

Abstract
Introduction
This study identified characteristics of victims of fatal scuba diving incidents to determine contributing factors and inform appropriate countermeasures.
Methods
The National Coronial Information System (NCIS) was searched to identify scuba diving deaths for 2001–2013, inclusive. Data were extracted from witness and police reports, medical histories and autopsies. Descriptive statistics were used to analyse these data.
Results
There were 126 scuba diving-related fatalities identified during the study period. The mean age was 44 years, 99 (79%) victims were male and 83 (77%) were either overweight or obese. Most deaths occurred in New South Wales and Queensland, often in a commercial setting. Twenty-three (79%) Queensland victims were overseas tourists. At least 52 (41%) were novices and 17 (13%) died during training or an introductory scuba experience. Only 35 (28%) were with a buddy when the incident occurred and at least 81 (64%) were still wearing weights when recovered.
Conclusions
The age of these victims may reflect an older cohort of participants and the associated higher prevalence of chronic medical conditions. The high prevalence of obesity suggests that this may be a risk factor. The high proportion of deaths in overseas tourists highlights an on-going need for appropriate screening and monitoring in what may be a higher risk cohort. The number of deaths that occurred under instruction highlights the importance of careful assessment of the site, prevailing conditions, an appropriate instructor-student ratio and close supervision.
Keywords: DAN – Divers Alert Network, Diving deaths, Diving incidents, Obesity, Research, Solo diving
Introduction
With more than 25,000 km of coastline and a mix of temperate and tropical waters including the Great Barrier Reef, Australia offers a variety of scuba diving opportunities for both locals and tourists. Like many adventure activities, scuba diving is conducted in a potentially hostile environment and involves certain risks. Such risks may arise from the diving environment itself or may be related to various other factors including: the participant’s physical, medical and psychological health; training or experience; equipment failure unfamiliarity or misuse; poor decision-making; and attitudinal factors. As a result, there is inevitably an associated morbidity and mortality,[ 1 - 7] which has been estimated to be 0.48 deaths per 100,000 dives for Australian residents.[ 8]
Earlier reports have suggested that the age of fatality victims has increased over time, raising concerns about the increased potential for co-existing medical conditions with age and their impact within the diving environment.[ 1 , 2 , 6 , 9] Some US data revealed an increase in the BMI of diving victims over recent decades.[ 1] Other factors including training, experience, supervision and equipment issues can affect diving safety and it is valuable to assess the influence of these over more recent times.[ 2 , 4 , 6]
In order to better understand the causation of Australian scuba diving fatalities and so enable the development of appropriate prevention strategies, it is important to know the characteristics and activities of Australian divers and to comprehensively document and carefully analyse diving fatalities. This has been achieved, in part, through the publication of annual Australian fatality reports.[ 10 - 21] However, it is valuable to examine the combined data to identify any trends that may impact safety.
The aim of this study was to identify the demographics and diving characteristics of victims of scuba diving fatalities in Australia from 2001 to 2013. Further reports will examine the chain of events in these fatalities including associated medical issues and, together, will better inform appropriate countermeasures.
Methods
This was a case series of scuba diving-related fatalities that occurred in Australian waters from 2001 to 2013, inclusive.
ETHICS APPROVAL
Approval for the study was received from the human research ethics committees of the Victorian Department of Justice, the Royal Prince Alfred Hospital and the Coroner’s Court of Western Australia, the Queensland Office of the State Coroner and Deakin University.
SEARCH
A comprehensive key word search was made of National Coronial Information System (NCIS)[ 22] to identify scuba diving-related deaths that were reported to various state coronial services for the years 2001–2013, inclusive. Key words included scuba, compressed air, compressed gas and underwater. As it can take many years for some coronial cases to be closed and the relevant data to become available, the particular period was selected as the principal investigator had access to more complete data for this period. Cases identified were matched with cases collected by the Divers Alert Network Asia-Pacific (DAN AP) via the media or the diving community to minimise the risk of over- or under-reporting.
REVIEW PROCEDURE
For cases in 2001 and 2002, the principal investigator reviewed the coronial reports in conjunction with Walker’s relevant Project Stickybeak reports published in the diving medical literature.[ 20 , 21] Project Stickybeak collected and reported Australian diving fatality data from 1972 and 2003, inclusive. The 2003 cases were reviewed by both Walker and the principal investigator, consensus reached and a report published.[ 19]
The procedure followed for cases between 2004 and 2012 was as follows:
1. Both the principal investigator and another investigator reviewed the police reports, witness statements and coronial reports and independently prepared a summary of each incident.
2. The principal investigator reviewed both datasets, investigated any discrepancies and prepared edited incident summaries.
3. The incident summaries, coronial and autopsy reports were independently reviewed by a research team comprising diving physicians, a forensic pathologist with extensive experience in diving autopsies, a retired judge and researchers with substantial experience in diver training, data collection and accident management.
4. Annual series reports were written and published.[ 10 - 18]
The principal investigator solely reviewed the coronial data for cases in 2013 and extracted relevant data.
Some historical fatality data from Project Stickybeak was combined with similar data from the current study period in order to investigate any trends over the extended period from 1965 to 2013, inclusive. Both sets of data were based on the available coronial files.
OUTCOME MEASURES
A range of outcome measures were extracted. These included diver demographics, origin, certifications and experience; dive location and setting; buddy circumstances, dive purpose and depth and equipment (weights, buoyancy compensation, breathing gas supply, equipment failure).
It is difficult to satisfactorily define diving experience as it is not only dependent on the number and recency of dives, also on the nature of these dives. Relevant background information was missing in many of the cases, so relatively simple and somewhat arbitrary definitions of experience were used, despite their shortcomings. A ‘novice’ was defined here as having done 30 dives or less, an ‘experienced diver’ had performed more than 30 dives, and a ‘very experienced’ diver had done at least 200 dives.
STATISTICAL ANALYSIS
Trends in numbers of deaths were modelled using log linear Poisson regression, which is the most appropriate analysis technique for trends in count data. This was modified for trends in female deaths by the addition of total deaths as a denominator allowing for analysis of trends in the proportion of deaths among women. Age at death is a continuous variable, so trends in mean age at death were modelled using weighted least squares regression. Trend analyses were done using the Stata 15 software.[ 23] The exception was where a trend appeared to change across the study period. In this case, the Poisson model was extended to allow the fitting of two simultaneous models using the ‘Joinpoint Method’. This technique fits two Poisson models joined at a ‘joinpoint’, with both the optimal position of the join (if any) and the model parameters estimated simultaneously using a sequential permutation test procedure.[ 24] This was done using the National Cancer Institute Joinpoint software.[ 25] Descriptive analyses based on means and standard deviations or medians and ranges as appropriate was conducted using SPSS Version 25 (IBM Armonk, NY; 2017). Comparisons of proportions employed odds ratios (OR) accompanied by 95% confidence intervals (95% CI). Trends in counts and proportions are reported as the average proportional change between time periods accompanied by 95% confidence intervals. The level of significance was 0.05.
Results
STUDY PERIOD 2001–2013
Demographics
There were 126 scuba diving fatalities during the study period. Despite annual fluctuations, there was little overall change over the study period in the mean age of the victims. The mean (SD) age was 44 (13) years and 99% (79%) of the victims were male (Figure 1).
Figure 1.

Distribution of scuba fatalities by age and sex (n = 126)
The body mass index (BMI) data were available for 108 victims. The mean (SD) BMI was 28.5 (5.0) kg·m2. Two thirds of victims were either overweight (BMI 25–29) or obese (BMI ≥ 30) (Figure 2).
Figure 2.
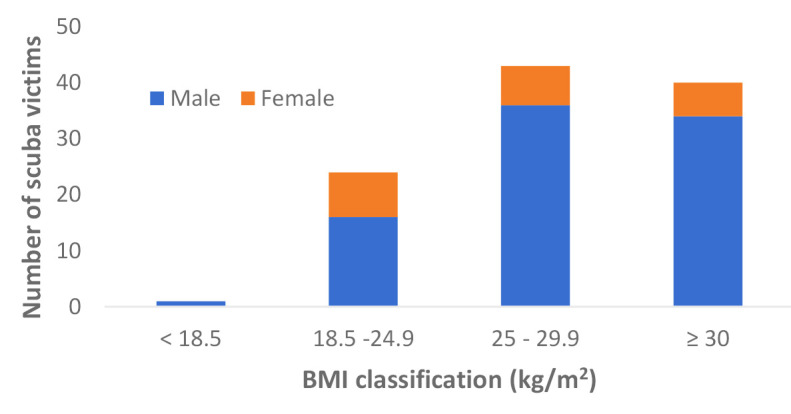
BMI classifications by sex for scuba victims (n = 108)
Of note, 12 (38%) of the 32 (25%) deaths determined to be cardiac-related were among victims who were obese, with BMIs ranging from 30 to 42 kg·m2. (The other major disabling agents were asphyxia (47%) and arterial gas embolism/pulmonary barotrauma (15%) which are discussed in a further paper).
Certifications and experience
The scuba diving certification levels were known for 90 victims (Table 1). Based on 74 cases with data on the period of diving, the median (IQR) was 3 (1–12) years. The median (IQR) number of dives performed prior to the fatal incident was 20 (5–100) dives.
Table 1. Certification levels of victims (n = 126) .
| Certification level | n (%) |
| None | 8 (6) |
| Under training | 12 (10) |
| Open water (OW) | 39 (31) |
| OW + other courses | 14 (11) |
| Technical | 10 (8) |
| Instructor | 7 (6) |
| Not reported | 36 (29) |
In addition to, or in the absence of a reported number of dives, witness statements from their buddies and/or families were also used to help determine the divers’ possible level of experience within the defined parameters. On this basis, 52 (41%) victims were defined as novices, 43 (34%) were experienced and 15 (12%) were very experienced. In 16 (13%) cases, indications of experience were unavailable. Nine (7%) victims died on their first dive and 15 (12%) within their first five dives. At least 12 of the scuba victims had not dived for periods ranging from six months to 11 years immediately prior to their fatal dive.
Location and setting
New South Wales and Queensland had the highest proportions of deaths with approximately one quarter of deaths each (Table 2). No deaths occurred in the Northern Territory or Australian Capital Territory. The mean (SD) age of the scuba diving victims varied little between states and territories.
Table 2. Distribution and mean age of scuba fatalities by state or territory (n = 126). n/a = not applicable .
| Location | n (%) | Age (years) mean (SD) |
| New South Wales | 32 (25) | 47 (13) |
| Queensland | 29 (23) | 46 (15) |
| Victoria | 20 (16) | 41 (14) |
| Western Australia | 19 (15) | 43 (9) |
| South Australia | 17 (13) | 41 (12) |
| Tasmania | 9 (7) | 47 (12) |
| Northern Territory | 0 (0) | n/a |
| Australian Capital Territory | 0 (0) | n/a |
Overall, 58 (46%) deaths occurred in a commercial setting, either on dive charters or under the supervision of a dive professional. More than 80% of scuba deaths in Queensland occurred in a commercial setting. The relative proportions by state and territory were Queensland (86), Victoria (50), New South Wales (41), Tasmania (33), Western Australia (26), South Australia (12), Northern Territory (0) and Australian Capital Territory (0).
Origin of victims
Overall, 35 (28%) victims were tourists. Twenty-four (83%) of the 29 scuba victims in Queensland were tourists, one from interstate and the remainder from overseas. The proportions of victims who were tourists in the other states and territories ranged from zero (Victoria, South Australia, Northern Territory, Australian Capital Territory), 11% (Western Australia), 16% (New South Wales) to 22% in Tasmania.
Buddy circumstances
Based on available reports, 13 (10%) victims had set out diving solo. Fifty-five (44%) had separated from their buddy or group, intentionally or unintentionally, prior to the incident and another 22 reportedly separated during the incident. No relevant information was available for one incident. Overall, only 35 (28%) victims were with their buddy or buddies at the time of their demise.
Based on the relevant data available for 112 of the incidents, there was a higher frequency of separation prior to the incident when the divers were within a group larger than two, rather than within a buddy pair. This occurred with 23/33 (70%) of victims in groups and 32/79 (41%) of victims in buddy pairs. (OR = 3.4; 95% CI = 1.4 to 8.1, P = 0.006).
Dive purpose
No activity details were available for one diver. Seventy-nine (63%) victims were essentially sightseeing. Twenty-three (18%) were harvesting seafood (recreationally) and spearfishing. Another diver was collecting cuttlefish eggs for research.
In addition there were five divers who died during work-related activities. Four of these were amateurs who died during activities such as clearing an anchor, unfouling a propeller or cleaning their boat’s hull. The last, an instructor, died while leading a deep technical dive using a closed-circuit rebreather (CCR).
Seventeen (13%) victims died while undergoing diver training or while being supervised by an instructor on an introductory scuba experience. One of these occurred while being trained by a friend, who was not a qualified instructor. The others occurred while under the care of certified instructors. The number of deaths in the various training programs were: introductory scuba (5), open water (6), advanced open water (2), rescue (1), technical (1), commercial (1) and unsanctioned (1).
Six of these deaths were associated with pre-existing medical conditions, another six were associated with poor supervision in adverse conditions, and at least two involved equipment problems precipitating a rapid ascent and subsequent cerebral arterial gas embolism (CAGE).
Depth of incident
The depth at which the incident occurred, or was believed likely to have occurred, was recorded in 116 incidents. The median (IQR) depth was 12 (6–21) metres (m), with a range of 0 to 125 m. Forty-six (37%) incidents occurred at a depth of ≤ 10 m, and 72% ≤ 20 m.
Weighting
In 21 cases the weighting circumstances were unreported, and six victims had not set out wearing any weights. Of the 99 victims who were known to have been wearing a weight belt or integrated weights at the time of diving, 81 (82%) were found still wearing the weights. Only 18 of the victims were known to have ditched their weights.
The amount of weight carried was known for 63 victims. The median (IQR) weight was 9 (6, 12) kg with a range of 2 to 20 kg. Thirty of the 33 divers who carried 9 kg or more were diving in temperate waters (i.e., below the Tropic of Capricorn).
Buoyancy compensators
Data were available about the buoyancy compensator device (BCD) circumstances in 95 of the incidents. Overall, 45 (47%) victims were found with an uninflated BCD and in only two cases was the BCD later found to be faulty. Of note, 38 of the 45 victims (84%) found with an uninflated BCD were also still wearing their weight belt.
Breathing gas supply
Six (5%) of victims had been breathing a gas other than air. Five of these were using closed-circuit rebreathers and carrying air and oxygen cylinders to provide the ‘bottom mix’. An open-circuit diver who died from fulminant DCS had been breathing air on the bottom and nitrox during decompression.
At least 42 (34%) of the victims had exhausted or near-exhausted their breathing gas supply. Sixty-four (51%) had sufficient gas to surface safely, with 40 (32%) having at least one quarter of their supply remaining. In 15 cases the gas supply circumstances were unstated or not applicable.
Equipment faults
There was no mention of any equipment examination in 13 cases and nothing abnormal reported in 72 cases. Police examiners reported finding faults with the equipment in 41 (33%) cases although most of the faults were thought not to have been a significant contributor to the fatalities. The faults identified and their frequency included breathing gas impurities (11), regulator (9), BCD (9), pressure gauge (4), closed circuit rebreather (1) and others (7).
Faulty (high reading) cylinder contents gauges were associated with and thought likely to have contributed to four incidents, all of which involved the victim running out of breathing gas. Most of the regulator faults (7 cases) involved perforated mouthpieces which allowed water aspiration. Most of the identified BCD problems (8) involved malfunctioning inflator/deflator mechanisms.
Equipment-related problems were the likely triggers in at least eight of the incidents. These included a detached demand valve, faulty tank valve, faulty inflators on a BCD and a drysuit, and out-of-date and faulty oxygen sensors on a rebreather.
There were 11 cases where the breathing gas did not meet the relevant Australian Standards.[ 26] n 10 of these, the water vapour and carbon dioxide levels were high, although not believed to have been contributory. In one case, excess oil in the breathing air was thought likely to have caused nausea and led to a rapid ascent with consequent CAGE.
COMBINING STUDY RESULTS WITH HISTORICAL DATA – 1965 TO 2013
The DAN AP database indicates that from 1965 to 2000 there were a total of 267 recorded fatalities involving scuba divers in Australian waters. The additional 126 cases from this current study period makes a total of 393 deaths from 1965 to 2013, inclusive. Some demographic data and trends revealed from these combined data are presented in Figures 3, 4 and 5 and Table 3.
Figure 3.

Scuba diving deaths in Australia, 1965–2013 (n = 393)
Figure 4.

Annual female deaths as a proportion of total deaths 1965–2013
Figure 5.

Age of scuba victims, 1965–2013
Table 3. Age measures of scuba victims, 1965–2013 .
| Age (years) | All n = 393 | Male n = 323 | Female n = 70 |
| Mean (SD) | 37.7 (13.5) | 38.1 (13.7) | 35.8 (12.6) |
| Range | 13–72 | 13–72 | 18–65 |
| % > 50 | 21 | 22 | 16 |
The Joinpoint trend analysis as shown in Figure 3 identified a statistically significant change in the trend in average scuba deaths in 1991. On average scuba diving deaths rose by a factor of 1.44 (95% CI 1.08 to 1.91) each decade between 1963 and 1991. This means that each decade had, on average, 44% more deaths than the previous decade. After 1991, there was no statistically significant trend.
Figure 4 shows the number of female deaths in each year as a proportion of total deaths, along with the trend line fitted by the Poisson model. Overall 18% of the scuba victims were females, with the proportion rising from 0% in 1965 to 27% in 2013. On average, the proportion of female scuba diving deaths rose across this period by a factor of approximately 1.30 (95% CI 1.11 to1.53) each decade.
The mean (range) age for the scuba divers was 33.7 (13–72) years. Table 3 shows the age data for the scuba victims as a group, and by gender.
Figure 5 shows the mean age at death in each year, along with the trend line fitted by the weighted least squares regression model for the years 1965 to 2013. The mean age rose by an average of 4.6 years (95% CI 3.4–5.7) for each decade. Mean age was approximately constant following 2001, suggesting that it may have reached a plateau at this point.
Discussion
Among the 126 scuba diving-related fatalities, the victims were predominantly middle-aged males and more than three quarters were overweight or obese. The majority of the divers were certified but around 40% were still novices. Most of the victims in Queensland were international tourists. Three quarters of the victims were alone at the time of their incident.
DEMOGRAPHIC FACTORS
Various surveys since 2001 have indicated that around three quarters of active Australian scuba divers were male.[ 8 , 27] Our finding that 80% of victims were males likely reflects their high participation rate as well as the greater prevalence of chronic medical conditions, especially cardiac and cardiovascular, in the male population.[ 28] The increase in the proportion of female victims over the extended period likely reflects increased participation by females.
National sporting surveys have also indicated that 30% of Australian scuba divers were aged 45 years or older,[ 8] consistent with that of survey respondents of mainly relatively inexperienced divers.[ 27] However, survey respondents of more active divers (e.g., DAN members and PADI members) were older, with medians in excess of 45 years.[ 27] By comparison, the ages of scuba diving victims have increased substantially over the decades but appear to have plateaued since 2000, with a median of 45 years. This is similar to the survey respondent cohort of more active divers.[ 27]
OVERWEIGHT OR OBESITY
The proportion of Australian scuba victims who were either overweight or obese (78%) was considerably higher than the 63% in the Australian adult population.[ 28] It was also much higher than the prevalence reported by three cohorts of Australian divers, which ranged from 40% in younger, less experienced divers, to 64% in older, active divers.[ 27]
The prevalence of obesity in the Australian scuba victims (35%) was also substantially higher than in the general community (28%)[ 28] and in the diver survey respondents.[ 27] This suggests that being overweight or obese may be a risk factor for a scuba diving fatality, which is often cardiac-related.[ 10 - 16 , 2 , 6] This is consistent with data from the general population that indicate an association between significant health conditions and being overweight or obese,[ 29 - 32] as well was an association between obesity and sudden cardiac death.[ 33 , 34]
Obesity per se can be a contributory factor to an incident.[ 35 , 36] The adverse effects of obesity on respiratory mechanics when immersed, the need for additional weights and increase in the hydrodynamic drag may act to compromise safety by adding to the cardiac workload. Undiagnosed obstructive sleep apnoea, diabetes, as well as hypertension and high cholesterol are more common in obese individuals and are all risk factors for coronary artery disease.[ 37]
ORIGIN OF VICTIMS, LOCATION AND SETTING OF DIVING
Diving in an unfamiliar setting can introduce additional risks due to the lack of local knowledge about factors such as sea conditions, underwater topography, differences in diving practices, cultural differences and language difficulty. This is exacerbated by inexperience.[ 10 - 18] Almost 30% of the scuba victims in this series were tourists, mainly from overseas. Queensland is a very popular destination for tourists and many dive or snorkel on the Great Barrier Reef, mostly in a commercial setting.[ 38] As such, it is unsurprising that almost one quarter of the scuba deaths occurred in this State, 80% of these involving tourists who were predominantly international.
Diving-related tourism is an important income source for Queensland and, in 1992, a regulated code of practice for diving activities was introduced in order to provide regulated safety guidelines for the industry in that state. This has been periodically updated, the latest version being released in 2018.[ 39] However, despite the comparatively high number of deaths, the estimated annual fatality rate for tourist scuba divers in Queensland is considerably lower than the overall rate for Australian residents.[ 8] The risk in Queensland may be partly mitigated by generally more favourable diving conditions and closer oversight as a result of enforcement of the code of practice. Although a code of practice has been created for Victoria, it is voluntary, likely unknown to many local dive professionals due to minimal promotion, and, in the long-time experience of these authors, is often not followed.[ 40]
One quarter of the scuba deaths occurred in New South Wales, most involving residents, and in non-commercial settings. New South Wales has a relatively large resident diving population, reportedly encompassing 27% of active Australian divers.[ 41] Its long and accessible coastline and variety of dive sites is conducive to independent diving and snorkelling.
Diving in the southern states can be more demanding with respect to colder water, rough and variable conditions, poorer visibility and the need for greater thermal insulation with its associated increased weighting requirements. This is reflected in the considerably higher annual scuba fatality rate estimated for Victoria.[ 8]
CERTIFICATION AND EXPERIENCE
Of the 90 scuba victims whose certification level had been recorded, almost all (91%) were known to be certified or were undergoing training at the time of their demise. This proportion was considerably higher than the 77% reported for scuba victims from 1972 to 1993[ 42] and suggests an improved recognition of the need for training and certification and/or possibly a greater ease of determining certification status due to the internet. Although, it is generally accepted that training reduces the likelihood of a mishap, there are few published data specifically supporting this. However, some reports indicate that diving fatality victims had often broken one or more of the general diving safety rules, so learning, and adhering to, such rules should provide a safety buffer.[ 43 , 44]
Although it was not investigated in this study, it is logical that, in general, competent swimmers are more likely to be more comfortable in the aquatic environment than poor swimmers. Swimming competency is assessed prior to diver certification, although the minimum requirements are basic[ 45 , 46] and some certified divers likely have poor aquatic skills. These do not hold them in good stead if challenged by difficult surface conditions.
Defining ‘experience’ in diving is extremely difficult, with the number of dives, time of accumulation, recency of activity and the nature of diving among the influencing factors. Given the varying definitions of experience used in previous fatality reports from Australia and elsewhere, it is difficult to confidently measure and compare changes in the level of experience of the victims over time. Although the defining criteria in this series were somewhat arbitrary, at least 46% of the victims had done a minimum of 30 dives, so experience per se is not necessarily protective. Factors such as recency of diving and relevance of experience were highlighted in this series, as was the need for specific skills and specialised training for more challenging environments.
It is likely that lack of recent diving affects the current competency of a diver and can be contributory to accidents. At least 12 of the scuba victims had not dived for periods ranging from six months to 11 years. A recurring theme in diving accident reports and also suggested in this series is ‘experienced’ divers getting into difficulties after an extended absence from diving. Unless practiced, it is inevitable that diving skills will deteriorate over time so re-familiarisation under controlled conditions is well-advised. Because certain medical conditions can affect diving safety, any potential change in an individual’s fitness to dive needs to be carefully considered and acted upon. Equipment requires proper inspection and servicing, especially after not being used for an extended period as deterioration can occur.[ 12]
It is concerning that 16 (13%) deaths in this series involved student divers, 11 of these 16 being novices, while participating in sanctioned training or an introductory scuba experience. Poor planning and inadequate supervision, often in adverse conditions, was identified as major contributors to many of these.[ 11 , 13]
BUDDY SYSTEM
The absence, or breakdown, of the ‘buddy system’ is another recurring theme in dive fatality reports.[ 2 , 47 , 48] However, it can sometimes be difficult to determine exactly when the actual separation occurred and at what stage of the chain of events. In this series, little more than one quarter of the victims were reported to have been with a buddy at the time of their demise. Although this is higher than the 18% reported in an earlier Australian series,[ 2] it indicates an on-going problem that needs to be further addressed.
The buddy system is taught to trainees as an important part of diving safety in a hostile environment where a diver might need assistance with equipment, entanglement, breathing gas supply, managing sea conditions and a variety of other potential problems. Training in self-sufficiency and the carrying of redundant equipment is a valuable safety measure. However, a well-trained and vigilant buddy can be an important asset in an emergency.
Perhaps with the exception of a team trained in that manner, diving in buddy groups larger than two introduces additional challenges in monitoring and maintaining contact.[ 4] In this series, victims were more than three times as likely to have separated if they were diving in a buddy group larger than two.
BECOMING POSITIVELY BUOYANT IN AN EMERGENCY
Delay to resuscitation adversely affects the outcome and precious time is lost if it is necessary to locate and recover a victim underwater. Therefore, it is better for an unconscious diver to be at the surface, rather than requiring a search and recovery from underwater.[ 49] It follows that, if a diver is in danger of becoming unconscious, whether underwater or on the surface, it is important to attain positive buoyancy. This can be achieved by inflating the BCD, ditching weights, or both. The exception to this is during a overhead environment dive where the surface is not directly accessible.
In an earlier review of Australian compressed gas diving-related fatalities, almost three quarters of the victims were found wearing their weights.[ 2] In this 2001–13 series, at least two thirds (possibly up to 82%) of the divers still had their weights in situ at the time of attempted rescue or recovery. This highlights an on-going problem of divers being reluctant, or unable, to effectively gain positive buoyancy in an emergency. In many cases it is probable that, by the time the divers recognised the need to do so they were too incapacitated to act effectively. Ditching the weight belt is an important emergency measure and training drill for divers, and needs to be practiced, embedded and periodically revisited.
ANNUAL SCUBA DIVING FATALITIES IN AUSTRALIA
Despite various progressive improvements over time, including the increasing and now ubiquitous use of BCDs, the authors are not aware of any clear ‘intervention’ such as new equipment, procedures or regulations that would explain the apparent plateauing of the annual fatalities as indicated in Figure 3. However, it appears likely that the trend resulted from reduced scuba diving activity and this will be discussed in a future report.
LIMITATIONS
As with any uncontrolled case series, the collection and analysis of the fatality data are subject to inevitable limitations and uncertainties associated with the investigations. Witness reports varied in their likely reliability. Police reports varied in their content, often related to the expertise of the investigators. Given that many incidents were unwitnessed, some of the assertions in the reports are speculative. Many data items were not available which rendered the study data incomplete, thus limiting the conclusions that can be drawn.
Conclusions
The older age of victims in this series may reflect a diving population with an increasing prevalence of age-related and chronic medical conditions. The high prevalence of obesity among these victims suggests that obesity may be a likely risk factor in such deaths, possibly due to cardiac stress and reduced fitness and mobility.
The higher frequency of deaths in NSW and Queensland likely reflects the greater participation in these states. The high proportion of deaths in overseas tourists diving with commercial operators in Queensland is consistent with the popularity of diving on the Great Barrier Reef but highlights an on-going need for appropriate screening and monitoring in what may be a higher risk cohort.
The substantial number of deaths that occurred during training or an introductory scuba experience highlights the importance of careful assessment of the dive site, the prevailing conditions, an appropriate instructor-student ratio and close supervision.
Mortality may also be reduced with improved buddy selection and monitoring, training in solo diving for those who do so, as well as greater emphasis and practice on the benefits of attaining positive buoyancy in the event of impending unconsciousness in the water.
Recommendation: Data collection for diving fatalities in Australia and elsewhere would be improved and standardised by the use of specific, dedicated proformas. An example of which can be found at: https://adsf.org.au/wp-content/uploads/2019/04/Data-Collection-1.pdf.
Footnotes
Acknowledgements
The authors acknowledge Monash University National Centre for Coronial Information for providing access to the National Coronial Information System; State and Territory Coronial Offices; various police officers, dive operators and divers who provided information on these fatalities. Acknowledgements are also due to Dr Douglas Walker and Dr Carl Edmonds for pioneering the investigation of diving fatalities in Australia, and to Dr Chris Lawrence, Dr Andrew Fock, Scott Jamieson, Tom Wodak, Dr Douglas Walker and Dr Richard Harris for their contributions to the annual case series.
Conflicts of interest and funding:
The authors have no conflicts to declare. This study was funded by DAN Asia Pacific and the ADSF.
Contributor Information
John Lippmann, Australasian Diving Safety Foundation, Canterbury, Victoria, Australia; Department of Public Health and Preventive Medicine, Monash University, Victoria, Australia.
Christopher Stevenson, School of Health and Social Development, Deakin University, Melbourne, Australia.
David McD Taylor, Emergency Department, Austin Hospital, Victoria, Australia; Department of Medicine, Melbourne University, Victoria, Australia.
References
- Buzzacott P, editor. A report on 2015 diving fatalities, injuries and incidents [Internet]. Durham (NC): Divers Alert Network; 2016. Available from: https://www.diversalertnetwork.org/medical/report/AnnualDivingReport-2017Edition.pdf. [cited 2019 September 21]. [Google Scholar]
- Lippmann J, Baddeley A, Vann R, Walker D. An analysis of the causes of compressed gas diving fatalities in Australia from 1972–2005 . Undersea Hyperb Med. 2013;40:49–61. [PubMed] [Google Scholar]
- Vann R, Lang M. Recreational diving fatalities . Undersea Hyperb Med. 2011;38:257–60. [PubMed] [Google Scholar]
- Cumming B, Peddie C, Watson J. A review of the nature of diving in the United Kingdom and of diving fatalities (1998–2009). In: Vann RD, Lang MA, editors . Recreational diving fatalities. Proceedings of the Divers Alert Network 2010 April 8–10 workshop. Durham (NC): Divers Alert Network; 2011. p. 99- 117. Available from: https://www.diversalertnetwork.org/files/Fatalities_Proceedings.pdf [cited 2019 July 21 [Google Scholar]
- Denoble PJ, Marroni A, Vann RD. Annual fatality rates and associated risk factors for recreational scuba diving.. In: Vann RD, Lang MA, editors . Recreational diving fatalities. Proceedings of the Divers Alert Network 2010 April 8–10 workshop. Durham (NC): Divers Alert Network; 2011. p. 73- 85. https://www.diversalertnetwork.org/files/Fatalities_Proceedings.pdf [cited 2019 July 21 [Google Scholar]
- Denoble PJ, Caruso JL, de L Dear G, Pieper CF, Vann RD. Common causes of open-circuit recreational diving fatalities . Undersea Hyperb Med. 2008;35:393–406. [PubMed] [Google Scholar]
- Germonpré P. The medical risks of underwater diving and their control . Int Sport Med J. 2006;7:1–15. [Google Scholar]
- Lippmann J, Stevenson C, McD Taylor D, Williams J. Estimating the risk of a diving fatality in Australia. Diving Hyperb Med. 2016;46:241–6. [PubMed] [Google Scholar]
- Denoble PJ, Pollock NW, Vaithiyanathan P, Caruso JL, Dovenbarger JA, Vann RD. Scuba injury death rate among insured DAN members . Diving Hyperb Med. 2008;38:182–8. [PubMed] [Google Scholar]
- Lippmann J, Lawrence C, Fock A, Jamieson S. Provisional report on diving-related fatalities in Australian waters 2012 . Diving Hyperb Med. 2018;48:141–67. doi: 10.28920/dhm48.3.141-167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lippmann J, Lawrence C, Fock A, Jamieson S, Harris R. Provisional report on diving-related fatalities in Australian waters 2011 . Diving Hyperb Med. 2016;46:207–40. [PubMed] [Google Scholar]
- Lippmann J, Lawrence C, Fock A, Wodak T, Jamieson S. Provisional report on diving-related fatalities in Australian waters 2010 . Diving Hyperb Med. 2015;45:154–75. [PubMed] [Google Scholar]
- Lippmann J, Lawrence C, Fock A, Wodak T, Jamieson S. Provisional report on diving-related fatalities in Australian waters 2009 . Diving Hyperb Med. 2013;43:194–217. [PubMed] [Google Scholar]
- Lippmann J, Walker D, Lawrence C, Fock A, Wodak T, Harris R, et al. Provisional report on diving-related fatalities in Australian waters 2008 . Diving Hyperb Med. 2013;43:16–34. [PubMed] [Google Scholar]
- Lippmann J, Walker D, Lawrence CL, Fock A, Wodak T, Jamieson S, et al. Provisional report on diving-related fatalities in Australian waters 2007 . Diving Hyperb Med. 2012;42:151–70. [PubMed] [Google Scholar]
- Lippmann J, Walker D, Lawrence C, Fock A, Wodak T, Jamieson S, et al. Provisional report on diving-related fatalities in Australian waters 2006 . Diving Hyperb Med. 2011;41:70–84. [PubMed] [Google Scholar]
- Walker D, Lippmann J, Lawrence C, Fock A, Wodak T, Jamieson S. Provisional report on diving-related fatalities in Australian waters 2005 . Diving Hyperb Med. 2010;40:131–49. [PubMed] [Google Scholar]
- Walker D, Lippmann J, Lawrence C, Houston J, Fock A. Provisional report on diving-related fatalities in Australian waters 2004 . Diving Hyperb Med. 2009;39:138–61. [PubMed] [Google Scholar]
- Walker D, Lippmann J. Provisional report on diving-related fatalities in Australian waters 2003 . Diving Hyperb Med. 2009;39:138–61. [PubMed] [Google Scholar]
- Walker D. Provisional report on diving-related fatalities in Australian waters 2002 . Diving Hyperb Med. 2008;38:8–28. [PubMed] [Google Scholar]
- Walker D. Provisional report on diving-related fatalities in Australian waters 2001 . Diving Hyperb Med. 2006;36:122–38. [PubMed] [Google Scholar]
- National Coronial Information System (NCIS) [Internet]. Administered by the Victorian Department of Justice and Regulation. Available from: http://www.ncis.org.au. [cited 2019 July 12]
- StataCorp. Stata Statistical Software: Release 15. College Station (TX): StataCorp LLC; 2017. [Google Scholar]
- Kim HJ, Fay MP, Feuer EJ, Midthune DN. Permutation tests for joinpoint regression with applications to cancer rates . Stat Med. 2000;19:335–51. doi: 10.1002/(sici)1097-0258(20000215)19:3<335::aid-sim336>3.0.co;2-z. [DOI] [PubMed] [Google Scholar]
- National Cancer Institute . Joinpoint trend analysis software. Version 4.5.0.1. Bethesda (MD): National Cancer Institute Statistical Methodology and Applications Branch, Surveillance Research Program; 2017. [Google Scholar]
- Standards Australia/Standards New Zealand . AS/NZS 2299.1:2015. Occupational diving operations. Part 1: Standard operational practice. Sydney: SAI Global Ltd; 2015. [Google Scholar]
- Lippmann J, McD Taylor D, Stevenson C, Williams JW. Challenges in profiling Australian scuba divers through surveys . Diving Hyperb Med. 2018;48:23–30. doi: 10.28920/dhm48.1.23-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Australian Bureau of Statistics [Internet] . 4364.0.55.001- National Health Survey: First results 2014–15. 2015. [cited 2017 February 04]. Available from: http://www.abs.gov.au/ausstats/abs@.nsf/Lookup/by%20Subject/4364.0.55.001~2014-15~Main%20Features~About%20the%20National%20Health%20Survey~3.
- Cohen A, Baker J, Ardern CI. Association between body mass index, physical activity, and health-related quality of life in Canadian adults . J Aging Phys Act. 2016;24:32–8. doi: 10.1123/japa.2014-0169. [DOI] [PubMed] [Google Scholar]
- Glogner S, Rosengren A, Olsson M, Gudbjörnsdottir S, Svensson AM, Lind M. The association between BMI and hospitalization for heart failure in 83,021 persons with Type 2 diabetes: a population-based study from the Swedish National Diabetes Registry . Diabet Med. 2014;31:586–94. doi: 10.111/dme.12340. [DOI] [PubMed] [Google Scholar]
- Müller-Nordhorn J, Muckelbauer R, Englert H, Grittner U, Berger H, Sonntag F, et al. Longitudinal association between body mass index and health-related quality of life . PLoS One. 2014;9(3):e93071-e. doi: 10.1371/journal/pone.009071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kearns B, Ara R, Young T, Relton C. Association between body mass index and health-related quality of life, and the impact of self-reported long-term conditions – cross-sectional study from the south Yorkshire cohort dataset . BMC Public Health. 2013;13:1009. doi: 10.1186/1471-2458-13-1009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Adabag S, Huxley RR, Lopez FL, Chen LY, Sotoodehnia N, Siscovick D, et al. Obesity related risk of sudden cardiac death in the atherosclerosis risk in communities study . Heart. 2015;101:215–21. doi: 10.1136/heartjnl-2015-307485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Plourde B, Sarrazin J-F, Nault I, Poirier P. Sudden cardiac death and obesity . Expert Rev Cardiovasc Ther. 2014;12:1099–110. doi: 10.1586/14779072.2014.952283. [DOI] [PubMed] [Google Scholar]
- Tavora F, Zhang Y, Zhang M, Li L, Ripple M, Fowler D, et al. Cardiomegaly is a common arrhythmogenic substrate in adult sudden cardiac deaths, and is associated with obesity . Pathology. 2012;44:187–91. doi: 10.1097/PAT.0b013e3283513f54. [DOI] [PubMed] [Google Scholar]
- Eckel RH. Obesity and heart disease: A statement for healthcare professionals from the Nutrition Committee, American Heart Association . Circulation. 1997;96:3248–50. doi: 10.1161/01.cir.96.9.3248. [DOI] [PubMed] [Google Scholar]
- Wilson PW. Established risk factors and coronary artery disease: The Framingham study . Am J Hypertens. 1994;7:7S–12S. doi: 10.1093/ajh/7.7.7s. [DOI] [PubMed] [Google Scholar]
- Binney J. The recreational dive and snorkelling in the Great Barrier Reef: Profile, economic contributions, risk and opportunities. Research publication No. 95. Queensland: Great Barrier Reef Marine Park Authority; 2009. Available from: http://elibrary.gbrmpa.gov.au/jspui/bitstream/11017/435/1/Recreational-dive-and-snorkelling-industry-GBRMP.pdf. [cited 2019 September 12]. [Google Scholar]
- Queensland Government. Recreational diving, recreational technical diving and snorkelling code of practice 2018. Office of Industrial Relations. Queensland: Workplace Health and Safety Queensland; 2018. Available from: https://www.worksafe.qld.gov.au/__data/assets/pdf_file/0004/152329/rec-diving-rec-tech-diving-snorkelling-COP-2018.pdf. [cited 2018 February 25]. [Google Scholar]
- Dive Industry Victoria Association. Code of practice for commercial providers of recreational snorkelling and scuba diving services in Victoria. Melbourne (VIC): Dive Industry Victoria Association; 2018. Available from: http://divingvictoriaassociation.com.au/?s=code+of+practice. [cited 2019 June 25]. [Google Scholar]
- Committee of Australian Sport and Recreation Officials (formerly, ‘Standing Committee on Recreation and Sport’) [Internet]. Participation in exercise, recreation and sport annual report 2010. Canberra: CASRO; 2011. Available from: http://www.ausport.gov.au/information/casro/ERASS. [cited 2016 December 12]. [Google Scholar]
- Walker D. Report on Australian diving deaths 1972–1993. Melbourne: JL Publications; 1998. [Google Scholar]
- Buzzacott P, Rosenberg M, Pikora T. Western Australian recreational scuba diving fatalities, 1992–2005 . Aust NZ J Public Health. 2009;33:212–4. doi: 10.1111/j.1753-6405.2009.00377.x. [DOI] [PubMed] [Google Scholar]
- Lagache E. Are divers choosing to die? Undersea J. 1993; 4: 50- 7. [Google Scholar]
- International Organisation for Standardisation . ISO 24801-2:2014. Recreational diving services – Safety-related minimum requirements for the training of recreational scuba divers – Part 2: Level 2 – Autonomous diver. Geneva: International Organisation for Standardisation; 2007. [Google Scholar]
- Recreational Scuba Training Council (RSTC) . Minimum course requirement for open water diver certification. Jacksonville (FL): Recreational Scuba Training Council; 2004. Available from: http://wrstc.com/downloads/03%20-%20Open%20Water%20Diver.pdf. [cited 2017 December 21] [Google Scholar]
- Buzzacott P, editor. Annual diving report: 2016 edition (Based on 2014 diving fatalities, injuries and incidents). Durham (NC): Divers Alert Network; 2016. Available from: https://www.diversalertnetwork.org/medical/report/AnnualDivingReport-2016Edition.pdf. [cited 2019 September 12] . [Google Scholar]
- McClelland A. Diving-related deaths in New Zealand 2000–2006 . Diving Hyperb Med. 2007;37:174–88. [Google Scholar]
- Harpur GD. Hypoxia in out-of-air ascents: a preliminary report. SPUMS Journal. 1994;14:24–28. [Google Scholar]