

The rapid rise in U.S. cases of COVID-19 caused by the new coronavirus SARS-CoV-2 prompted a sharp curtailment in nonurgent outpatient visits in U.S. ophthalmology practices in mid-March 2020, followed by variable resumption in May 2020.1 Although, during this period, providers in many specialties were able to transition to providing care through telehealth, eyecare providers faced additional challenges due to the lack of experience and capability for remote assessment of key elements of an in-person eye examination.2–4
With approval by the institutional review board of the University of California, San Francisco, we distributed an anonymized electronic survey to eyecare providers, including residents, fellows, attending physicians, and optometrists in the University of California, San Francisco, Department of Ophthalmology on April 21, 2020, when only urgent outpatient visits were allowed, and then again 5 weeks later, on May 26, 2020, as routine outpatient visits were gradually resumed.
In the 2 months prior to the pandemic-induced shutdown of all nonemergent eye services on March 16, 2020, no telehealth visits were performed among the 6401 encounters in January 2020 and the 5567 encounters in February 2020. Immediately thereafter, the number of telehealth encounters rose from a baseline of 66 (3%) in March 2020 to 537 (57%) in April 2020. After limited reopening on May 4, 2020, telehealth encounters declined to 421 (35%) in May. In April 2020, the number of telehealth visits peaked at 9% of the preshutdown baseline.
A total of 72 eyecare providers were eligible for participation in the survey. Of these, 43 participants (60%) completed the first survey in April 2020; 35 participants (49%) completed the follow-up survey. In the April survey, 91% of respondents reported having performed telehealth visits in the previous week; that proportion dropped to 71% after reopening began (Table 1). In the follow-up survey, the proportion of participants who planned to decrease their number of telehealth visits increased from 2% to 17%; conversely, the proportion of participants who planned to increase telehealth visits decreased from 67% to 14%.
Table 1.
Characteristics of telehealth encounters as self-reported by eyecare providers.
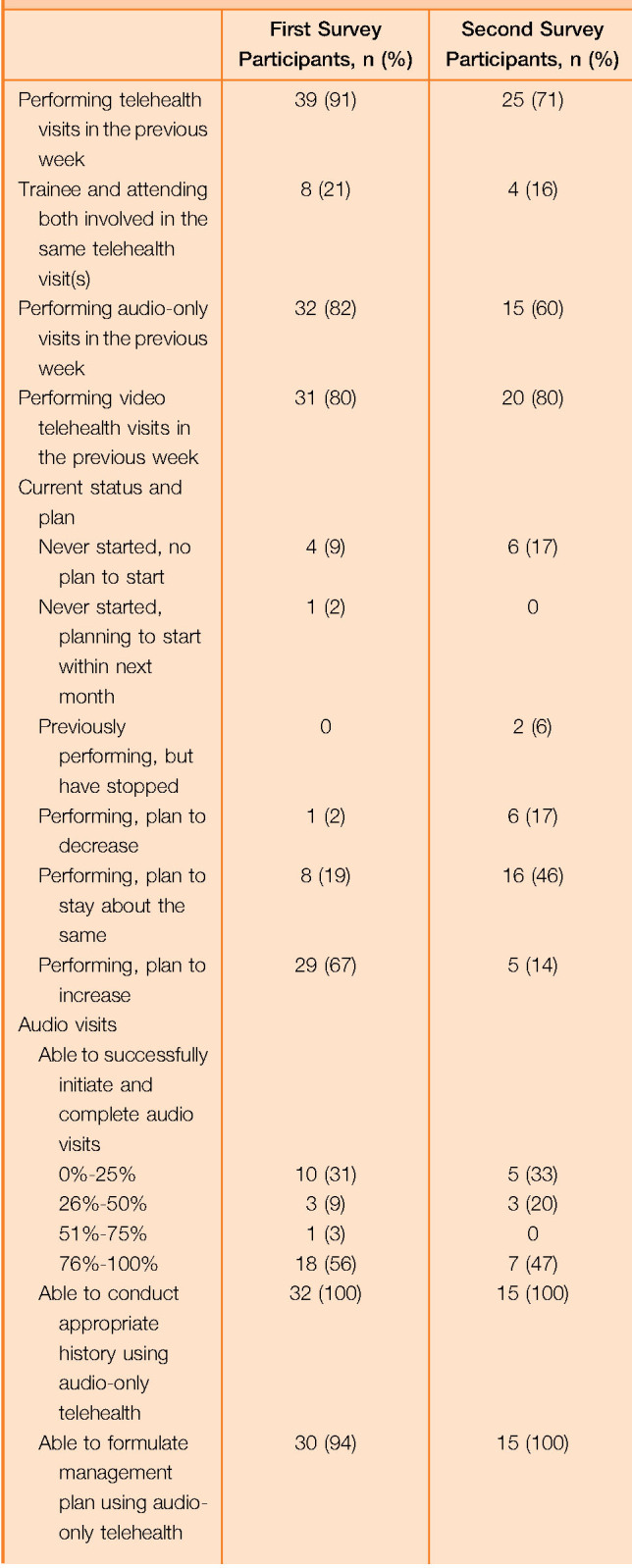
| First Survey Participants, n (%) | Second Survey Participants, n (%) | |
| Performing telehealth visits in the previous week | 39 (91) | 25 (71) |
| Trainee and attending both involved in the same telehealth visit(s) | 8 (21) | 4 (16) |
| Performing audio-only visits in the previous week | 32 (82) | 15 (60) |
| Performing video telehealth visits in the previous week | 31 (80) | 20 (80) |
| Current status and plan | ||
| Never started, no plan to start | 4 (9) | 6 (17) |
| Never started, planning to start within next month | 1 (2) | 0 |
| Previously performing, but have stopped | 0 | 2 (6) |
| Performing, plan to decrease | 1 (2) | 6 (17) |
| Performing, plan to stay about the same | 8 (19) | 16 (46) |
| Performing, plan to increase | 29 (67) | 5 (14) |
| Audio visits | ||
| Able to successfully initiate and complete audio visits | ||
| 0%-25% | 10 (31) | 5 (33) |
| 26%-50% | 3 (9) | 3 (20) |
| 51%-75% | 1 (3) | 0 |
| 76%-100% | 18 (56) | 7 (47) |
| Able to conduct appropriate history using audio-only telehealth | 32 (100) | 15 (100) |
| Able to formulate management plan using audio-only telehealth | 30 (94) | 15 (100) |
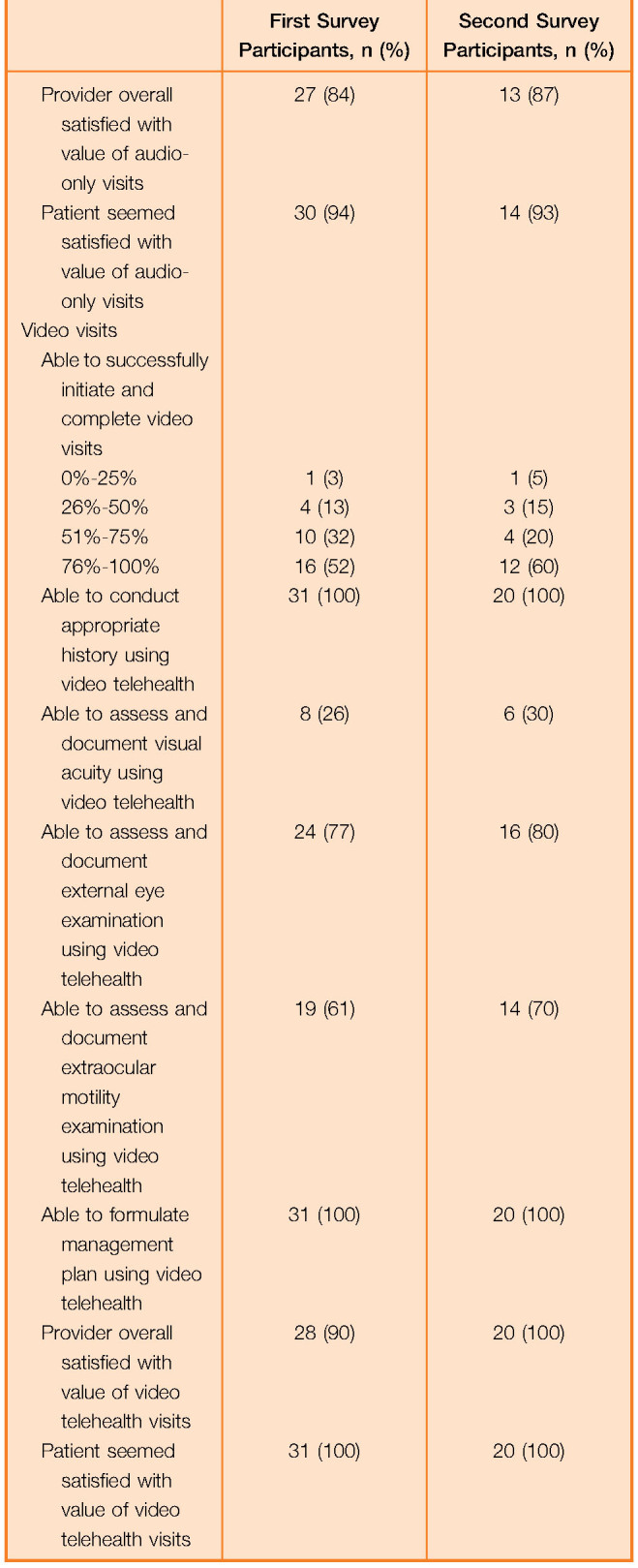
| Provider overall satisfied with value of audio-only visits | 27 (84) | 13 (87) |
| Patient seemed satisfied with value of audio-only visits | 30 (94) | 14 (93) |
| Video visits | ||
| Able to successfully initiate and complete video visits | ||
| 0%-25% | 1 (3) | 1 (5) |
| 26%-50% | 4 (13) | 3 (15) |
| 51%-75% | 10 (32) | 4 (20) |
| 76%-100% | 16 (52) | 12 (60) |
| Able to conduct appropriate history using video telehealth | 31 (100) | 20 (100) |
| Able to assess and document visual acuity using video telehealth | 8 (26) | 6 (30) |
| Able to assess and document external eye examination using video telehealth | 24 (77) | 16 (80) |
| Able to assess and document extraocular motility examination using video telehealth | 19 (61) | 14 (70) |
| Able to formulate management plan using video telehealth | 31 (100) | 20 (100) |
| Provider overall satisfied with value of video telehealth visits | 28 (90) | 20 (100) |
| Patient seemed satisfied with value of video telehealth visits | 31 (100) | 20 (100) |
Most participants reported being able to obtain history and formulate management plans whether performing audio-only or video-based telehealth encounters. Less than one third of respondents who performed video telehealth visits reported assessing visual acuity (Table 1). Social distancing was ranked as the most important benefit of telehealth. The inability to perform adequate examination and/or testing was perceived to be the most important barrier to adoption of telehealth by 86% and 94% of participants in the initial and follow-up surveys, respectively.
Respondents who felt telehealth “should be important” or “will be important” in eyecare after the pandemic also reported having performed a higher number of telehealth visits in the week prior to the survey (P < .05) (Table 2). Higher usage of audio and video visits was also correlated with believing that validated visual acuity assessment tools were important for telehealth (P < .05) (Table 2). Overall, 94% of respondents felt that telehealth should play an important role in eyecare after the COVID-19 pandemic.
Table 2.
Provider attitudes toward telehealth and correlation with frequency of performing telehealth in the initial survey.

| Statement | Strongly Disagree, n (%) | Somewhat Disagree, n (%) | Neither Agree nor Disagree, n (%) | Somewhat Agree, n (%) | Strongly Agree, n (%) | Correlation with the No. of Audio Visits Performed, Spearman σ (95% CI) | Correlation with the No. of Video Visits Performed, Spearman σ (95% CI) |
| Telehealth will play an important role in eyecare after the COVID-19 pandemic | 1 (2) | 2 (5) | 5 (12) | 15 (35) | 20 (47) | 0.43 (0.14, 0.73); P = .003 | 0.35 (0.07, 0.65); P = .02 |
| Telehealth should play an important role in eyecare after the COVID-19 pandemic | 0 | 2 (5) | 1 (2) | 17 (40) | 23 (54) | 0.37 (0.07, 0.69); P = .01 | 0.35 (0.06, 0.67); P = .02 |
| The development of validated tools for remote assessment of visual acuity will be important for facilitating the adoption of telehealth in eyecare | 0 | 0 | 0 | 6 (14) | 37 (86) | 0.37 (0.07, 0.80); P = .01 | 0.35 (−0.04, 0.71); P = .02 |
| The development of remote imaging capabilities will be important for facilitating the adoption of telehealth in eyecare | 0 | 0 | 1 (2) | 10 (23) | 32 (74) | 0.26 (−0.13, 0.68); P = .09 | 0.21 (−0.18, 0.58); P = .17 |
More than 90% of the providers were conducting telehealth encounters within a few weeks of the curtailment of in-person outpatient care. However, only few respondents reported assessing visual acuity. Indeed, the top barrier to the telehealth adoption in the survey results was the “inability to perform adequate examination and/or testing.” Our data suggest that a perceived lack of validated visual acuity assessment and imaging tools might be an important barrier to further adoption and expansion of telehealth in eyecare. Increasing demand for telehealth in eyecare might encourage more widespread development and deployment of low-cost remote assessment tools, including smartphone-based applications, for visual acuity measurement, motility assessment, and imaging, and emerging technologies such as virtual reality goggle-enabled perimetry. Notwithstanding current limitations, more than 90% of participants responded that telehealth should play an important role in eyecare in the postpandemic period.
Our study was conducted among eyecare providers at a single academic center, so results might not be generalizable to other regions or healthcare settings. It was conducted over a relatively short period of time during the initial phase of the COVID-19 pandemic. Continuation of the study over a longer interval of time might yield additional insights. Nonetheless, this study suggests interest among eyecare providers in adopting telehealth, not only during the COVID-19 crisis but beyond as well.
Acknowledgments
Dr. Gerami Seitzman and Dr. Jeremy Keenan gave helpful comments regarding the survey design.
Footnotes
Supported in part by unrestricted grants from Research to Prevent Blindness and That Man May See, Inc.
Disclosures: None of the authors have a financial or proprietary interest in any material or method mentioned.
REFERENCES
- 1.Wang C, Horby PW, Hayden FG, Gao GF. A novel coronavirus outbreak of global health concern. Lancet 2020;395:470–473 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Caetano R, Silva AB, Guedes ACCM, de Paiva CCN, da Rocha Ribeiro G, Santos DL, da Silva RM. Challenges and opportunities for telehealth during the COVID-19 pandemic: ideas on spaces and initiatives in the Brazilian context. Cad Saude Publica 2020;36:e00088920. [DOI] [PubMed] [Google Scholar]
- 3.Rathi S, Tsui E, Mehta N, Zahid S, Schuman JS. The current state of teleophthalmology in the United States. Ophthalmology 2017;124:1729–1734 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Williams AM, Kalra G, Commiskey PW, Bowers EMR, Rudolph BR, Pitcher MD, Dansingani KK, Jhanji V, Nischal KK, Sahel JA, Waxman EL, Fu R. Ophthalmology practice during the coronavirus disease 2019 pandemic: the University of Pittsburgh experience in promoting clinic safety and embracing video visits. Ophthalmol Ther 2020;9:1–9 [DOI] [PMC free article] [PubMed] [Google Scholar]