

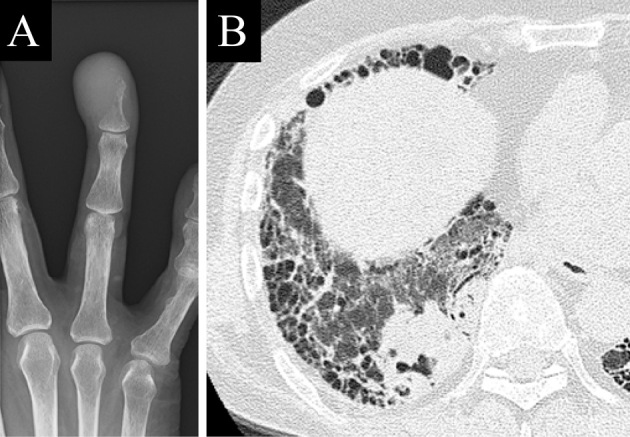
A 70-year-old man with rheumatoid arthritis and interstitial pneumonia presented to our hospital with swelling of the right third finger (Picture 1). His past medical history was significant, with pulmonary tuberculosis and diabetes mellitus secondary to oral prednisolone treatment. An X-ray of the right hand showed osteolysis of the distal phalange (Picture 2A). Chest computed tomography revealed interstitial pneumonia and a cavitary lesion in the right lower lung (Picture 2B). A biopsy of the phalange revealed squamous cell carcinoma and other examinations, including a test for tuberculosis, were negative. Subsequently, sputum cytology also showed squamous cell carcinoma, which was compatible with acrometastasis of lung cancer. Acrometastasis, defined as bone metastasis located distal to the elbow and knee, accounts for 0.1% of all metastatic bone lesions (1). Although acrometastasis is infrequent, clinicians should be aware of this type of metastasis because it is sometimes difficult to distinguish with tuberculous dactylitis and other osteomyelitis in patients with undiagnosed cancer (1,2).
Picture 1.

Picture 2.
The authors state that they have no Conflict of Interest (COI).
References
- 1. Stomeo D, Tulli A, Ziranu A, et al. Acrometastasis: a literature review. Eur Rev Med Pharmacol Sci 19: 2906-2915, 2015. [PubMed] [Google Scholar]
- 2. Sahoo TK, Das SK, Majumdar SK, Senapati SN, Parida DK. Digital acrometastasis as initial presentation in carcinoma of lung a case report and review of literature. J Clin Diagn Res 10: XD01-XD02, 2016. [DOI] [PMC free article] [PubMed] [Google Scholar]