

Abstract
INTRODUCTION:
Adolescence is characterized by a rapid phase of growth and development during which the requirement of nutrition and micronutrients is relatively high. Although there is a decreasing trend in the prevalence of undernutrition among adolescents, the current prevalence of undernutrition is still very high (41.9%). Adolescents with good nutrition knowledge are more likely to follow healthy eating habits. In the light of this, the current study was planned to assess the baseline nutrition-related knowledge of adolescent girls and the effectiveness of nutrition education material (flipchart) in increasing their nutrition-related knowledge.
MATERIALS AND METHODS:
A school-based interventional study was conducted among adolescent girls of class 9th of a school in an urban slum of Delhi. A structured pretested Knowledge Assessment Questionnaire consisting of 10 multiple-choice questions in Hindi with a maximum score of 10 was used. The intervention was a nutrition education session conducted by doctors of Community Health department using specially designed flipcharts covering important aspects of nutrition relevant for adolescent girls. A demonstration of food items and charts and flex material was also given. The total sample size was 265 adolescent girls.
RESULTS:
Baseline knowledge as assessed by mean pretest score was poor (3.698 ± 1.81). The students’ baseline knowledge was significantly associated with mother's educational status (P = 0.024). There was a significant increase (mean difference was 1.7890 ± 0.1434) in the nutrition-related knowledge of the participants after the intervention (P < 0.001). The proportion of students who improved, i.e., 147 (55.47%) was more than proportion who deteriorated (25 [9.43%]) after the educational session. This difference was found to be statistically significant (P ≤ 0.001).
CONCLUSION:
Nutrition knowledge was found poor among school-going adolescent girls, which significantly improved after the nutrition education session.
Keywords: Adolescent girls, flipchart, health education, nutrition, nutrition education, prepost study
Introduction
Adolescents constitute one-fifth of the total population, and India has the largest national population of adolescents (25%) which is 21.0% of the total population of India.[1,2] Adolescents which is defined as age between 10 and 19 years of age is characterized by a rapid phase of growth and development during which the requirement of nutrition and micronutrients is relatively high.[3] Malnutrition in this age group can be due to various factors such as the continuation of childhood malnutrition, food insecurity in households, or faulty dietary habits and food fads. Adolescence is characterized by some psychological changes[4,5] and development of their own personality which impact their dietary habits that can be in either way. Although there is a decreasing trend in the prevalence of under nutrition among the late adolescent group, the current prevalence of under nutrition is still very high (41.9%).[6] Furthermore, the prevalence of anemia is very high (>60%) among this age group.[7] Girls are at much higher risk of malnutrition and related chronic illness due to their reproductive characteristics and other sociocultural issues like negligence toward girl child in the family, early marriages, and teen pregnancy.[3] Skipping the daily meals which leads to undernutrition, and at the same time, consuming junk food and fast food which leads to overweight, is very common among adolescents revealing the double edge of the issue.[8]
Adolescents with good nutrition knowledge are more likely to follow healthy eating habits.[9,10] Therefore, it is very important to educate them about nutrition and explain to them the importance of eating a balanced diet. Nutrition education has been a promising solution to improve dietary habits. Previously also, it has been noted that the lack of knowledge of dietary requirements and nutritive value of various food groups is the main contributor to malnutrition in developing countries like India.[11]
Adolescence is a time period from where the individual starts taking care of themselves almost independently. There is a higher chance for the adolescent to start wrong eating habits in their life.[12] Although this age group is vulnerable to various ill habits, at the same time, it is an age of opportunity. Spreading awareness by nutrition education interventions during these formative years is likely to have positive effects on their current health. This positive benefit will continue into adulthood as healthy preferences for themselves as well as their future families.[13] Nutrition education in this age group has significantly improved nutrition-related behavior and even their academic performance.[11]
Despite various programs and initiatives taken by the Government of India to tackle the problem of malnutrition in the country, involving the adolescent age group, like SABLA, Mid-day Meal Program, ICDS nutrition-related problems still continue to be a major public health problem. Very less importance is given to nutrition education in our existing health programs, and also, there is poor implementation of the nutrition education component of the existing programs.[14,15] There are very few studies conducted, especially in India to see the effect of health education on knowledge related to nutrition. Therefore, this study was planned to see if a simple flipchart containing basic messages about food groups (proteins, carbohydrates, fat, and minerals) and a balanced diet can show some improvement in the pretest scores. This study is especially relevant to the particular social class (lower and lower middle) from which the participants were as, these children are vulnerable to malnutrition due to unavailability of food, adding to it is the lack of knowledge about good food choices and the propaganda about junk food and other unhealthy food choices in media, social media, movies, etc.
Materials and Methods
The present study was an interventional study designed to spread nutrition-related knowledge among the adolescents as well as to assess the effectiveness of the nutrition education material (flipchart) prepared. A school-based pre–post study was conducted among adolescent girls of class 9th of a government high school situated in an urban slum of Delhi. Due permissions were obtained from the principal of the school and Institutional Ethical Committee. Class 9th was selected according to the availability, as the remaining classes with adolescent students were involved in other school activities (mainly examinations and class tests); therefore, the school principal gave permission to conduct the study in adolescent girls studying in the ninth standard only. The inclusion criteria were as follows:
Permission to conduct the study was granted by the school principal
Age between 10 and 18 years old
Studying in the selected government school of Delhi, which was situated in a slum and resettlement colony of East Delhi
Present in school on the day of the intervention, i.e., the nutrition education session using “Flipchart”
Gave verbal consent to become part of the study.
Those who did not fulfill these inclusion criteria were excluded by corollary. The participants were explained about the study completely, and assent was obtained by a show of hands. They were told that their participation was purely voluntary and that they could leave the session and the study midway without any repercussions.
A structured pretested Knowledge Assessment Questionnaire consisting of 10 multiple-choice questions in the local language (Hindi) with maximum scoring 10 was administered. The score obtained by the study subjects was further categorized as poor (0–4), good (5–7), and better (8–9). A perfect score of 10 was considered as “best”. The questions were about balanced diet, various food groups (carbohydrates, fats, proteins, vitamins, and minerals), and their nutritive value and anemia.
The items included in the questionnaire were:
Balanced Diet
Protein-rich food items
Carbohydrate-rich food items
Fat-rich food items
Calories in 1 g fat
Body mass index (BMI) formula
Normal BMI in adults
Food items to prevent Anemia
Symptoms of Anemia
Lack of which nutrient in the diet causes anemia.
Variables controlled were parents’ education and the age of the participant. It was assumed that girls coming to a government school in a slum area must belong to a similar social class. All participants belonged to the same class in the school, i.e., the ninth standard. Therefore, it can also be assumed that their exposure to information about nutrition in the curriculum would be similar. These variables were used to compare the results at the time of analysis. The participants were given 15 min to answer this pretest.
The intervention was a nutrition education session conducted by doctors of the Community Health Department using the flipcharts [Figure 1] for students in four groups. Girls were explained about balanced diet and importance of including macro- and micronutrients in their diet, giving examples to make it interesting. Questions were encouraged and a two-way discussion was fostered. Participation was encouraged by calling few to the front and repeat the key messages imparted during the session. The talk was given in a friendly and light atmosphere. The session took 45 min. Posttest was administered on the same day, immediately after the session and demonstration.
Figure 1.
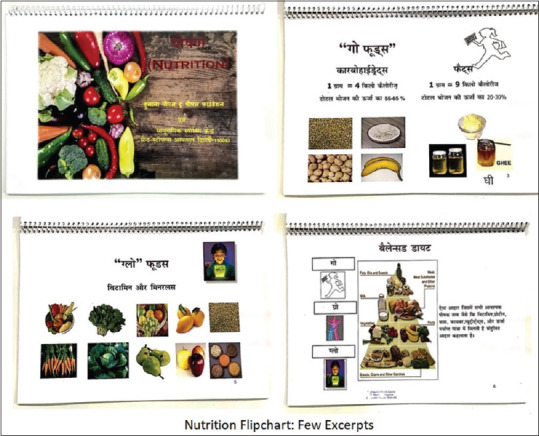
Excerpts from “Nutrition” flipchart used to conduct the education session intervention
A demonstration of food items of various groups and easy methods of including them in our daily diet to make it a balanced meal was also explained. The auxiliary nurse midwives (ANMs) and development assistants of our department were involved in this demonstration, which was held at a common area for all students. Proper training and meetings were conducted with them beforehand to explain the sequence of events of the intervention, and they were also trained about the demonstration of the food groups. Many posters and flex material on nutrition were also displayed. Permission was obtained from the school principal and verbal consent was obtained from all the participating students.
The main outcome variable was an improvement in nutrition-related knowledge of the study subjects. Data were recorded and organized in MS Excel and analyzed on SPSS16. Qualitative data were assessed by McNemar test and McNemar–Bowker test and test scores were assessed by paired t-test, ANOVA test, and Krauskal–Wallis test; P < 0.05 was taken as statistically significant.
Results
A total of 286 students answered the pretest, but there were 21 dropouts (7.3%) as some students had an examination on the day, and 265 students answered the posttest. Therefore, analysis of 265 students was done. All the girls were in the age group of 13–15 years [Table 1]. The baseline knowledge as assessed by mean pretest score was poor (3.698 ± 1.81). The education of parents was thought to be an important determinant of baseline knowledge. The parents of majority study subjects were poorly educated (66.8% mothers and 50.4% fathers were illiterate or were educated till less than primary school) [Table 2]. On assessing the students’ baseline knowledge with a mother's education, it was found that there was a positive association between their mean pretest score and their mother's education (P < 0.024) [Table 3]. The mean pretest score was highest (4.176) of students whose mother's had more than 10 years of schooling (P < 0.024). On comparison of the baseline scores with fathers’ education, no significant association was observed [Table 4].
Table 1.
Distribution of the study subjects based on the age of study subjects
| Age group | Frequency (%) |
|---|---|
| 13-15 | 173 (65.3) |
| 15-17 | 63 (23.8) |
| 17-19 | 29 (10.9) |
| Total | 265 (100.0) |
Table 2.
Distribution of the study subjects based on the parent’s education status
| Education status | Mother’s education n (%) | Father’s education n (%) |
|---|---|---|
| Illiterate - 5th class | 177 (66.8%) | 133 (50.4%) |
| Class 6-10th pass | 71 (26.7%) | 88 (33.3%) |
| >10th pass | 17 (6.4%) | 43 (16.2%) |
| Total | 265 (100%) | 264* (100%) |
*One participant did not give information on father’s education status
Table 3.
Association of mean pretest score with mother’s education
| Mother’s education | n | Mean pretest score±SD |
|---|---|---|
| Illiterate - 5th class | 177 | 3.565±1.9092 |
| Class 6-10th pass | 71 | 3.915±1.5834 |
| >10th pass | 17 | 4.176±1.5506 |
| Total | 265 | 3.698±1.8110 |
P<0.024, Kruskal -Wallis test. SD: Standard deviation
Table 4.
Association of mean pretest score with father’s education (n=264*)
| Father’s education | n | Mean±SD |
|---|---|---|
| Illiterate - 5th class | 133 | 3.752±2.0204 |
| Class 6th-10th pass | 88 | 3.591±1.6091 |
| >10th pass | 43 | 3.721±1.5326 |
| Total | 264* | 3.693±1.8127 |
ANOVA, P=0.808. *One participant did not give information on father’s education level. SD: Standard deviation
The mean score of the students in pretest was 3.698 ± 1.703 which increased to 5.487 ± 1.811 after the intervention. The mean difference was 1.7890 ± 0.1434. There was a significant increase in the nutrition-related knowledge of the participants after the intervention (P < 0.001) [Table 5]. Overall, the study subjects improved from “poor” score to “better” score after our intervention. The maximum score obtained in posttest was 9 of 10.
Table 5.
Comparison of test score before and after intervention
| Score | n | Mean±2SD | Mean difference±2SE | P |
|---|---|---|---|---|
| Pretest score | 265 | 3.698±1.703 | 1.7890±0.1434 | <0.001 |
| Posttest score | 265 | 5.487±1.811 |
Paired t-test. t, dF=12.475,264. SE: Standard error, SD: Standard deviation
It was interesting to know that although the baseline knowledge regarding symptoms of anemia was very low (13.96%), but at the same time, 71.32% of the children could answer correctly about the iron-rich food which prevents anemia. Protein-rich food was correctly identified by 73.96% of the participants. Posttest scores improved in questions about balanced diet, protein-rich food, carbohydrate-rich food, fat-rich food, iron-rich food, symptoms of anemia, and cause of anemia. There was a significant improvement in knowledge after intervention except response to the question on “the nutrient whose deficiency causes Anemia?” [Table 6].
Table 6.
Item wise comparison of accuracy before and after test
| Items of questionnaire | Overall correct response | Discordant pair of response | Test statistic# | P | ||
|---|---|---|---|---|---|---|
| Correct pretest, n (%) | Correct posttest, n (%) | Correct posttest -incorrect pretest | Incorrect Posttest -correct pretest | |||
| Balanced diet | 64 (24.15) | 106 (40.0) | 72 (27.16) | 30 (11.32) | 16.480 | <0.001 |
| Protein rich food items | 196 (73.96) | 231 (87.17) | 51 (19.24) | 16 (6.03) | 17.253 | <0.001 |
| Carbohydrate rich food items | 76 (28.68) | 110 (41.50) | 71 (26.79) | 37 (13.96) | 10.083 | <0.001 |
| Fat rich food items | 135 (50.94) | 201 (75.85) | 96 (36.22) | 30 (11.32) | 33.531 | <0.001 |
| Calories in 1 g fat | 61 (23.02) | 173 (65.28) | 134 (50.56) | 22 (8.30) | 78.981 | <0.001 |
| BMI formula | 92 (34.71) | 152 (57.35) | 91 (34.33) | 31 (11.69) | 28.533 | <0.001 |
| Normal BMI in adult | 38 (14.33) | 165 (62.26) | 136 (51.32) | 9 (3.39) | 109.49 | <0.001 |
| Food items to prevent anemia | 189 (71.32) | 219 (82.64) | 53 (20.0) | 23 (8.67) | 11.065 | <0.001 |
| Symptoms of anemia | 37 (13.96) | 63 (23.77) | 45 (16.98) | 19 (7.16) | 9.765 | <0.002 |
| Anemia causing nutrient | 56 (21.13) | 72 (27.17) | 50 (18.86) | 34 (12.83) | 2.678 | <0.102 |
#dF=1, McNemar test for discordant pairs. BMI: Body mass index
According to the pretest scores, 191 (72.08%) students had performed poor, 63 (23.77%) performed good, and 11 (4.15%) had performed better. Posttest scores revealed that 72 (27.17%) students had performed poor, 165 (62.26%) had performed good, and 28 (10.57%) students had performed better. Of 191 students who performed poorly in pretest, 55 (28.79%) remained poor, 120 (62.83%) performed good, and 16 (8.38%) performed better. Among 63 students, who performed good, 15 (23.81%) deteriorated to poor, 37 (58.73%) remained good, and 11 (17.46%) performed better. Similarly, of 11 who performed better, 10 (90.91%) deteriorated to poor and good, while 1 remain better (9.09%). The proportion of students who improved, i.e., 147 (55.47%) was more than proportion who deteriorated (25 [9.43%]). This difference in proportion was found to be statistically significant (McNemar–Bowker test, P ≤ 0.001) [Table 7].
Table 7.
Comparison of performance before and after intervention
| Performance before intervention | Performance after intervention | Total, n (%) | ||
|---|---|---|---|---|
| “Poor,” n (%) | “Good,” n (%) | “Better,” n (%) | ||
| Poor | 55 (28.8) | 120 (62.8) | 16 (8.4) | 191 (100) |
| Good | 15 (23.8) | 37 (58.7) | 11 (17.5) | 63 (100) |
| Better | 2 (18.2) | 8 (72.7) | 1 (9.1) | 11 (100) |
| Total | 72 (27.2) | 165 (62.3) | 28 (10.6) | 265 (100) |
McNemar-Bowker test criterion value - 93.029. P<0.001
Discussion
This study aimed to observe the difference a nutrition education session could make in the knowledge of adolescent girls regarding balanced diet, the importance of various food groups (containing macro- and micronutrients) in a daily diet, understanding the causation, symptoms, effects of anemia, and malnutrition in a manner different from their regular classroom teaching, using a colorful flipchart and demonstration.
Nutrition is covered in school textbooks, but sessions like ours make the information imparted more interesting for adolescents, and practical tips to incorporate healthy nutrition practices could also be explained. Previously also, studies have noted that school-based nutrition interventions can play a major role in dietary change among adolescents.[16] Interactive and participatory approach of learning gives rich dividends for improving knowledge, which is the first step toward behavior change.
We conducted the nutrition education session among adolescent girls studying in a government school, and the children coming to this school, which is situated in a slum and resettlement colony, had a similar socioeconomic background as all children coming to that school were from the same community. The importance of having correct information about nutrition is even greater for adolescents coming from disadvantaged sections as they can carry that knowledge to their homes and help families in modifying the meal planning to include nutritious and balanced choices for their meals. In a seminal study by 2019 Economics Nobel Prize winners, Banerjee and Duflo, it was observed that in India, the poor do not spend whatever little money they have on food.[17] Among nonfood items, a significant amount was spent on purchasing alcohol and tobacco.[17] The authors noted that, even for the extremely poor, for every 1 percent increase in the food expenditure, about half goes into purchasing more calories, and half goes into purchasing more expensive (and presumably better tasting) calories.[17] This gap between theory and practice can be bridged by adolescents if they know the importance of nutritious balanced and wholesome food.
Adolescence is a transition phase between childhood and adulthood.[18] Rapid developmental and behavioral changes occur with increased risk-taking behavior, emotional reactivity, and autonomy.[19] Future behavior patterns affecting adult health are established during adolescence.[20]
Apart from affecting their own future lives, knowledge about healthy behaviors influences their current/present family and also their future family after marriage in case of adolescent girls. Especially in case of knowledge about healthy diet and nutrition, this holds true as traditionally in Indian society, women cook and young girls help their mothers in preparing food for the entire family. Many times adolescent girls cook the entire meal themselves for their family. Educating the adolescent girl about nutrition can therefore have an effect on food choices for the entire family for a lifetime. We also observed that with increasing educational status of mothers, the pretest scores of study subjects improved. Therefore, mother's education had a significant role in nutrition-related knowledge of their adolescent girls. This showed that the old adage “educate a women and she educates the family” holds true. In a study by Giuseppe Grosso et al. too, a similar significant association was present between nutrition knowledge of participants’ and parents’ education level. The mean score of participants was 8.5 (standard deviation [SD] = 4.9) in students whose parents were uneducated and 12.3 (SD = 2.6) among students whose parents had completed university education.[9]
The health, and even more importantly, the knowledge, attitudes, and practices of adolescents are regarded as essential factors when predicting the process of epidemiological transition of a population. The current lifestyles of adolescents, such as eating habits and reproductive behavior, are crucial for the health and disease patterns that will be observed in future.[21] The parallel processes of demographic and epidemiological transition are currently occurring at a remarkable speed in India.[22] Today, every fifth person in India is an adolescent.[23] The food choices our children make today, will have an immense bearing on the health status of Indian population in future, when they grow up. Therefore, equipping adolescents with correct and practical knowledge about healthy and balanced food will have far-reaching consequences for the country too. Adolescence should not be considered only as an age of vulnerability but should be seen as an age of opportunity.
Nutrition education is widely used for a range of population groups as a medium to deliver healthy diet and nutrition information.[24] Flipcharts are an easy and less expensive method to give information to small groups of people. It is re-usable, easy to carry, and hold the attention of the audience as it uses few words and many pictures to explain the message. Furthermore, this medium is not as impersonal as mass media, and questions from the audience are encouraged. The information can easily be adapted to cater to local needs. This method is very suitable to give nutrition education to poor people also who may be illiterate, and therefore, pictorial messages may be easily understood and remembered. This method may be easily applicable for use at the primary health care (PHC) level for improving the knowledge and practices of the people. ANMs and ASHA workers can be trained to use these flipcharts to conduct their community meetings, and using flipcharts helps to standardize the key messages that are imparted by these different cadres of health workers at the PHC level.
The study also revealed that there is a significant improvement in nutrition-related knowledge after giving one nutrition session using a flipchart, demonstration of food groups and methods of including them in the diet. Similarly, nutrition education as an effective tool in imparting nutrition knowledge has been advocated by various studies conducted in India such as Gupta et al., Bandyopadhyay et al., Naghashpour et al., and Singh et al.[11,25,26,27]
In a study in South Italy, 37.5% answered correctly about a balanced diet.[9] A study from Bangladesh by Alam et al. reported that less than half of the adolescent girls correctly named high-protein foods which were lentils (21%), meat (32%), and fish (43%). Knowledge on vitamin- and mineral-rich foods was common; 75% mentioned vegetables and 51% mentioned fruits as vitamin- and mineral-rich foods.[10] The MARG (medical education for children/adolescents for Realistic prevention of obesity and diabetes and for healthy aging) school-based interventional study conducted in three cities of North India, namely New Delhi, Agra, and Jaipur showed a similar increase in the posttest scores.[13]
Health education plays a very important role in health systems. Health education as applied to health and disease issues is defined as “A process with intellectual, psychological, and social dimensions relating to activities which increase the abilities of people to make informed decisions affecting their personal, family, and community well-being. This process, based on scientific principles, facilitates learning and behavioral change in both health personnel and consumers, including children and youth,” (Joint Committee, 1973).[28] The findings of this study too corroborate that small informal sessions of education can play a role in improving knowledge of adolescent girls, which, in turn, will help health system to prevent nutrition-related deficiency and disorders. This study also gives hope that such sessions on a larger scale by involving multiple small groups can help to improve basic nutrition-related knowledge in large groups of adolescents. It may even be applied to adolescent boys and adults, but that is a matter for further research. Even if the people are poor, having correct knowledge will enable them to make good food choices and eat a balanced diet, which would lead to an improvement in the nutritional status of all members of the family.
A limitation of this study is that the waning effect of time on memory has not been analyzed. A retention posttest could have been administered. However, due to examination in school, the retention study could not be planned. Another limitation is that information provided during the session could not be exhaustive due to time constraints. However, the utmost attempt was made to cover the basic and most important topics pertaining to nutrition like balanced diet and anemia.
Conclusion
Nutrition knowledge was found poor among school-going adolescent girls which significantly improved after nutrition education sessions. The nutrition session conducted using the nutrition education material prepared by the community health department of a tertiary care hospital along with the demonstration session significantly improved nutrition knowledge of these students. Hence, introducing a nutrition-oriented session along with practical demonstration will go a long way. Furthermore, schools provide an easily accessible setting for interventions targeted at children and parents to promote a healthy lifestyle. Recently, our prime minister has announced his highly ambitious POSHAN ABHIYAN and National Poshan mission, and nutrition education is also a part of this program; our recommendation is to incorporate nutrition education using such creative methods for better understanding of adolescents.
Financial support and sponsorship
This intervention was supported financially by Humana People to People Foundation.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
We would like to acknowledge the support of Humana People to People Foundation who funded the project “A Model for development and health of vulnerable adolescents and their families,” under which this intervention was conducted in the school. We also want to gratefully acknowledge the guidance given by Dr. S.K. Kapoor, Prof. Emeritus, Community Health Department, St. Stephen's Hopsital during the preparation of the manuscript. We acknowledge the dedication and hard work of all staff members who worked tirelessly to make this event in the school a success.
References
- 1.UNICEF. The State of the World's Children 2011: Adolescence: An age of Opportunity. [Last accessed on 2018 Mar 23]. Available from: http://wwwuniceforg/sowc2011/pdfs/SOWC-2011-Main-Report_EN_02092011pdf .
- 2.Sivagurunathan C, Umadevi R, Rama R, Gopalakrishnan S. Adolescent health: Present status and its related programmes in India? Are we in the right direction. J Clin Diagn Res. 2015;9:LE01–6. doi: 10.7860/JCDR/2015/11199.5649. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.World Health Organization. Regional Office for South East Asia. Child and Adolescent Health and development: Adolescent Nutrition. [Last accessed on 2018 Mar 30]. Available from: http://www.searo.who.int/entity/child_adolescent/topics/adolescent_health/adolescent_nutrition/en/
- 4.World Health Organization. Health for the World's Adolescents a Second Chance in the Second Decade. 2014. [Last accessed on 2018 Feb 23]. Available from: http://wwwwhoint/adolescent/second-decade .
- 5.World Health Organization, Regional Office for South East Asia. Adolescent Nutrition: A Review of the Situation in Selected South-East Asian Countries. 2006. [Last accessed on 2018 Feb 23]. Available from: http://apps.searo.who.int/pds_docs/B0239.pdf .
- 6.National Family Health Survey (NFHS-4), 2015-16: India. International Institute of Population Science, Mumbai. 2017 [Google Scholar]
- 7.Toteja GS, Singh P, Dhillon BS, Saxena BN, Ahmed FU, Singh RP, et al. Prevalence of anemia among pregnant women and adolescent girls in 16 districts of India. Food Nutr Bull. 2006;27:311–5. doi: 10.1177/156482650602700405. [DOI] [PubMed] [Google Scholar]
- 8.Kotecha PV, Patel SV, Baxi RK, Mazumdar VS, Shobha M, Mehta KG, et al. Dietary pattern of schoolgoing adolescents in urban Baroda, India. J Health Popul Nutr. 2013;31:490–6. doi: 10.3329/jhpn.v31i4.20047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Grosso G, Mistretta A, Turconi G, Cena H, Roggi C, Galvano F. Nutrition knowledge and other determinants of food intake and lifestyle habits in children and young adolescents living in a rural area of Sicily, South Italy. Public Health Nutr. 2013;16:1827–36. doi: 10.1017/S1368980012003965. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Alam N, Roy SK, Ahmed T, Ahmed AM. Nutritional status, dietary intake, and relevant knowledge of adolescent girls in rural Bangladesh. J Health Popul Nutr. 2010;28:86–94. doi: 10.3329/jhpn.v28i1.4527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Singh A, Grover K, Sharma N. Effectiveness of nutrition intervention to overcome the problem of Anaemia. Food Sci Res J. 2014;5:184–9. [Google Scholar]
- 12.Neumark-Sztainer D, Story M, Falkner NH, Beuhring T, Resnick MD. Sociodemographic and personal characteristics of adolescents engaged in weight loss and weight/muscle gain behaviors: Who is doing what? Prev Med. 1999;28:40–50. doi: 10.1006/pmed.1998.0373. [DOI] [PubMed] [Google Scholar]
- 13.Shah P, Misra A, Gupta N, Hazra DK, Gupta R, Seth P, et al. Improvement in nutrition-related knowledge and behaviour of urban Asian Indian school children: Findings from the 'Medical education for children/Adolescents for Realistic prevention of obesity and diabetes and for healthy aGeing'(MARG) intervention study. Br J Nutrit. 2010;104:427–36. doi: 10.1017/S0007114510000681. [DOI] [PubMed] [Google Scholar]
- 14.Taneja G, Dixit S, Khatri A, Yesikar V, Raghunath D, Chourasiya S. A study to evaluate the effect of nutritional intervention measures on admitted children in selected nutrition rehabilitation centers of Indore and Ujjain divisions of the state of Madhya Pradesh (India) Indian J Community Med. 2012;37:107–15. doi: 10.4103/0970-0218.96096. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Meena JK, Verma A, Kumar R. Evaluation of Integrated Childhood Development Services (ICDS) program implementation in an urban slum of Delhi, India. Int J Res Med Sci. 2017;5:3443–7. [Google Scholar]
- 16.Wang D, Stewart D, Chang C, Shi Y. Effect of a school-based nutrition education program on adolescents’ nutrition-related knowledge, attitudes and behaviour in rural areas of China. Environ Health Prev Med. 2015;20:271–8. doi: 10.1007/s12199-015-0456-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Banerjee AV, Duflo E. The economic lives of the poor. Econ Perspect. 2007;21:141–67. doi: 10.1257/jep.21.1.141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Jaworska N, MacQueen G. Adolescence as a unique developmental period. J Psychiatry Neurosci. 2015;40:291–3. doi: 10.1503/jpn.150268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Casey BJ, Jones RM, Hare TA. The adolescent brain. Ann N Y Acad Sci. 2008;1124:111–26. doi: 10.1196/annals.1440.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Sawyer SM, Afifi RA, Bearinger LH, Blakemore SJ, Dick B, Ezeh AC, et al. Adolescence: A foundation for future health. Lancet. 2012;379:1630–40. doi: 10.1016/S0140-6736(12)60072-5. [DOI] [PubMed] [Google Scholar]
- 21.Omran AR, Al-Hafez G. Health Education for Adolescent Girls EMRO Nonserial Publication, WHO Regional Office for the Eastern Mediterranean. 2006 [Google Scholar]
- 22.Yadav S, Arokiasamy P. Understanding epidemiological transition in India. Glob Health Action. 2014;7:23248. doi: 10.3402/gha.v7.23248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Office of Registrar General and Census Commissioner, Government of India. Census of India. 2011. [Last accessed on 2018 Apr 23]. Available from: http://censusindia.gov.in/
- 24.Lua PL, Putri Elena WD. The impact of nutrition education interventions on the dietary habits of college students in developed nations: A brief review. Malays J Med Sci. 2012;19:4–14. [PMC free article] [PubMed] [Google Scholar]
- 25.Gupta N, Kochar G. Role of nutrition education in improving the nutritional awareness among adolescent girls. Int J Nutrit Wellness. 2008;7:1–4. [Google Scholar]
- 26.Bandyopadhyay L, Maiti M, Dasgupta A, Paul B. Intervention for improvement of knowledge on anemia prevention: A schoolbased study in a rural area of West Bengal. Int J Health Allied Sci. 2017;6:69–74. [Google Scholar]
- 27.Naghashpour M, Shakerinejad G, Lourizadeh MR, Hajinajaf S, Jarvandi F. Nutrition education based on health belief model improves dietary calcium intake among female students of junior high schools. J Health Popul Nutr. 2014;32:420–9. [PMC free article] [PubMed] [Google Scholar]
- 28.Joint Committee on Health Education Terminology. New definitions: Report of the 1972-1973. Hlth Educ Monogr. 1973;1:63–70. doi: 10.1111/j.1746-1561.1974.tb01909.x. [DOI] [PubMed] [Google Scholar]