

Abstract
Following the emergence of COVID-19 outbreak, numbers of studies have been conducted to curtail the global spread of the virus by identifying epidemiological changes of the disease through developing statistical models, estimation of the basic reproduction number, displaying the daily reports of confirmed and deaths cases, which are closely related to the present study. Reliable and comprehensive estimation method of the epidemiological data is required to understand the actual situation of fatalities caused by the epidemic. Case fatality rate (CFR) is one of the cardinal epidemiological parameters that adequately explains epidemiology of the outbreak of a disease. In the present study, we employed two statistical regression models such as the linear and polynomial models in order to estimate the CFR, based on the early phase of COVID-19 outbreak in Nigeria (44 days since first reported COVID-19 death). The estimate of the CFR was determined based on cumulative number of confirmed cases and deaths reported from 23 March to 30 April, 2020. The results from the linear model estimated that the CFR was 3.11% (95% CI: 2.59% – 3.80%) with R2 value of 90% and p-value of < 0.0001. The findings from the polynomial model suggest that the CFR associated with the Nigerian outbreak is 3.0% and may range from 2.23% to 3.42% with R2 value of 93% and p-value of <0.0001. Therefore, the polynomial regression model with the higher R2 value fits the dataset well and provides better estimate of CFR for the reported COVID-19 cases in Nigeria.
Keywords: Coronavirus, COVID-19, SARS-CoV-2, Case fatality rate (CFR), Epidemiology, Regression analysis
1. Introduction
Coronavirus disease 2019 (COVID-19) is a novel viral disease caused by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), which led to a global pandemic. The virus was first discovered and reported in Wuhan, China, in December 2019, which were later reported in other countries [1]. As of 30 April 2020, more than three million confirmed cases of COVID-19 were reported globally with 217,769 deaths [2]. However, Nigeria had 1,932 confirmed, 319 discharged and 58 death cases of COVID-19 spreading across 34 states and the Federal Capital Territory FCT on that day [3].
Nigeria reported first COVID-19 confirmed case on 27 February 2020, when an Italian citizen tested positive for the virus. Consequently, the government, like other governments of affected countries, implemented non-pharmaceutical interventions to contain the spread of the virus in the country. As of 20 March 2020, the Nigerian government restricted international travel on 15 high incidence countries namely, China, Italy, Iran, Norway, South Korea, Spain, Japan, France, Germany, United States of America, United Kingdom, Netherlands, Switzerland, Sweden and Austria [4]. The temporary closure of schools was imposed on 20 March 2020 [5]. Among others interventions including border restriction, work-from-home arrangements for civil servants, restrictions of social and religious gatherings, wearing of facial masks, social distancing, states and national lockdowns were implemented on 30 March 2020.
Following the emergence of COVID-19 and its global spread, numbers of studies have been conducted to examine statistical model of epidemiology data [6]. The COVID-19 cases were investigated using dynamic statistical techniques [7], estimation of fatality rate of COVID-19 was studied [8] and, the transmission dynamics of the virus was examined [9].
Despite the rapid spread of the virus and continuous rising cases and deaths in the recent days especially in Nigeria, there is still lack of studies estimating the CFR of the outbreak in timeline of the pandemic. The CFR is one of the pivotal parameters required to understand the basic epidemiological features of the outbreak [10]. As a result, the present paper estimates the CFR of COVID-19 during the first weeks of first reported death of the pandemic in Nigeria through statistical regression analysis. The CFR represents the proportion of cases who eventually die from a disease [11]. Hopefully, the estimated CFR could provide a better understanding of near future trends for successful control of the global COVID-19 pandemic in Nigeria.
2. Methods
2.1. Source of data
The data used in this work were obtained from the Nigeria Center for Disease Control (NCDC) and World Health Organization (WHO) situation reports, which have been publicly released on their websites [2]. The collected data include cumulative number of COVID-19 confirmed cases and deaths, which are essentials indicators for determining CFR of the epidemic.
2.2. Statistical model
In this study, simple linear and polynomial regression models were used to estimate the CFR of COVID-19 epidemiologic data in Nigeria. In all cases, the cumulative number of confirmed cases termed as predictor variable while cumulative deaths a response variable of the model. The slope of the fitted line was considered as an estimate of the CFR, and the confidence interval (CI, 95%) of CFR was calculated from the standard error of the slope. In order to minimize variation in the course of estimation of the CFR in the initial stage of outbreak when no death occurred, the time since first reported death was used as the starting point of these models. The values of coefficient of determination (R 2, value of 0.91–0.99) usually quantify a tight linear trend and could be as an effective parameter in estimating a good fit for the model [12]. Details of these models were provided in [13]. The expression of linear and polynomial regression model that were used in this study are respectively given in equation. 1 and equation. 2:
| (1) |
| (2) |
where I is the intercept, S, S1, and S2 are the respective slopes of the models.
3. Results and discussions
3.1. Distribution patterns of the collected epidemiological data of COVID-19 in the early phase of the outbreak in Nigeria
The first COVID-19 confirmed case was reported in Nigeria on 27 of February, imported by an Italian citizen. The first fatal death due to the global pandemic was reported on 23 March 2020 [14]. As of 14 April 2020, Nigeria had 12 functional testing facilities in eight states, with a capacity to conduct a minimum of 1,500 tests per day in Lagos state and 1,000 tests per FCT and other states [15]. Until 30 April 2020, the updated situation report by NCDC was given; 15,759 samples were tested, 1,932 confirmed cases, 319 discharge cases and 58 confirmed fatalities were reported in Nigeria. The highest daily number (204) of COVID-19 confirmed cases was reported. The new reported cases in Nigeria increased in a daily basis due to a series of factors, which would facilitate the spread of the virus. The factors may include inadequate of medical supplies, poor medical conditions [16] and scarcity of virus testing centers.
Fig. 1 displays COVID-19 spreading patterns since the confirmation of the first index. The figure suggests that there was a rapid increase in the number of confirmed cases which may lead to gradual increase in deaths cases. Fig. 2 shows the distribution patterns of the epidemic across the top 10 affected states. The selected states for this graph are Lagos, Kano, FCT, Gombe, Borno, Ogun, Edo, Katsina, Bauchi and Sokoto. The graph indicates that the distribution patterns of the epidemiological data could be skewed due to lack of adequate testing centers among other factors in the country. Furthermore, the epidemiological data in Table 1 suggests that Lagos state has the highest number of confirmed cases (50.52%), taking up more than half of the total number of confirmed cases in Nigeria, which indicates the availability of medical care and adequate testing centers in the state. But, Sokoto state, with 36 (1.86%) confirmed cases and number of deaths [4], had the highest mortality rate (11.11%) in Nigeria, this indicates an evidences of poor healthcare services in the state. Other states with the high mortality rates, as depicted in Fig. 3 include Borno (9.09%), Edo (6.81%), Bauchi (5.26%) and Katsina (5.00%). Lack of quality healthcare and insufficient testing centers among other factors may be contributed to the regular rise in mortality rates of COVID-19 in these states.
Fig. 1.

Distribution of COVID-19 epidemiological data in Nigeria showing the trend patterns of cumulative number of confirmed cases and deaths since first reported index.
Fig. 2.
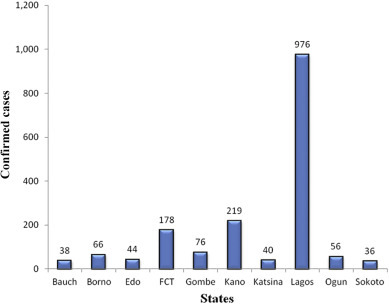
Distribution of COVID-19 epidemiological data in Nigeria Showing top ten states with highest reported cases.
Table 1.
Distribution pattern of top 10 selected COVID-19 states based on cumulative number of confirmed cases since first index in Nigeria. The percentage of cumulative cases (PCC) and mortality rates (MR) in each state were listed.
| Sates | Confirmed cases | PCC (%) | Deaths | MR(%) rounded down |
|---|---|---|---|---|
| Lagos | 976 | 50.5 | 21 | 2.1 |
| Kano | 219 | 11.3 | 3 | 1.3 |
| FCT | 178 | 9.2 | 3 | 1.6 |
| Gombe | 76 | 3.9 | 0 | 0.0 |
| Borno | 66 | 3.4 | 6 | 9.0 |
| Ogun | 56 | 2.9 | 1 | 1.7 |
| Edo | 44 | 2.2 | 3 | 6.8 |
| Katsina | 40 | 2.0 | 2 | 5.0 |
| Bauchi | 38 | 1.9 | 2 | 5.2 |
| Sokoto | 36 | 1.8 | 4 | 11.1 |
Fig. 3.

Distribution of mortality rates by states for top ten selected states.
3.2. Estimation of CFR of COVID-19 in the early phase of the outbreak in Nigeria
The derived results of the fitting models are shown in Fig. 4 A gives the results obtained from linear regression model that estimated the CFR of COVID-19 as 3.11% (95% CI: 2.59%–3.80%) and R 2 − value of 0.90 with p-value<0.0001 for the time period since first reported death until 30 April 2020 in Nigeria. Fig. 4B presents the results of polynomial model that estimated the CFR of COVID-19 for 3.0% (95% CI: 2.23%–3.42%) with value of coefficient of determination, R 2 − value of 0.93 and p-value<0.0001. For all the cases, the results indicate that in the initial stage of COVID-19, the reported confirmed cases and deaths were mostly satisfying both the linear and polynomial models based on linear regression models. Therefore, the estimated CFR in this study based on COVID-19 cumulative confirmed cases and cumulative confirmed deaths derived from both the linear and polynomial models could give better understandings of the epidemic in Nigeria. However, as shown in both figures, three different trends have shown gradual decreasing and increasing patterns at the initial stage of the graphs, which may affect the estimated results of the CFR and can be studied in future.
Fig. 4.

Estimation of CFR using statistical regression models for COVID-19 epidemiological data of 44 days since the first reported death on April 30th, 2020. (A) is the estimation of CFR by simple linear regression model fitting. (B) is the estimation of CFR by polynomial regression model fitting.
4. Recommendations
The estimated CFR level of 0.03% in Nigeria will be maintained in the near future only if there are no significant changes in healthcare facilities, detection methods, continuous clinical treatments, and other factors. Government and relevant stakeholders should provide sufficient bed space and associated clinical care services in order to achieve a successful and effective control of COVID-19 in Nigeria. However, based on our estimate of the CI derived from polynomial regression model, the estimated CFR in Nigeria will be less than 0.3%, if the aforementioned factors will be improved.
5. Conclusion
Since the outbreak of COVID-19 pandemic in China, the virus has been documented across the globe. By 30 April 2020, Nigeria had 1,932 confirmed, 319 discharged and 58 death cases of COVID-19 across 34 states and the FCT. This paper showed the distribution patterns and estimates the CFR of COVID-19 epidemiological data of Nigeria during 44 days of outbreak since first reported death. Since the first pandemic death in Nigeria reported on March 18th, we collected a 44 day epidemic data and computed CFR based on regression model. Compared to other mathematical models like the dynamic transmission model our model is straightforward and does not require complex parameter assumptions. Our findings suggest that the regression mode provides comprehensive estimation of CFR, which could be served as a threshold for successful control of COVID-19 in Nigeria, by studying the future trends of CFR.
Acknowledgements
The authors thanked the NCDC and WHO for the release of COVID-19 data on their websites to conduct this study.
Conflict of interest statement
The authors declare that there are no conflicts of interest.
Author contributions
Ahmad Abubakar Suleiman: Conceptualization, Methodology, Software, Writing- Original draft. Aminu Suleiman: Data curation, Visualization. Usman Aliyu Abdullahi: Investigation, Supervision, Validation. Suleiman Abubakar Suleiman: Writing- Reviewing and Editing.
References
- 1.Kwok K.O., Wong V.W.Y., Wei W.I., Wong S.Y.S., Tang J.W.T. Epidemiological characteristics of the first 53 laboratory - confirmed cases of COVID-19 epidemic in Hong Kong, 13 February 2020. Euro. Surveill. 2020;25(16) doi: 10.2807/1560-7917.ES.2020.25.16.2000155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.WHO Coronavirus Disease (Covid-19) - Situation Report – 101, April 30 2020. 2020. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports (accessed 1 May 2020)
- 3.NCDC COVID-19 case update, 11:50pm April 30th, 2020. 2020. https://ncdc.gov.ng/diseases/ (accessed 1 May 2020)
- 4.Nejo A. Coronavirus : Work from home, Fayemi tells Ekiti civil servant, The Punch newspaper. 2020. https://punchng.com/breaking-coronavirus-work-from-home-fayemi-tells-ekiti-civil-servants (accessed 21 March 2020)
- 5.Adegboye O.A., Adekunle A.I., Gayawan E. Early transmission dynamics of novel coronavirus (COVID-19) in Nigeria. Int. J. Environ. Res. Public Health. 2020;17:3054. doi: 10.3390/ijerph17093054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Zhao S., Musa S.S., Lin Q., Ran J., Yang G., Wang W., Lou Y., Yang L., Gao D., He D. Estimating the unreported number of novel coronavirus (2019-nCoV) cases in China in the first half of January 2020: a data-driven modelling analysis of the early outbreak. J. Clin. Med. 2020;9:388. doi: 10.3390/jcm9020388. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sarkodie S.A., Owusu P.A. Investigating the cases of novel coronavirus disease (COVID-19) in China using dynamic statistical techniques. Heliyon. 2020;6 doi: 10.1016/j.heliyon.2020.e03747. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Yang S., Cao P., Du P., Wu Z., Zhuang Z., Yang L., Yu X., Zhou Q., Feng X., Wang X., Li W., Liu E., Chen J., Chen Y., He D. Early estimation of the case fatality rate of COVID-19 in mainland China: a data-driven analysis. Ann. Transl. Med. 2020;8(4):128. doi: 10.21037/atm.2020.02.66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Li Q., Guan X., Wu P., Wang X., Zhou L., Tong Y., Ren R., Leung K.S., Lau E.H., Wong J.Y. Early transmission dynamics in wuhan, China, of novel coronavirus–infected pneumonia. N. Engl. J. Med. 2020;382:1199–1207. doi: 10.1056/NEJMoa2001316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Wallinga J., Teunis P. Different epidemic curves for severe acute respiratory syndrome reveal similar impacts of control measures. Am. J. Epidemiol. 2004;160:509–516. doi: 10.1093/aje/kwh255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Manuel B., Richard K., Sarah T., Hans H.H., Andreas W.F., Richard N.A. 2019- novel coronavirus (2019-nCoV): estimating the case fatality rate - a word of caution. Swiss Med. Wkly. 2020;150 doi: 10.4414/smw.2020.20203. [DOI] [PubMed] [Google Scholar]
- 12.Öztoprak F., Javed A. Case fatality rate estimation of COVID-19 for European countries: Turkey’s current scenario amidst a global pandemic; comparison of outbreaks with European countries. EJMO. 2020;4(2):149–159. doi: 10.14744/ejmo.2020.60998. [DOI] [Google Scholar]
- 13.Dalah C.M., Singh V.V., Abdullahi I., Suleiman A.A. The study of HIV/AIDS trend in Yobe state for the prescribed period (1999 – 2019) Int. J. Stat. Appl. 2020;10:10–16. doi: 10.5923/j.statistics.20201001.02. [DOI] [Google Scholar]
- 14.Salako O., Okunade K., Habeebu M., Toye M., Oluyede G., Fagbenro G., Salako B. Upheaval in cancer care during the COVID-19 outbreak. Ecancermedicalscience. 2020;14 doi: 10.3332/ecancer.2020.ed97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.NCDC National strategy to scale up access to Coronavirus disease testing in Nigeria. 2020. https://covid19.ncdc.gov.ng/media/files/COVID19TestingStrategy (accessed 16 April 2020)
- 16.Ohia C., Bakarey A.D., Ahmad T. COVID-19 and Nigeria: putting the realities in context. Int. J. Infect. Dis. 2020;95:279–281. doi: 10.1016/j.ijid.2020.04.062. [DOI] [PMC free article] [PubMed] [Google Scholar]