

Abstract
Introduction:
Patient-specific guides are used in the correction of malunion sequelae in adult distal radius fractures. They allow a tridimensional correction of radial glenoid orientation. However, lengthening is small in those indications. Distal radius epiphysiodesis correction is much rarer and patient-specific guide after three-dimensional (3D) planning has never been reported for this indication in the literature.
Case Report:
We report the case of a 16-year-old teenager with a chronic painful wrist and an ulnar positive variance after a post-traumatic epiphysiodesis sequela of the radius. The radius was 11mm shorter than the ulna. An anatomic reconstruction was decided with a lengthening of the radius. Pre-operative planning and patient-specific guide allowed to control an important radial lengthening, to limit the morbidity of the iliac crest bone graft harvesting, to shape the graft precisely, and to maintain a correct radial glenoid orientation despite the important soft tissue tension. Clinical and radiological results at 6 months showed a complete disappearance of pain, optimal objective and subjective functional scores, and an improvement in the distal ulnar variance (7mm). The teenager went back to sport without limitation or pain.
Conclusion:
3Dplanning and intraoperative patient-specific guides in radial epiphysiodesis sequelae allow achieving 3D accurate measures of the graft and of the deformation, guiding the position and the orientation of the distal metaphysis cut of the radius, and limiting the morbidity of the iliac graft harvesting. In that case, it allowed restoring the full function of the wrist without remaining pain.
Keywords: Patient-specific instrumentation, pre-operative planning, epiphysiodesis sequelae wrist disorders
Learning Point of the Article:
Preoperative planning and use of a distal radius patient specific guide enable to standardize the osteotomy surgery against a freehand procedure that requires a harder learning curve.
Introduction
Symmetric or asymmetric lengthening of the radius can be indicated to decrease the pain and to improve the function of the forearm and the wrist. In adults, it is most of the time indicated to correct a distal radius malunion related to a fracture sequelae. It is also often indicated in children with congenital malformations with interesting clinical results as described in the recent literature[1, 2]. Since the past decades, three-dimensional (3D)planification softwares have demonstrated their benefits in arthroplasty, realignment osteotomy, or fracture fixation to plan the various steps of the procedure[3]. The 3Dprinting technology allows building patient-specific guide according to the previous virtual planification with a demonstrated accuracy and reproducibility in many cases. Here, we report an original utilization of a patient-specific guide after 3Dplanification in a case of radius epiphysiodesis sequelae with an important radial shortening.
Case Report
Our patient was 16 years old and he was a student with no particular medical history. The patient and his parents gave their informed consent to report this case. He presented a left upper limb trauma when he was 12 years old that was orthopedically treated by a cast during 3 weeks. Since then, he presented pain in his wrist, especially at sport and when he was leaning on his left hand. His pain was quoted at 7/10 (visual analog scale) and he reported a severe handicap at sport. Clinical examination showed a normal range of motion of his wrist with a normal but painful pronosupination motion. It revealed distal radioulnar instability with a protrusion of the ulnar head (Fig. 1) without instability of the extensor carpi ulnaris tendon. The radioulnar ballottement test of the radioulnar joint, the fovea sign, and the chair test were positive. The clunk test was negative. The symptomatology was marked by a severe functional concern when leaning on his hand during gym classes or when playing basketball. The patient-rated wrist evaluation (PRWE) score was at 51/100 (pain = 31, function = 20), the QuickDASH score was at 43/100. The pain was specifically localized on the ulnar side of the wrist by the patient. No nerve compression or vascular signs were detected. X-rays of the wrist revealed a shortening of the radius with a high radioulnar index (11mm on the anteroposterior view) and an ulnocarpal impingement (Fig. 2). This was highlighted on the magnetic resonance imaging T1sequence of the wrist that revealed overpressure cysts of the triquetrum (Fig. 3). The radioulnar joint surface on the radial side was flat[4]. A lengthening of the radius with an iliac crest autograft was indicated as a reconstructive surgery to recover the normal length of the radius. A bilateral wrist computed tomographyscan was performed with a 3D reconstruction to evaluate the needed lengthening according to the contralateral side. The position and the orientation of the metaphyseal osteotomy were also calculated. A lengthening of 10mm in the longitudinal axis was calculated. The final position of the plate, the length of its screws, and the dimensions of the graft were also generated (Fig. 4). A patient-specific guide was 3Dprinted (Allians Radius®, Newclip) to guide the osteotomy during the surgery. The 3D-printed material of the guide was done in PA2200 uspcl6 (polyamide). Under locoregional anesthesia and with a tourniquet, a volar Henry approach was performed to expose the distal radius. The distal part of the brachioradialis tendon was released at its radial insertion. The guide was applied on the metaphysis of the radius; a K-wire was positioned to evaluate the good position of the guide on the metaphysis with a fluoroscopy control. The holes of the plate were drilled previously. The osteotomy was performed with a 0.8mm saw blade and completed with an osteotome. A specific distractor with 1.8 pins was used to spread the two fragments. To avoid the buckling of the wire and the rotation of the fragment under the distraction stress, a Meary distractor was used and left in place. This allowed the stretching of the soft tissues during the iliac crest taking and it facilitated the insertion of the graft. A tricortical iliac crest bone graft of 10mm length was then taken on the homolateral side. The tricortical graft was then positioned into the osteotomy site flush to the anterior radial surface. The plate was screwed on the radius using the previously drilled holes (Fig. 5). The tourniquet was deflated (50 min). A cautious hemostasis was done and the approach was closed as usual. A removable sling was used to immobilize the patient during 1 month and a passive mobilization of the wrist was started the day after surgery. At 6-month post-operative(Fig. 6), the radius was consolidated with no more clinical deformation. The radioulnar index was improved (5mm on the anteroposterior view) with no more ulnocarpal impingement. The extension was symmetric at 65°, the flexion was at 80° versus 90° on the contralateral side, the radial and ulnar inclinations were at 5° and 40°, respectively, on both sides. The PRWE was at 2/100 (pain = 2/50, function = 0/50), the Quick DASH score was at 2/100. The patient presented no more pain on the ulnar side and was back to sport. No neurologic symptoms were found.
Figure 1.

Clinical examination of the wrist with the protrusion of the ulnar head and the fovea sign.
Figure 2.

X-rays of both wrists.
Figure 3.

Magnetic resonance imaging of the wrist showing the ulnocarpal conflict with the related overpressure cysts.
Figure 4.
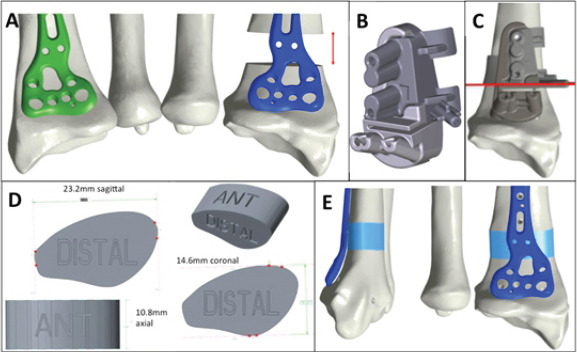
Pre-operative three-dimensional (3D) planification from the wrist computed tomographyscans of both sides. (a) Evaluation of the elongation target length. (b) 3D modelization of the patient-specific guide. (c) Assessment of the position and the orientation of the osteotomy. (d) Measures of the needed graft. (e) Graft and plate in final position.
Figure 5.
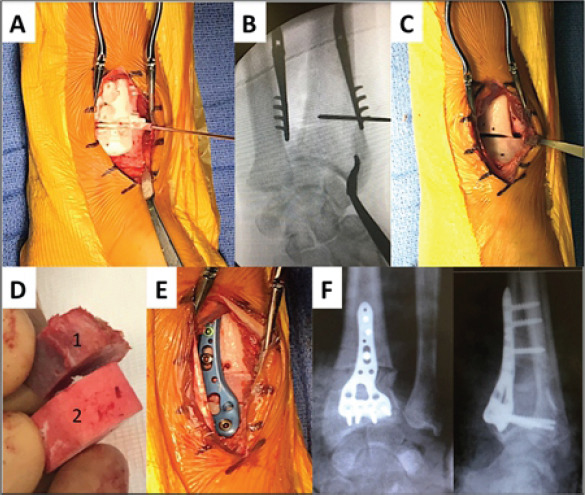
Pre-operative steps of the radial lengthening. (a) Positioning of the patient-specific guide on the distal extremity of the radius. (b) Fluoroscopic control of the position of the K-wire marker. (c) Osteotomy of the radius with the drilled holes of the final plate. (d) Iliac crest bone graft (1) and three-dimensional-printed planned surrogate (2). (e) Graft and plate in their final position. (f) Front and side wrist final X-rays.
Figure 6.

Clinical and radiological results at 6 months of follow-up. The clinical deformation of the wrist is reduced and the radioulnar index has been improved.
Discussion
This clinical case shows the feasibility of a 3Dplanned and guided lengthening osteotomy in the particular case of an epiphysiodesis of the radius with a severe radial loss of length (10mm). A shortening of the ulna was not chosen in that case because we wanted to restore the anatomy of the radius rather than achieve a palliative procedure. Such a computer-assisted lengthening in this specific indication of epiphysiodesis sequelae has not been described yet. Several authors have already made the description and shown the accuracy of the 3D patient-specific guided osteotomy in cases of adult distal radius malunion[5,6]. They discuss its superiority against a freehand procedure that often allows less correction than expected [7]. In fact, the lengthening osteotomy is a highly demanding procedure. In the present case, the osteotomy correction required the control of its 3D direction and the positioning of the cut (4 geometric parameters to control). Then, the needed rotation and translation of the fragments had to be applied in the three planes (six geometric parameters to control). To achieve the first step, the planned patient-specific guide allowed the cutting with very few fluoroscopic controls and at the good place. The rotation and the translation of the fragments were then controlled by the graft shape and the position of the radius plate whose screw holes were previously drilled. Many advantages of this technique can be highlighted. It allows a reduction in the exposition time to the fluoroscopy and so makes the procedure safer, especially in young patients as reported here. It reduces the duration of the surgery and of the tourniquet[8].The pre-operative planning and the use of the guide enable to standardize the osteotomy surgery against a freehand procedure that requires a harder learning curve. Leong et al., in a comparative study, have demonstrated the benefits of the computer-assisted surgical planning combined with a patient-specific surgical guide for distal radius malunions in adults[9]. In their recent meta-analysis, de Muinck et al. showed a significant improvement of functional results for the distal radius malunions[10]. We consider that the pre-operative brainstorming itself during the planning can be considered as a simulation step that makes the surgeon more efficient in this kind of surgery. Another advantage is the limitation of the harvesting of the iliac crest bone graft. In our case, a surrogate gave us the exact sizes of the iliac crest bone graft to harvest and it was applied on the crest cortical to guide the saw cut. A limited sampling decreases the scar and the donor site morbidity (nerve injury, blood loss, hematoma, subcutaneous dimple, …). Then, the added iliac scare was better tolerated by the patient. It may also give less post-operative pain and this is a major concern for the post-operative pain management since the patients often complain about the pain at the iliac crest harvesting site.
Conclusion
Epiphysiodesis sequela of the wrist can be easily assessed with a 3Dplanning system. Then, the correction of the deformation can be optimized before surgery to reach the best anatomical results. An intraoperative printed guide makes the procedure more secure, reduces the exposition time to the fluoroscopy, the time of the surgery, and the size of the scare and further studies must be performed to estimate those benefits.
Clinical Message.
3D planning and intraoperative patient-specific guides in radial epiphysiodesis sequelae allow achieving 3D accurate measures of the graft and of the deformation, guiding the position and the orientation of the distal metaphysis cut of the radius, and limiting the morbidity of the iliac graft harvesting. In that case, it allowed a complete restoration of the wrist function without remaining pain.
Biography



Footnotes
Conflict of Interest: Nil
Source of Support: Nil
Consent: The authors confirm that Informed consent of the patient is taken for publication of this case report
References
- 1.Farr S, Mindler G, Ganger R, Girsch W. Bone lengthening in the pediatric upper extremity. J Bone Joint Surg Am. 2016;98:1490–503. doi: 10.2106/JBJS.16.00007. [DOI] [PubMed] [Google Scholar]
- 2.Miller A, Lightdale-Miric N, Eismann E, Carr P, Little KJ. Outcomes of isolated radial osteotomy for volar distal radioulnar joint instability following radial malunion in children. J Hand Surg Am. 2018;43:81.e1–8. doi: 10.1016/j.jhsa.2017.07.012. [DOI] [PubMed] [Google Scholar]
- 3.Roner S, Vlachopoulos L, Nagy L, Schweizer A, Fürnstahl P. Accuracy and early clinical outcome of 3-dimensional planned and guided single-cut osteotomies of malunited forearm bones. J Hand Surg Am. 2017;42:1031.e1–8. doi: 10.1016/j.jhsa.2017.07.002. [DOI] [PubMed] [Google Scholar]
- 4.Tolat AR, Stanley JK, Trail IA. A cadaveric study of the anatomy and stability of the distal radioulnar joint in the coronal and transverse planes. J Hand Surg Br. 1996;21:587–94. doi: 10.1016/s0266-7681(96)80136-7. [DOI] [PubMed] [Google Scholar]
- 5.Miyake J, Murase T, Moritomo H, Sugamoto K, Yoshikawa H. Distal radius osteotomy with volar locking plates based on computer simulation. Clin OrthopRelat Res. 2011;469:1766–73. doi: 10.1007/s11999-010-1748-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kunz M, Ma B, Rudan JF, Ellis RE, Pichora DR. Image-guided distal radius osteotomy using patient-specific instrument guides. J Hand Surg Am. 2013;38:1618–24. doi: 10.1016/j.jhsa.2013.05.018. [DOI] [PubMed] [Google Scholar]
- 7.vonCampe A, Nagy L, Arbab D, Dumont CE. Corrective osteotomies in malunions of the distal radius:Do we get what we planned? Clin OrthopRelat Res. 2006;450:179–85. doi: 10.1097/01.blo.0000223994.79894.17. [DOI] [PubMed] [Google Scholar]
- 8.Bauer DE, Zimmermann S, Aichmair A, Hingsammer A, Schweizer A, Nagy L, et al. Conventional versus computer-assisted corrective osteotomy of the forearm:A retrospective analysis of 56 consecutive cases. J Hand Surg Am. 2017;42:447–55. doi: 10.1016/j.jhsa.2017.03.024. [DOI] [PubMed] [Google Scholar]
- 9.Leong NL, Buijze GA, Fu EC, Stockmans F, Jupiter JB DistalRadius Malunion (DiRaM) collaborative group. Computer-assisted versus non-computer-assisted preoperative planning of corrective osteotomy for extra-articular distal radius malunions:A randomized controlled trial. BMC MusculoskeletDisord. 2010;11:282. doi: 10.1186/1471-2474-11-282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.deMuinck Keizer RJ, Lechner KM, Mulders MA, Schep NW, Eygendaal D, Goslings JC. Three-dimensional virtual planning of corrective osteotomies of distal radius malunions:A systematic review and meta-analysis. Strategies Trauma Limb Reconstr. 2017;12:77–89. doi: 10.1007/s11751-017-0284-8. [DOI] [PMC free article] [PubMed] [Google Scholar]