

Abstract
Objectives:
The purpose of this study was to examine the association between abnormal hemoglobin (Hb) level and stroke severity (as assessed by the National Institutes of Health Stroke Scale [NIHSS]). The study further aimed to describe the demographic and clinical characteristics of stroke patients in the middle region of Saudi Arabia.
Methodology:
We performed a retrospective review of all medical records of the stroke patients who were treated at a major hospital in Qassim province between 2016 and 2018. Reviewed data (n = 400) included demographics, Hb level on admission, type of stroke (ischemic vs. hemorrhagic), stroke risk factors, and NIHSS scores. Analysis of variance (ANOVA) test was used to assess the univariate association between NIHSS and Hb level. Regression statistics were utilized to examine the effect of abnormal Hb level on NIHSS scores while controlling for the other study variables. Data were analyzed using Statistical Package for the Social Sciences.
Results:
Sixty-nine percent of the patients were men. More young women than men (≤39 years) had a stroke. Ischemic stroke is considerably more common than hemorrhagic stroke (a ratio of 12.7:1). ANOVA test showed that the mean score of NIHSS was significantly lower among patients with a normal Hb level. Regression showed that NIHSS scores were significantly associated with abnormal Hb level, in terms of low and high level.
Conclusions:
This study demonstrated further evidence of the association between abnormal Hb level NIHSS. Thus, our results emphasize the predictive importance of Hb level on identifying individuals who might be at higher risk of worse neurological outcomes after stroke. Physicians need to be cognizant of the negative effect of abnormal Hb level on the outcomes of stroke patients.
Keywords: Abnormal hemoglobin levels, Saudi Arabia, severity, stroke
Introduction
Stroke is rated the second leading cause of mortality and one of the biggest causes of long-term disability all over the world.[1] Stroke is a common health problem in Saudi Arabia (SA). In 2014, a study found that the incidence of stroke in SA was 30 cases per 100,000 people per year.[2] A more recent study in 2018 reported a higher incidence of stroke among Saudis (57.64 cases per 100,000 people per year).[3] Similar to the case in the U.S,[4] there is a similarity in the regional variation of stroke rates in SA. A study by Alahmari and Paul in 2016 found that Al-Qassim region was among the top regions in SA in the prevalence of stroke along with Qunfudhah, Al Hassa, and Jazan regions.[5]
Stroke is defined as the rapid loss of brain function due to a disturbance in the blood supply to the brain.[6] A stroke happens when a part of the brain has an insufficient or interrupted blood supply and decreased oxygenation and nutrition to brain tissue.[7] Ischemic and hemorrhagic strokes are believed to have opposite mechanisms. Ischemic stroke, which is comparatively more common than hemorrhagic stroke, is characterized by limitation of blood supply to the brain, whereas hemorrhagic is described by the presence of too much blood within the closed cranial cavity tissue.[6,7]
Multiple risk factors, with various magnitudes, have been identified to be associated with increased risk of acute stroke, including age, gender, hypertension, diabetes mellitus, dyslipidemia, obesity, cardiovascular disease, smoking, and previous stroke.[8] On the other hand, additional coexisting conditions may increase stroke severity, resulting in worse outcomes in terms of both mortality and disabilities. Among these conditions are the accompanying abnormal (low or high) hemoglobin (Hb) levels. Hb has a direct relation with blood supply and the delivery of oxygen to the central nervous system.[9] A substantial body of research revealed that low Hb level on admission (i.e., anemia) among stroke patients was associated with more severe stroke.[9-17] Furthermore, a pilot study on the association between baseline Hb at the time of stroke and discharge destination showed that midrange levels were associated with a better discharge outcome.[18] Contrasting the low-Hb level, the effect of high Hb-level on stroke severity has been less frequently addressed in the scientific literature.[9-17] Yet, most available studies revealed that high Hb level on admission among stroke patients was also associated with more severe stroke.[11,12,16,17]
The economic burden of stroke on health-care systems is high. According to the latest report by the center for disease control and prevention care for stroke, in the U.S, stroke survivors were estimated to cost 18.8 billion dollars in a single year in addition to 15.5 billion dollars as a result of premature mortality and loss of productivity.[4] There are no clear data on the economic burden of stroke in SA; nevertheless, the burden is expected to be high, especially while rehabilitation therapy is included in the public insurance system.
This study aimed to examine the association between abnormal Hb level and stroke severity (National Institutes of Health Stroke Scale [NIHSS] scores) and among Saudi stroke patients. The study further aimed to describe the demographic and clinical characteristics of stroke patients in the middle region of SA.
Methodology
This is a retrospective review of the medical records of stroke patients (n=400), who were treated at King Fahad Specialist Hospital (KFSH) in Al-Qassim region from 2016 to 2018. Patients younger than 18 years of age were excluded from the study. This exclusion criterion was applied owing to the extremely low number of cases among this age group (n = 2). Accordingly, the total number of studied stroke cases was 398.
Ethical approval to review the KFSH records was obtained from the Qassim Region Research Ethics Committee.
The reviewed data included two demographic variables: gender and age. The variable of age was further categorized into four groups (18–39 years=1; 40–59 years=2; 60–79 years=3; 80 years or more=4). In addition, the type of stoke was determined (ischemic=1, hemorrhagic=2). Hb level on admission in grams per deciliter (g/dL) was measured as a continuous variable and later converted to three categorical variables in accordance with Mayo Clinic’s (low ≤12 g/dl for females and <13.5 g/dL for males; normal=12–15.5 g/dL for females and 13.5–17.5 g/dl for males; and high ≥5.5 g/dL for females and > 17.5 g/dL for males).[19] The severity of stroke was assessed using the NIHSS,[20] which ranges from 1 to 42, with higher scores signifying more severe adverse effects.
Statistical analysis
The reviewed data were coded and entered into an excel spreadsheet for initial editing, and then exported to Statistical Package for the Social Sciences (SPSS) version 20 (IBM SPSS, Inc Chicago IL, USA) for statistical analysis. Proper descriptive statistics, based on the type of variables (continuous/categorical), was employed to provide an overall picture of the stroke patients. Gender differences were assessed using independent samples t-test for continuous variables and Chi-square test (χ2) for categorical variables. General linear model analysis of variance (ANOVA) was used to assess the Univariate association between Hb level (low, normal, and high) and stroke severity (NIHSS scores). Multiple regression analysis was performed to identify the influence of Hb level on stroke severity. Before analysis, all categorical variables were coded into dummy variables. For example, a risk factor was coded (1) when it was present, and coded (0) when it was absent (reference group). Age, dummy-coded gender, and dummy-coded stroke risk factors were entered in the first step as controlled variables, whereas the Hb level was entered in the second step. A P =0.05 was considered statistically significant.
Results
Demographic and clinical characteristics of stroke patients
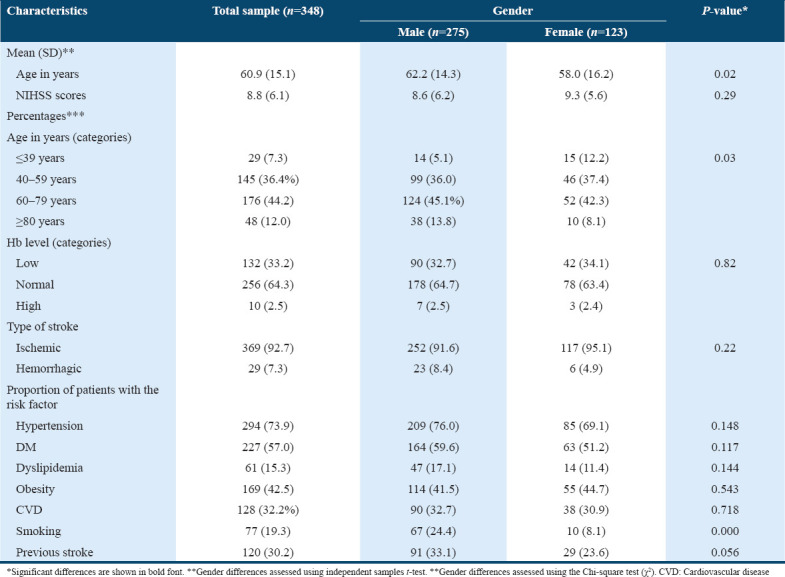
Approximately two-thirds of the patients (69.1%) were males (male to female ratio was 2.2:1). The mean age of the stroke patients was 60.1 years and the most dominant age group was 60–79 years. The mean Hb level was 13.2 g/dL. Furthermore, around one-third of the patients (33.2%) had anemia on admission, whereas 2.5% had above normal Hb level. The mean NIHSS total score was 8.8 (SD = 6.1). Our results showed that ischemic stroke is much more common than hemorrhagic one (a ratio of 12.7:1).
Concerning gender differences in characteristics of stroke patients, there were only two significant differences revealed. First, younger females (39 years of age or younger) and older males (80 years of age or older) were more likely to experience stroke events than their counterparts. Second, males were more likely to be smokers than females. Table 1 summarizes the demographic and clinical characteristics of stroke patients in addition to gender differences.
Table 1.
Characteristics of the stroke patients according to their gender
Association between Hb level and stroke severity
Table 2 shows the result of ANOVA test and Tukey’s post hoc test in NIHSS scores according to Hb level (low, normal, and high). The results revealed that the mean score of NIHSS was significantly lower among patients with normal Hb levels, in other words, abnormally low and high Hb levels were associated with more severe stroke.
Table 2.
Univariate association between Hb level and stroke severity
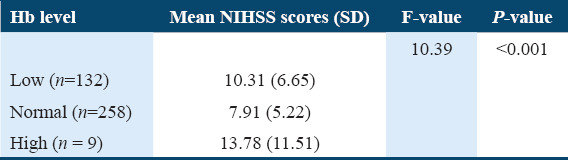
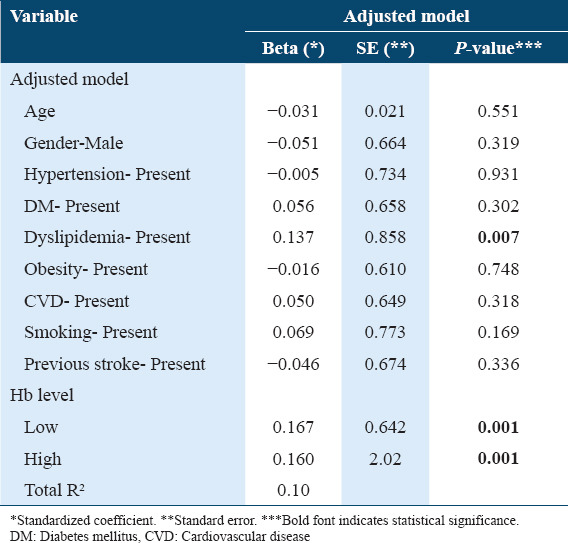
Table 3 summarizes the bivariate association of NIHSS scores with Hb level while controlling for the other variables. The results showed that NIHSS scores were significantly associated with abnormal Hb level in terms of low and high levels with a predictive value of 10%.
Table 3.
Multiple linear regression analysis of Hb level on stroke severity
Discussion
In accordance with previous data from SA,[2] Saudi men have more strokes than women (men-to women ration=2.2/1). Remarkably, the opposite trend arises from U.S studies.[21] According to Bushnel et al., more American women are experiencing strokes than men as female life expectancy at birth is higher than that of males.[21]
Concerning the age of onset, the mean age of our population was 60.9 years, which is far younger than the average age of presentation in the U.S population with the average age being 69.3 years.[22] This variation may be partly attributed to the differences in life expectancy between the two countries.
Concerning the type of stroke, our results revealed a bigger difference in the ratio between ischemic and hemorrhagic stroke (12.7/1) compared to two local studies in the early nineties with ratios of 3.2/1 and 6.7/1.[23,24] The arising dominance of ischemic stroke over the hemorrhagic one might be attributed to the socioeconomic changes which SA has been witnessing for the past few decades. These changes have resulted in alteration in lifestyles, including lack of exercise and an unhealthy diet, which led to the high prevalence of obesity, hypertension, and diabetes.[25] The notation that half of the stroke-related deaths are attributable to poor management of the controllable risk factors[26] highlights the need to better management strategies of stroke risk factors.
Our results showed that women were more likely than men to have a stroke in the age group of 39 years or younger. This finding is inconsistent with data from U.S,[21] which reported that men have strokes at younger ages compared to women. Further national research is needed to explain why these differences occur. In general, there are variations in the rates of stroke by both age group and gender by age group. Therefore, it is recommended to collect data based on age-specific rates by gender to facilitate the interpretation of stroke trends in the targeted population.[22]
The results of this study demonstrate evidence of the association between Hb level and stroke severity. Patients with abnormal Hb levels at the time of admission (low and high) were more likely to experience more severe strokes, whereas patients with midrange Hb levels were less likely to experience severe strokes. The adverse effects of low-Hb level (anemia) on stroke severity have been addressed in multiple previous studies. Milionis et al.[15] found that anemia on presentation was a significant predictor of adverse outcomes among stroke patients. Moreover, higher mortality rates were reported among stroke patients with anemia on admission.[11-13,16] Contrasting the low-Hb level, the effect of high Hb-level on stroke severity has not been adequately addressed in the scientific literature. Among available studies, Furlan et al. concluded that a high Hb level on admission was associated with more morbidity and mortality, in addition to a longer hospital stay.[12] Moreover, a recent systematic review and meta-analysis analysis of UK regional registry data revealed an association between mortality and abnormally high Hb on presentation and among stroke patients.[11] Consistent with our hypothesis, three previous studies reported a nonlinear association between stroke severity and Hb level.[12,16,17] Naess et al. in their recent study explored a U-shaped association between stroke severity and Hb level, which were evident in the Lowess smoother curves.[17] In addition, Tanne et al. found that the risk of mortality in stroke patients increases at both extremes of Hb levels.[16] The results of the study of Furlan et al. also indicated nonlinearity in the influence of abnormal Hb level in mortality in stroke patients (according to the resulted Kaplan-Meier curves).[12]
As the study has significantly demonstrated that abnormal Hb level is linked to a poorer outcome for stroke patients, it is imperative to identify subjects at high risk and optimize the management. At present, there is insufficient evidence to provide strong recommendations regarding which Hb level to be targeted, and which transfusion strategy to use (indication vs. contraindication). A randomized trial is needed to confirm the benefit and safety of any therapy before we consider it. For stroke patients with high Hb level, if the etiology is hyperviscosity, then hemodilution with venesection may be the safest acute treatment.
There were limitations to our study. We had only one baseline measurement of Hb level. Therefore, we were not able to determine whether long-term changes in Hb level were associated with stroke risk. Furthermore, we did not categorize anemia according to its types. Moreover, we did not collect data on stroke “non-survivors” from the included population. Such data could have provided further comparisons on the patient’s characteristics, especially the accompanying Hb level. Nevertheless, our study has a major strength, namely being the first study in SA, and maybe in the Middle East, to address the relationship between Hb level and NIHSS.
Conclusion
Our study demonstrated an association between abnormal Hb level (both low level and high level) and the severity of stroke. It may be important to treat anemia in the presence of acute stroke because this treatment will improve the delivery of oxygen to the brain. Future research may include the examination of whether giving blood transfusion/treating a high Hb level will help and mentioning in improving the severity of stroke and mortality rate.
Authors’ Declaration Statements
Ethics approval and consent to participate
Ethical approval obtained from Regional Committee of Bio-Ethics (REC) Qassim Region. The study was approved by the Institutional Ethics Committee.
Availability of data and material
Data and material available upon request.
Competing interests
None declared.
Funding Statement
No funding sources.
Author’s Contribution
NA participated in literature review, writing the manuscript, overall review of the whole paper; MSA and STA participated in data collection, data entry, literature review, writing the introduction.
Acknowledgment
We would like to acknowledge the data collectors: Marwa Moslih Alharbi, Mahamadallah Al-Harbi, Muna Abdulaziz Almijmaj, Lama Nasser Hameed, and Meaad Hamad Alkhyari.
References
- 1.Katan M, Luft A. Seminars in Neurology. Vol. 38. United States: Thieme Medical Publishers; 2018. Global burden of stroke; pp. 208–11. [DOI] [PubMed] [Google Scholar]
- 2.Asirvatham AR, Marwan MZ. Stroke in Saudi Arabia:A review of the recent literature. Pan Afr Med J. 2014;17:14. doi: 10.11604/pamj.2014.17.14.3015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Alhazzani AA, Mahfouz AA, Abolyazid AY, Awadalla NJ, Katramiz K, Faraheen A, et al. In hospital stroke mortality:Rates and determinants in Southwestern Saudi Arabia. Int J Environ Res Public Health. 2018;15:927. doi: 10.3390/ijerph15050927. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Cassel CK, Ek K. Functional Neurobiology of Aging. United States: Academic Press; 2001. Demography and epidemiology of age-associated neuronal impairment; pp. 31–50. [Google Scholar]
- 5.Alahmari K, Paul SS. Prevalence of stroke in Kingdom of Saudi Arabia-through a physiotherapist diary. Mediter J Soc Sci. 2016;7:228. [Google Scholar]
- 6.Chang YL, Hung SH, Ling W, Lin HC, Li HC, Chung SD. Association between ischemic stroke and iron-deficiency anemia:A population-based study. PLoS One. 2013;8:e82952. doi: 10.1371/journal.pone.0082952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sims NR, Muyderman H. Mitochondria, oxidative metabolism and cell death in stroke. Biochim Biophys Acta. 2010;1802:80–91. doi: 10.1016/j.bbadis.2009.09.003. [DOI] [PubMed] [Google Scholar]
- 8.Zahari WN, Supriyanto E, Mahmud N. Stroke risk prediction model. Int J Biol Biomed. 2019;4:1–6. [Google Scholar]
- 9.Li Z, Zhou T, Li Y, Chen P, Chen L. Anemia increases the mortality risk in patients with stroke:A meta-analysis of cohort studies. Scientific reports. 2016;6:26636. doi: 10.1038/srep26636. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Akins PT, Glenn S, Nemeth PM, Derdeyn CP. Carotid artery thrombus associated with severe iron-deficiency anemia and thrombocytosis. Stroke. 1996;27:1002–5. doi: 10.1161/01.str.27.5.1002. [DOI] [PubMed] [Google Scholar]
- 11.Barlas RS, Honney K, Loke YK, McCall SJ, Bettencourt-Silva JH, Clark AB, et al. Impact of hemoglobin levels and anemia on mortality in acute stroke:Analysis of UK regional registry data, systematic review, and meta-analysis. J Am Heart Assoc. 2016;5:e003019. doi: 10.1161/JAHA.115.003019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Furlan JC, Fang J, Silver FL. Acute ischemic stroke and abnormal blood hemoglobin concentration. Acta Neurol Scand. 2016;134:123–30. doi: 10.1111/ane.12521. [DOI] [PubMed] [Google Scholar]
- 13.Kaiafa G, Savopoulos C, Kanellos I, Mylonas KS, Tsikalakis G, Tegos T, et al. Anemia and stroke:Where do we stand? Acta Neurol Scand. 2017;135:596–602. doi: 10.1111/ane.12657. [DOI] [PubMed] [Google Scholar]
- 14.Mehta PJ, Chapman S, Jayam-Trouth A, Kurukumbi M. Acute ischemic stroke secondary to iron deficiency anemia:A case report. Case Rep Neurol Med. 2012;2012:487080. doi: 10.1155/2012/487080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Milionis H, Papavasileiou V, Eskandari A, D'Ambrogio-Remillard S, Ntaios G, Michel P. Anemia on admission predicts short-and long-term outcomes in patients with acute ischemic stroke. Int J Stroke. 2015;10:224–30. doi: 10.1111/ijs.12397. [DOI] [PubMed] [Google Scholar]
- 16.Tanne D, Molshatzki N, Merzeliak O, Tsabari R, Toashi M, Schwammenthal Y. Anemia status, hemoglobin concentration and outcome after acute stroke:A cohort study. BMC Neurol. 2010;10:22. doi: 10.1186/1471-2377-10-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Naess H, Logallo N, Waje-Andreassen U, Thomassen L, Kvistad CE. U-shaped relationship between hemoglobin level and severity of ischemic stroke. Acta Neurol Scand. 2019;140:56–61. doi: 10.1111/ane.13100. [DOI] [PubMed] [Google Scholar]
- 18.Diamond PT, Gale SD, Evans BA. Relationship of initial hematocrit level to discharge destination and resource utilization after ischemic stroke:A pilot study. Arch Phys Med Rehabil. 2003;84:964–7. doi: 10.1016/s0003-9993(03)00009-1. [DOI] [PubMed] [Google Scholar]
- 19.Mayo Clinic. Hemoglobin Test: Results. 2019. [Last accessed on 2020 Apr 14]. Available from: https://www.mayoclinic.org/tests-procedures/hemoglobin-test/about/pac-20385075 .
- 20.Goldstein LB, Bertels C, Davis JN. Interrater reliability of the NIH stroke scale. Arch Neurol. 1989;46:660–2. doi: 10.1001/archneur.1989.00520420080026. [DOI] [PubMed] [Google Scholar]
- 21.Bushnell CD, Chaturvedi S, Gage KR, Herson PS, Hurn PD, Jimenez MC, et al. Sex differences in stroke:Challenges and opportunities. J Cereb Blood Flow Metab. 2018;38:2179–91. doi: 10.1177/0271678X18793324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Li C, Baek J, Sanchez BN, Morgenstern LB, Lisabeth LD. Temporal trends in age at ischemic stroke onset by ethnicity. Ann Epidemiol. 2018;28:686–90. doi: 10.1016/j.annepidem.2018.07.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Al Rajeh S, Awada A, Niazi G, Larbi E. Stroke in a Saudi Arabian national guard community. Analysis of 500 consecutive cases from a population-based hospital. Stroke. 1993;24:1635–9. doi: 10.1161/01.str.24.11.1635. [DOI] [PubMed] [Google Scholar]
- 24.Yaqub BA, Shamena AR, Kolawole TM, Patel PJ. Cerebrovascular disease in Saudi Arabia. Stroke. 1991;22:1173–6. doi: 10.1161/01.str.22.9.1173. [DOI] [PubMed] [Google Scholar]
- 25.Al-Nozha MM, Abdullah M, Arafah MR, Khalil MZ, Khan NB, Al-Mazrou YY, et al. Hypertension in Saudi Arabia. Saudi Med J. 2007;28:77. [PubMed] [Google Scholar]
- 26.Avan A, Digaleh H, Di Napoli M, Stranges S, Behrouz R, Shojaeianbabaei G, et al. Socioeconomic status and stroke incidence, prevalence, mortality, and worldwide burden:An ecological analysis from the global burden of disease study 2017. BMC Med. 2019;17:191. doi: 10.1186/s12916-019-1397-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data and material available upon request.