

Abstract
This study aimed to investigate associations between Brief Job Stress Questionnaire (BJSQ)-measured job stress factors and sickness absence in Japanese workers. Among 551 healthy, employed Japanese men and women (age range: 21-73 years) who underwent mental health examinations at the Osaka Medical Center for Health Science and Promotion between 2006 and 2009, 197 (67 men, 130 women) consented to participate in this study. Their sickness absences until the end of March 2010 were then followed-up via postal mail survey, with 112 participants effectively responding to the question on sickness absence (56.9%). The hazard ratio (HR) and 95% confidence interval (CI) were calculated using the Cox proportional hazards model, adjusting for age, sex, and lifestyle factors. Among the 112 respondents, 12 took sickness absence after their study entry, as found during the mean 2.3 years of follow-up (258.8 person-years). Among all sickness absences, those of eight participants were because of mental illness. Physical demands were positively associated with increased risks of all sickness absence (adjusted HR: 2.78, 95% CI: 1.01-7.64). Physical demands were predictive for all sickness absence, and should be alleviated at workplaces to prevent such absence.
Keywords: depressive symptoms, job stressor, physical demands, physical environment, sickness absence
Introduction
Sickness absence due to chronic illnesses such as mental illnesses, diabetes mellitus, cardiovascular diseases, cancer, respiratory diseases, low back pain, and musculoskeletal problems can significantly decrease productivity1). An adverse psychosocial work environment, including burdensome job demands and poor job control, has been found to increase the risk of sickness absence2-6). Of special note, the psychosocial work environment can greatly impact mental well-being5). Indeed, a systematic review revealed that adverse work environment, with aspects such as low decision latitude, high job stress, and bullying, increased depressive symptoms over time7).
In recent years, certified industrial accidents due to mental disorders have been increasing in Japan8). To prevent mental disorders, from December 2015, changes based on amendments to Japan’s Industrial Safety and Health Act have required employers to introduce a “stress-check system” in workplaces that have ≥50 regular employees. Workplaces with <50 regular employees are encouraged, but not required, to administer such checks. This system is aimed at preventing work-related illness by helping employees identify impacts of job stress, and helping employers improve their work environments.
The Ministry of Health, Labour and Welfare of Japan9) recommended use of the Brief Job Stress Questionnaire (BJSQ)10) for the stress check. This consists of 57 items graded on a four-point Likert-type scale to measure job stressors (17 items), psycho-physical complaints (29 items), support for workers (nine items), and job and life satisfaction (two items). A few prospective studies have examined associations between the BJSQ and sickness absence. One revealed that the upper quartile among psycho-physical complaints increased risk of sickness absence due to depression or depressive symptoms11). Another showed that high quantitative job overload increased risk of recurrent sickness absence due to depression12). Recently Tsutsumi et al.13) investigated whether high stress levels as per the BJSQ and, in accordance with the above-mentioned Ministry’s recommendation of a stress check program manual, can predict sickness absence. High stress is defined as the highest level of stress response or having a moderate or higher level of stress response, together with the highest level of job stressors (or lowest level of social support in the workplace). Employees with high stress levels have an elevated risk of long-term sickness absence13).
Since 2010 and before the introduction of the stress-check system, mental health checkups have been conducted at the Osaka Medical Center for Health Science and Promotion to examine the association of mental stress levels with somatic and psychological symptoms. In one of the stress response examinations at the checkups, participants were assessed on their acute cardiovascular reactivity to stressful tasks through measurements of their blood pressure, heart rate, heart rate variability, and peripheral blood flow. Our previous study investigated associations between the BJSQ and acute cardiovascular reactivities to stressful tasks14). Among the job stressors in the BJSQ, not only quantitative but also qualitative job overload, physical demands, and poor physical environment were associated with the measured reactivity. Although a previous study by Endo et al.12) used only quantitative job overload for job stressors in relation to recurrent sickness absence, other job stressors may be predictive for sickness absence. While the stress-check system has been mandated for workplaces with ≥50 regular employees, the abovementioned mental health checkups included employees, such as teachers, who are in workplaces with <50. Our data allowed us to investigate associations between job stressors as measured via the BJSQ and sickness absence with employees including those in smaller workplaces and before introduction of that system.
The present study aimed to investigate associations between job stressor factors as measured by the BJSQ and sickness absence in Japanese workers. We hypothesized that quantitative and qualitative job overload, physical demand, and poor physical environment were positively associated with sickness absence risk. We also investigated whether those job stressors were associated with that risk after controlling for depressive symptoms.
Subjects and methods
Mental health checkups
A “physical and mental refresh course” comprising mental health checkups was conducted at the Osaka Medical Center for Health Science and Promotion between 2001 and 2009. The checkups were conducted to measure associations between stress levels and the effect on somatic and psychological symptoms. Stress levels were assessed using several psychological questionnaires, as well as physiological markers such as blood pressure, heart rate, blood flow, and hormonal indices. Checkups could be applied for through companies in the Osaka region, as well as on the Osaka Medical Center for Health Science and Promotion website.
The data from these checkups have been reported elsewhere14-16), as have the data on cardiovascular reactivity and sickness absences17).
Participants
A total of 551 Japanese workers (212 men, 339 women; age range: 21-73 years) underwent the abovementioned checkups between 2006 and 2009, as the baseline survey. The most frequent occupation reported among workers was teacher (54% of men, 67% of women). This was because enrollment was advertised through health insurance societies in Osaka. The study was explained to all 551 applicants, and 197 (67 men, 130 women) subsequently gave written consent to take part in the study.
Sickness absence data on the 197 participants from the date of their mental health checkups through March 31, 2010, were followed-up using a postal mailed questionnaire. This included a question on sickness absence: “Have you taken sickness absence since the mental health checkup?” If participants responded “Yes”, they were also asked to indicate the date the sickness absence began. If the participants took sickness absence several times, they were instructed to indicate the date of the first time since the checkups. They were asked their reasons for absence from among physical illness, and/or mental illness, and/or other reasons, such as caring for aged parents.
Among the 197 contacted, 119 completed the questionnaire (response rate: 60.4%). A total of 115 (40 men, 75 women) responded regarding whether they had taken sickness absence. Three had taken absence before the mental health checkups, and were therefore excluded from the analyses. Ultimately, 112 (39 men, 73 women) respondents were included in the analysis (effective response rate: 56.8%). Figure 1 is a flowchart on selection of participants in this study. Table 1 shows the participants’ measured variables at the baseline.
Figure 1.
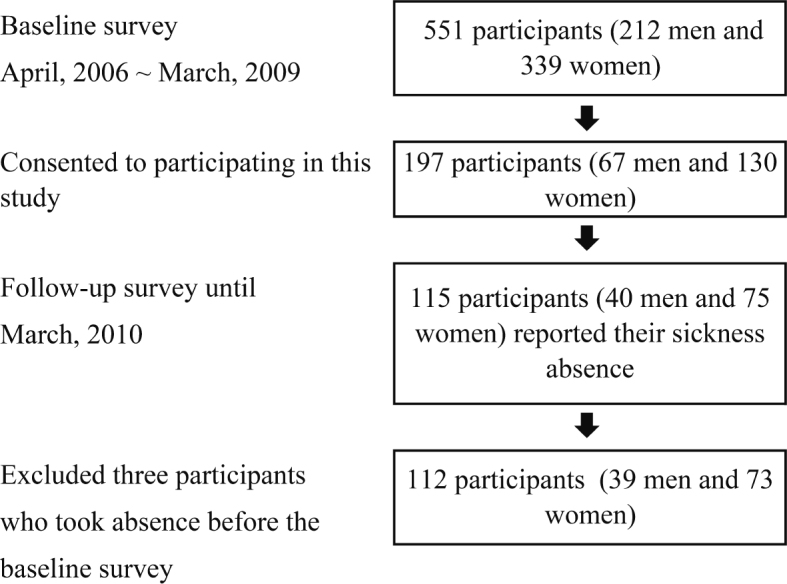
Flowchart of subject selection and participation
Table 1.
Participants’ means (SDs) and proportions of measured variables
| Quantitative job overload | Mean and SD | 9.4 | 2.1 |
| Qualitative job overload | Mean and SD | 9.2 | 1.9 |
| Physical demands | Mean and SD | 2.4 | 0.9 |
| Interpersonal conflict | Mean and SD | 7.1 | 1.7 |
| Poor physical environment | Mean and SD | 2.6 | 0.9 |
| Age (years) | Mean and SD | 48.7 | 8.0 |
| Body Mass Index (kg/m2) | Mean and SD | 23.1 | 3.0 |
| Depressive symptoms | Mean and SD | 17.2 | 9.7 |
| Women | % | 65.2 | |
| Management position or professional | % | 76.8 | |
| (Teachers | % | 60.7) | |
| Current smokers | % | 8.9 | |
| Current drinkers | % | 50.0 | |
| Physically active | % | 56.3 | |
| Medical history of diabetes mellitus | % | 5.4 | |
| Medical history of hypertension | % | 12.5 | |
| Medical history of hyperlipidemia | % | 42.0 |
Ethics approval and consent to participate
The present study was conducted after obtaining approval from the Ethics Committee of the Osaka Medical Center for Health Science and Promotion (#4).
Questionnaires and measurements
The BJSQ was used10), with 57 items graded on a four-point Likert-type scale to measure job stressors, psycho-physical complaints, and support for workers. Cronbach’s alpha coefficients, calculated based on the present data, are shown in parentheses. In this study, the effects of quantitative (three items; alpha: 0.82) and qualitative job overload (three items; alpha: 0.73), physical demands (one item), interpersonal conflicts (three items; alpha: 0.64), and poor physical environment (one item) were assessed. Sample items are as follows: “You have to do an enormous amount of work” for quantitative job overload, “You have to focus your attention quite a lot” for qualitative job overload, “You do a lot of physical work” for physical demands, “There are differences of opinion within your department” for interpersonal conflicts, and “The environment of your workplace (noise, light, humidity, and ventilation) is not so good” for poor physical environment.
Depressive symptoms were assessed using the Japanese translation of the Center for Epidemiologic Studies Depression Scale (CES-D)18,19), of which 20 items (alpha: 0.88) were scored from 0 (not at all) to 3 (for >5 days). Although a score of ≥16 has been used extensively as the cutoff point for classification of “highly depressed” on this scale18), we used the CES-D score and BJSQ score in the present study.
Sex and age were asked about in investigation for potential confounding factors. Participants were asked about their current work, and their occupational status was categorized as manager/professional or general worker. Teachers were categorized as professionals based on preceding studies and vital statistics in Japan20,21). Participants were asked about their smoking status, which was categorized as current smoker or never/ex-smoker, and alcohol drinking status, which was categorized as current drinker or never/ex-drinker. The scale of the Japan Arteriosclerosis Longitudinal Study was used to evaluate physical activity22). Participants were asked whether they had exercised regularly for >15 minutes within the previous 3 months, and were categorized as physically active if they answered “Yes.” Information on medication was asked and use of medication for antihypertension, diabetes mellitus, or hyperlipidemia was identified.
Height in feet (wearing stockings or socks) and weight in light clothing were measured at the mental health checkups. Body mass index was calculated (kg/m2). Blood pressure was measured, and peripheral blood was collected between 2 p.m. and 4 p.m. at the front desk of the mental health facility. Hypertension was defined as systolic blood pressure ≥140 mmHg, and/or diastolic blood pressure ≥90 mmHg, and/or use of antihypertensive medication. Diabetes mellitus was defined as fasting glucose level of ≥126 mg/dL or non-fasting glucose level of ≥200 mg/dL, and/or the use of medication for diabetes mellitus. Hyperlipidemia was defined as total cholesterol level ≥220 mg/dL and/or use of medication for hyperlipidemia. Participants with a medical history of such conditions were categorized as having hypertension and/or diabetes mellitus and/or hyperlipidemia. No participant had a history of stroke or myocardial infarction.
Statistical methods
The crude hazard ratio (HR) and 95% confidence interval (95% CI) from sickness absence according to job stressors, including quantitative job overload, qualitative job overload, physical demands, interpersonal conflict, and poor physical environment, and age- and sex-adjusted HRs, were calculated using the Cox proportional hazards model. Crude HR, age- and sex-adjusted HRs, and the 95% CIs from sickness absence in accordance with all sickness, excluding other reasons and depressive symptoms, were also calculated. The adjusted HRs and 95% CIs were calculated to investigate associations between the job stressors, depressive symptoms, and sickness absence, adjusting for age, sex (reference: men), occupation (reference: managers/professionals), and alcohol consumption habits (reference: non-drinkers). Among the potential confounding factors, a t-test indicated occupation and alcohol consumption habits were significantly associated with job stressors; therefore, these two variables were used in the models (Appendix). Teachers, because they were a majority of the participants, were also compared with other occupations in the model (reference: other occupations). All statistical analyses were performed with IBM SPSS Statistics for Windows, Version 25 (IBM Corp., Armonk, NY, USA).
Results
During the mean 2.3 years (standard deviation: 0.9, range: 0.02-3.69) of follow-up of 112 healthy employees (258.8 person-years), 12 (4 men, 8 women) took sickness absence for any reason and 10 (4 men, 6 women) for all sickness, excluding other reasons; among them, 8 (3 men, 5 women) took sickness absence due to mental illness. Table 2 shows details of those 12 participants.
Table 2.
Details about participants who took sickness absence
| No. | Sex | Age | Occupation | Reason of sickness
absence |
| 1 | Woman | 41 | Office worker | Mental illness |
| 2 | Woman | 44 | Office worker | Mental illness |
| 3 | Woman | 56 | Teacher | Mental illness |
| 4 | Woman | 58 | Teacher | Mental illness |
| 5 | Woman | 31 | Teacher | Mental illness |
| 6 | Woman | 61 | Teacher | Physical illness |
| 7 | Woman | 33 | Teacher | Other reasons |
| 8 | Woman | 29 | Teacher | Other reasons |
| 9 | Man | 33 | Labor worker | Mental illness |
| 10 | Man | 52 | Teacher | Mental illness |
| 11 | Man | 51 | Teacher | Mental illness |
| 12 | Man | 54 | Teacher | Physical illness |
Table 3 shows crude HRs and adjusted HRs in relation to all sickness absence. For associations between job stressors and all sickness absence, crude and age- and sex-adjusted HRs of physical demands increased, 2.16 (95% CI: 0.96-4.86) and 2.23 (95% CI: 0.98-5.06), respectively. However, those HRs did not reach statistical significance. When HRs were adjusted for all potential confounding factors, physical demands (adjusted HR: 2.78, 95% CI: 1.01-7.64) were found associated with increased risk of sickness absence. When two cases of sickness absence due to other reasons were excluded, physical demands (adjusted HR: 3.07, 95% CI: 1.02-9.25) were strongly associated with an increased risk of sickness absence. The variance inflation factors for age, sex, occupation, and alcohol consumption habits were all low (<1.4), suggesting no multicollinearity problems.
Table 3.
Associations between work stressors, depressive symptoms, and sickness absence
| Crude
HR |
95% CI | Age and sex
adjusted-HR |
95% CI | Multivariable
adjusted-HR# |
95% CI | ||||
| Sickness absence due to all causes (n = 12) | |||||||||
| Quantitative job overload | 0.85 | 0.60 | 1.20 | 0.80 | 0.55 | 1.17 | 0.79 | 0.51 | 1.22 |
| Qualitative job overload | 0.91 | 0.56 | 1.47 | 1.00 | 0.60 | 1.68 | 0.98 | 0.52 | 1.84 |
| Physical demands | 2.16 | 0.96 | 4.86 | 2.23 | 0.98 | 5.06 | 2.78 | 1.01 | 7.64 |
| Interpersonal conflict | 1.17 | 0.80 | 1.71 | 1.08 | 0.73 | 1.61 | 1.12 | 0.72 | 1.75 |
| Poor physical environment | 1.91 | 0.92 | 3.95 | 1.96 | 0.93 | 4.14 | 2.19 | 0.92 | 5.25 |
| Depressive symptoms | 1.05 | 0.99 | 1.11 | 1.04 | 0.99 | 1.10 | 1.06 | 0.98 | 1.14 |
| Sickness absence due to all sickness (n = 10) | |||||||||
| Quantitative job overload | 0.81 | 0.53 | 1.24 | 0.82 | 0.53 | 1.25 | 0.80 | 0.50 | 1.27 |
| Qualitative job overload | 0.78 | 0.43 | 1.45 | 0.78 | 0.41 | 1.46 | 0.83 | 0.42 | 1.64 |
| Physical demands | 2.74 | 0.97 | 7.77 | 2.74 | 0.96 | 7.88 | 3.07 | 1.02 | 9.25 |
| Interpersonal conflict | 1.20 | 0.75 | 1.91 | 1.20 | 0.75 | 1.94 | 1.18 | 0.73 | 1.90 |
| Poor physical environment | 1.93 | 0.79 | 4.73 | 1.94 | 0.80 | 4.73 | 1.92 | 0.77 | 4.78 |
| Depressive symptoms | 1.07 | 0.99 | 1.15 | 1.07 | 0.99 | 1.15 | 1.07 | 0.99 | 1.16 |
| Sickness absence due to mental problems (n = 8) | |||||||||
| Quantitative job overload | 1.21 | 0.70 | 2.10 | 1.19 | 0.68 | 2.08 | 1.05 | 0.60 | 1.83 |
| Qualitative job overload | 0.70 | 0.37 | 1.34 | 0.73 | 0.36 | 1.48 | 0.86 | 0.41 | 1.77 |
| Physical demands | 1.89 | 0.68 | 5.22 | 1.86 | 0.67 | 5.11 | 1.65 | 0.48 | 5.62 |
| Interpersonal conflict | 1.32 | 0.86 | 2.02 | 1.28 | 0.83 | 1.98 | 1.19 | 0.73 | 1.94 |
| Poor physical environment | 1.48 | 0.63 | 3.47 | 1.48 | 0.64 | 3.44 | 1.38 | 0.53 | 3.61 |
| Depressive symptoms | 1.09 | 1.02 | 1.16 | 1.08 | 1.01 | 1.15 | 1.07 | 0.98 | 1.16 |
# Age, sex, job position, and alcohol habits were adjusted.
For associations between depressive symptoms and all sickness absence, no HRs reached statistical significance. However, regarding associations between depressive symptoms and sickness absence due to mental illness, the crude HR (1.09, 95% CI: 1.02-1.16) and age- and sex-adjusted HR (1.08, 95% CI: 1.01-1.15) showed increased risks of such absence (Table 3). After adjusting for all confounding factors, the association had lower significance (adjusted HR: 1.07, 95% CI: 0.98-1.16) but still showed the same tendency. Job stressors, however, were not associated with risk of sickness absence due to mental illness.
There was no significant association between occupation and sickness absence (adjusted HR: 1.67, 95% CI: 0.22-12.62 for all and 2.08, 95% CI: 0.24-18.26 for mental illness). There was also no significant association when teachers were compared with other occupations (adjusted HR: 2.29, 95% CI: 0.34-15.30 for all and 1.53, 95% CI: 0.19-12.02 for mental illness).
Discussion
The present study investigated associations between the job stress factors measured by the BJSQ and risk of sickness absence, using the data collected at the mental health checkups. Among 112 participants who were followed-up from their entry in the mental health checkups in 2006-2009 until May 2010, 12 took sickness absence. After adjusting for potential confounding factors, results showed that physical demands were associated with an increased risk of sickness absence. When limited to eight sickness absences due to mental illness, the association between the job stressors in the BJSQ and sickness absence showed the same tendency but was attenuated. Depressive symptoms were associated with increased risks of sickness absence due to mental illness. Physical demands indicated in the BJSQ could be predictive for sickness absence for any reason.
In the present study, workers who performed a great deal of physical work had increased risk of all forms of sickness absence. This result was consistent with previous studies conducted in Demark and Sweden, collectively revealing that physical work demands were a risk factor for sickness absence23-25). Physical demands, such as uncomfortable work positions, including extreme bending of the body or twisting of the neck or back, and working mainly in a standing or squatting position were risk factors for development of musculoskeletal disorders26), cardiovascular disease27), or sickness absence24,25). Uncomfortable working positions, lifting or carrying loads, and pushing or pulling loads also increased sickness absence23,25). In our previous study of associations between the job stressors in the BJSQ and cardiovascular reactivities to stressful tasks, physical demands were associated with such reactivities15). Notably, physical demands were associated with reactivities of blood pressure and peripheral blood flow in male managers/professionals. Workers who performed a great deal of physical work may be reflective of individual vulnerability to stressors, and their stress responses may increase, which could lead to health problems and sickness absence. However, in the present study, the majority of sickness absence was due to mental illness. Moreover, there were only two absences due to physical illness, with two for other reasons. Physical demands are a potential risk factor for sickness absence for any reason28).
Regarding sickness absence due to mental illness, depressive symptoms were associated, while job stressors measured by the BJSQ were not significantly associated. This result may be attributed to our small sample size, of which the power was insufficient for reaching statistical significance. Another hypothetical reason may be a mediating effect of depressive symptoms between job stressors and sickness absence due to mental illness. A previous study revealed that the upper quartile of psycho-physical complaints was predictive for increased sickness absence due to depression11). A prospective study of the BJSQ revealed that the high stress levels measured by combination of psychological stress response and job stressors were associated with sickness absence from mental health disorders29). High stress levels in the BJSQ, based on recommendation of the stress check program manual, mainly focus on the psychological stress response, rather than job stressors. In a cross-sectional study using the BJSQ, quantitative and qualitative job overload were found positively associated with psychological complaints30). The job stressors may not be directly associated with sickness absence due to mental illness, however, they increased workers’ psychological complaints or depressive symptoms, which could lead to mental illness, including depression, and then to sickness absence. Whether depressive symptoms mediate associations between the job stressors and sickness absence due to mental illness should be investigated in future studies with a larger sample and long-term follow-up.
We combined teachers, who comprised the majority of professionals in the study population, with managers in a higher occupational status category. Certain factors should be considered here. Teachers in Japan are subjected to higher stress levels than other occupations31). Indeed, in 2009-2011, 0.6% of Japanese teachers were suspended from their jobs because of mental disorders32). In accordance with such findings, compared with other professions, teachers in the present study scored higher in quantitative and qualitative job overload and physical demands (Appendix). Job stressors may vary among occupations; in the study sample, when teachers were compared with other occupations on sickness absence, for whatever reason, there was no significant difference. The small sample may not have permitted us to distinguish the effect teachers’ occupational characteristics have on sickness absence. Future studies should address this factor.
The present study had some other limitations. First was the relatively low number of participants and a low response rate for recruitment, despite our efforts to notify candidates. This small sample did not permit us to analyze sex-based differences in the associations between job stressors and sickness absence. Furthermore, an unrepresentative sample of Japanese working men and women could lead to biased results. Participation was also voluntary because the present study was conducted along with a local medical examination provided outside of the workplace. Measured job stressors were not reflective of certain workplace characteristics but rather were individuals’ perceived levels. The sample in the present study may contain people especially conscious of their mental health, and/or may be a group at high risk for mental problems. A previous prospective study conducted within a company11) found 14 of 1,810 employees developed depression during 1.8 years of follow-up (0.8%); in comparison, the present study had nine sickness absences due to mental illness among the 112 participants, during a mean 2.3 years of follow-up (8.0%). Furthermore, follow-up time differed depending on when a participant was enrolled. Information on sickness absence were obtained by a self-report via postal mail. Care should be taken in interpreting the results because of measurement and recall bias. Other potential confounding factors not considered in the present study should be taken into account for future studies because multiple factors may underlie perceived symptoms and lead to sickness absence.
Despite limitations in the present study, as explained above, we found job stress factors measured by the BJSQ at mental health checkups outside of workplaces were robustly predictive for sickness absence. This study supports the effectiveness of the BJSQ, even though it was measured before the introduction of the stress-check system and was applied for employees in smaller workplaces. Additionally, physical demands were predictive for increased sickness absence owing to whatever reason, after adjusting for potential confounding factors. However, although the associations between job stressor factors and sickness absence due to mental illness were weak, depressive symptoms were associated with such absence. Physical demands could be improved using workplace interventions, and their implementation could be used to prevent all forms of sickness absence, along with assessment of workers’ perceived work-related stress levels.
Acknowledgments
This study was supported in part by KAKENHI grants from the Japan Society for the Promotion of Science (grant numbers: 22390123, 26670334) and the Japan Small- and Medium-Sized Enterprise Welfare Foundation (FULLHAP). We thank Edanz Group (www.edanzediting.com/ac) for editing a draft of this manuscript.
Conflict of interest disclosure
The authors declare that they have no competing interests.
Appendix
Appendix.
Comparisons between groups by demographic variables in job stress factors
| Manager/Professional
(n = 86) |
General workers
(n = 26) |
p# | Teacher
(n = 68) |
Other occupations
(n = 44) |
p# | |||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | |||
| Quantitative job overload | 9.4 | 2.1 | 8.8 | 2.0 | 0.16 | 9.6 | 2.1 | 8.8 | 2.1 | 0.047 |
| Qualitative job overload | 9.5 | 1.7 | 7.9 | 1.9 | 0.001 | 9.6 | 1.7 | 8.4 | 1.9 | 0.001 |
| Physical demands | 2.6 | 0.8 | 1.7 | 0.7 | <0.001 | 2.6 | 0.8 | 1.9 | 0.8 | <0.001 |
| Interpersonal conflict | 7.1 | 1.7 | 7.2 | 2.0 | 0.73 | 7.1 | 1.5 | 7.0 | 2.0 | 0.76 |
| Poor physical environment | 2.6 | 0.9 | 2.6 | 0.9 | 0.87 | 2.6 | 0.9 | 2.6 | 0.9 | 0.99 |
| Current smoker
(n = 10) |
Non-smoker
(n = 102) |
p# | Current drinker
(n = 57) |
Non-drinker
(n = 55) |
p# | |||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | |||
| Quantitative job overload | 9.6 | 2.0 | 9.3 | 2.1 | 0.62 | 9.5 | 2.1 | 9.1 | 2.2 | 0.26 |
| Qualitative job overload | 9.3 | 1.1 | 9.1 | 1.9 | 0.73 | 9.1 | 1.8 | 9.1 | 1.8 | 0.85 |
| Physical demands | 2.5 | 0.7 | 2.3 | 0.9 | 0.59 | 2.4 | 0.9 | 2.4 | 0.8 | 0.94 |
| Interpersonal conflict | 8.0 | 1.5 | 7.0 | 1.7 | 0.081 | 7.3 | 1.8 | 6.9 | 1.6 | 0.24 |
| Poor physical environment | 2.7 | 0.8 | 2.6 | 0.9 | 0.69 | 2.8 | 0.9 | 2.4 | 0.9 | 0.018 |
| Physically active
(n = 64) |
Non-active (n = 48) |
p# | History of diabetes millitus (n = 6) |
Without diabetes millitus (n = 106) |
p# | |||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | |||
| Quantitative job overload | 9.1 | 2.1 | 9.5 | 2.1 | 0.40 | 9.8 | 1.5 | 9.3 | 2.1 | 0.52 |
| Qualitative job overload | 8.9 | 2.0 | 9.4 | 1.6 | 0.098 | 10.0 | 0.9 | 9.1 | 1.9 | 0.22 |
| Physical demands | 2.2 | 0.8 | 2.5 | 0.9 | 0.051 | 2.7 | 0.5 | 2.3 | 0.9 | 0.37 |
| Interpersonal conflict | 7.1 | 1.7 | 7.0 | 1.8 | 0.80 | 6.3 | 1.6 | 7.1 | 1.7 | 0.27 |
| Poor physical environment | 2.7 | 0.9 | 2.5 | 0.9 | 0.27 | 2.5 | 1.0 | 2.6 | 0.9 | 0.81 |
| History of hypertension (n = 14) |
Without hypertension (n = 98) |
p# | History of hyperlipidemia (n = 47) |
Without hyperlipidemia (n = 65) |
p# | |||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | |||
| Quantitative job overload | 9.1 | 2.2 | 9.3 | 2.1 | 0.69 | 9.4 | 2.2 | 9.2 | 2.0 | 0.75 |
| Qualitative job overload | 9.5 | 1.0 | 9.1 | 1.9 | 0.39 | 9.2 | 1.9 | 9.0 | 1.8 | 0.68 |
| Physical demands | 2.4 | 0.9 | 2.3 | 0.9 | 0.74 | 2.3 | 0.9 | 2.4 | 0.8 | 0.86 |
| Interpersonal conflict | 7.2 | 1.4 | 7.1 | 1.8 | 0.77 | 7.1 | 1.9 | 7.1 | 1.6 | 0.93 |
| Poor physical environment | 2.6 | 0.8 | 2.6 | 0.9 | 0.82 | 2.6 | 1.0 | 2.6 | 0.9 | 0.89 |
# p values were based on a t-test to compare two groups.
References
- 1.de Vroome EM, Uegaki K, van der Ploeg CP, et al. Burden of sickness absence due to chronic disease in the Dutch workforce from 2007 to 2011. J Occup Rehabil, 25: 675-684, 2015. [DOI] [PubMed] [Google Scholar]
- 2.Kivimäki M, Vahtera J, Kawachi I, et al. Psychosocial work environment as a risk factor for absence with a psychiatric diagnosis: an instrumental-variables analysis. Am J Epidemiol, 172: 167-172, 2010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.D’Souza RM, Strazdins L, Broom DH, Rodgers B, Berry HL. Work demands, job insecurity and sickness absence from work. How productive is the new, flexible labour force? Aust N Z J Public Health, 30: 205-212, 2006. [DOI] [PubMed] [Google Scholar]
- 4.Virtanen M, Vahtera J, Pentti J, Honkonen T, Elovainio M, Kivimäki M. Job strain and psychologic distress influence on sickness absence among Finnish employees. Am J Prev Med, 33: 182-187, 2007. [DOI] [PubMed] [Google Scholar]
- 5.Mather L, Bergström G, Blom V, Svedberg P. High job demands, job strain, and iso-strain are risk factors for sick leave due to mental disorders: a prospective Swedish twin study with a 5-year follow-up. J Occup Environ Med, 57: 858-865, 2015. [DOI] [PubMed] [Google Scholar]
- 6.Kondo K, Kobayashi Y, Hirokawa K, et al. Job strain and sick leave among Japanese employees: a longitudinal study. Int Arch Occup Environ Health, 79: 213-219, 2006. [DOI] [PubMed] [Google Scholar]
- 7.Theorell T, Hammarström A, Aronsson G, et al. A systematic review including meta-analysis of work environment and depressive symptoms. BMC Public Health, 15: 738, 2015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.The Japanese Ministry of Health, Labour and Welfare. Workers’ compensation due to mental disorders. (in Japanese) 2016. http://www.mhlw.go.jp/file/04-Houdouhappyou-11402000-Roudoukijunkyokuroudouhoshoubu-Hoshouka/h27_seishin.pdf. Accessed 2016 Dec 14.
- 9.The Japanese Ministry of Health, Labour and Welfare. Stress checks and other mental health measures at the workplace, overwork measures, etc. 2015. http://www.mhlw.go.jp/bunya/roudoukijun/anzeneisei12/index.html. Accessed 2016 Dec 05.
- 10.Shimomitsu T, Haratani T, Ohno Y. The final development of the Brief Job Stress Questionnaire mainly used for assessment of the individuals. (in Japanese). In: Kato M, editor. Ministry of Labour sponsored grant for the prevention of work-related illness: The 1999 report. Tokyo: Tokyo Medical College, 126-164, 2000. [Google Scholar]
- 11.Wada K, Sairenchi T, Haruyama Y, Taneichi H, Ishikawa Y, Muto T. Relationship between the onset of depression and stress response measured by the Brief Job Stress Questionnaire among Japanese employees: a cohort study. PLoS One, 8: e56319, 2013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Endo M, Muto T, Haruyama Y, Yuhara M, Sairenchi T, Kato R. Risk factors of recurrent sickness absence due to depression: a two-year cohort study among Japanese employees. Int Arch Occup Environ Health, 88: 75-83, 2015. [DOI] [PubMed] [Google Scholar]
- 13.Tsutsumi A, Shimazu A, Eguchi H, Inoue A, Kawakami N. A Japanese Stress Check Program screening tool predicts employee long-term sickness absence: a prospective study. J Occup Health, 60: 55-63, 2018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hirokawa K, Nagayoshi M, Ohira T, et al. Menopausal status in relation to cardiovascular stress reactivity in healthy Japanese participants. Psychosom Med, 76: 701-708, 2014. [DOI] [PubMed] [Google Scholar]
- 15.Hirokawa K, Ohira T, Nagayoshi M, et al. Occupational status and job stress in relation to cardiovascular stress reactivity in Japanese workers. Prev Med Rep, 4: 61-67, 2016. a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hirokawa K, Ohira T, Nagayoshi M, et al. Dehydroepiandrosterone-sulfate is associated with cardiovascular reactivity to stress in women. Psychoneuroendocrinology, 69: 116-122, 2016. b. [DOI] [PubMed] [Google Scholar]
- 17.Hirokawa K, Ohira T, Kajiura M, et al. Cardiovascular reactivity to acute stress associated with sickness absence among Japanese men and women: a prospective study. Brain Behav, 10: e01541, 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Radloff LS. The CES-D scale. A self-report depression scale for research in the general population. Appl Psychol Meas, 1: 385-401, 1977. [Google Scholar]
- 19.Shima S, Shikano T, Kitamura T, Asai K. New self-rating scale for depression. (in Japanese) Seishin Igaku, 27: 717-723, 1985. [Google Scholar]
- 20.Fukuda Y, Nakamura K, Takano T. Accumulation of health risk behaviours is associated with lower socioeconomic status and women’s urban residence: a multilevel analysis in Japan. BMC Public Health, 27: 53, 2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Saeki N, Hiroko T, Sakata F. Vital statistics by occupation and industry. Koseino Shihyo, 47: 10-16, 2000. [Google Scholar]
- 22.Naito Y, Harada A, Inoue S, Kitabatake Y, Arao T, Ohashi Y. Report of the physical activity research of the Japan Arteriosclerosis Longitudinal Study. Research in Exercise Epidemiology, 5: 1-7, 2003. [Google Scholar]
- 23.Lund T, Labriola M, Christensen KB, Bültmann U, Villadsen E. Physical work environment risk factors for long term sickness absence: prospective findings among a cohort of 5357 employees in Denmark. BMJ, 332: 449-452, 2006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Bang Christensen K, Lund T, Labriola M, Villadsen E, Bültmann U. The fraction of long-term sickness absence attributable to work environmental factors: prospective results from the Danish Work Environment Cohort Study. Occup Environ Med, 64: 487-489, 2007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Andersen LL, Fallentin N, Thorsen SV, Holtermann A. Physical workload and risk of long-term sickness absence in the general working population and among blue-collar workers: prospective cohort study with register follow-up. Occup Environ Med, 73: 246-253, 2016. [DOI] [PubMed] [Google Scholar]
- 26.Andersen JH, Haahr JP, Frost P. Risk factors for more severe regional musculoskeletal symptoms: a two-year prospective study of a general working population. Arthritis Rheum, 56: 1355-1364, 2007. [DOI] [PubMed] [Google Scholar]
- 27.Krause N, Brand RJ, Kaplan GA, et al. Occupational physical activity, energy expenditure and 11-year progression of carotid atherosclerosis. Scand J Work Environ Health, 33: 405-424, 2007. [DOI] [PubMed] [Google Scholar]
- 28.Thielen K, Nygaard E, Andersen I, Diderichsen F. Employment consequences of depressive symptoms and work demands individually and combined. Eur J Public Health, 24: 34-39, 2014. [DOI] [PubMed] [Google Scholar]
- 29.Tsutsumi A, Nagami M, Yoshikawa T, Kogi K, Kawakami N. Participatory intervention for workplace improvements on mental health and job performance among blue-collar workers: a cluster randomized controlled trial. J Occup Environ Med, 51: 554-563, 2009. [DOI] [PubMed] [Google Scholar]
- 30.Horita Y, Otsuka Y. Relationships between workers’ interpersonal helping behavior, social supports, job stressors, psychological stress responses, and vigor in manufacturing industry. (in Japanese) Sangyo Eiseigaku Zasshi, 56: 259-267, 2014. [DOI] [PubMed] [Google Scholar]
- 31.Kusagai Y. Teachers’ thinking about leaves of absence and resignation: literature review and future issues. (in Japanese) Kokorono Kenkou, 33: 33-39, 2018. [Google Scholar]
- 32.Ministry of Education, Culture, and Sports, Science and Technology Mental health countermeasure for teachers. (in Japanese) http: //www.mext.go.jp/component/b_menu/shingi/toushin/__icsFiles/afieldfile/2013/03/29/1332655_03.pdf. Accessed 2019 June 21.