

Abstract
The Xen Gel Stent lowers intraocular pressure by shunting aqueous humor to the subconjunctival space. While published studies include both open conjunctiva and closed conjunctiva approaches, most publications feature a closed conjunctiva, ab interno approach. While this approach is widely used, other approaches may be preferred for some patients. This paper provides details on surgical steps and tips for enhancing outcomes for an open conjunctiva technique for the implantation of the Xen Gel Stent, as well as reasoning as to when this approach should be used.
Electronic supplementary material
The online version of this article (10.1007/s12325-020-01278-1) contains supplementary material, which is available to authorized users.
Keywords: Glaucoma, Glaucoma surgery, Ophthalmology, Surgical technique, XEN Gel Stent
Key Summary Points
| The XEN Gel Stent lowers intraocular pressure by shunting aqueous humor to the subconjunctival space. |
| Published studies include both open conjunctiva and closed conjunctiva approaches to implantation. |
| While the popularity of micro-invasive glaucoma surgery has favored the adaption of a closed conjunctiva approach, some surgeons have found great benefit in an open conjunctiva approach. |
| This paper provides details on surgical steps of an open conjunctiva implantation of the gel stent and tips for enhancing outcomes. |
Introduction
The Xen Gel Stent (Allergan) is a surgical implant designed to lower intraocular pressure (IOP) via the creation of a subconjunctival filtration pathway for aqueous humor. The device’s length (6 mm) and luminal diameter (45 μm) provide sufficient resistance to help control outflow and prevent hypotony in the early postoperative period. Multiple studies have shown that the device has an excellent safety profile and comparable efficacy to trabeculectomy and other subconjunctival drainage devices [1, 2].
Grover and colleagues reported 12-month efficacy and safety results in eyes with refractory glaucoma implanting the Xen via an ab interno approach, after opening and dissecting the conjunctiva to apply sponges soaked with mitomycin C (MMC) (0.2 mg/ml for 2 min) [1]. In contrast, the majority of published studies report a Xen implantation method without conjunctival dissection and an ab interno approach [3–5]. However, many glaucoma surgeons find that there remains a benefit to an open conjunctiva approach both for implantation and revision, as it may allow for better and more consistent results in patients where a closed conjunctiva approach may not be ideal due to ocular tissue or anatomical considerations.
Since the Xen Gel Stent was launched in 2017, one fortuitous feature has been the ability to adapt the surgical implantation procedure to the demands of the individual patient. The authors of this paper are Xen experts who continue to implant the stent by opening the conjunctiva and then using either an ab interno or an ab externo approach to place it. Table 1 provides a brief comparison of the two surgical techniques, their advantages and their disadvantages. This paper will provide details on their surgical steps for this approach, as well as tips for enhancing outcomes. This article does not contain any studies with human participants or animals performed by any of the authors.
Table 1.
Comparison of Xen implantation techniques
| Ab interno open conjunctiva | Ab externo open conjunctiva | |
|---|---|---|
| Technique |
1. Corneal traction suture is optional 2. Conjunctival peritomy and dissection are performed 3. Main and side port incisions (clear cornea) are made—AC is filled with cohesive OVD 4. The injector is inserted through he main incision, across anterior chamber towards the target area. 5. The needle enters the trabecular meshwork and is advanced through the sclera exiting 2 mm posterior to limbus using countertraction. 6. The stent is deployed and adjusted as needed. 7. Flow is confirmed after removing OVD and priming the bleb 8. Tenon’s layer and conjunctiva are sutured closed |
1. Corneal traction suture may be placed in the superior cornea 2. Conjunctival peritomy and dissection are performed 3. Side port is optional—only needed if using OVD 4. The injector is placed in sclera 2–2.5 mm from the limbus; using the traction suture for countertraction 5. The needle is advanced through sclera until visible in AC 6. The stent is deployed and adjusted as needed 7. Flow of aqueous is confirmed by visualizing beading at the distal end of the stent 8. Tenon’s layer and conjunctiva are sutured closed |
| Advantages |
1. Better control of placement of stent in the angle 2. Can be easily combined with phacoemulsification |
1. Expands the targeted area of implantation to the supero-temporal quadrant 2. Can be performed without corneal incisions or viscoelastic use 3. Easiest transition for glaucoma surgeons 4. Safer in phakic eyes |
| Disadvantages |
1. Requires maneuvers in the AC 2. Can be challenging in eyes with corneal opacification |
1. Entry into AC cannot be performed under gonioscopic guidance |
Advantages of An Open Conjunctiva, Ab Interno Placement
Two benefits to the open conjunctiva approach are the ability to work with patients with conjunctival scarring and the ability to better control placement of the stent.
In a closed conjunctiva approach, the Xen Gel Stent applicator needle needs to be positioned just beneath the conjunctiva for optimal implant placement. This requires a healthy and mobile conjunctiva to be tented up for delivery of the implant in the subconjunctival space, and usually means that patients who have conjunctival scarring in the target area (from previous incisional glaucoma surgery) should be excluded to avoid perforation. With an open conjunctiva approach, an area of scarring can be easily avoided.
In addition, the open conjunctiva approach allows the surgeon to dissect or move the Tenon’s capsule away, choose the exact location for placement, and then easily make small adjustments. The microstent can be pulled out or pushed further into the anterior chamber to ensure that the it is positioned properly in the anterior chamber and sub-Tenon’s space.
Ensuring ideal positioning of the distal end of the stent by placing it beneath Tenon’s layer and conjunctiva can improve the predictability of results, as well as create a more diffuse and posteriorly directed bleb. Placing the device beneath the Tenon’s layer can also help prevent the device erosion through the conjunctiva. In the pivotal study by Grover and colleagues [1], no erosions were seen with the open conjunctiva approach.
Open Conjunctiva, Ab Interno Placement Technique
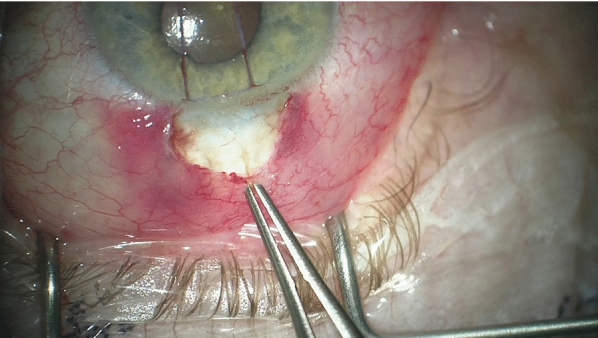
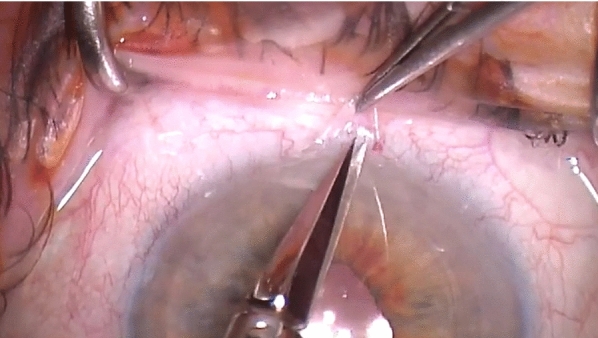
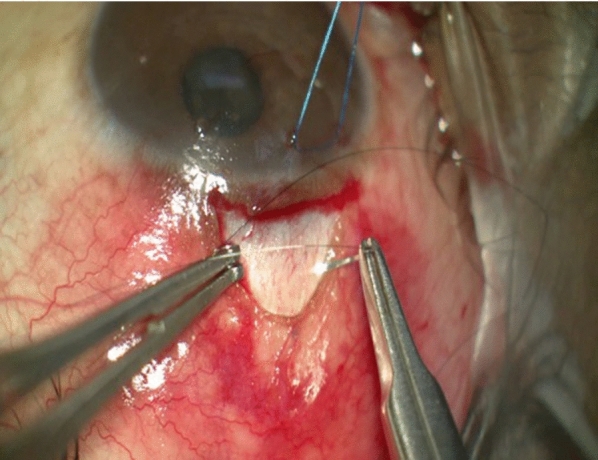
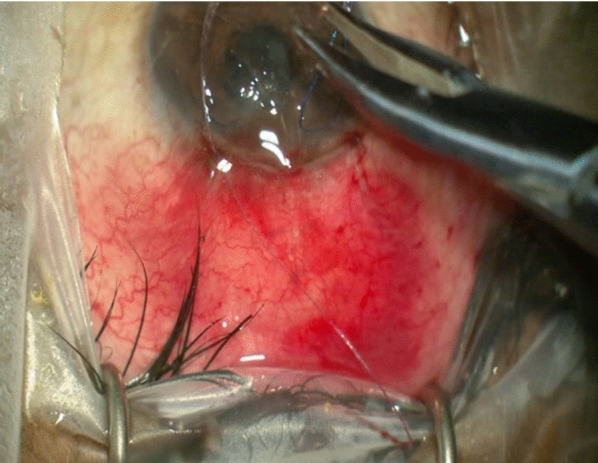
Some authors (JP) prefer to start the procedure with a retrobulbar block so that the patient remains comfortable and still during the procedure, but the procedure can also be carried out under topical anesthesia, sub-conjunctiva, or sub-Tenon’s injection of Lidocaine (with epinephrine). A corneal traction suture can be placed to help rotate the eye downward (Fig. 1). A 3- to 4-mm superior conjunctival peritomy is made at the 12 o’clock position to create a conjunctival flap (fornix-based) (Fig. 2). Vannas scissors (Sklars) can be used to make a small opening in the conjunctiva; dissection is continued posteriorly until Tenon’s is incised at the point of insertion. A good-sized pocket is dissected with blunt Westcott scissors (Fig. 3), and cautery is used as needed to control any bleeding.
Fig. 1.
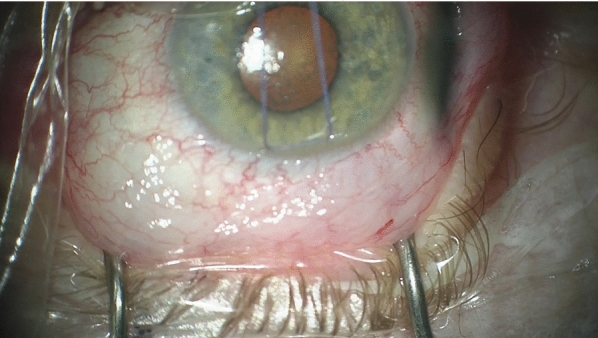
Corneal traction suture place for counter traction
(image courtesy of Joseph F. Panarelli, MD)
Fig. 2.
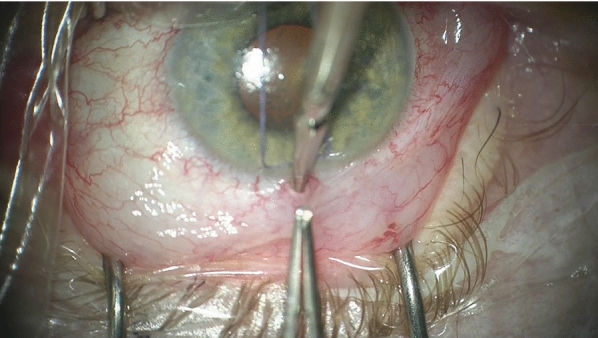
Conjunctival peritomy at 12 o’clock with Vannas scissors
(image courtesy of Joseph F. Panarelli, MD)
Fig. 3.
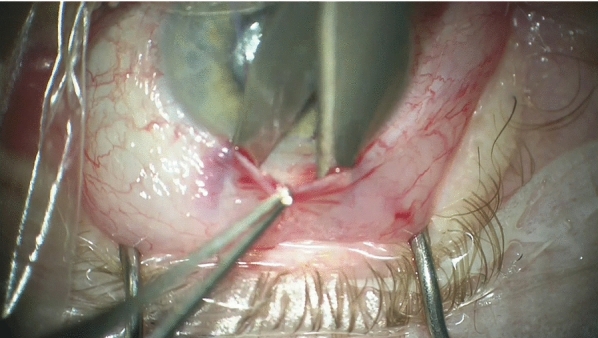
Blunt dissection to ensure good size pocket
(image courtesy of Joseph F. Panarelli, MD)
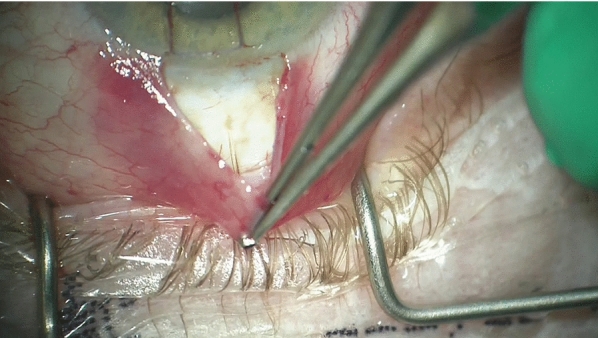
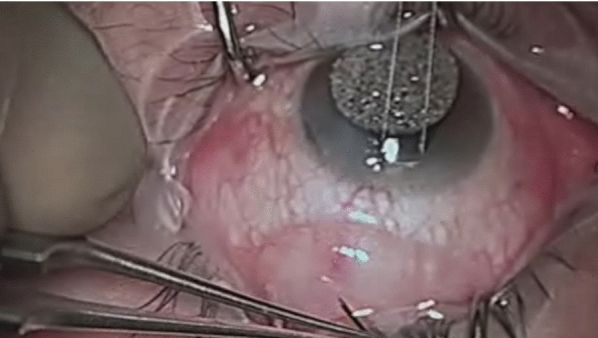
Once the dissection is complete, a paracentesis, as well as a 2-mm clear, corneal wound are made, and the anterior chamber is filled with a cohesive viscoelastic. The needle of the injector is inserted through the main incision and advanced across the anterior chamber toward the targeted quadrant and into the angle. The needle enters the trabecular meshwork and is pushed through the sclera, exiting 2 mm posterior to the limbus with the needle’s beveled tip oriented upward. A second instrument (cyclodialysis spatula, Vera hook, etc.) can be inserted into the paracentesis to help stabilize the eye during this step. After the needle exits the sclera, any torsion or counterforce should be released to assume a natural position of the eye prior to delivering the stent, which is then deployed by moving forward the blue slider of the injector. An ideally implanted stent should be visible 2–3 mm outside the sclera with 1 mm in the anterior chamber. Stent position in the angle can be verified with a gonioscopy lens. The open peritomy and direct visualization of the external tip of the Xen Gel Stent (Fig. 4) allow the surgeon to easily make micro-adjustments. Tying forceps can be used to pull the stent out or push it into the anterior chamber to ensure that it is properly positioned (Fig. 5).
Fig. 4.
Direct visualization of the stent during deployment
(image courtesy of Joseph F. Panarelli, MD)
Fig. 5.
Tying forceps used make micro-adjustments of the implant, ensuring 1-2-3 placement
(image courtesy of Joseph F. Panarelli, MD)
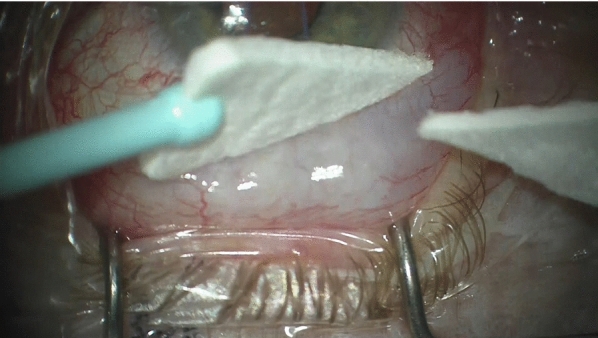
The next step is to check for flow through the stent. After the viscoelastic has been removed from the anterior chamber, a Weck-cel (BVI Medical) can be used to touch the distal end of the device to make sure there is some slow percolation of fluid (Fig. 6).
Fig. 6.
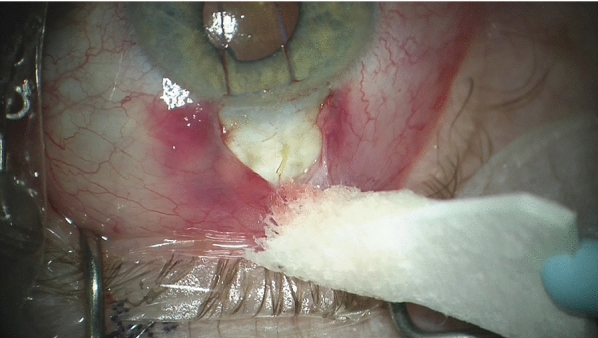
Direct outflow check through the stent
(image courtesy of Joseph F. Panarelli, MD)
If no fluid is detected, the device can be primed by back-flushing the device with balanced salt solution (BSS) in a 25-gauge cannula. The conjunctiva and Tenon’s layers are then brought up over the device (Fig. 7) and closed in a watertight fashion (Fig. 8). This can be carried out with two winged sutures, or a short running closure on one side, along with two horizontal mattress stitches to close the limbal incision. The corneal incisions should be hydrated with BSS and a bleb should form (priming the bleb). A Seidel test can be performed to ensure there is no conjunctival or corneal incision leakage.
Fig. 7.
Conjunctiva and Tenon brought over the implant for closure
(image courtesy of Joseph F. Panarelli, MD)
Fig. 8.
Conjunctival closure
(image courtesy of Brian Francis, MD)
Patients can be injected with a bolus of corticosteroid at the completion of the case followed by topical corticosteroids at home. Patients are typically kept on steroids four times a day for 1 month, two times a day for the second month, and then tapered over the third month.
Ensuring ideal positioning of the distal end of the Xen Gel Stent beneath Tenon’s layer has resulted in more predictable surgical outcomes for the authors and less need for post-operative manipulation such as needling. Blebs also tend to be more diffuse and posteriorly directed.
Open Conjunctiva Xen implantation via (post phaco) ab interno placement (MP4 82185 kb)
Advantages of An Open Conjunctiva, Ab Externo Placement
There are unique benefits to an ab externo placement of the Xen Gel Stent, which have led many surgeons to include this technique to their surgical armamentarium. The first benefit is to expand the targeted area of implantation. When the stent is placed ab interno, it is typically left in the superonasal quadrant as it is difficult to pivot the injector in the main incision and move further temporal. An ab externo approach provides easy accessibility to the entire superior quadrant. The ab externo technique is especially advantageous in patients who have had previous trabeculectomy in the superior or superonasal areas, as the Xen Gel Stent can be placed much further from pre-existing scar tissue than with an ab interno approach.
A second benefit to an ab externo approach is that it avoids maneuvers inside the anterior chamber and obviates the need for corneal incisions and the use of viscoelastic. Absence of maneuvers inside the anterior chamber may eliminate reported and potential complications, such as corneal wound leaks, retained viscoelastic and consequent IOP spikes, lens or endothelial cell touch, among others [1]. In phakic eyes, the ab externo approach essentially eliminates the risk of inadvertent damage to the lens capsule. This benefit is especially important in phakic patients with significant lens rise and a shallow chamber where concomitant phacoemulsification may not be indicated.
Third, the ab externo technique may be the easiest transition technique for glaucoma surgeons new to the use of the Xen Gel Stent, as it most closely utilizes existing surgical skills and does not involve any new angle-surgery skills. Opening and closing of the conjunctiva is similar to trabeculectomy, and the insertion technique with the Xen injector needle is very similar to the creation of a needle track for the insertion of tube shunts.
Finally, as mentioned above, the open conjunctiva approach allows the surgeon to dissect or move the Tenon’s capsule away and to easily make micro-adjustments of the stent by grasping it directly. The stent can be pulled out or pushed further into the anterior chamber to ensure that it is positioned properly.
Open Conjunctiva, Ab Externo Placement Technique
A 7.0 Vicryl (polyglactin 910; Johnson & Johnson Vision) traction suture may be placed in the superior cornea to rotate the eye looking down. A peritomy (around 2 mm for RC and 1 clock hour for DY), ideally at 12 o’clock, followed by a blunt dissection to break the adhesions between the conjunctiva and the Tenon’s at the limbus, is more than sufficient to allow for delivery of the device (Fig. 9).
Fig. 9.
An approximately 2-mm peritomy is created, and Vanass scissors are used to open the conjunctiva
(image courtesy of Randy Craven, MD)
As with trabeculectomy, the vessels can be cauterized, if desired. Next, a Tenon’s incision is made to enter sub-Tenon’s space and expose the bare sclera (Fig. 10).
Fig. 10.
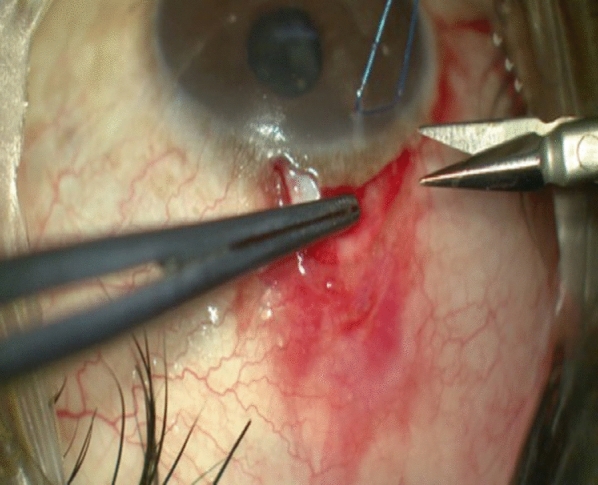
Tenon’s incision is made at the limbus to enter the sub-Tenon’s space and expose the bare sclera
(Image courtesy of David Yan, MD)
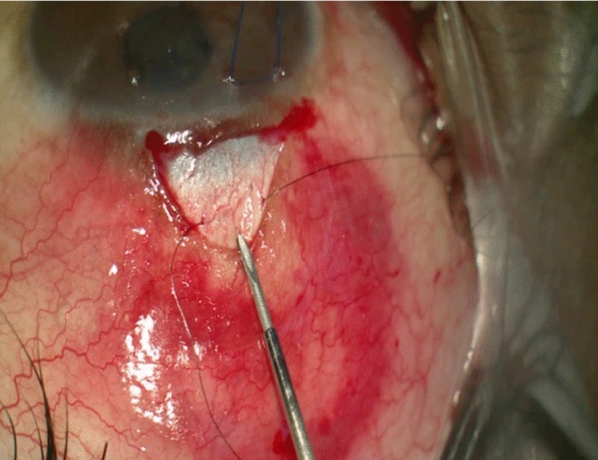
An optional tenectomy can be performed in cases of significant Tenon’s thickening due to race, inflammation, scarring from previous surgery or other risk factors (Fig. 11). Performing a limited tenectomy may decrease the risk of stent obstruction/early failure. However, this may potentially lead to a higher risk of erosion through the conjunctiva. The Xen injector is then placed bevel up in the sclera, 2.0–2.5 mm from the limbus (Fig. 12); the original traction suture can be released and used for counter traction as the applicator needle is advanced through the sclera.
Fig. 11.
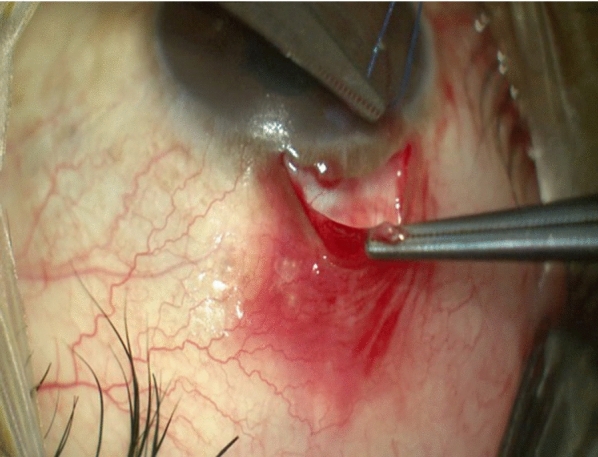
Tenectomy may be performed in cases of significant Tenon’s presence
(image courtesy of David Yan, MD)
Fig. 12.
Enter the eye 2–2.5 mm from the limbus
(image courtesy of Randy Craven, MD)
Advance the needle superficially until the tip is at the surgical limbus. The needle is then tilted downwards by about 30° and advanced until it enters the anterior chamber. The most common problems encountered during the delivery process are amputation of the stent or pulling the stent back out of the anterior chamber due to the tendency of the needle to flick upwards. These can be avoided by rotating the injector needle 90° or beveling down prior to deploying the stent and ensuring there is no upwards or side pressure on the injector. One option to avoid any issues when deploying the stent is to pull the injector back slightly (the sleeve of the injector should be about 1 mm from the scleral needle entry point) prior to pushing the blue slider forward. There is no need for forward pressure for the needle to stay in place within the scleral tunnel unlike with an ab interno delivery approach.
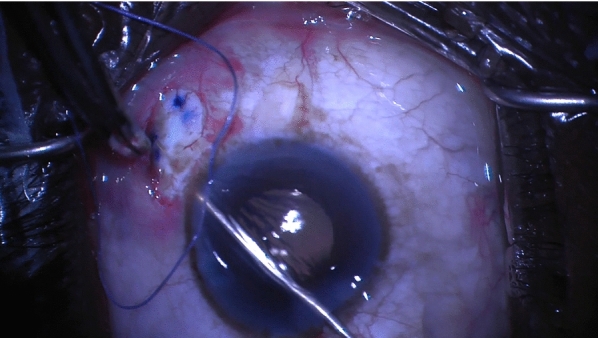
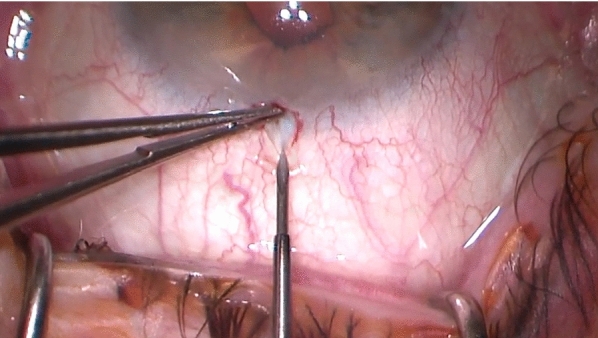
Once the stent is fully released, the flow of aqueous can be confirmed. As this technique does not create an entry into the anterior chamber, the anterior chamber remains very stable without the use of viscoelastic. At this point, a slow but steady flow of aqueous through the device can usually be visible. If no flow is seen, it is often due to peri-tubular flow. One of the authors (D.Y.) uses a pre-placed 10.0 nylon encircling suture (before the injector enters the sclera) approximately 1 mm posterior to the limbus to reduce peri-tubular filtration and the risk of early hypotony (Fig. 13). The Xen injector is then placed bevel up 1 mm posterior to the pre-placed scleral suture (Fig. 14). Beading of aqueous will frequently start as soon as an encircling suture is tied (Fig. 15) in these cases.
Fig. 13.
A 10.0 nylon encircling suture is pre-placed ~ 1.0 mm posterior to the limbus to reduce peri-tubular filtration
(image courtesy of David Yan, MD)
Fig. 14.
Injector is then placed bevel up ~ 1 mm posterior to the pre-placed scleral suture
(image courtesy of David Yan, MD)
Fig. 15.
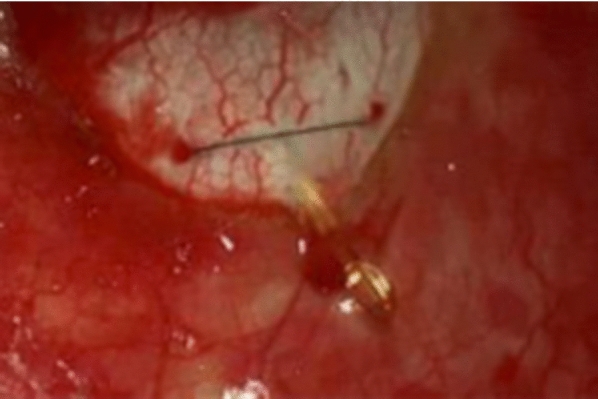
Note beading of aqueous at distal end of the Xen Gel Stent after 10.0 nylon suture has been tied tight
(image courtesy of David Yan, MD)
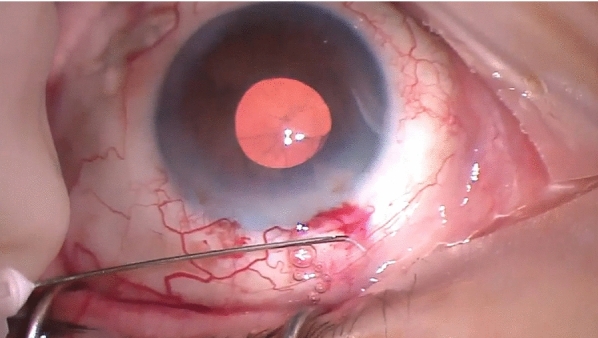
Once flow has been confirmed, the length and position of the Xen Gel Stent can be adjusted with tying forceps so that it is 1 mm in the anterior chamber (Fig. 16).
Fig. 16.
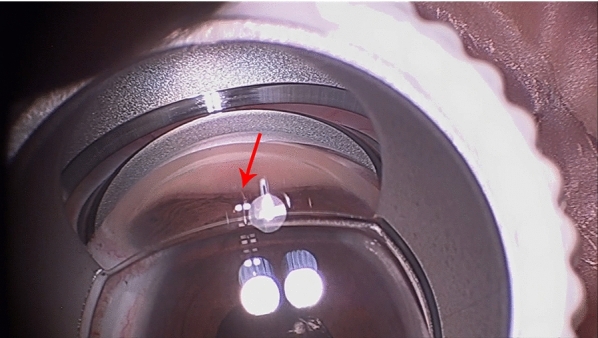
The length and position of the Xen Gel Stent can be checked with gonioscopy prior to closing the conjunctiva
(image courtesy of Brian Francis, MD)
If the tip of the Xen Gel Stent is lifting off the wall of the sclera, it may be advantageous to secure the tip of the stent back against the scleral wall with a 10.0 nylon suture. This will reduce the risk of conjunctival erosion, especially in patients where a tenectomy was necessary.
The Tenon’s layer and conjunctiva are then pulled anteriorly and closed (in two steps or both layers at once) with Vicryl sutures (Fig. 17) or 10-0 Nylon, creating a watertight closure with two wings or a running suture technique, as per surgeon preference. Care should be taken when pulling the conjunctiva forward to avoid dragging the Xen into the anterior chamber. Ideal placement with this technique is the Xen Gel Stent tip to be either directly under the conjunctiva (when generous tenectomy is performed) or tucked inferior underneath Tenon’s capsule.
Fig. 17.
Conjunctival closure
(image courtesy of David Yan, MD)
XEN Ex open Conjunctiva (MP4 67809 kb)
Open Conjunctiva XEN implantation via ab externo (no forward bias) (MP4 39220 kb)
Open Conjunctiva XEN implantation via ab externo (injector pulled back) (MP4 113191 kb)
Open Conjunctiva XEN implantation via ab externo placement (MP4 111191 kb)
Peri-operative/Adjunctive Use of Antifibrotic Agents
Most cases of failure following glaucoma filtering surgeries are related to the proliferation of fibroblasts, synthesis of extracellular matrix, and subsequent development of subconjunctival fibrosis [6]. Research has been carried out to investigate the potential for excising Tenon’s capsule [7, 8], placing valve implants above Tenon’s [9], and locating filtering blebs under Tenon’s [10]. However, it seems that the most important element to a successful glaucoma filtering surgery is the use of antimetabolites [1, 11, 12].
As the Xen Gel Stent procedure results in a subconjunctival filtration bleb, the use of MMC or 5 fluorouracil to control subconjunctival and episcleral fibrosis is becoming the standard of care. Initial studies of the Xen Gel Stent, without the use of an antifibrotic agent, resulted in failure rates of between 50% and 80% [1, 13]. Failure rates in single digits have been published in trials that included use of the MMC with the Xen Gel Stent procedure [2, 14, 15].
The authors employ antifibrotic agents according to the characteristics of the specific patient and their preferences. We present here four perioperative approaches employed by these authors.
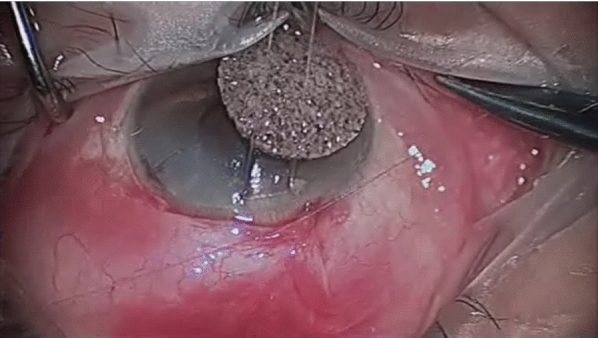
Option 1 Prior to starting the peritomy, MMC may be injected (0.4 mg/ml × 0.1 ml) approximately 10 mm posterior to the limbus, followed by use of a Weck-cel at the limbus to limit anterior spread of MMC. If a lower concentration of MMC is desired, it may be mixed with the Lidocaine. Due to the diffuse and posteriorly directed bleb, some authors (J.P.) feel comfortable injecting a higher concentration of MMC (60–80 mcg) at the beginning of the procedure (Figs. 18, 19).
Fig. 18.
MMC is injected > 10 mm from the limbus prior to conjunctival opening and stent implantation
(image courtesy of Brian Francis, MD)
Fig. 19.
Weck-cel placed at the limbus to limit anterior spread of MMC and kept posteriorly
(image courtesy of Joseph F. Panarelli, MD)
Option 2 MMC-soaked sponges may be placed posteriorly underneath Tenon’s after both the conjunctiva and Tenon’s have been dissected.
Option 3 MMC can be applied with a canula into the dissected subconjunctiva space ~ 4 mm posterior to the distal end of the Xen Gel Stent (~ 8 mm posterior to the limbus) after the stent has been placed (Fig. 20). A small amount of balanced salt solution can be used to diffuse the MMC and create a larger bleb.
Fig. 20.
MMC is injected > 8 mm from the limbus after conjunctival dissection and stent implantation
(image courtesy of Randy Craven, MD)
Option 4 MMC may be injected subconjunctivally at the end of the case after the conjunctiva has been closed. Since the Xen Gel Stent is already in place, it is desirable to repressurize the anterior chamber with BSS to ensure there is no ingress of MMC into the anterior chamber.
Applying MMC after conjunctival dissection has the advantage of minimizing hydration of the Tenon’s, preserving the natural tissue architecture and ease of dissection.
Open Conjunctiva Revision of Xen Gel Stent
A Xen Gel Stent surgery that has failed can be addressed via needling or by open conjunctiva revision. One of the authors (D.Y.) usually performs needling in cases where there is a focal bleb with a “ring of steel” limiting the bleb size; it should have a good conjunctiva that is mobile, not inflamed or vascularized outside of the ring. Many surgeons (B.F.) have transitioned to proceed directly to an open conjunctiva revision as the success rate seems to be higher with longer lasting effect.
Open revision can be performed in any case of Xen failure due to fibrosis, encapsulation when medical management or needling was not successful (clinically seen as a focal encapsulated bleb or a sleeve of tissue seen surrounding the distal tip of the implant) or in the presence of a curled and not freely mobile distal tip, indicating that it is embedded in Tenons tissue. Prior to surgery, confirm that the proximal end of the implant in the anterior chamber is in good position and not blocked with iris tissue.
Surgical Technique
If a subconjunctival injection of MMC is preferred, start with a dose of MMC between 40 and 80 μg in the area surrounding the distal tip of the failed implant. An alternative is applying MMC via sponges once the tissue is opened.
A conjunctival peritomy is made at the limbus, keeping Tenon's insertion intact.
A blunt posterior dissection is carried out to separate Tenon's from the conjunctiva.
Careful dissection of the capsule or tissue surrounding the implant with Vannas scissors is performed to uncover the Xen Gel Stent. If the implant is damaged during this step, a new implant can be placed via ab externo approach.
If the Tenon’s layer is thickened and fibrotic, perform a limited removal of the tissue in the filtration zone.
At this point, flow through the device should be confirmed. If there is no apparent outflow from the Xen Gel Stent, it may be unblocked by inserting the stent tip inside a 27G cannula mounted on a 3-ml syringe and flushing the stent with BSS into the anterior chamber.
If MMC is applied via sponges, it should be done at this time.
BSS is used to wash out MMC. The cannula can be inserted more posteriorly to provide posterior tissue dissection to facilitate a larger and more posterior filtration zone.
The conjunctiva is closed using the surgeon’s preferred technique. Two wing sutures with 8.0 Vicryl on a BV needle with the knots buried is preferred by most of the authors of this paper. If needed, add a central mattress suture at the limbus.
XEN surgical revision (MP4 157096 kb)
The key takeaway points are (1) reapplication of MMC, (2) freeing up Tenon’s adhesions, (3) creating a space between Tenon’s and sclera for the distal tip of the implant (rather than in the subconjunctival space), and (4) ensuring integrity and function of the implant (a new implant can be placed if needed).
One of the authors (B.F.) anecdotally found the success rate to be approximately 70–80%. Based on the high success rate in his hands, an open conjunctiva revision is his go-to procedure after Xen Gel Stent failure. Traditional filtration glaucoma surgery is recommended if this approach fails.
Discussion
A retrospective cohort study was conducted by Yan et al. [16] on 45 consecutive patients with previous glaucoma surgery and conjunctival scarring who underwent ab externo, open conjunctiva Xen Gel Stent implantation. At 12 months after Xen placement, 71% of patients had an IOP less than 18 mmHg or an IOP reduction greater than 20% on no medications, while 96% of patients met the same IOP criteria with IOP lowering medications. Patients with conjunctival scarring from previous surgery are generally poor candidates for Xen Gel Stent implantation by a closed conjunctiva, ab interno approach, and a tube shunt is more commonly utilized after the first glaucoma surgery has failed. The results of this retrospective study are encouraging for expanding the scope of usage for the Xen Gel Stent to more challenging cases by adopting an open conjunctiva, ab externo technique. One author (J.P.) reports that, in patients implanted with the Xen Gel Stent using an open conjunctiva, ab externo approach, less than 5% of his patients require a needling procedure, and the remaining authors concur that their needling rates have plummeted (unpublished data). None of the authors of this paper have seen any erosions with this technique to date, likely because the implant is deeper in the tissue, leaving a protective layer of Tenon’s above the distal end of the tip. Based on personal clinical experience, some authors (B.F.) prefer the open conjunctiva, ab externo approach in patients that have a lower target IOP of around 10–12 mmHg. While a comparative study has not been carried out, the clinical experience of the authors has led them to believe that an open conjunctiva approach allows for a lower IOP compared to a closed conjunctiva approach.
Opening the conjunctiva with a small incision provides many advantages. First, it allows for direct anatomical confirmation of stent placement and the possibility of placement in the superotemporal conjunctiva. Second, it allows for clear separation of the Tenon’s insertion from the episclera and a nice posterior “pocket” where the Xen Gel Stent can be placed to achieve a posterior bleb and avoids the stent getting tangled in the Tenon’s. In addition, it provides the option to perform a tenectomy if the tissues are found to be scarred or thickened upon initial dissection. Third, this approach allows anti-metabolites to be injected near the distal tip of the Xen Gel Stent under the conjunctiva or applied with sponges, based on surgeon preference.
Conclusion
The benefits of the ab externo technique include easier visualization of the angle in patients with a very shallow chamber, with severe corneal opacity, or with extremely deep-set eyes and open access to cauterize bleeding in cases with increased hyperemia. Additionally, it allows surgeons to limit the trauma secondary to intraocular surgery (corneal incisions, anterior chamber manipulation, etc.) The ab interno technique, on the other hand, lends itself to use with cataract surgery. Hence, proficiency with both approaches helps the surgeon customize gel stent surgery to the needs of the individual patient and greatly expands the scope of utilization of the Xen Gel Stent to patients with a wide variety of challenges.
Acknowledgements
Funding
The Rapid Service Fees were funded by Allergan, PLC (Irvine, CA). The authors participated in a consensus panel on this topic for which they were reimbursed. However, they were not provided honoraria for any time spent developing, reviewing or editing this manuscript, or for contributing videos.
Editorial Assistance
Editorial assistance in the preparation of this article was provided by Adrianne Resek, MA. Support for this assistance was funded by Allergan, PLC (Irvine, CA, USA).
Authorship
All authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Disclosures
Joseph Panarelli, Randy Craven, David Yan and Brian Francis declare that they are consultants for Allergan, PLC (Irvine, CA, USA).
Compliance with Ethics Guidelines
This article does not contain any studies with human participants or animals performed by any of the authors.
Data Availability
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Footnotes
Enhanced Digital Features
To view enhanced digital features for this article go to 10.6084/m9.figshare.11836185.
References
- 1.Grover DS, Flynn WJ, Bashford KP, et al. Performance and safety of a new ab interno gelatin stent in refractory glaucoma at 12 months. Am J Ophthalmol. 2017;183:25–36. doi: 10.1016/j.ajo.2017.07.023. [DOI] [PubMed] [Google Scholar]
- 2.Schlenker MB, Gulamhusein H, Conrad-Hengerer I, et al. Efficacy, safety, and risk factors for failure of standalone ab interno gelatin microstent implantation versus standalone trabeculectomy. Ophthalmology. 2017;124:1579–1588. doi: 10.1016/j.ophtha.2017.05.004. [DOI] [PubMed] [Google Scholar]
- 3.Lenzhofer M, Kersten-Gomez I, Sheybani A, et al. Four-year results of a minimally invasive transscleral glaucoma get stent implantation in a prospective multi-centre study. Clin Exp Ophthalmol. 2018;47(5):581–587. doi: 10.1111/ceo.13463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mansouri K, Guidotti J, Rao HL, et al. Prospective evaluation of standalone XEN gel implant and combined phacoemulsification-XEN gel implant surgery: 1-year results. J Glaucoma. 2018;27(2):140–147. doi: 10.1097/IJG.0000000000000858. [DOI] [PubMed] [Google Scholar]
- 5.Gillmann K, Bravetti GE, Mermoud A, Rao HL, Mansouri K. XEN gel stent in pseudoexfoliative glaucoma: 2-year results of a prospective evaluation. J Glaucoma. 2019;28(8):676–684. doi: 10.1097/IJG.0000000000001295. [DOI] [PubMed] [Google Scholar]
- 6.Skuta GL, Parrish RK., II Wound healing in glaucoma filtering surgery. Surv Ophthalmol. 1987;32(3):149–170. doi: 10.1016/0039-6257(87)90091-9. [DOI] [PubMed] [Google Scholar]
- 7.Miller KN, Blasini M, Shields MB, Ho C-H. A comparison of total and partial tenonectomy with trabeculectomy. Am J Ophthalmol. 1991;111(3):323–326. doi: 10.1016/S0002-9394(14)72317-7. [DOI] [PubMed] [Google Scholar]
- 8.Awadein A, El Sayed YM. Excision of tenon capsule in pediatric trabeculectomy: a controlled study. J Glaucoma. 2016;25(1):39–44. doi: 10.1097/IJG.0000000000000220. [DOI] [PubMed] [Google Scholar]
- 9.Elhefney EM, Al-Sharkawy HT, Kishk HM. Supra-tenon capsule implantation of the ahmed glaucoma valve in refractory pediatric glaucoma. J Glaucoma. 2016;25(9):732–737. doi: 10.1097/IJG.0000000000000514. [DOI] [PubMed] [Google Scholar]
- 10.Zigiotti GL, Savini G, De Caro R, et al. The features of Tenon’s capsule at the limbus. Ital J Anat Embryol. 1997;102(1):5–11. [PubMed] [Google Scholar]
- 11.Khaw PT, Chiang M, Shah P, Sii F, Lockwood A, Khalili A. Enhanced trabeculectomy: the moorfields safer surgery system. Dev Ophthalmol. 2017;59:15–35. doi: 10.1159/000458483. [DOI] [PubMed] [Google Scholar]
- 12.Cairns JE. Clear-cornea trabeculectomy. Trans Ophthalmol Soc UK. 1985;104(Pt 2):142–145. [PubMed] [Google Scholar]
- 13.Morgan WH, Quill B, Cringle SJ, House PH, Yu DY. Long-Term Results Using Gelatin Microfistulae Implantation without Antimetabolite. Ophthalmology. 2018;125(11):1828–1829. doi: 10.1016/j.ophtha.2018.05.024. [DOI] [PubMed] [Google Scholar]
- 14.Hengerer FH, Kohnen T, Mueller M, et al. Ab interno gel implant for the treatment of glaucoma patients with or without prior glaucoma surgery: 1-year results. J Glaucoma. 2017;26(12):1130–1136. doi: 10.1097/IJG.0000000000000803. [DOI] [PubMed] [Google Scholar]
- 15.De Gregorio A, Pedrotti E, Russo L, Morselli S. Minimally invasive combined glaucoma and cataract surgery: clinical results of the smallest ab interno gel stent. Int Ophthalmol. 2017 doi: 10.1007/s10792-017-0571-x. [DOI] [PubMed] [Google Scholar]
- 16.Zhang A, Abadeh A, Yan DB, Ahmed IIK. Ab externo implantation technique for Xen 45 microstent in eyes with previous surgery. Presented at the Canadian Ophthalmological Society Annual Meeting. June 13, 2019. Quebec, Quebec.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.