.12 | 0.001 | 0.486 |
| Mother's education (1–9)‡ | 51 | 7 | 64 | 6 | 31.31 | <0.001 | 0.522 |
| Δ objective social status (−8 to 8) | 41 | 0 | 52 | 0 | 9.46 | 0.396 | 0.319 |
| Subjective social status | |||||||
| Current subjective social status, U.S. (1–9) | 51 | 6 | 64 | 5 | 12.95 | 0.073 | 0.336 |
| Childhood subjective social status, U.S. (1–9)‡ | 51 | 6 | 64 | 4 | 32.72 | <0.001 | 0.533 |
| Δ subjective social status (−8 to 8)* | 51 | −1 | 64 | 0 | 19.37 | 0.022 | 0.410 |
Income coded 1 = less than $5,000, 2 = $5,000 through $11,999, 3 = $12,000 through $15,999, 4 = $16,000 through $24,999, 5 = $25,000 through $34,999, 6 = $35,000 through $49,9997 = $50,000 through $74,999, 8 = $75,000 through $99,999, 9 = $100,000 and greater; Parent's Education Coded 1 = elementary school or less, 2 = middle school, 3 = some high school, 4 = high school graduate/GED equivalent, 5 = postsecondary school other than college, 6 = some college, 7 = college graduate, 8 = some graduate school, 9 = graduate degree.
P < 0.05.
P < 0.01.
P < 0.001.
CES-D, The Center for Epidemiological Studies-Depression; ETISR, Early Traumatic Inventory Self-Report; GEDS, General Ethnic Discrimination Scale; PSS, Perceived Stress Scale.
3.2. Temporal summation phenomenon
Collapsed across ethnicity groups, average pain intensity ratings after the 10th contact was significantly greater than average pain intensity ratings after the first contact at the phalanx, metacarpal, and trapezius for both the 180 and 300 g von Frey monofilaments (P's < 0.001, Cohen's d's ≥ 1.085), indicating temporal summation across sites and stimulus intensities.
3.3. Ethnic differences in temporal summation
Figure 2 depicts temporal pain summation between Latinx-Americans and NHWs for the 180 and 300 g weights when averaged across the 3 body testing sites. Analyses revealed significant main effects of monofilament weight, F1,114 = 21.29, P < 0.001, = 0.157, and ethnicity, F1,114 = 4.49, P = 0.036, = 0.038, but no weight × ethnicity interaction (P = 0.404, = 0.006).
Figure 2.
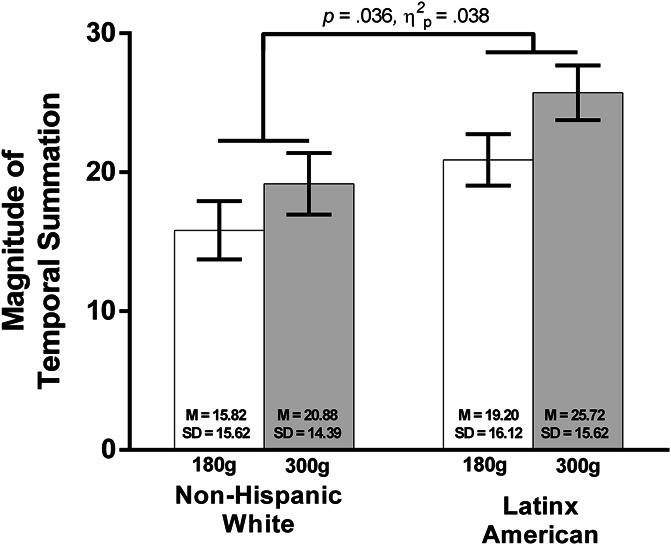
Comparison of differences for mechanical temporal summation to the 180 and 300 g von Frey by ethnicity. Collapsed across body sites and ethnicity, greater summation was demonstrated at 300 g relative to 180 g. Moreover, collapsed across body sites and monofilament weights, Latinx-Americans displayed greater temporal summation relative to NHWs. Mean ± SEM. MNHW180 g = 15.82, SDNHW180 g = 15.62; MLatinx180 g = 20.88, SDLatinx180 g = 14.39; MNHW300 g = 19.20, SDNHW300 g = 16.12; MLatinx300 g = 25.72, SDLatinx300 g = 15.62. NHW, non-Hispanic White.
3.4. Correlations between adversity and mechanical temporal summation
Temporal summation of mechanical pain significantly correlated across the 3 anatomical sites (metacarpal, phalanx, and trapezius) and 2 filament weights (180 and 300 g) (r ≥ 0.56, P < 0.001). Therefore, temporal summation of mechanical pain was averaged across the 3 sites to create an average total mechanical temporal summation of pain that was used in subsequent correlation analyses.
Table 2 displays correlations separated by ethnicity. A complete set of correlation matrices separated by ethnicity are included in Supplemental Tables 1 and 2 (available at http://links.lww.com/PR9/A73 and http://links.lww.com/PR9/A74). The trauma subscale, composite, and symptom scores were not significantly associated with temporal summation for either ethnicity group. Recent and lifetime experiences of ethnic discrimination were both inversely associated with mechanical temporal summation, but only for Latinx-Americans. However, there were no significant differences between the discrimination–temporal summation correlations across ethnicities (Table 3).
Table 2.
Ethnicity correlations comparisons between temporal summation demographics, mood, trauma, discrimination, and social status.
| Variables | Ethnicity | |
|---|---|---|
| Non-Hispanic White | Latinx-American | |
| Demographic | ||
| Gender | 0.06 | −0.03 |
| Mood | ||
| Depressive symptoms (CESD) | 0.10 | −0.01 |
| Perceived stress (PSS) | −0.08 | 0.05 |
| Trauma | ||
| Trauma total (ETISR) | −0.09 | −0.17 |
| Trauma general (ETISR) | 0.00 | −0.05 |
| Trauma physical (ETISR) | −0.11 | −0.06 |
| Trauma emotional (ETISR) | −0.16 | −0.17 |
| Trauma sexual (ETISR) | 0.15 | −0.14 |
| Trauma—disturbance symptoms (ETISR) | 0.04 | −0.24 |
| Trauma—dissociative symptoms (ETISR) | −0.01 | 0.07 |
| Discrimination | ||
| Ethnic discrimination—recent (GEDS) | −0.14 | −0.32† |
| Ethnic discrimination—lifetime (GEDS) | −0.24 | −0.34† |
| Ethnic discrimination—appraisal (GEDS) | −0.11 | −0.22 |
| Objective social status | ||
| Father's education | 0.03 | 0.22 |
| Mother's education | −0.03 | 0.22 |
| Household income—current | −0.22 | 0.02 |
| Household income—childhood | 0.09 | 0.10 |
| Δ objective social status | −0.22 | −0.39† |
| Subjective social status | ||
| Subjective social status—current | 0.07 | −0.03 |
| Subjective social status—childhood | 0.23 | 0.23 |
| Δ subjective social status | −0.15 | −0.30* |
Gender coded 0 = women, 1 = men; income coded 1 = less than $5,000, 2 = $5,000 through $11,999, 3 = $12,000 through $15,999, 4 = $16,000 through $24,999, 5 = $25,000 through $34,999, 6 = $35,000 through $49,9997 = $50,000 through $74,999, 8 = $75,000 through $99,999, 9 = $100,000 and greater; Father and Mother Education Coded 1 = elementary school or less, 2 = middle school, 3 = some high school, 4 = high school graduate/GED equivalent, 5 = postsecondary school other than college, 6 = some college, 7 = college graduate, 8 = some graduate school, 9 = gaduate degree; CES-D = Center for Epidemiological Studies Depression Scale; ETISR, Early Traumatic Inventory Self-Report; GEDS = General Ethnic Discrimination Scale; PSS = Perceived Stress Scale; Δ objective social status = current household income − childhood household income; Δ subjective social status = current subjective social status − childhood subjective social status.
P < .05.
P < .01.
Table 3.
Difference between correlation coefficients across ethnicity.
| Non-Hispanic White | Latinx-American | z | P | |||||
|---|---|---|---|---|---|---|---|---|
| N | r | P | N | r | P | |||
| Ethnic discrimination (GEDS) | ||||||||
| Recent | 51 | −0.138 | 0.333 | 65 | −0.322 | 0.009 | −0.99 | 0.322 |
| Lifetime | 51 | −0.237 | 0.094 | 65 | −0.338 | 0.006 | 0.57 | 0.569 |
| Social status | ||||||||
| Δ objective social status | 41 | −0.22 | 0.167 | 52 | −0.394 | 0.004 | 0.89 | 0.374 |
| Δ subjective social status | 51 | −0.152 | 0.287 | 64 | −0.298 | 0.017 | 0.80 | 0.424 |
None of the cross-sectional childhood or present-day markers of objective social status or subjective social status were significantly associated with mechanical temporal summation for Latinx-Americans or NHWs. Changes in objective (ie, family household income) and subjective social status across the lifespan were significantly and inversely associated with mechanical temporal summation for Latinx-Americans, but not for NHWs. However, there were no significant differences between Δ social status–temporal summation correlations across ethnicities (Table 3).
4. Discussion
The current study found that Latinx-Americans reported experiencing significantly greater trauma, greater discrimination, and lower social status. Latinx-Americans likewise experienced significantly greater temporal summation. Finally, increased recent and lifetime experiences of ethnic discrimination, along with upward changes in objective and subjective social status across the lifespan, significantly correlated with decreased temporal summation for Latinx-Americans (Table 2). However, there were no significant differences between the correlation coefficients for Latinx and NHWs (Table 3).
Greater temporal summation for Latinx-Americans seen in the current study is consistent with a recent study examining laboratory pain sensitivity in a large combined cohort of participants identifying as either healthy or having temporomandibular disorder across ethnicity groups.60 Considering evidence supporting the clinical relevance of dynamic laboratory pain sensitivity measures,24,26,38,83 greater summation may represent a potential pain risk factor for Latinx-Americans.
4.1. The relationship between ethnicity, adversities, adversity correlates, and mechanical temporal summation of pain
Consistent with prior literature,72 Latinx-Americans in the current study reported greater trauma experiences relative to NHWs. Trauma experiences did not significantly correlate with greater temporal summation for either ethnic group. Contrary to the current study's hypotheses, greater recent and lifetime ethnic discrimination experiences significantly correlated with lower temporal summation for Latinx-Americans. The negative relationship between discrimination responses and temporal summation, however, was comparable to the NHW group.
The current findings differ from previous studies that observe that greater childhood adversity and ethnic discrimination associated significantly with enhanced central sensitization markers.54,90,91,93 It is conceivable that the differences in patterns between the studies may be due to differences in the samples studied. For example, although some previous studies examining childhood trauma and central sensitization markers also sampled pain-free young adults within a university setting, such studies actively recruited samples stratified on childhood adversity, consisting predominantly of NHWs.90,91,93 Regarding racial discrimination, earlier laboratory studies focused only on discrimination and pain sensitivity among African Americans and associations with central sensitization markers have been inconsistent. For example, a significantly positive relationship between discrimination and temporal summation occurred in one study consisting primarily of African Americans with chronic pain from the community,54 but another study observed no significant relationship for pain-free African Americans.12 Even beyond laboratory pain testing studies, recent evidence suggests that perceived ethnic discrimination correlates significantly with greater clinical pain intensity (r = 0.21) and pain disability (r = 0.27) among Latinx individuals recruited from a government-subsidized community-based outpatient clinic.6 However, Bakhshaie et al.'s (2019) study composed largely of non-U.S.-native participants (88.4%) who predominantly spoke Spanish as their first language (96.6%) and earned less than $14,999 per year (55.9%),6 a contrast to the U.S.-native Latinx-Americans from higher household incomes assessed in the current study (Table 1). The stated hypotheses in the current study regarding the relationship between trauma and discrimination was derived from the aforementioned laboratory pain testing studies that assessed either a different ethnicity group (African Americans), a different trauma group (ie, stratified high vs low trauma), or a different setting (ie, community population). Although African Americans and Latinx-Americans are both minoritized people of color, there are fundamental differences between the 2 populations including generational trauma experiences and discrimination (eg, history of slavery and current political climate around U.S. immigration). Recent work would also suggest that heterogeneity within a minoritized population can also contribute to differences in clinical pain outcomes.6 However, considering expected Latinx-American growth over decades in the United States, along with the unique histories and current sociopolitical realities experienced by Latinx-Americans and their subgroups (eg, Mexican, Central-American, South-American), it is important to evaluate the specific contexts (eg, regions, study settings, and socioeconomic status), cultures (eg, values, beliefs, histories, and nativity), and adversities (eg, trauma and discrimination) that may contribute to their pain experiences. Specifically, future studies must resist simple extrapolation from other groups.
Of the status markers, neither objective nor subjective social status indices during childhood or present day significantly related to temporal summation across groups. This finding differs from prior work describing significant relationships between social status and physical pain8,28,30,32,40,44,48,57,62,66,81,87 and temporal summation.38 Instead, downward changes in objective (ie, family household income decreased over time) and subjective social status (ie, subjective social status decreased over time) across the lifespan—such that individuals reported a decrease in status since childhood—significantly correlated with greater temporal summation for Latinx-Americans. However, there were no significant differences between ethnicity groups for either correlation coefficient. The relationship between downward social status across the lifespan and pain in the current study is consistent with prior work demonstrating significant relationships with downward objective social status across the lifespan and low back pain in adulthood.48,52 The current study extends the literature by demonstrating that both downward objective and subjective social status across the lifespan correlates with enhanced temporal summation, a central sensitization proxy. In line with social causation hypotheses,22 downward social status may put individuals at future risk for chronic pain by promoting central sensitization, whereas maintained or increased status may reduce risk. Given evidence suggesting pain conditions, such as chronic back pain, relate with greater temporal summation,56,80 the current findings may offer insight into the relationship between social status across the lifespan, central sensitization, and chronic pain risk.
4.2. Limitations
The current study possesses limitations for consideration. First, this study used cross-sectional data with correlations, limiting causal interpretations and suggesting the need for future longitudinal research.
Second, this study tested pain-free individuals to examine whether ethnicity and adverse experiences related to endogenous pain processing phenomenon that could contribute to chronic pain risk. Although temporal summation is greater in individuals with clinical pain,65,78 enhanced temporal summation of pain also occurs in nonclinical populations,13,55 suggesting that the risk for greater pain severity may manifest before clinical pain development. However, although studying a pain-free sample allows for examining group differences and relationships while ruling out the influence of disease status, it also limits the ability to know whether the findings generalize to Latinx-Americans experiencing clinical pain.
Third, university samples limit the current study to presumably more resilient, high-functioning individuals of greater socioeconomic status who may have experienced less traumatic and discriminatory events and had greater resources to cope. Although the sample consists of U.S. natives, excluding any first-generation immigrants who may experience greater adversities, demographic research suggests 27% to 47% of second-and-higher generation Latinx-Americans have experienced recent maltreatment because of their ethnicity.51 Nevertheless, considering consistent relationships between pain, trauma,3,9,42,43,74,79,82,90,91,92–93 and socioeconomic status,8,28,30,32,40,44,48,57,62,81,87 the current study's makeup may too restricted to observe intersectional interactions between ethnicity, adversity, and temporal summation. Thus, future replication of the current study among more diverse community and nonnative samples with lower socioeconomic status is warranted.
Fourth, a male, African-American experimenter conducted all laboratory procedures. His demographics could have affected participants' responses even with efforts to minimize observer bias.
Fifth, the current study's ETISR measure did not assess trauma past 18 years of age. Childhood trauma was of primary interest, given Latinx-Americans disproportionately experience childhood trauma relative to NHWs.50,72 Therefore, future studies should evaluate lifetime trauma experiences.
Finally, although we randomized laboratory task order before temporal summation testing, equated the same procedures before the temporal summation task across participants, and enforced rests between tasks, participants in the current study completed several tasks. Carryover effects are possible, potentially moderating the current results. Therefore, the current study warrants replication.
4.3. Conclusions
The current study is the first to observe greater mechanical temporal summation of pain among completely pain-free Latinx-Americans relative to NHWs. Although Latinx-Americans in the current study also reported greater adversities and adversity correlates, counter to hypotheses and earlier work among African Americans, greater recent and lifetime experiences of ethnic discrimination associated with less temporal summation, suggesting that different mechanisms may underlie the relationship between discrimination and pain for Latinx-Americans and African Americans. However, future research will need to inspect discrimination measures more critically to make sure standard self-report measures are equally valid, representative of the most important discrimination events, and predictive of different pain outcomes among unique minoritized demographic groups.
In a novel finding, decreases in objective and subjective social status across the lifespan (from childhood to the present) correlated with greater temporal summation. Dynamic social status measures that reflect change across the lifespan may predict centralized pain risk above solely assessing current or cross-sectional socioeconomic status measures. Future research is needed to explore whether this relationship is not only replicable, but also incrementally predictive for pain risk among community samples.
Taken together, the present findings highlight the complex association between adversities, adversity correlates, and pain. A better understanding of the impact of such experiences for this particularly important, yet understudied, group may help explain the mechanisms underlying the relationship between adversities, adversity correlates, and pain risk for Latinx-Americans.
Disclosures
The authors have no conflicts of interest to declare.
Acknowledgements
The authors thank the participants and research staff involved in the project. F.S. Rassu was supported by funding from Texas A&M University's College of Liberal Arts and the Office of Graduate and Professional Studies. N. Nanavaty was supported by a National Science Foundation Graduate Research Fellowship. The content is solely the responsibility of the authors and does not necessarily reflect the views of the National Science Foundation. Preliminary parts of this research have been presented at the American Psychological Association's 2019 Convention.
Footnotes
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Supplemental digital content is available for this article. Direct URL citations appear in the printed text and are provided in the HTML and PDF versions of this article on the journal's Web site (www.painrpts.com).
Appendix A. Supplemental digital content
Supplemental digital content associated with this article can be found online at http://links.lww.com/PR9/A73 and http://links.lww.com/PR9/A74.
References
- [1].Adler NE. Health disparities through a psychological lens. Am Psychol 2009;64:663–73. [DOI] [PubMed] [Google Scholar]
- [2].Adler NE, Epel E, Castellazzo G, Ickovics J. Relationship of subjective and objective social status with psychological and physical health in healthy white women. Heal Psychol 2000;19:586–92. [DOI] [PubMed] [Google Scholar]
- [3].Affleck G, Tennen H, Urrows S, Higgins P. Person and contextual features of daily stress reactivity: individual differences in relations of undesirable daily events with mood disturbance and chronic pain intensity. J Pers Soc Psychol 1994;66:329–40. [DOI] [PubMed] [Google Scholar]
- [4].Allison PD. Missing data. 1st ed Thousand Oaks, CA: SAGE Publications, 2002. [Google Scholar]
- [5].Arendt-Nielsen L, Graven-Nielsen T. Central sensitization fibromyalgia and other musculoskeletal disorders. Curr Pain Headache Rep 2003;7:355–61. [DOI] [PubMed] [Google Scholar]
- [6].Bakhshaie J, Rogers AH, Mayorga NA, Ditre J, Rodríguez-Cano R, Ruiz AC, Viana AG, Garza M, Lemaire C, Ochoa-Perez M, Bogiaizian D, Zvolensky MJ. Perceived racial discrimination and pain intensity/disability among economically disadvantaged latinos in a federally qualified health center: the role of anxiety sensitivity. J Immigr Minor Heal 2019;21:21–9. [DOI] [PubMed] [Google Scholar]
- [7].Bendtsen L. Central sensitization in tension-type headache—possible pathophysiological mechanisms. Cephalalgia 2000;20:486–508. [DOI] [PubMed] [Google Scholar]
- [8].Blyth FM, March LM, Brnabic AJM, Jorm LR, Williamson M, Cousins MJ. Chronic pain in Australia: a prevalence study. PAIN 2001;89:127–34. [DOI] [PubMed] [Google Scholar]
- [9].Boisset‐Pioro MH, Esdaile JM, Fitzcharles MA. Sexual and physical abuse in women with fibromyalgia syndrome. Arthritis Rheum 1995;38:235–41. [DOI] [PubMed] [Google Scholar]
- [10].Bolen J, Schieb L, Jm H, Cg H, Theis K, Lb M. Differences in the prevalence and impact of arthritis among racial/ethnic groups in the US. Natl Heal Interview Surv Prev Chronic Dis 2010;7:A64. [PMC free article] [PubMed] [Google Scholar]
- [11].Bremner JD, Bolus R, Mayer EA. Psychometric properties of the early trauma inventory—self report. J Nerv Ment Dis 2007;195:211–18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Bulls HW, Goodin BR, McNew M, Gossett EW, Bradley LA. Minority aging and endogenous pain facilitatory processes. Pain Med 2016;17:1037–48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Bulls HW, Lynch MK, Petrov ME, Gossett EW, Owens MA, Terry SC, Wesson-Sides KM, Goodin BR. Depressive symptoms and sleep efficiency sequentially mediate racial differences in temporal summation of mechanical pain. Ann Behav Med 2017;51:673–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Burgess DJ, Grill J, Noorbaloochi S, Griffin JM, Ricards J, Van Ryn M, Partin MR. The effect of perceived racial discrimination on bodily pain among older African American men. Pain Med 2009;10:1341–52. [DOI] [PubMed] [Google Scholar]
- [15].Carey TS, Freburger JK, Holmes GM, Jackman A, Knauer S, Wallace A, Darter J. Race, care seeking, and utilization for chronic back and neck pain: population perspectives. J Pain 2010;11:343–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [16].Chen J, Vargas-Bustamante A, Mortensen K, Ortega AN. Racial and ethnic disparities in health care access and utilization under the affordable care act. Med Care 2016;54:140–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Cintron A, Morrison RS. Pain and ethnicity in the United States: a systematic review. J Palliat Med 2006;9:1454–73. [DOI] [PubMed] [Google Scholar]
- [18].Cohen J. Statistical power analysis for the behavioral sciences, 2nd ed Hillsdale, NJ: Lawrence Erlbaum, 1988. [Google Scholar]
- [19].Cohen S, Williamson G. Perceived stress in a probability sample of the United States. In: Spacapan S, Oskamp S, editors. The social psychology of health: claremont symposium on applied social psychology. Newbury Park: Sage, 1988, Vol. 13 pp. 31–67. [Google Scholar]
- [20].Cruz-Almeida Y, Sibille KT, Goodin BR, Petrov ME, Bartley EJ, Riley JL, III, King CD, Glover TL, Sotolongo A, Herbert MS, Schmidt JK, Fessler BJ, Staud R, Redden D, Bradley LA, Fillingim RB. Racial and ethnic differences in older adults with knee osteoarthritis. Arthritis Rheumatol 2014;66:1800–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Cundiff JM, Matthews KA. Is subjective social status a unique correlate of physical health? A meta-analysis. Heal Psychol 2017;36:1109–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Dahl E. Social mobility and health: cause or effect? Br Med J 1996;313:435–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Dugan SA, Lewis TT, Everson-Rose SA, Jacobs EA, Harlow SD, Janssen I. Chronic discrimination and bodily pain in a multiethnic cohort of midlife women in the Study of Women's Health Across the Nation. PAIN 2017;158:1656–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Edwards RR. Individual differences in endogenous pain modulation as a risk factor for chronic pain. Neurology 2005;65:437–43. [DOI] [PubMed] [Google Scholar]
- [25].Edwards RR. The association of perceived discrimination with low back pain. J Behav Med 2008;31:379–89. [DOI] [PubMed] [Google Scholar]
- [26].Edwards RR, Sarlani E, Wesselmann U, Fillingim RB. Quantitative assessment of experimental pain perception: multiple domains of clinical relevance. PAIN 2005;114:315–9. [DOI] [PubMed] [Google Scholar]
- [27].Eide PK. Wind-up and the NMDA receptor complex from a clinical perspective. Eur J Pain 2000;4:5–15. [DOI] [PubMed] [Google Scholar]
- [28].Elliott AM, Smith BH, Penny KI, Smith WC, Chambers Wa. The epidemiology of chronic pain in the community. Lancet 1999;354:1248–52. [DOI] [PubMed] [Google Scholar]
- [29].Epps CD, Ware LJ, Packard A. Ethnic wait time differences in analgesic administration in the emergency department. Pain manag. Nurs 2008;9:26–32. [DOI] [PubMed] [Google Scholar]
- [30].Eriksen J, Jensen MK, Sjøgren P, Ekholm O, Rasmussen NK. Epidemiology of chronic non-malignant pain in Denmark. PAIN 2003;106:221–8. [DOI] [PubMed] [Google Scholar]
- [31].Faucett J, Gordon N, Levine J. Differences in postoperative pain severity among four ethnic groups. J Pain Symptom Manage 1994;9:383–9. [DOI] [PubMed] [Google Scholar]
- [32].Feldman CH, Dong Y, Katz JN, Donnell-Fink LA, Losina E. Association between socioeconomic status and pain, function and pain catastrophizing at presentation for total knee arthroplasty. BMC Musculoskelet Disord 2015;16:1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Fontenot KR, Semega JL, Kollar MA. Income and poverty in the United States: 2017. Washington, US Census Nureau, 2018. pp. P60–263. [Google Scholar]
- [34].Franzini L, Fernandez-Esquer ME. The association of subjective social status and health in low-income Mexican-origin individuals in Texas. Soc Sci Med 2006;63:788–804. [DOI] [PubMed] [Google Scholar]
- [35].Gagnon CM, Matsuura JT, Smith CC, Stanos SP. Ethnicity and interdisciplinary pain treatment. Pain Pract 2014;14:532–40. [DOI] [PubMed] [Google Scholar]
- [36].Garza JR, Glenn BA, Mistry RS, Ponce NA, Zimmerman FJ. Subjective Social Status and self-reported health among US-born and immigrant latinos. J Immigr Minor Heal 2017;19:108–19. [DOI] [PubMed] [Google Scholar]
- [37].Geiss LS, Wang J, Cheng YJ, Thompson TJ, Barker L, Li Y, Albright AL, Gregg EW. Prevalence and incidence trends for diagnosed diabetes among adults aged 20 to 79 years, United States, 1980-2012. JAMA 2014;312:1218–26. [DOI] [PubMed] [Google Scholar]
- [38].Goodin BR, Bulls HW, Herbert MS, Schmidt J, King CD, Glover TL, Sotolongo A, Sibille KT, Cruz-Almedia Y, Staud R, Fessler BJ, Redden DT, Bradley LA, Fillingim RB, Cruz-Almeida Y, Staud R, Fessler BJ, Redden DT, Bradley LA, Fillingim RB. Temporal summation of pain as a prospective predictor of clinical pain severity in adults aged 45 years and older with knee osteoarthritis: ethnic differences. Psychosom Med 2014;76:302–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [39].Goodin BR, Pham QT, Glover TL, Sotolongo A, King CD, Sibille KT, Herbert MS, Cruz-Almeida Y, Sanden SH, Staud R, Redden DT, Bradley LA, Fillingim RB. Perceived racial discrimination, but not mistrust of medical researchers, predicts the heat pain tolerance of African Americans with symptomatic knee osteoarthritis. Heal Psychol 2013;32:1117–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [40].Goodman SM, Mandl LA, Mehta B, Navarro-Millan I, Russell LA, Parks ML, Dey SA, Crego D, Figgie MP, Nguyen JT, Szymonifka J, Zhang M, Bass AR. Does education level mitigate the effect of poverty on total knee arthroplasty outcomes? Arthritis Care Res 2018;70:884–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [41].Hallqvist J, Lynch J, Bartley M, Lang T, Blane D. Can we disentangle life course processes of accumulation, critical period and social mobility? An analysis of disadvantaged socio-economic positions and myocardial infarction in the Stockholm Heart Epidemiology Program. Soc Sci Med 2004;58:1555–62. [DOI] [PubMed] [Google Scholar]
- [42].Häuser W, Kosseva M, Üceyler N, Klose P, Sommer C. Emotional, physical, and sexual abuse in fibromyalgia syndrome: a systematic review with meta-analysis. Arthritis Care Res 2011;63:808–20. [DOI] [PubMed] [Google Scholar]
- [43].Howard FM. Abuse history and chronic pain in women: I. Prevalences of sexual abuse and physical abuse. Obstet Gynecol 1995;85:158–9. [DOI] [PubMed] [Google Scholar]
- [44].Johannes CB, Le TK, Zhou X, Johnston JA, Dworkin RH. The prevalence of chronic pain in United States adults: results of an internet-based survey. J Pain 2010;11:1230–9. [DOI] [PubMed] [Google Scholar]
- [45].Kim HJ, Yang GS, Greenspan JD, Downton KD, Griffith KA, Renn CL, Johantgen M, Dorsey SG. Racial and ethnic differences in experimental pain sensitivity: systematic review and meta-analysis. PAIN 2017;158:194–211. [DOI] [PubMed] [Google Scholar]
- [46].Krieger N. Methods for the scientific study of discrimination and health: an ecosocial approach. Am J Public Health 2012;102:936–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [47].Krogstad JM, López G. Roughly half of Hispanics have experienced discrimination. Fact Tank News Numbers, 2016. Available at: http://www.pewresearch.org/facttank/2016/06/29/roughly-half-of-hispanics-have-experienced-discrimination/. [Google Scholar]
- [48].Lallukka T, Viikari-Juntura E, Raitakari OT, Kähönen M, Lehtimäki T, Viikari J, Solovieva S. Childhood and adult socio-economic position and social mobility as determinants of low back pain outcomes. Eur J Pain 2014;18:128–38. [DOI] [PubMed] [Google Scholar]
- [49].Landrine H, Klonoff EA, Corral I, Fernandez S, Roesch S. Conceptualizing and measuring ethnic discrimination in health research. J Behav Med 2006;29:79–94. [DOI] [PubMed] [Google Scholar]
- [50].Llabre MM, Schneiderman N, Gallo LC, Arguelles W, Daviglus ML, Gonzalez F, Isasi CR, Perreira KM, Penedo FJ. Childhood trauma and adult risk factors and disease in hispanics/latinos in the US: results from the hispanic community health study/study of latinos (HCHS/SOL) sociocultural ancillary study. Psychosom Med 2017;79:172–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [51].Lopez MH, Gonzales-Barrera A, Krogstad JM. More latinos have serious concerns about their place in America under trump. Pew Res Cent 2018;54. [Google Scholar]
- [52].Lourenço S, Correia S, Alves L, Carnide F, Silva S, Lucas R. Intergenerational educational trajectories and lower back pain in young women and men. Acta Reumatol Port 2017;2017:73–81. [PubMed] [Google Scholar]
- [53].Magni G, Rossi MR, Rigatti-Luchini S, Merskey H. Chronic abdominal pain and depression. Epidemiologie findings in the United States. Hispanic health and nutrition examination survey. PAIN 1992;49:77–85. [DOI] [PubMed] [Google Scholar]
- [54].Mathur VA, Kiley KB, Haywood C, Bediako SM, Lanzkron S, Carroll CP, Buenaver LF, Pejsa M, Edwards RR, Haythornthwaite JA, Campbell CM. Multiple levels of suffering discrimination in health-care settings is associated with enhanced laboratory pain sensitivity in sickle cell disease. Clin J Pain 2016;32:1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [55].Mechlin B, Heymen S, Edwards CL, Girdler SS. Ethnic differences in cardiovascular-somatosensory interactions and in the central processing of noxious stimuli. Psychophysiology 2011;48:762–73. [DOI] [PubMed] [Google Scholar]
- [56].Meints SM, Wang V, Edwards RR. Sex and race differences in pain sensitization among patients with chronic low back pain. J Pain 2018;19:1461–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [57].Moulin DE, Clark AJ, Speechley M, Morely-Foster PK. Chronic pain in Canada - prevalence, treatment, impact and the role of opioid analgesia. Pain Res Manag 2002;7:179–84. [DOI] [PubMed] [Google Scholar]
- [58].Nguyen M, Ugarte C, Fuller I, Haas G, Portenoy RK. Access to care for chronic pain: racial and ethnic differences. J Pain 2005;6:301–14. [DOI] [PubMed] [Google Scholar]
- [59].Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of childhood and adult obesity in the United States, 2011-2012. JAMA 2014;311:806–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [60].Ostrom C, Bair E, Maixner W, Dubner R, Fillingim RB, Ohrbach R, Slade GD, Greenspan JD. Demographic predictors of pain sensitivity: results from the OPPERA study. J Pain 2017;18:295–307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [61].Ostrove JM, Adler NE, Kuppermann M, Washington AE. Objective and subjective assessments of socioeconomic status and their relationship to self-rated health in an ethnically diverse sample of pregnant women. Heal Psychol 2000;19:613–18. [DOI] [PubMed] [Google Scholar]
- [62].Portenoy RK, Ugarte C, Fuller I, Haas G. Population-based survey of pain in the United States: differences among white, African American, and Hispanic subjects. J Pain 2004;5:317–28. [DOI] [PubMed] [Google Scholar]
- [63].Price DD, Hu JW, Dubner R, Gracely RH. Peripheral suppression of first pain and central summation of second pain evoked by noxious heat pulses. PAIN 1977;3:57–68. [DOI] [PubMed] [Google Scholar]
- [64].Price DD, Staud R. Neurobiology of fibromyalgia syndrome. J Rheumatol 2005;32:22–8. [PubMed] [Google Scholar]
- [65].Price DD, Staud R, Robinson ME, Mauderli AP, Cannon R, Vierck CJ. Enhanced temporal summation of second pain and its central modulation in fibromyalgia patients. PAIN 2002;99:49–59. [DOI] [PubMed] [Google Scholar]
- [66].Quiton RL, Leibel DK, Boyd EL, Waldstein SR, Evans MK, Zonderman AB. Sociodemographic patterns of pain in an urban community sample. PAIN 2020;161:1044–51. [DOI] [PubMed] [Google Scholar]
- [67].Radloff L. The CED-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas 1977;1:385–401. [Google Scholar]
- [68].Reyes-Gibby CC, Aday LA, Todd KH, Cleeland CS, Anderson KO. Pain in aging community-dwelling adults in the United States: non-hispanic Whites, non-hispanic blacks, and hispanics. J Pain 2007;8:75–84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [69].Richardson JTE. Eta squared and partial eta squared as measures of effect size in educational research. Educ Res Rev 2011;6:135–47. [Google Scholar]
- [70].Riley JL, Cruz-Almeida Y, Glover TL, King CD, Goodin BR, Sibille KT, Bartley EJ, Herbert MS, Sotolongo A, Fessler BJ, Redden DT, Staud R, Bradley LA, Fillingim RB. Age and race effects on pain sensitivity and modulation among middle-aged and older adults. J Pain 2013;15:272–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [71].Ritterman Weintraub ML, Fernald LCH, Adler N, Bertozzi S, Syme SL. Perceptions of social mobility: development of a new psychosocial indicator associated with adolescent risk behaviors. Front Public Heal 2015;3:1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [72].Roberts AL, Gilman SE, Breslau J, Breslau N, Koenen KC. Race/ethnic differences in exposure to traumatic events, development of post-traumatic stress disorder, and treatment-seeking for post-traumatic stress disorder in the United States. Psychol Med 2011;41:71–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [73].Sanchón-Macias V, Prieto-Salceda D, Bover-Bover A, Gastaldo D. Relationship between subjective social status and perceived health among Latin American immigrant women. Rev Lat Am Enfermagem 2013;21:1353–9. [DOI] [PubMed] [Google Scholar]
- [74].Scott KM. Association of childhood adversities and early-onset mental disorders with adult-onset chronic physical conditions. Arch Gen Psychiatry 2011;68:838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [75].Simons AMW, Groffen DAI, Bosma H. Socio-economic inequalities in all-cause mortality in Europe: an exploration of the role of heightened social mobility. Eur J Public Health 2013;23:1010–12. [DOI] [PubMed] [Google Scholar]
- [76].Singh-Manoux A, Marmot MG, Adler NE. Does subjective social status predict health and change in health status better than objective status? Psychosom Med 2005;67:855–61. [DOI] [PubMed] [Google Scholar]
- [77].Staud R, Robinson ME, Price DD. Temporal summation of second pain and its maintenance are useful for characterizing widespread central sensitization of fibromyalgia patients. J Pain 2007;8:893–901. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [78].Staud R, Vierck CJ, Cannon RL, Mauderli AP, Price DD. Abnormal sensitization and temporal summation of second pain (wind-up) in patients with fibromyalgia syndrome. PAIN 2001;91:165–75. [DOI] [PubMed] [Google Scholar]
- [79].Stickley A, Koyanagi A, Kawakami N. Childhood adversities and adult-onset chronic pain: results from the world mental health survey, Japan. Eur J Pain 2015;19:1418–27. [DOI] [PubMed] [Google Scholar]
- [80].Tesarz J, Wolfgang E, Treede RD, Gerhardt A. Altered pressure pain thresholds and increased wind-up in adult chronic back pain patients with a history of childhood maltreatment. PAIN 2016;157:1. [DOI] [PubMed] [Google Scholar]
- [81].Thompson KA, Terry EL, Sibille KT, Gossett EW, Ross EN, Bartley EJ, Glover TL, Vaughn IA, Cardoso JS, Sotolongo A, Staud R, Hughes LB, Edberg JC, Redden DT, Bradley LA, Fillingim RB, Goodin BR. At the intersection of ethnicity/race and poverty: knee pain and physical function. J Racial Ethn Heal Disparities 2019;6:1131–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [82].Tietjen GE, Brandes JL, Peterlin BL, Eloff A, Dafer RM, Stein MR, Drexler E, Martin VT, Hutchinson S, Aurora SK, Recober A, Herial NA, Utley C, White L, Khuder SA. Childhood maltreatment and migraine (part II): emotional abuse as a risk factor for headache chronification. Headache 2010;50:32–41. [DOI] [PubMed] [Google Scholar]
- [83].Treede R. The role of quantitative sensory testing in the prediction of chronic pain. PAIN 2019;160:s66–9. [DOI] [PubMed] [Google Scholar]
- [84].Verne GN, Price DD. Irritable bowel syndrome as a common precipitant of central sensitization. Curr Rheumatol Rep 2002;4:322–8. [DOI] [PubMed] [Google Scholar]
- [85].Vilagut G, Forero CG, Barbaglia G, Alonso J. Screening for depression in the general population with the center for epidemiologic studies depression (CES-D): a systematic review with meta-analysis. PLoS One 2016;11:1–17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [86].Walker Taylor JL, Campbell CM, Thorpe RJ, Whitfield KE, Nkimbeng M, Szanton SL. Pain, racial discrimination, and depressive symptoms among African American women. Pain Manag Nurs 2018;19:79–87. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [87].Woo J, Leung J, Lau E. Prevalence and correlates of musculoskeletal pain in Chinese elderly and the impact on 4-year physical function and quality of life. Public Health 2009;123:549–56. [DOI] [PubMed] [Google Scholar]
- [88].Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain. PAIN 2011;152:S2–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [89].Woolf CJ. Evidence for a central component of post-injury pain hypersensitivity. Nature 1983;306:686. [DOI] [PubMed] [Google Scholar]
- [90].You DS, Albu S, Linsenbardt H, Meagher MW. Cumulative childhood adversity as a risk factor for common chronic pain conditions in young adults. Pain Med 2018;20:486–94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [91].You DS, Creech SK, Meagher MW. Enhanced area of secondary hyperalgesia in women with multiple stressful life events: a pilot study. Pain Med 2016;17:1859–64. [DOI] [PubMed] [Google Scholar]
- [92].You DS, Meagher MW. Childhood adversity and pain facilitation. Psychosom Med 2018;80:869–79. [DOI] [PubMed] [Google Scholar]
- [93].You DS, Meagher MW. Childhood adversity and pain sensitization. Psychosom Med 2016;78:1084–93. [DOI] [PubMed] [Google Scholar]
- [94].Zell E, Strickhouser JE, Krizan Z. Subjective social status and health: a meta-analysis of community and society ladders. Heal Psychol 2018;37:979–87. [DOI] [PubMed] [Google Scholar]
- [95].Zvolensky MJ, Bakhshaie J, Garza M, Valdivieso J, Ortiz M, Bogiaizian D, Robles Z, Vujanovic A. Anxiety sensitivity and subjective social status in relation to anxiety and depressive symptoms and disorders among Latinos in primary care. J Anxiety Disord 2015;32:38–45. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental digital content associated with this article can be found online at http://links.lww.com/PR9/A73 and http://links.lww.com/PR9/A74.