

Median sternotomy is still the access of choice for many cardiac surgical procedures. There are different retractors available, each with its specific indication. Sternal wound healing still occurs in 0.4–7% of all cases (1,2). In order to prevent wound healing complications, mechanical forces on the sternum should be distributed evenly, while achieving optimal surgical sight for the performed procedure (3,4). Here, we present a novel sternal retractor offering a wide range of uses ranging from minimally invasive upper sternotomy approaches to full sternotomy during complex combined CABG and multi-valve procedures.
The universal retractor can be used for every type of sternal access in cardiac surgery, ranging from minimally invasive incisions using the J-type mini-sternotomy, Z-type mini-sternotomy to full sternotomy approaches. Different variety of blades sizes as well as their flexibility (aprox. 15 degrees) allow during sternum retraction to adapt to individual thoracic cavity stiffness of the patient and allow for even more distribution of mechanical forces applied to the sternum, thus minimizing surgical damage. The retractor can also be used for harvesting internal thoracic arteries using the IMA retractor blade. Utilizing the retractor for valvular surgery is feasible by applying the ball joint adapter suitable for different accessories, including atrial retractors for mitral and tricuspid valve surgery (Figure 1, Video 1). Due to its size, different kind of OPCAB stabilizers can be easily fitted.
Figure 1.

(A) Universal retractor for harvesting the A. thoracica internal, (B) for Mitral and tricuspid valve surgery using the ball joint adapter suitable for different accessories, including atrial retractors, (C) off pump coronary artery revascularization configuration, (D) minimally invasive configuration.
Video 1.
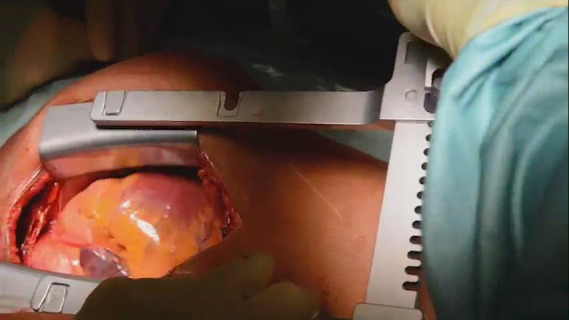
Short overview about the different configurations of the universal retractor.
The new, universal retractor simplifies surgical procedures and reduces the necessity to have different kind of retractors available, since one retractor can be easily adopted for different kind of cardiac surgeries. Even if the necessity occurs to change the planned procedure during the operation, e.g., from CABG to combined CABG with valve surgery, the retractor can remain in place.
There are so far no studies available concerning the wound healing occurrence in patients with the novel retractor. However, one would assume, that the flexible blades would allow for a more even distribution of mechanical forces on the sternum, thus limiting surgical damage. Using potentiometer analysis would be a feasible approach to verify this possible advantage over current retractor models. With cost efficiency in cardiac surgery, reducing the need for different retractors with the possibility of easy adaption to the performed procedure the new universal retractor seems to be beneficial.
Supplementary
The article’s supplementary files as
Acknowledgments
Funding: None.
Ethical Statement: The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Provenance and Peer Review: This article was a free submission to the editorial office, Journal of Thoracic Disease. The article did not undergo external peer review.
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (http://dx.doi.org/10.21037/jtd-20-1051). SC reports personal fees from Fehling, during the conduct of the study. The other authors have no conflicts of interest to declare.
References
- 1.Bolotin G, Buckner GD, Campbell NB, et al. Tissue-disruptive forces during median sternotomy. Heart Surg Forum 2007;10:487-92. 10.1532/HSF98.20071121 [DOI] [PubMed] [Google Scholar]
- 2.Sjögren J, Malmsjö M, Gustafsson R, et al. Poststernotomy mediastinitis: a review of conventional surgical treatments, vacuum-assisted closure therapy and presentation of the Lund University Hospital mediastinitis algorithm. Eur J Cardiothorac Surg 2006;30:898-905. 10.1016/j.ejcts.2006.09.020 [DOI] [PubMed] [Google Scholar]
- 3.Aigner P, Eskandary F, Schlöglhofer T, et al. Sternal force distribution during median sternotomy retraction. J Thorac Cardiovasc Surg 2013;146:1381-6. 10.1016/j.jtcvs.2013.07.075 [DOI] [PubMed] [Google Scholar]
- 4.Pai S, Dunn RM, Babbitt R, et al. Characterization of forces on the sternal midline following median sternotomy in a porcine model. J Biomech Eng 2008;130:051004. 10.1115/1.2948401 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
The article’s supplementary files as