

Abstract
Purpose
Because of the anticipated surge in cases requiring intensive care unit admission, the high aerosol-generating risk of tracheal intubation, and the specific requirements in coronavirus disease (COVID-19) patients, a dedicated Mobile Endotracheal Rapid Intubation Team (MERIT) was formed to ensure that a highly skilled team would be deployed to manage the airways of this cohort of patients. Here, we report our intubation team experience and activity as well as patient outcomes during the COVID-19 pandemic.
Methods
The MERIT members followed a protocolized early tracheal intubation model. Over a seven-week period during the peak of the pandemic, prospective data were collected on MERIT activity, COVID-19 symptoms or diagnosis in the team members, and demographic, procedural, and clinical outcomes of patients.
Results
We analyzed data from 150 primary tracheal intubation episodes, with 101 (67.3%) of those occurring in men, and with a mean (standard deviation) age of 55.7 (13.8) yr. Black, Asian, and minority ethnic groups accounted for 55.7% of patients. 91.3% of tracheal intubations were performed with videolaryngoscopy, and the first pass success rate was 88.0%. The 30-day survival was 69.2%, and the median [interquartile range] length of critical care stay was 11 [6–20] days and of hospital stay was 12 [7–22] days. Seven (11.1%) MERIT healthcare professionals self-isolated because of COVID-19 symptoms, with a total 41 days of clinical work lost. There was one reported incident of a breach of personal protective equipment and multiple anecdotal reports of doffing breaches.
Conclusion
We have shown that a highly skilled designated intubation team, following a protocolized, early tracheal intubation model may be beneficial in improving patient and staff safety, and could be considered by other institutions in future pandemic surges.
Electronic supplementary material
The online version of this article (10.1007/s12630-020-01804-3) contains supplementary material, which is available to authorized users.
Keywords: intubation, COVID-19, tracheostomy
Résumé
Objectif
En raison de l’augmentation anticipée du nombre de cas nécessitant une admission à l’unité de soins intensifs, du risque élevé de génération d’aérosols de l’intubation trachéale et des exigences spécifiques aux patients atteints du coronavirus (COVID-19), nous avons créé une équipe mobile dédiée pour l’intubation trachéale rapide (MERIT - Mobile Endotracheal Rapid Intubation Team) afin de garantir qu’une équipe hautement qualifiée puisse être déployée pour prendre en charge les voies aériennes de cette cohorte de patients. Notre objectif était de rapporter l’expérience et l’activité de notre équipe d’intubation ainsi que les devenirs des patients pendant la pandémie de COVID-19.
Méthode
Les membres de l’équipe MERIT ont suivi un modèle d’intubation trachéale précoce basé sur un protocole. Pendant sept semaines autour du pic de la pandémie, des données prospectives ont été colligées concernant l’activité de la MERIT, les symptômes et diagnostics de COVID-19 parmi les membres de l’équipe, ainsi que les données démographiques, procédurales et les devenirs cliniques des patients.
Résultats
Nous avons analysé les données de 150 épisodes d’intubations trachéales initiales, dont 101 (67,3 %) survenus chez des hommes, avec un âge moyen (écart type) de 55,7 (13,8) ans. Les personnes noires, asiatiques et de minorités ethniques représentaient 55,7 % des patients. Au total, 91,3 % des intubations trachéales ont été réalisées par vidéolaryngoscopie, et le taux de réussite au premier essai était de 88,0 %. Le taux de survie à 30 jours était de 69,2 %, et la durée médiane (écart interquartile) de séjour aux soins intensifs était de 11 (6-20) jours et de 12 (7-22) jours à l’hôpital. Sept (11,1 %) professionnels de la santé de l’équipe MERIT se sont mis en auto-isolement en raison de symptômes de la COVID-19, pour un total de 41 jours de travail clinique perdus. Un incident de bris de stérilité de l’équipement de protection individuelle a été rapporté, et de multiples bris lors du déshabillage ont également été rapportés de façon anecdotique.
Conclusion
Nous avons démontré qu’une équipe d’intubation désignée et hautement qualifiée, respectant un modèle d’intubation trachéale précoce basé sur un protocole, pourrait contribuer à améliorer la sécurité des patients et du personnel. La création d’une telle équipe est envisageable dans d’autres établissements lors de futurs épisodes pandémiques.
On 31 December 2019 in Wuhan, China, a pneumonia of unknown cause was first reported to the World Health Organization. This pneumonitis was attributed to the novel severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) leading to coronavirus disease (COVID-19). As of 20 July 2020, more than 14 million cases of COVID-19 and nearly 600,000 deaths have been reported worldwide.1 The International Severe Acute Respiratory and emerging Infections Consortium (ISARIC) have reported that almost a fifth of patients who have been hospitalized need level 2 and 3 care2 and between 58% and 88% of patients admitted to critical care settings require tracheal intubation and mechanical ventilation.2–4 The Intensive Care National Audit and Research Centre (ICNARC) have reported a 51% mortality rate in patients admitted to critical care settings.5
Because of the rapid spread of the disease and the anticipated vast number of cases requiring hospital and intensive care unit (ICU) admission, we commenced surge planning at the end of February 2020 in our large multidisciplinary central London teaching hospital with a high consequence infectious diseases centre.6 This included the redeployment and training of anesthetic staff on COVID-19 patient management.7 Owing to the high aerosol-generating risk of tracheal intubation and the evolving specific considerations for COVID-19 patients, a dedicated Mobile Endotracheal Rapid Intubation Team (MERIT) was formed to ensure that a highly skilled team would be deployed to manage the airways of and provide excellent clinical care to these patients when it was most needed.
The outcomes of patients cared for by a specific airway team, along with the clinical activity and outcomes of intubation team members has not yet been reported. We therefore aimed to report both the MERIT experience and activity and patient outcomes over a seven-week period at our institution. These data will allow clinicians to understand pathways that may prove useful for subsequent pandemic surges.
Methods
As per the Health Research Authority Decision Tool and our institutional Research and Development Lead, formal application of ethical approval was waived for this service evaluation. We obtained approval from the Guy’s and St Thomas’ NHS Foundation Trust Audit and Quality Improvement Department, which was granted from 16 March 2020 to 3 August 2020 (Approval ID 10780). This study adhered to the strengthening reporting of observational studies in epidemiology (STROBE) checklist.8 We performed a prospective, observational, cohort study at a tertiary centre of patients with respiratory failure due to COVID-19 that required airway management between 23 March and 11 May 2020. This time period was selected as the interval during which the MERIT service was established, and the peak surge activity occurred. Inclusion criteria for patients were those who received a primary tracheal intubation, defined as the first episode of tracheal intubation for respiratory failure due to suspected or confirmed COVID-19 or requiring tracheal intubation for airway protection or cardiopulmonary resuscitation; and age ≥ 18 yr. We also included data on MERIT activity overall, which was any airway management episode that required the involvement of any members of the team, e.g., tracheostomy, tracheal tube change, awake tracheal intubation.
Our management of patients was standardized throughout the pandemic. We instituted a protocolized early tracheal intubation model, with predetermined ventilatory strategies thereafter. Tracheal intubation was considered when patients had peripheral oxygen saturations < 92%; inspired oxygen (FIO2) requirement of ≥ 60% via face mask; respiratory rate ≥ 25 breaths·min−1; and increased work of breathing or a failed four-hour trial of awake prone positioning. Non-invasive ventilation and high-flow nasal oxygen were not utilized in patients suitable for intubation. This institutional strategy was determined prior to the COVID-19 surge to minimize the risk of aerosol-generation, staff resource utilization, and high expected oxygen consumption of non-invasive techniques. All tracheal intubations were performed by MERIT, who recorded patient demographics, frequency of intubations, and procedural details and complications. Complications included hypotension (systolic blood pressure < 90 mmHg), desaturation (saturations < 90% after induction of anesthesia), dental damage (any damage or removal of teeth), bronchial intubation (clinical confirmation of the endotracheal tube in the right main bronchus), and failed intubation (unsuccessful insertion of an endotracheal tube). Patients were then transferred to, managed on, and followed up in the critical care unit. Data on staff exposure and self-isolation were collected by the investigating team, who were also the service delivery leads.
The tracheal intubation team consisted of 23 anesthesiologists (21 consultants and two advanced airway fellows) and 40 anesthetic assistants. All members of the intubating team were volunteers, and those who were sufficiently skilled, experienced, and had no health restrictions were selected; no members withdrew from this clinical responsibility. Each four-person team consisted of two anesthesiologists and two anesthetic assistants. For every 24-hr period, three teams were present, each covering a 13-hr shift from 08:00 to 21:00 and 20:00 to 09:00, and a further two teams present covering either a 08:00 to 18:00 or 10:00 to 21:00 shift, ensuring 24/7 cover across all hospital areas.
Each weekly rota consisted of seven anesthesiologists who would work resident shifts consisting of one long day (13 hr), one regular day (nine hours), and one night (13 hr), and a reserve night shift (to cover any periods of illness or self-isolation amongst other team members), and one day off (each night shift accounted for two days). There were three such rotas running in parallel throughout the study period and this rota was developed specifically to cover all airway interventions during the pandemic period. The MERIT members had no other clinical responsibilities during this time period, but would assist in ICU patient transfers and management of other emergency patients, if available. No routine surgical activity was undertaken by MERIT members throughout this period. All team members had knowledge of the protocols and were proficient in the clinical management of airway emergencies.
With safety of staff and patients prioritized, we established small-group in situ simulation training for all MERIT members. In situ training for all team members has been shown to be an effective strategy for building teamwork and managing crisis situations,9–11 and potentially improving clinical outcomes.12 Our training initially consisted of donning and doffing of personal protective equipment (PPE), followed by tracheal intubation drills and emergency front-of-neck airway skills. The drills included communication, ergonomics, the use of checklists, and team debriefings after each session.13 We designed a COVID-19–specific tracheal intubation checklist and action card given the paucity of national guidance at the time (eFigs 1–3, available as Electronic Supplementary Material). MERIT was designed to be a self-sufficient, rapidly mobile team, thus all team members had their own PPE available for every airway procedure they attended, including fit-tested FFP3 respirators, visors, long-sleeved gowns, and gloves.14
A single-use videolaryngoscope was the tracheal intubation device of choice,15 and included either the i-view videolaryngoscope (Intersurgical Ltd., Wokingham, UK) or the Airtraq® (Fannin, Dublin, Ireland). The videolaryngoscope was chosen because it potentially reduces the time to tracheal intubation, improves the first pass success rate, allows all team members to observe the laryngoscopic view, and increases the distance between the laryngoscopist and patient thereby reducing the risk of aerosol or droplet exposure.16–19 Nevertheless, individual anesthesiologists could opt to use an alternative device for clinical or other indications. A flexible bronchoscope was available in the event of a failed tracheal intubation20 and a single-use bronchoscope was chosen because the risk of patient cross-contamination is zero,21 they are portable and lightweight, and they are quicker and easier to set-up than reusable flexible bronchoscopes.22 For other airway management episodes such as awake tracheal intubation and tracheostomy insertion, standardized protocols were adhered to,23,24 although modifications were implemented to reduce the aerosol-generating potential, and advanced PPE was donned throughout.
Data on patients who received a primary tracheal intubation by the MERIT were collected on standardized data capture forms and transcribed to a Microsoft Excel (Microsoft, Inc., Redmond, WA, USA) spreadsheet. We analyzed the outcomes of patients who received primary tracheal intubation for COVID-19, and we also described other airway management episodes that MERIT were involved in, including reintubations, tracheal tube exchanges, or tracheostomy formation. Descriptive statistical analyses and Kaplan–Meier curves for survival for both the whole cohort and stratified by age quintiles were performed using R Version 4.0.0 (The R Foundation for Statistical Computing, Vienna, Austria), and continuous variables were reported as mean (standard deviation) or median [interquartile range (IQR)] as appropriate. A convenience sample over a seven-week period was selected.
Results
In total, 200 airway procedures were performed: primary tracheal intubations (n = 150); reintubations (n = 11); tracheal tube changes (n = 11); awake tracheal intubations (n = 2); and assisting with percutaneous (n = 24) and surgical tracheostomies (n = 2). All awake tracheal intubations and surgical tracheostomies were performed in the operating theatre, and all reintubations, tracheal tube changes, and percutaneous tracheostomies were performed in the ICU. There were no reported complications for any of these procedures. In total, 165 of the patients included in this study were confirmed to be COVID-19 positive, 127 of whom were patients receiving primary tracheal intubations, with the rest either being unknown or negative.
The nature of MERIT activity changed with time according to the demands of the pandemic. Initially, the primary demand was for de novo tracheal intubation, this was then followed by tracheal tube changes and reintubations, followed by assistance with tracheostomies (Fig. 3). Analyzing the distribution of workload over the 24-hr period allowed us to change the working pattern according to where the demand was highest. Ninety-six (64.0%) tracheal intubations were performed between 10:00 and 20:00 (Fig. 4), during which time we provided additional MERIT cover.
Fig. 3.

Overall activity of the intubation team by date during the study period. Blue, primary intubations; orange, reintubations; green, tracheal tube change; yellow, tracheostomy
Fig. 4.

The number of interventions performed by the intubation team at different times of the day
Seven (11.1%) MERIT members (five consultant anesthesiologists and two anesthetic assistants) had to self-isolate during the seven-week period because of COVID-19 symptoms (fever, anosmia, fatigue, cough, sore throat, myalgia) but none were hospitalized. This resulted in them being unavailable to work for a total of 41 days (mean 5.9 days). During the data collection period, there was limited availability of reverse transcriptase polymerase chain reaction testing for staff members, and thus a clinical diagnosis of COVID-19 was self-reported. No radiological investigations were undertaken in any of the MERIT members reporting a COVID-19 outcome. Three MERIT members who self-isolated because of symptoms consistent with COVID-19 subsequently had positive antibody tests. Causal episodes for SARS-CoV-2 transmission were unclear, but no exposures outside of the clinical setting were reported by team members. A single reported incidence of PPE breach was identified by one team member who did not wear a visor, but this clinician did not go on to report a COVID-19 outcome. For all other interventions, full PPE was used throughout exposure periods. There were multiple anecdotal episodes of PPE breaches reported during doffing (e.g., inadvertent skin contact with contaminated items, incorrect order of doffing, clothing contamination). As these breaches were not anticipated a priori, we did not formally collect and assess data on this aspect of personal protection.
We analyzed data from 150 patients (Table 1) who received primary intubations by MERIT. The median [IQR] time from hospital admission to tracheal intubation was 1 [0–2] day. For tracheal intubations performed within the emergency department, the median time from admission to intubation was 67 [43–136] min. Prior to tracheal intubation, the mean (SD) FIO2 was 82 (25)%, arterial oxygen saturations 92 (7)%, and respiratory rate 31 (10) breaths·min−1.
TABLE 1.
Baseline demographics and comorbidities of patients who underwent emergency intubation. Data are n (%) or mean (SD)
| Overall (n = 150) | |
|---|---|
| Males | 101 (67.3%) |
| Age (yr) | 55.7 (13.8) |
| Ethnicity | |
| Asian | 11 (7.4%) |
| Black | 54 (36.2%) |
| Mixed | 2 (1.3%) |
| White | 66 (44.3%) |
| Other | 16 (10.7%) |
| Body mass index (kg·m−2) | 29.8 (6.8) |
| Diabetes | 57 (38.3%) |
| Hypertension | 67 (45.0%) |
| Ischemic heart disease | 9 (6.0%) |
| Chronic obstructive pulmonary disease | 8 (5.4%) |
| Asthma | 21 (15.1%) |
| Hypercholesterolemia | 33 (22.1%) |
| Obstructive sleep apnea | 8 (5.4%) |
| Chronic kidney disease | 9 (6.1%) |
| Smoker | 4 (2.8%) |
| Obesity | 57 (38.3%) |
| Location of intubation | |
| Critical care area | 17 (11.3%) |
| Emergency department | 56 (37.3%) |
| Other | 77 (51.3%) |
SD = standard deviation
Of the 150 primary tracheal intubations in which procedural data were included, the majority of patient’s tracheas were intubated with the assistance of videolaryngoscopy (n = 137, 91.3%) (eFig. 4, available as ESM), and 88% were intubated successfully at the first attempt. Facemask ventilation was performed in 5/150 (3.3%) patients during the tracheal intubation process with supraglottic airway devices being used in 7/150 (4.7%) patients; four of these were in patients having cardiopulmonary resuscitation and the supraglottic airway devices were inserted before MERIT arrived because of clinical urgency not lack of MERIT availability. There were no cases where patients were intubated due to delay in the arrival of MERIT. Complications reported for primary tracheal intubations are shown in Fig. 1. There were three deaths reported during the immediate period of the intubation episode, all of whom were patients already undergoing cardiopulmonary resuscitation when MERIT were called; the time of death in these three cases was reported once resuscitation had ceased.
Fig. 1.
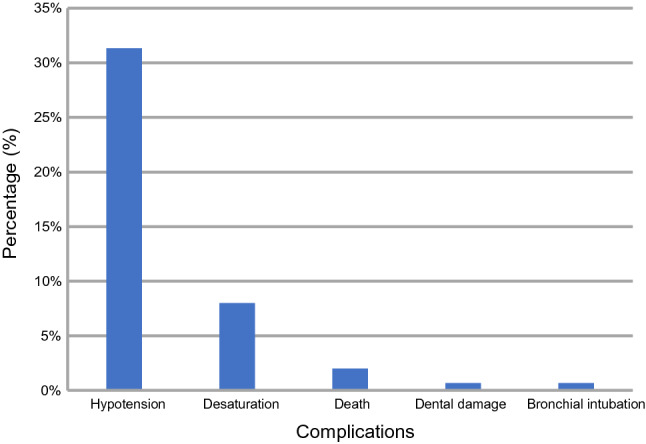
The incidence of complications of primary tracheal intubations performed by the intubation team. Hypotension was defined as systolic blood pressure < 90 mmHg, desaturation as saturations < 90% after induction of anesthesia, dental damage as any damage or removal of teeth, and bronchial intubation as clinical confirmation of the endotracheal tube in the right main bronchus
At analysis, all 150 patients had at least 30 days elapse since their initial tracheal intubation. Of these, 46 (30.66%) patients died, 50 (33.33%) remained in hospital, and 54 (36%) were discharged home, with a median [IQR] length of critical care stay of 9 [5–13.65] days and hospital length of stay of 11.5 [8.0–17.0] days. A tracheostomy was inserted in 33 (27.3%) of patients, and prone position ventilation in 53 (39.3%) patients, with 48 (35.0%) patients requiring renal replacement therapy. Kaplan–Meier curves for the whole cohort and stratified by age are shown in Fig. 2. There was no difference in survival between men and women (log-rank test, P = 0.82).
Fig. 2.
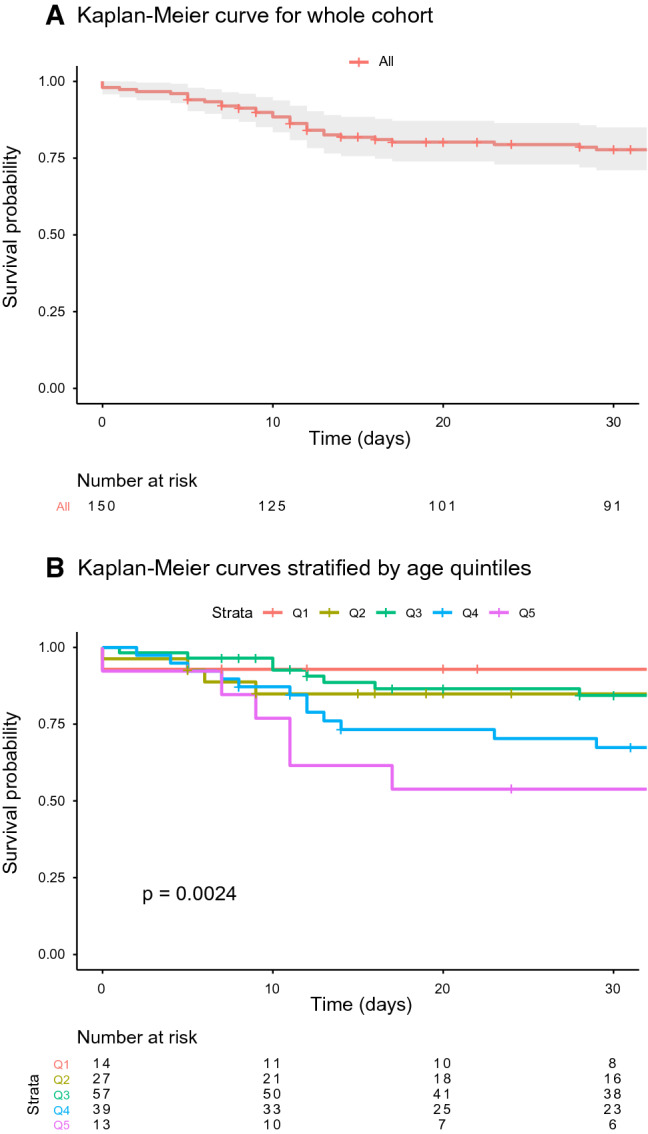
Kaplan–Meier survival curves (a) for the whole cohort, (b) stratified by age. Age strata are in quintiles; Q1 = youngest quintile, Q5 = oldest quintile
Discussion
We report a prospective, observational cohort study of patients with COVID-19 requiring tracheal intubation, with an overall 30-day survival of approximately 70%. We show that an early tracheal intubation strategy performed by specialist teams, along with protocolized ventilatory management, can be associated with favourable patient outcomes. We have outcomes that appear superior to the ICNARC data set, which reports 51% overall mortality and 65% mortality in patients receiving advanced respiratory support.5 Whilst our data do not provide definitive evidence for early vs late intubation, and influences on outcomes were likely multifactorial, our data suggests that this strategy may have contributed to positive clinical outcomes in our cohort.
The ISARIC study reported that, of the 17% of patients who were admitted into an ICU or high-dependency unit, 33.1% died, with a mean length of ICU stay of 10.8 days.2 In their report, the mean and median durations from admission to tracheal intubation (or receiving invasive mechanical ventilation) were 3.6 days and two days respectively. We therefore intubated patients relatively early in their hospital course, and physiologic parameters were acceptable, but our outcome data are comparable. That said, there are several differences in both clinical management and demographics that precludes direct comparison with international, multicentre data sets such as the ISARIC study. Firstly, we present single-centre data that reflect standardized protocols, training, and clinical management, which is juxtaposed with the diversity in management strategies in the ISARIC study. Secondly, it is unclear if specialized intubation teams were involved in patient care in centres included in the ISARIC study, nor of the make-up, experience, or standards they may have operated to. Thirdly, our patient demographics varied from the ISARIC database. Although our patients were younger (56 yr vs 73 yr), we had more male (67% vs 57%) and fewer white patients (44% vs 83%).
There are a number of controversies surrounding tracheal intubation of patients presenting with COVID-19 pneumonitis, such as whether they should have their tracheas intubated (particularly in the early stages), the optimal technique, and patient outcomes. With a paucity of high-quality clinical data supporting or refuting early tracheal intubation strategies, this debate remains nuanced and inconclusive.25–27 Tracheal intubation of critically ill patients is a high-risk procedure, particularly in patients with severe COVID-19.20 A 10.4% mortality rate within 24 hr of intubation has been reported in a retrospective observational study from two centres in China, with international experts recommending optimization of tracheal intubation; however, the outcome data in that report was only limited to 24 hr after tracheal intubation.28 We instituted a tracheal intubation protocol and simulation training program prior to establishing the MERIT service and our first pass success rate and videolaryngoscopy utilization was similar to that reported by Yao et al., yet our outcomes were superior.28 We therefore surmise that intervention before significant physiologic decompensation could have potentially contributed to our comparatively successful clinical management.
We report 11.1% of the MERIT members requiring self-isolation during the seven-week study period. El-Boghdadly et al. found that approximately one in ten healthcare workers involved in tracheal intubation of patients with or suspected of COVID-19 subsequently reported symptoms or laboratory-confirmed COVID-19 diagnosis.15 That study reported 5,148 intubation episodes across 17 countries involving assistants and intubators and acknowledge that the exposure source may not just be attributed to the tracheal intubation episode. Despite our MERIT members being exposed to multiple intubations, the rate of healthcare workers self-isolating because of suspected or confirmed COVID-19 is similar to that reported by El-Boghdadly et al. That said, the utilization of adequate PPE was greater in this current study compared with the data presented by El-Boghdadly et al.; thus, one might expect the rates of COVID-19 transmission to healthcare workers to be lower in our institutional cohort. Nevertheless, the data from El-Boghdadly et al. show that the use of PPE was not associated with decreased risk of transmission, so the reasons for the rates of MERIT-reported COVID-19 remain uncertain. Moreover, the availability and use of PPE is merely one element of personal protection. Despite wearing adequate PPE, our anecdotal findings of PPE breaches, particularly during the doffing process, suggests that healthcare workers could still potentially be exposed to SARS-CoV-2. As noted previously, a causal association between tracheal intubation and COVID-19 in MERIT members cannot be determined, as there are multiple potential sources of infection (e.g., public transport, family members, other workplace-related exposures). Overall, the flexibility that was built into our clinical service provision ensured consistent delivery of MERIT activity was maintained despite the loss of more than a tenth of our workforce due to self-isolation, suggesting this was an important component of our approach.
The favourable outcome data reported in this study also highlights the potential advantages of establishing a highly skilled and well-drilled team to manage the intubations in a pandemic where there is a rapid surge in the number of cases over a short duration. Had we taken a week longer to establish this service, then just over 15% of the intubations would have already occurred (Fig. 4). By being an independent, flexible team, we were also able to adapt the service according to the demand and provide additional cover during the busiest times. The nature of the service also changed with time from primary intubations to assisting with tracheostomies (Fig. 4). This would not have been possible if the team were inexperienced or inflexible, highlighting the importance of team composition (Fig. 3).
Limitations of this study are that it was an uncontrolled single-centre study, provided no comparative data, and had conservative patient numbers. We are unable to draw definitive conclusions about the impact of our intubation team on patient outcomes given the multidimensional aspects of their care. Strengths include the consistent adherence to protocolized care, and patient demographics that are representative of larger data sets.
In conclusion, our data show that early tracheal intubation of patients with COVID-19 using a designated skilled team following a protocolized approach may contribute to favourable outcomes for patients, staff, and institutions. This can be achieved by establishing and training a designated mobile and self-sufficient tracheal intubation team.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Acknowledgments
Author contributions
Imran Ahmad, Kariem El-Boghdadly contributed to the study conception and design and manuscript preparation. Jeyanjali Jeyarajah, Ganeshkrishna Nair, Sophie Ragbourne, and Benjamin Vowles contributed to the data collection. Danny J. N. Wong, Kariem El-Boghdadly, and Ganeshkrishna Nair contributed to the statistical analysis. All authors contributed to manuscript amendment.
Acknowledgement
I would like to dedicate this study to my late father, Mr Daud Ahmad, who sadly passed away of COVID-19 pneumonitis during the conduct of this study at our hospital. We miss you dearly and your memory lives long in our hearts, may you forever rest in peace.
Disclosures
Imran Ahmad has previously received honoraria and educational funding from Fisher & Paykel Healthcare Ltd., Ambu, BioMarin, and Verathon Medical. Kariem El-Boghdadly has received educational and research funding from Fisher & Paykel Healthcare Ltd., GE Healthcare, and Ambu. These have no influence on the submitted work. No other conflicts of interest were declared.
Funding statement
None.
Editorial responsibility
This submission was handled by Dr. Alana M. Flexman, Associate Editor, Canadian Journal of Anesthesia.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.World Health Organization. Coronavirus disease (COVID-19) pandemic. Latest updates. Available from URL: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed August 2020).
- 2.International Severe Acute Respiratory and emerging Infection Consortium. COVID-19 Clinical Research Resources. Available from URL: https://isaric.tghn.org/covid-19-clinical-research-resources (accessed August 2020).
- 3.Arentz M, Yim E, Klaff L, et al. Characteristics and outcomes of 21 critically ill patients with COVID-19 in Washington State. JAMA. 2020;323:1612–1614. doi: 10.1001/jama.2020.4326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Grasselli G, Zangrillo A, Zanella A, et al. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy region. Italy. JAMA. 2020;323:1574–1581. doi: 10.1001/jama.2020.5394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Intensive Care National Audit and Research Centre. COVID-19 Report. Available from URL: https://www.icnarc.org/Our-Audit/Audits/Cmp/Reports (accessed August 2020).
- 6.Arabi YM, Murthy S, Webb S. COVID-19: a novel coronavirus and a novel challenge for critical care. Intensive Care Med. 2020;46:833–836. doi: 10.1007/s00134-020-05955-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Carenzo L, Costantini E, Greco M, et al. Hospital surge capacity in a tertiary emergency referral centre during the COVID-19 outbreak in Italy. Anaesthesia. 2020;75:928–934. doi: 10.1111/anae.15072. [DOI] [PubMed] [Google Scholar]
- 8.von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2020;61:344–349. doi: 10.1016/j.jclinepi.2007.11.008. [DOI] [PubMed] [Google Scholar]
- 9.Goldhaber-Fiebert SN, Howard SK. Implementing emergency manuals: can cognitive aids help translate best practices for patient care during acute events? Anesth Analg. 2013;117:1149–1161. doi: 10.1213/ANE.0b013e318298867a. [DOI] [PubMed] [Google Scholar]
- 10.Schmutz J, Manser T. Do team processes really have an effect on clinical performance? A systematic literature review. Br J Anaesth. 2013;110:529–544. doi: 10.1093/bja/aes513. [DOI] [PubMed] [Google Scholar]
- 11.Marshall SD, Touzell A. Human factors and the safety of surgical and anaesthetic care. Anaesthesia. 2020;75(Suppl 1):e34–e38. doi: 10.1111/anae.14830. [DOI] [PubMed] [Google Scholar]
- 12.Draycott T, Sibanda T, Owen L, et al. Does training in obstetric emergencies improve neonatal outcome? BJOG. 2006;113:177–182. doi: 10.1111/j.1471-0528.2006.00800.x. [DOI] [PubMed] [Google Scholar]
- 13.Russ SJ, Sevdalis N, Moorthy K, et al. A qualitative evaluation of the barriers and facilitators toward implementation of the WHO surgical safety checklist across hospitals in England: lessons from the “Surgical Checklist Implementation Project”. Ann Surg. 2015;261:81–91. doi: 10.1097/SLA.0000000000000793. [DOI] [PubMed] [Google Scholar]
- 14.Cook TM. Personal protective equipment during the coronavirus disease (COVID) 2019 pandemic – a narrative review. 2020; 75: 920-7. [DOI] [PubMed]
- 15.El-Boghdadly K, Wong DJ, Owen R, et al. Risks to healthcare workers following tracheal intubation of patients with COVID-19: a prospective international multicentre cohort study. Anaesthesia. 2020 doi: 10.1111/anae.15170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hall D, Steel A, Heij R, Eley A, Young P. Videolaryngoscopy increases ‘mouth-to-mouth’ distance compared with direct laryngoscopy. Anaesthesia. 2020;75:822–823. doi: 10.1111/anae.15047. [DOI] [PubMed] [Google Scholar]
- 17.Wilson NM, Norton A, Young FP, Collins DW. Airborne transmission of severe acute respiratory syndrome coronavirus-2 to healthcare workers: a narrative review. Anaesthesia. 2020;75:1086–1095. doi: 10.1111/anae.15093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Lewis SR, Butler AR, Parker J, et al. Videolaryngoscopy versus direct laryngoscopy for adult patients requiring tracheal intubation. Cochrane Database Syst Rev. 2016 doi: 10.1002/14651858.CD011136.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Cook TM, Boniface NJ, Seller C, et al. Universal videolaryngoscopy: a structured approach to conversion to videolaryngoscopy for all intubations in an anaesthetic and intensive care department. Br J Anaesth. 2018;120:173–180. doi: 10.1016/j.bja.2017.11.014. [DOI] [PubMed] [Google Scholar]
- 20.Cook TM, El-Boghdadly K, McGuire B, McNarry AF, Patel A, Higgs A. Consensus guidelines for managing the airway in patients with COVID-19: guidelines from the Difficult Airway Society, the Association of Anaesthetists the Intensive Care Society, the Faculty of Intensive Care Medicine and the Royal College of Anaesthetists. Anaesthesia. 2020;75:785–799. doi: 10.1111/anae.15054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Mouritsen JM, Ehlers L, Kovaleva J, Ahmad I, El-Boghdadly K. A systematic review and cost effectiveness analysis of reusable vs. single-use flexible bronchoscopes. Anaesthesia 2020; 75: 529-40 [DOI] [PMC free article] [PubMed]
- 22.Krugel V, Bathory I, Frascarolo P, Schoettker P. Comparison of the single-use Ambu® aScopeTM 2 vs the conventional fibrescope for tracheal intubation in patients with cervical spine immobilisation by a semirigid collar. Anaesthesia. 2013;68:21–26. doi: 10.1111/anae.12044. [DOI] [PubMed] [Google Scholar]
- 23.Ahmad I, El-Boghdadly K, Bhagrath R, et al. Difficult Airway Society guidelines for awake tracheal intubation (ATI) in adults. Anaesthesia. 2020;75:509–528. doi: 10.1111/anae.14904. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Takhar A, Walker A, Tricklebank S, et al. Recommendation of a practical guideline for safe tracheostomy during the COVID-19 pandemic. Eur Arch Otorhinolaryngol. 2020;277:2173–2184. doi: 10.1007/s00405-020-05993-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Tobin MJ, Laghi F, Jubran A. Caution about early intubation and mechanical ventilation in COVID-19. Ann Intensive Care. 2020 doi: 10.1186/s13613-020-00692-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Marini JJ, Gattinoni L. Management of COVID-19 respiratory distress. JAMA. 2020 doi: 10.1001/jama.2020.6825. [DOI] [PubMed] [Google Scholar]
- 27.Gattinoni L, Coppola S, Cressoni M, Busana M, Rossi S, Chiumello D. COVID-19 does not lead to a “typical” acute respiratory distress syndrome. Am J Respir Crit Care Med. 2020;201:1299–1300. doi: 10.1164/rccm.202003-0817LE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Yao W, Wang T, Jiang B, et al. Emergency tracheal intubation in 202 patients with COVID-19 in Wuhan, China: lessons learnt and international expert recommendations. Br J Anaesth. 2020;125:e28–e37. doi: 10.1016/j.bja.2020.03.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.