

Abstract
Ergogenic supplements to improve athletic performance are commonly used among college athletes, but little is known about their association with eating disorder symptoms. The objective of this study was to examine associations between ergogenic supplement use and disordered eating attitudes and behaviors among university students, and to compare differences by sex. Undergraduate students from 10 top-ranked National College Athletics Association (NCAA) Division I colleges completed an online survey on supplement use, athletic activities, and eating attitudes and behaviors. Among 1633 university students, males (38.9%) reported higher rates of current supplement use than females (15.2%) (p < .001). In linear regression models adjusting for athletic status and body mass index, current supplement use was associated with higher Eating Disorders Examination-Questionnaire (EDE-Q) Global, Shape Concern, and Restraint scores in both males and females. Supplement use was associated with driven/compelled exercise (OR 2.00, 95% CI 1.33–2.99) in males and diuretic (OR 6.39, 95% CI 2.02–20.22) and diet pill use (OR 3.07, 95% CI 1.79–5.27) in females. Results suggest ergogenic supplement use is common in undergraduates and associated with disordered eating attitudes and behaviors. Clinicians should screen for disordered eating behaviors particularly in young adults who use ergogenic supplements.
Keywords: Ergogenic supplement use, anabolic androgenic steroid, eating behaviors, university, college, athletes
Introduction
Ergogenic supplements are dietary aids intended to improve athletic performance, with widespread use (88-99%) among college athletes (Burns, Schiller, Merrick, & Wolf, 2004; Froiland, Koszewski, Hingst, & Kopecky, 2004; Kristiansen, Levy-Milne, Barr, & Flint, 2005). Ergogenic supplements include, but are not limited to, anabolic androgenic steroids (AAS), creatine, amino acids, nitric oxide, and protein supplements. Ergogenic supplements are not regulated by the Food and Drug Administration (FDA) and thus, there is limited data on true athletic performance benefits as well as potential detrimental health consequences of supplements (Cohen, 2014; Pope et al., 2014). Given the lack of FDA regulation, supplements may be contaminated with dangerous, unlisted ingredients, or have different dosages of ingredients than stated on the label (Cohen, 2014; Cohen, Maller, DeSouza, & Neal-Kababick, 2014). Therefore, use of these supplements may have unintended health consequences (Frati, Busardo, Cipolloni, Dominicis, & Fineschi, 2015; Pope et al., 2014; Smith, Agharkar, & Gonzales, 2014; Thiblin et al., 2015).
Ergogenic supplement use has been associated with other high risk behaviors, such as heavy alcohol use, illicit drug use, and increased sexual activity (Bahrke & Yesalis, 2004; Bailey, Gahche, Miller, Thomas, & Dwyer, 2013; Buckman, Farris, & Yusko, 2013), as well as low self-esteem and self-perceived low academic achievement (Kindlundh, Hagekull, Isacson, & Nyberg, 2001). Little is known, however, about associations between supplement use and disordered eating behaviors, such as binge eating, vomiting, and laxative or diuretic use for weight loss. Disordered eating behaviors are associated with increased risk for depression (Neumark-Sztainer, Wall, Larson, Eisenberg, & Loth, 2011), alcohol and tobacco use (Piran & Robinson, 2006), and poor nutritional intake and quality (Neumark-Sztainer et al., 2011), and constitute some of the core criteria for a Diagnostic and Statistical Manual, 5th Edition (DSM-5) eating disorder diagnosis (American Psychiatric Association, 2013). Athletes may be at increased risk of disordered eating behaviors (Darcy, Hardy, Lock, Hill, & Peebles, 2013), given the emphasis on leanness and/or muscularity in certain sports, and these behaviors may differ by sex (Galli, Petrie, Reel, Chatterton, & Baghurst, 2014). However, less is known about the relationship between disordered eating and ergogenic supplement use, and any associated sex differences.
The few studies to examine the relationship between disordered eating and ergogenic supplement use have mostly focused on men and AAS use. AAS use for appearance purposes has been shown to be associated with eating disorder pathology among men (Murray, Griffiths, Mond, Kean, & Blashill, 2016) and AAS use was associated with greater eating disorder symptoms among gay and bisexual men in Australia and New Zealand (Griffiths, Murray, Dunn, & Blashill, 2017). However, these studies did not include women or other ergogenic supplements. While some other studies have examined broader appearance and performance enhancing drugs beyond AAS and their associations with eating disorders, these studies were in men (Hildebrandt, Alfano, & Langenbucher, 2010) and an Italian sample (Piacentino et al., 2017), and did not use the Eating Disorders Examination-Questionnaire, a widely used measure of eating disorder symptoms. Thus, understanding of gender differences in the association between ergogenic supplement use and eating disorders remains limited, particularly in the USA and among university students.
Understanding the association between ergogenic supplement use and disordered eating behaviors is important to inform 1) screening and prevention programs for disordered eating behaviors and eating disorders, 2) screening and prevention programs for AAS use and potentially harmful ergogenic supplement use; and 3) public policies regarding the regulation of ergogenic supplement use. The objective of the current study was to examine associations between supplement use and disordered eating attitudes and behaviors in a college population. We hypothesized that ergogenic supplement users would be more likely to engage in disordered eating behaviors than nonusers. We also examined these associations according to sex; given the nascent evidence to date on potential sex differences, secondary hypotheses remained exploratory.
Methods
Participants and Procedure
This cross-sectional study recruited university students, ages 18–26, from the top 10 National College Athletics Association (NCAA) Division I universities based on women’s swimming in the United States in the prior year, which represented geographically diverse regions. Participants were recruited through a social media site to complete an anonymous online survey examining athletics and health. Athletes of all offered sports were oversampled through direct messages on their social media account based upon their sport team’s public online roster. Both athletes and non-athletes were recruited through online advertisements targeted at the age group and universities desired. To encourage participation, participants who completed the survey were eligible to enter a raffle that distributed two iPhones. A true response rate cannot be reliably determined from the online advertising. However, data indicate that the survey website’s online consent form was viewed 3,339 times and 1,688 participants completed the survey. Thus, a proxy response rate is estimated at 50.6%. Participants were excluded for failure to meet inclusion criteria (n = 21), nonexistent or very incomplete responses (n = 18); duplicate entries (n = 5); or disclosure of untruthful responses (n = 8). We further excluded 44 male (7.1%) and 73 female (7.5%) participants with missing data for the primary variables of interest for the analysis. There were no significant differences in demographic or BMI characteristics of participants who were included versus excluded and patterns of missing data were consistent with missing at random. This study was conducted in compliance with the Stanford University Panel on Medical Research in Human Subjects and the NCAA. Informed consent was obtained online prior to completion of the survey, which took approximately 30 minutes to complete.
Undergraduate students (N = 1516) completed the questionnaire (59.4% female, n = 900) with a mean age of 20.9±1.7 SD (range 18–27). Participants self-reported race/ethnicity: Caucasian (74.4%), Asian (9.8%), Hispanic (5.7%), African-American (4.9%), Native Hawaiian/Pacific Islander (0.3%), and Other (4.9%).
Measures
The online survey asked multiple questions about eating behaviors and activity, utilizing standardized and published measures whenever possible. The online survey was clearly separated by measure.
Eating Disorder Examination Questionnaire (EDE-Q).
The EDE-Q is a self-report questionnaire that assesses disordered eating attitudes and behaviors over the previous 28 days (Fairburn & Beglin, 2008). Responses on 28 items are on a 7- point scale, anchored by 0 (no days) and 6 (every day), and higher scores reflect greater eating-related pathology. The measure provides a Global score and four subscale scores: Restraint, Eating Concern, Shape Concern, and Weight Concern. In clinical and non-clinical ED samples, the EDE-Q has demonstrated high internal consistency, test-retest reliability, and correlations with other measures of ED pathology (Berg, Peterson, Frazier, & Crow, 2012). Cronbach’s alpha for males and females, respectively, was .93 and .95 for the Global score, .74 and .81 for the Restraint subscale, .78 and .86 for the Eating Concern subscale, .81 and .85 for the Weight Concern subscale, and .88 and .91 for the Shape Concern subscale.
Individual behaviors analyzed from the EDE-Q included binge eating, vomiting, laxative use, and compulsive exercise in the past 28 days. Driven or compulsive exercise was based upon EDE-Q item 18 (“Over the past 28 days, how many times have you exercised in a “driven” or “compulsive” way as a means of controlling your weight, shape or amount of fat or to burn off calories?”), which has been shown to have concordance with compulsive exercise as measured by the Compulsive Exercise Test (Young et al., 2017). “Any” behavior was defined as reporting ≥ 1 episode of each of the respective behaviors in the past 28 days as has been defined in prior EDE-Q norms publications (Lavender, De Young, & Anderson, 2010; Nagata, Capriotti et al., 2019).
Project Eating Among Teens (EAT).
Participants were also asked if they had used diuretics or diet pills to lose weight in the past month, which are common weight control behaviors used by adolescents and young adults that are not asked in the EDE-Q (Neumark-Sztainer et al., 2011). These questions were based on “extreme unhealthy weight control behavior” questions (96% agreement ≥1 behavior, r = .66) from Project EAT a population-based study of eating patterns and weight concerns among adolescents (Neumark-Sztainer, 2010).
Ergogenic Supplement Use.
The online survey included questions on current (use in past 30 days) and ever-use of 10 specific types of ergogenic supplements. Participants were asked, “Are you CURRENTLY taking any of the following supplements to gain muscle or lose fat?” and “Have you EVER used any of the following supplements to gain muscle or lose fat?” Participants were asked to mark all that apply among: anti-estrogens; human growth hormone; nitric oxide; amino acids and branched chain amino acids; protein powders, bars, and drinks; fat-burner supplements; Dehydroepiandrosterone (DHEA); creatine; androstenedione; and anabolic androgenic steroids. For each supplement, participants were categorized into current supplement user (past 30 days), ever supplement user, or nonuser.
Sports Participation and Exercise.
Participants self-identified athletic status and participation in specific sports. Participants were categorized into three groups based upon their activity level using categories that have been previously reported (Darcy et al., 2013): Low Activity (LA; participants not engaged in regular activity or sport), Recreational athlete (REC; those engaging in regular recreational sport or exercise without competition in the past year), and Competitive Athlete (CA; athletes who participated in at least one competitive sport in the past 12 months with or without addition of regular recreational exercise). Though a focus of the study was on athletes, it was important to include participants with differing levels of activity, including low activity, for comparison purposes.
Demographics.
Participants self-reported demographic information including age, sex, and race/ethnicity.
Data Analysis
Statistical analyses were performed using STATA 15.0 software, with statistical significance set at p < .05. Current and ever supplement use was compared between sexes (chi-squared or Fisher’s exact test). Current supplement users versus non-current users were compared in terms of weight control practices (chi-squared test) and EDE-Q Global and subscale scores (independent samples t-test). Linear regression models were used to analyze associations between current supplement use and EDE-Q scores and behaviors, adjusting for activity level and body mass index. Activity level was categorized into Low Activity, Recreational Athlete, and Competitive Athlete, with Low Activity as the reference group. The residuals of the regression models approximated a normal distribution. In sensitivity analyses, we used linear regression to analyze associations between 1) protein supplement use and 2) non-protein supplement use and EDE-Q scores and behaviors, adjusting for activity level and body mass index. The data that support the findings of this study are available from the corresponding author upon reasonable request.
Results
The prevalence of supplement use by sex is presented in Table 1. Overall, males reported higher current (36.7% vs 13.2%, p < .001) and ever (55.8% vs 22.4%, p < .001) supplement use as compared with females.
Table 1.
Current and ever use of ergogenic supplements among male (N=616) and female (N=900) university students
| Ergogenic supplement use | Current use | Ever use | ||||
|---|---|---|---|---|---|---|
|
|
|
|||||
| Male | Female | p a | Male | Female | p a | |
|
|
|
|||||
| % (n) | % (n) | % (n) | % (n) | |||
| Anti-estrogens | 0.2 (1) | 0 (0) | .227 | 0.7 (4) | 0 (0) | .015 |
| Human growth hormone | 0 (0) | 0 (0) | NA | 0.3 (2) | 0 (0) | .087 |
| Nitric oxide | 3.4 (21) | 0.1 (1) | <.001 | 8.1 (50) | 0.2 (2) | <.001 |
| Amino acids, Branched-chain amino acids | 3.7 (23) | 0.7 (6) | <.001 | 7.6 (47) | 1.1 (10) | <.001 |
| Protein powders, bars, drinks | 25.5 (157) | 6.0 (54) | <.001 | 46.3(285) | 14.4 (130) | <.001 |
| Fat-burner supplement | 0.7 (4) | 1 (9) | .467 | 4.6 (28) | 4.4 (40) | .926 |
| Dehydroepiandrosterone (DHEA) | 0 (0) | 0.1 (1) | .408 | 0.2 (1) | 0.1 (1) | .787 |
| Creatine | 6.2 (38) | 0.4 (4) | <.001 | 21.8 (134) | 1.6 (14) | <.001 |
| Androstenedione | 0.2 (1) | 0 (0) | .227 | 0.3 (2) | 0 (0) | .087 |
| Anabolic androgenic steroids | 0.3 (2) | 0 (0) | .087 | 1.0 (6) | 0.1 (1) | .015 |
| Any Supplement | 36.7 (226) | 13.2 (119) | <.001 | 55.8 (344) | 22.4 (202) | <.001 |
Note:
Comparisons of specific supplement use by sex, chi-square or Fisher’s exact tests. Bold items indicate minimum significance of p < .05.
Male university students reported higher current use of nitric oxide, amino acids, protein powders, bars and drinks, and Creatine than female students (Table 1; all ps < .001). Male university students also reported higher ever use of anti-estrogens, nitric oxide, amino acids, protein supplements, Creatine, androstenedione, and androgenic anabolic steroids than female students (all ps < .05). Among males but not females, there were significant differences in current (p < .001) and ever (p < .001) use of any supplement within activity level groups.
Among males, 6.7% (n = 41) had low activity, 26.8% (n = 165) were recreational athletes, and 66.6% (n = 410) were competitive athletes. Among females, 7.7% (n = 69) had low activity, 36.6% (n = 329) were recreational athletes, and 55.8% (n = 502) were competitive athletes. Male competitive athletes had the highest rates of current supplement use, followed by recreational athletes, and those with low activity (Figure 1). Similar trends were noted in females, though current supplement use was lower.
Figure 1.
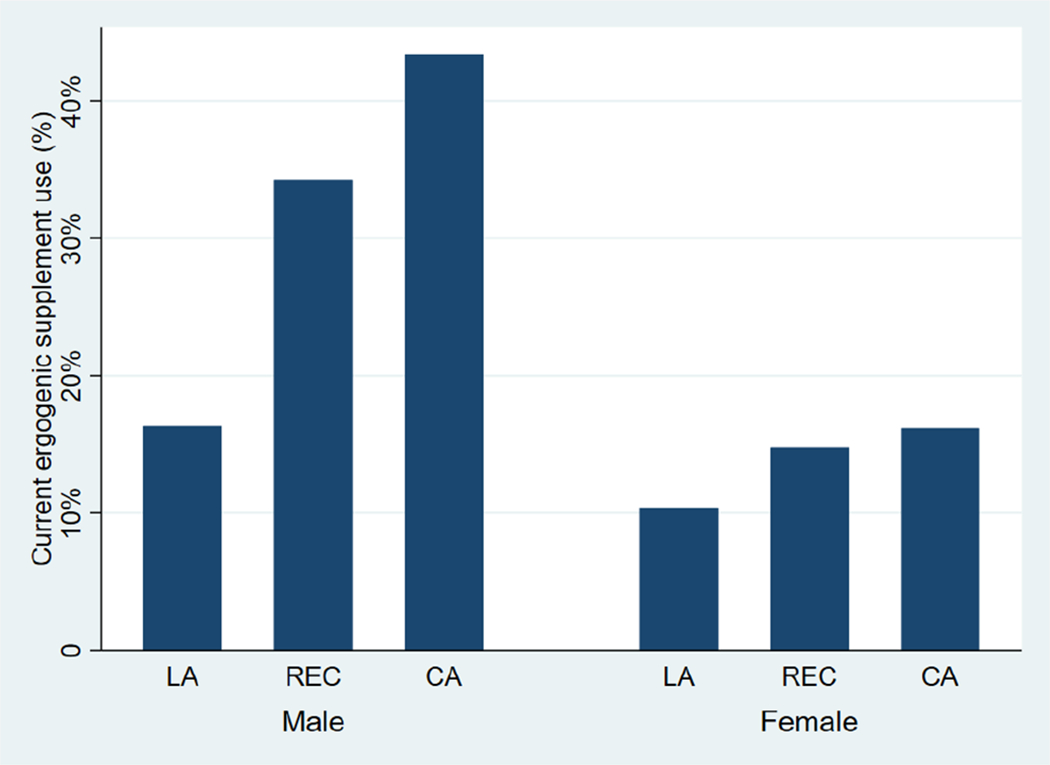
Ergogenic supplement use and level of activity, by sex
LA=Low Activity, REC=Recreational athlete, CA=Competitive Athlete
In unadjusted comparisons, female supplement users had higher EDE-Q Global (2.0 vs 1.7, p = .02), Shape Concern (2.8 vs 2.3, p = .003), and Restraint (1.9 vs 1.6, p = .02) scores than nonusers (Table 2). Male supplement users had higher EDE-Q Global (1.0 vs .7, p < .001), Shape Concern (1.4 vs 1.1, p = .007), and Restraint (1.3 vs 0.8; p < .001) scores than nonusers. When comparing disordered eating behavior in current supplement users with nonusers, female users were more likely to have reported diuretic (3.4% vs 0.5%, p = .002) or diet pill use (9.2% vs 1.7%, p < .001) for the purposes of weight loss in the past month. Male users were more likely to report any compulsive exercise (28.1% vs 15.5%, p < .001) than nonusers in the past month.
Table 2.
Eating Disorders Examination Questionnaire (EDE-Q) Scores and eating behaviors, by current supplement use
| Males | Females | |||||
|---|---|---|---|---|---|---|
|
|
||||||
| Ergogenic supplement use | Current user | Non-user | p-value | Current user | Non-user | p-value |
|
|
||||||
| N | 226 | 390 | 119 | 781 | ||
|
|
||||||
| EDE-Q Scale | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | ||
|
|
|
|||||
| Global | 1.0 (0.9) | 0.7 (0.9) | < .001 | 2.0 (1.3) | 1.7 (1.3) | .02 |
| Eating Concern | 0.3 (0.6) | 0.2 (0.6) | .22 | 1.0 (1.2) | 0.9 (1.2) | .24 |
| Shape Concern | 1.3 (1.2) | 1.1 (1.2) | .007 | 2.8 (1.6) | 2.3 (1.6) | .003 |
| Weight Concern | 0.9 (1.1) | 0.7 (1.0) | .05 | 2.2 (1.6) | 2.0 (1.5) | .07 |
| Restraint | 1.3 (1.3) | 0.8 (1.1) | <. 001 | 1.9 (1.5) | 1.6 (1.5) | .02 |
|
|
|
|||||
| Behaviors, any (≥1 in past 28 days) | % (n) | % (n) | % (n) | % (n) | ||
|
|
|
|||||
| Binge eating | 18.6% (42) | 16.2% (63) | .44 | 34.5% (41) | 34.6% (270) | .98 |
| Vomiting | 2.7% (6) | 1.8% (7) | .47 | 15.1% (18) | 11.7% (91) | .23 |
| Laxative use | 0.5% (1) | 0.5% (2) | .92 | 4.2% (5) | 1.7% (13) | .07 |
| Diuretic use | 0% (0) | 0.0% (0) | NA | 3.4% (4) | 0.5% (4) | .002 |
| Diet Pill | 2.7% (6) | 1.3% (5) | .22 | 9.2% (11) | 1.7% (13) | < .001 |
| Driven/compulsive exercise | 28.1% (62) | 15.5% (60) | < .001 | 31.4% (37) | 30.4% (236) | .83 |
In linear regression models adjusting for athletic status and body mass index, current supplement use was associated with higher EDE-Q Global, Shape Concern, and Restraint scores in both males (Table 3) and females (Table 4). Among females but not males, recreational athletes had higher EDE-Q scores in all domains compared to non-athletes. In terms of behaviors, supplement use was associated with past month compulsive exercise (OR 1.97, 95% CI 1.30, 2.99; p = .001) in males; for females, supplement use was associated with diuretic (OR 6.57, 95% CI 1.61, 26.73; p = .009) and diet pill use (OR 6.55, 95% CI 2.78, 15.39; p < .001) in logistic regression models.
Table 3.
Associations between ergogenic supplement use and Eating Disorders Examination Questionnaire (EDE-Q) Scores and eating behaviors in males (n=616)
| Supplement Use | Recreational Athlete | Competitive Athlete | ||||
|---|---|---|---|---|---|---|
|
|
||||||
| B (95% CI) | p-value | B (95% CI) | p-value | B (95% CI) | p-value | |
|
|
||||||
| EDE-Q Scale | ||||||
| Global | 0.23 (0.091, 0.38) | .001 | 0.07 (−0.22, 0.36) | .64 | −0.17 (−0.45, 0.10) | .22 |
| Eating Concern | 0.06 (−0.05, 0.16) | .30 | 0.02 (−0.20, 0.23) | .89 | −0.08 (−0.29, 0.12) | .43 |
| Shape Concern | 0.27 (0.10–0.47) | .006 | −0.12 (−0.52, 0.28) | .56 | −0.53 (−0.91, −0.15) | .006 |
| Weight Concern | 0.15 (−0.02, 0.32) | .09 | 0.02 (−0.33, 0.37) | .91 | −0.26 (−0.60, 0.07) | .12 |
| Restraint | 0.45 (0.26, 0.64) | <.001 | 0.36 (−0.03, 0.76) | .07 | 0.19 (−0.18, 0.56) | .31 |
|
|
||||||
| Behaviors, any (≥1 in past 28 days) | OR (95% CI) | p-value | OR (95% CI) | p-value | OR (95% CI) | p-value |
|
|
||||||
| Binge eating | 1.21 (0.77, 1.88) | .41 | 0.57 (0.25, 1.31) | .19 | 0.57 (0.26, 1.23) | .15 |
| Vomiting | 1.29 (0.42, 3.95) | .66 | 0.76 (0.21, 2.82) | .68 | -- | -- |
| Laxative use | 1.18 (0.09, 15.24) | .90 | -- | -- | 0.20 (0.02, 2.60) | 0.22 |
| Diuretic use | -- | -- | -- | -- | -- | -- |
| Diet Pill | 1.71 (0.50, 6.01) | .40 | 3.06 (0.89, 10.50) | .08 | -- | -- |
| Driven/compulsive exercise | 1.97 (1.30, 2.99) | .001 | 3.82 (1.10, 13.17) | .03 | 2.20 (0.65, 7.44) | .20 |
Note: B = beta coefficient from linear regression; OR = odds ratio from logistic regression; All models include supplement use, athletic status, and body mass index. B for Recreational Athlete and Competitive Athlete categories are in comparison to Low Activity (reference group). Bold items indicate minimum significance of p <.05.
Table 4.
Associations between ergogenic supplement use and Eating Disorders Examination Questionnaire (EDE-Q) Scores and eating behaviors in females (n=900)
| Supplement Use | Recreational Athlete | Competitive Athlete | ||||
|---|---|---|---|---|---|---|
|
|
||||||
| B (95% CI) | p-value | B (95% CI) | p-value | B (95% CI) | p-value | |
|
|
||||||
| EDE-Q Scale | ||||||
| Global | 0.26 (0.01, 0.50) | .04 | 0.52 (0.19, 0.84) | .002 | 0.27 (−0.04, 0.59) | .09 |
| Eating Concern | 0.11 (−0.11, 0.34) | .33 | 0.39 (0.09, 0.70) | .01 | 0.20 (−0.10, 0.49) | .19 |
| Shape Concern | 0.40 (0.11, 0.69) | .006 | 0.48 (0.09, 0.86) | .02 | 0.12 (−0.25, 0.50) | .52 |
| Weight Concern | 0.22 (−0.06, 0.49) | .13 | 0.53 (0.16, 0.91) | .005 | 0.19 (−0.17, 0.55) | .31 |
| Restraint | 0.29 (0.01, 0.57) | .04 | 0.67 (0.29, 1.05) | .001 | 0.59 (0.22, 0.96) | .002 |
|
|
||||||
| Behaviors, any (≥1 in past 28 days) | OR (95% CI) | p-value | OR (95% CI) | p-value | OR (95% CI) | p-value |
|
|
||||||
| Binge eating | 0.96 (0.64, 1.44) | .84 | 2.02 (1.09, 3.75) | .03 | 1.94 (1.06, 3.54) | .03 |
| Vomiting | 1.32 (0.76, 2.28) | .33 | 2.51 (0.87, 7.24) | .088 | 2.13 (0.75, 6.07) | .16 |
| Laxative use | 2.63 (0.91, 7.59) | .07 | 1.93 (0.75, 4.98) | .17 | -- | -- |
| Diuretic use | 6.57 (1.61, 26.73) | .009 | 1.67 (0.41, 6.82) | .47 | -- | -- |
| Diet Pill | 6.55 (2.78, 15.39) | <.001 | 3.03 (1.28, 7.18) | .01 | -- | -- |
| Driven/compulsive exercise | 1.00 (0.65, 1.52) | .99 | 7.21 (2.82, 18.44) | <.001 | 5.43 (2.14, 13.78) | <.001 |
Note: B = beta coefficient from linear regression; OR = odds ratio from logistic regression; All models include supplement use, athletic status, and body mass index. B for Recreational Athlete and Competitive Athlete categories are in comparison to Low Activity (reference group). Bold items indicate minimum significance of p <.05.
In sensitivity analyses using linear regression models, protein supplement use was associated with EDE-Q Restraint Subscale scores only, whereas non-protein supplement use was associated with EDE-Q Global and Restraint Subscale scores in males, adjusting for athletic status and BMI (Appendix A). Among females, non-protein supplement use was associated with EDE-Q Global and all subscale scores in linear regression models adjusting for athletic status and BMI (Appendix B).
Discussion
Results of the current study indicate that ergogenic supplement use is common among university students of all activity levels, even among those reporting low activity. In general, a step-wise increase was observed in rates of current ergogenic supplement use with increasing levels of physical activity, particularly in males. For instance, males who participate in competitive sports reported the highest rates of current supplement use. The prevalence of ergogenic supplement use in the subsample of college athletes (competitive athletes) is lower than rates reported previously among college athletes (Burns et al., 2004; Froiland et al., 2004; Kristiansen et al., 2005). However, the prevalence of ergogenic supplement use in the overall sample was comparable to rates previously reported in college students (Lieberman et al., 2015). Both male and female supplement users reported higher EDE-Q Global Scores, Shape Concerns, and Restraint than non-supplement users.
In this dataset, several sex differences were noted. Males (37%) were significantly more likely to report current ergogenic supplement use than females (13%); prior studies have reported higher rates of supplement use in females compared to males, but some of these studies included vitamin and mineral or nutritional supplements not necessarily used for athletic performance enhancement (Froiland et al., 2004; McDowall, 2007). Females who were currently using supplements were more likely to report diuretic and diet pill use for weight control, whereas male current supplement users were more likely to report driven/compulsive exercise than nonusers. This suggests that males and females may opt to use supplements to achieve different goals. Specifically, supplement use among males was not significantly associated with any binge eating, vomiting, laxative use, or diet pill use. Supplement use among females was not significantly associated with any binge eating, vomiting, laxative use, or driven/compulsive exercise. Together, these findings suggest that differences exist specific to diet pill use versus driven/compulsive exercise such that the perceived function of each of these compensatory behaviors may impact behavior, and differ by sex. For example, diet pill use may be more related to a desire for weight loss (endorsed by females) whereas driven/compulsive exercise (endorsed by males) may be more related to a desire for increased muscularity.
Similar to rates previously reported (Burns et al., 2004), 44% of males in this sample had used protein powders in the past, with 21% having used Creatine. Both of these supplements are intended to boost muscle mass; therefore, males may be more likely to use supplements for muscle building and for exercise performance enhancement (Calzo, Corliss, Blood, Field, & Austin, 2013; Nagata, Murray et al., 2019). Ergogenic supplement use was associated with higher odds of any compulsive exercise in the past month in males but not in females, underscoring the possibility that the intersection of supplement use and maladaptive exercise among males may derive from efforts to increase muscularity (Nagata et al., 2019).
Female users, on the other hand, with higher rates of disordered weight control practices and higher EDE-Q scores than nonusers, may be more likely to take supplements for the purposes of weight control or weight loss (Chernyak & Lowe, 2010). Ergogenic supplement use was associated with higher odds of any diuretic and diet pill use in females but not males. Prior studies in college athletes have reported that 11% of female rowers and 3% of female runners have used diuretics (Karlson, Becker, & Merkur, 2001), similar to the rates in our sample.
EDE-Q Global scores were higher in both male and female supplement users than among non-supplement users. Supplement users also had significantly higher Shape Concern and Restraint (but not Eating Concern and Weight Concern) subscales than nonusers in both males and females. Female non-supplement users in the current study had EDE-Q Global and subscale scores comparable to published norms, suggesting that these participants were representative of the “typical” college female (Luce, Crowther, & Pole, 2008). In contrast, female supplement users reported EDE-Q scores that were significantly higher than these norms in the Global Score, the Shape Concern subscale, and the Restraint subscale. Although statistical differences were noted, the magnitude of differences were small, and interpretations regarding supplement use and risk for disordered eating should be made with caution. It is possible that the association between ergogenic supplement use and eating disorder symptoms may differ by supplement type. In females, non-protein supplements were associated with EDE-Q Global and all subscale scores, and seemed to be driving the associations found between ergogenic supplements and eating disorder symptoms. Although protein supplements were the most commonly reported supplement in both males and females, these products did not seem to influence the association between ergogenic supplements and EDE-Q. Among males, protein supplement use was only associated with the EDE-Q Restraint subscale, but not any of the other subscales or Global score. Among females, protein supplement use was only associated between Shape Concern and Restraint subscales, but not Eating Concern, Weight Concern, or Global score. It is possible that these lower scores on measures of eating pathology among males may reflect the influence of sporting category. For example, prior work has indicated lower scores on attitudinal eating pathology among male athletes in leanness-oriented sports; in contrast, these male athletes in were more likely to report greater use of disordered-eating behavior as compared with non-leanness sport counterparts (McDonald, Pritchard, & McGuire, 2019). Future work might stratify the lines of inquiry included in the current study by sport category. Protein supplements such as protein powders, bars, and drinks, may be more mainstream and used as a snack or meal replacement and be ingested for different reasons than amino acids, creatine, and human growth hormone. Future research could examine which individual ergogenic supplements are associated with the highest eating disorder symptom risk, both across gender and activity level.
Female recreational athletes had significantly higher EDE-Q Global and subscale scores compared to non-athletes in regression models. Competitive athletes had significantly higher EDE-Q Restraint subscale scores than non-athletes, but not for Global or other subscale scores. The reason for higher EDE-Q scores among female recreational athletes is not entirely clear, but may be related to the relatively similar rates of ergogenic supplement use among recreational and competitive female athletes and higher EDE-Q scores among females. Female recreational athletes had higher odds of any vomiting or driven/compulsive exercise, but not binge eating, laxative use, diuretic use, or diet pill use.
This study has several limitations. Participants who were more interested in exercise and eating behaviors may have demonstrated selection bias, and have been more likely to complete the survey. The current study data cannot comment on frequency of supplement use as this was not assessed. Although our ergogenic supplement questions had adequate face validity and had been piloted, these questions were not fully validated and we are not aware of fully validated questionnaires on ergogenic supplement use. In addition, current users were defined as those who had used the supplement in the past thirty days, while there may be a subset of participants with considerably more frequent use, which should be examined in future work. Despite these limitations, strengths of the study included a large collegiate sample with a range of activity levels.
Ergogenic supplement use is common in a college population and is associated with disordered eating behaviors. Ergogenic supplement use was higher in males than females, which may reflect muscularity-oriented goals. Given current study findings, clinicians should consider screening for ergogenic supplement use in university students, particularly males with higher levels of sports participation (i.e., both competitive and recreational engagement). Further, among those who report ergogenic supplement use, providers may also consider screening for and counseling about disordered eating behaviors, including questions that can specify motivation for supplement use (e.g., for weight loss). Future research should evaluate the efficacy of specific ergogenic supplements in achieving athletic or appearance-enhancement as well as potential adverse health consequences. This would allow for clearer health recommendations in the use of specific ergogenic supplements, particularly in populations including collegiate athletes where usage may be elevated.
Clinical Implications.
Ergogenic supplement use to enhance athletic performance is more common in male (39%) compared to female (15%) university students.
University students who use ergogenic supplements may be at higher risk for disordered eating attitudes and behaviors than those who do not use ergogenic supplements.
Ergogenic supplement use compared to non-use is associated with higher Eating Disorders Examination-Questionnaire (EDE-Q) Global, Shape Concern, and Restraint scores in both males and females.
Ergogenic supplement use compared to non-use is associated with driven/compelled exercise in males and diuretic and diet pill use in females in linear regression models.
Clinicians should consider screening for disordered eating behaviors particularly in young adults who use ergogenic supplements.
Acknowledgments:
The authors would like to acknowledge the ATHLETICS consortium, research assistants at the Stanford WEIGHT Lab, and all participants.
Funding: Dr. Nagata is a participant in the Pediatric Scientist Development Program (K12HD00085033), funded by the American Academy of Pediatrics and the American Pediatric Society; Dr. Peebles is supported by the National Institute of Diabetes and Digestive and Kidney Diseases [K23DK100558]; Dr. Gorrell is supported by the National Institutes of Health [T32MH018261–33]. Original study design and data collection supported by the Stanford Undergraduate Research Program.
Appendix A.
Associations between protein and non-protein supplement use and Eating Disorders Examination Questionnaire (EDE-Q) Scores and eating behaviors in males (n=616)
| Protein Supplement Use | Non-protein supplement use | |||
|---|---|---|---|---|
|
|
||||
| B (95% CI) | p-value | B (95% CI) | p-value | |
| EDE-Q Scale | ||||
| Global | 0.07 (−0.09, 0.23) | .385 | 0.34 (0.11, 0.56) | .003 |
| Eating Concern | −0.05 (−0.17, 0.06) | .366 | 0.11 (−0.05, 0.28) | .184 |
| Shape Concern | 0.06 −(0.15, 0.28) | .568 | 0.30 (−0.01, 0.60) | .057 |
| Weight Concern | −0.08 (−0.27, 0.11) | .381 | 0.24 (−0.03, 0.51) | .085 |
| Restraint | 0.35 (0.14, 0.57) | .001 | 0.70 (0.40, 1.00) | <0.001 |
|
|
||||
| Behaviors, any (≥1 in past 28 days) | OR (95% CI) | p-value | OR (95% CI) | p-value |
|
|
||||
| Binge eating | 0.86 (0.52, 1.43) | .560 | 0.67 (0.31, 1.47) | .321 |
| Vomiting | 0.46 (0.10, 2.10) | .315 | 3.56 (1.05, 12.02) | .041 |
| Laxative use | -- | -- | -- | -- |
| Diuretic use | -- | -- | -- | -- |
| Diet Pill | 3.25 (0.94, 11.30) | 0.06 | 5.67 (1.53–21.00) | .009 |
| Driven/compulsive exercise | 1.68 (1.08, 2.62) | .02 | 2.28 (1.28–4.07) | .005 |
Note: B = beta coefficient from linear regression; OR = odds ratio from logistic regression; All models include supplement use, athletic status, and body mass index. Bold items indicate minimum significance of p < .05.
Appendix B.
Associations between protein and non-protein supplement use and Eating Disorders Examination Questionnaire (EDE-Q) Scores and eating behaviors in females (n=900)
| Protein Supplement Use | Non-protein supplement use | |||
|---|---|---|---|---|
|
|
||||
| B (95% CI) | p-value | B (95% CI) | p-value | |
| EDE-Q Scale | ||||
| Global | 0.32 (−0.02, 0.67) | .067 | 0.97 (0.39, 1.54) | .001 |
| Eating Concern | 0.05 (−0.27, 0.38) | .741 | 0.74 (0.19, 1.28) | .009 |
| Shape Concern | 0.47 (0.05, 0.88) | .028 | 1.05 (0.36, 1.75) | .003 |
| Weight Concern | 0.22 (−0.18, 0.62) | .281 | 0.96 (0.29, 1.63) | .005 |
| Restraint | 0.55 (0.15, 0.95) | .008 | 1.12 (0.44, 1.79) | .001 |
|
|
||||
| Behaviors, any (≥1 in past 28 days) | OR (95% CI) | p-value | OR (95% CI) | p-value |
|
|
||||
| Binge eating | 0.52 (0.28, 0.99) | .047 | 1.16 (0.45, 3.04) | .757 |
| Vomiting | 1.48 (0.70, 3.15) | .303 | 2.82 (0.98, 8.09) | .055 |
| Laxative use | 1.00 (0.13, 7.82) | .996 | 7.06 (1.45, 34.48) | .016 |
| Diuretic use | 5.77 (1.09, 30.47) | .039 | 17.77 (3.30, 95.78) | .001 |
| Diet Pill | 4.06 (1.28, 12.89) | .017 | 26.76 (8.57, 83.57) | <.001 |
| Driven/compulsive exercise | 1.13 (0.62, 2.04) | .689 | 2.27 (0.88, 5.87) | .091 |
Note: B = beta coefficient from linear regression; OR = odds ratio from logistic regression; All models include supplement use, athletic status, and body mass index. Bold items indicate minimum significance of p < .05.
Footnotes
Conflict of Interest: On behalf of all authors, the corresponding author states that there is not conflict of interest.
References
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th Ed. ed.). Arlington, VA: American Psychiatric Publishing. [Google Scholar]
- Bahrke MS, & Yesalis CE (2004). Abuse of anabolic androgenic steroids and related substances in sport and exercise. Current Opinion in Pharmacology, 4(6), 614–620. doi: 10.1016/j.coph.2004.05.006 [DOI] [PubMed] [Google Scholar]
- Bailey RL, Gahche JJ, Miller PE, Thomas PR, & Dwyer JT (2013). Why US adults use dietary supplements. JAMA Internal Medicine, 173(5), 355–361. doi: 10.1001/jamainternmed.2013.2299 [DOI] [PubMed] [Google Scholar]
- Berg KC, Peterson CB, Frazier P, & Crow SJ (2012). Psychometric evaluation of the eating disorder examination and eating disorder examination-questionnaire: A systematic review of the literature. The International Journal of Eating Disorders, 45(3), 428–438. doi: 10.1002/eat.20931 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buckman JF, Farris SG, & Yusko DA (2013). A national study of substance use behaviors among NCAA male athletes who use banned performance enhancing substances. Drug and Alcohol Dependence, 131(1–2), 50–55. doi: 10.1016/j.drugalcdep.2013.04.023 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burns RD, Schiller MR, Merrick MA, & Wolf KN (2004). Intercollegiate student athlete use of nutritional supplements and the role of athletic trainers and dietitians in nutrition counseling. Journal of the American Dietetic Association, 104(2), 246–249. doi: 10.1016/j.jada.2003.11.013 [DOI] [PubMed] [Google Scholar]
- Calzo JP, Corliss HL, Blood EA, Field AE, & Austin SB (2013). Development of muscularity and weight concerns in heterosexual and sexual minority males. Health Psychology : Official Journal of the Division of Health Psychology, American Psychological Association, 32(1), 42–51. doi: 10.1037/a0028964 [doi] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chernyak Y, & Lowe MR (2010). Motivations for dieting: Drive for thinness is different from drive for objective thinness. Journal of Abnormal Psychology, 119(2), 276–281. doi: 10.1037/a0018398 [DOI] [PubMed] [Google Scholar]
- Cohen PA (2014). Hazards of hindsight--monitoring the safety of nutritional supplements. The New England Journal of Medicine, 370(14), 1277–1280. doi: 10.1056/NEJMp1315559 [DOI] [PubMed] [Google Scholar]
- Cohen PA, Maller G, DeSouza R, & Neal-Kababick J (2014). Presence of banned drugs in dietary supplements following FDA recalls. Jama, 312(16), 1691–1693. doi: 10.1001/jama.2014.10308 [DOI] [PubMed] [Google Scholar]
- Darcy AM, Hardy KK, Lock J, Hill KB, & Peebles R (2013). The eating disorder examination questionnaire (EDE-Q) among university men and women at different levels of athleticism. Eating Behaviors, 14(3), 378–381. doi: 10.1016/j.eatbeh.2013.04.002 [doi] [DOI] [PubMed] [Google Scholar]
- Fairburn CG, & Beglin S (2008). Eating disorder examination questionnaire. In Fairburn CG (Ed.), Cognitive behavior therapy and eating disorders (pp. 309–313). New York: Guilford Press. [Google Scholar]
- Frati P, Busardo FP, Cipolloni L, Dominicis ED, & Fineschi V (2015). Anabolic androgenic steroid (AAS) related deaths: Autoptic, histopathological and toxicological findings. Current Neuropharmacology, 13(1), 146–159. doi: 10.2174/1570159X13666141210225414 [doi] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Froiland K, Koszewski W, Hingst J, & Kopecky L (2004). Nutritional supplement use among college athletes and their sources of information. International Journal of Sport Nutrition and Exercise Metabolism, 14(1), 104–120. [DOI] [PubMed] [Google Scholar]
- Galli N, Petrie TA, Reel JJ, Chatterton JM, & Baghurst TM (2014). Assessing the validity of the weight pressures in sport scale for male athletes. Psychology of Men & Masculinity, 15(2), 170–180. doi: 10.1037/a0031762 [DOI] [Google Scholar]
- Griffiths S, Murray SB, Dunn M, & Blashill AJ (2017). Anabolic steroid use among gay and bisexual men living in australia and new zealand: Associations with demographics, body dissatisfaction, eating disorder psychopathology, and quality of life doi://doi-org.ucsf.idm.oclc.org/10.1016/j.drugalcdep.2017.10.003 [DOI] [PubMed] [Google Scholar]
- Hildebrandt T, Alfano L, & Langenbucher JW (2010). Body image disturbance in 1000 male appearance and performance enhancing drug users doi://doi-org.ucsf.idm.oclc.org/10.1016/j.jpsychires.2010.01.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Karlson KA, Becker CB, & Merkur A (2001). Prevalence of eating disordered behavior in collegiate lightweight women rowers and distance runners. Clinical Journal of Sport Medicine: Official Journal of the Canadian Academy of Sport Medicine, 11(1), 32–37. [DOI] [PubMed] [Google Scholar]
- Kindlundh AM, Hagekull B, Isacson DG, & Nyberg F (2001). Adolescent use of anabolic-androgenic steroids and relations to self-reports of social, personality and health aspects. European Journal of Public Health, 11(3), 322–328. [DOI] [PubMed] [Google Scholar]
- Kristiansen M, Levy-Milne R, Barr S, & Flint A (2005). Dietary supplement use by varsity athletes at a canadian university. International Journal of Sport Nutrition and Exercise Metabolism, 15(2), 195–210. [DOI] [PubMed] [Google Scholar]
- Lavender JM, De Young KP, & Anderson DA (2010). Eating disorder examination questionnaire (EDE-Q): Norms for undergraduate men. Eating Behaviors, 11(2), 119–121. doi: 10.1016/j.eatbeh.2009.09.005 [doi] [DOI] [PubMed] [Google Scholar]
- Lieberman HR, Marriott BP, Williams C, Judelson DA, Glickman EL, Geiselman PJ, . . . Mahoney CR (2015). Patterns of dietary supplement use among college students. Clinical Nutrition (Edinburgh, Scotland), 34(5), 976–985. doi: 10.1016/j.clnu.2014.10.010 [DOI] [PubMed] [Google Scholar]
- Luce KH, Crowther JH, & Pole M (2008). Eating disorder examination questionnaire (EDE-Q): Norms for undergraduate women. The International Journal of Eating Disorders, 41(3), 273–276. doi: 10.1002/eat.20504 [doi] [DOI] [PubMed] [Google Scholar]
- McDonald AH, Pritchard M, & McGuire MK (2019). Self-reported eating disorder risk in lean and non-lean NCAA collegiate athletes. Eating and Weight Disorders: EWD, doi: 10.1007/s40519-019-00681-0 [DOI] [PubMed] [Google Scholar]
- McDowall JA (2007). Supplement use by young athletes. Journal of Sports Science & Medicine, 6(3), 337–342. [PMC free article] [PubMed] [Google Scholar]
- Murray SB, Griffiths S, Mond JM, Kean J, & Blashill AJ (2016). Anabolic steroid use and body image psychopathology in men: Delineating between appearance- versus performance-driven motivations. Drug and Alcohol Dependence, 165, 198–202. doi: 10.1016/j.drugalcdep.2016.06.008 [doi] [DOI] [PubMed] [Google Scholar]
- Nagata JM, Capriotti MR, Murray SB, Compte EJ, Griffiths S, Bibbins-Domingo K, . . . Lunn MR (2019). Community norms for the eating disorder examination questionnaire among cisgender gay men. European Eating Disorders Review: The Journal of the Eating Disorders Association, doi: 10.1002/erv.2708 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nagata JM, Murray SB, Bibbins-Domingo K, Garber AK, Mitchison D, & Griffiths S (2019). Predictors of muscularity-oriented disordered eating in US young adults: A prospective cohort study. Int J Eat Disord, 52(12), 1380–1388. doi: 10.1002/eat.23094 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Neumark-Sztainer D (2010). Project EAT 2010 and F-EAT surveys - derived variables and scales. Retrieved from http://docs.sph.umn.edu/epich/eat/EAT2010_FEAT_Psychometrics.pdf [Google Scholar]
- Neumark-Sztainer D, Wall M, Larson NI, Eisenberg ME, & Loth K (2011). Dieting and disordered eating behaviors from adolescence to young adulthood: Findings from a 10-year longitudinal study. Journal of the American Dietetic Association, 111(7), 1004–1011. doi: 10.1016/j.jada.2011.04.012 [doi] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Piacentino D, Kotzalidis GD, Longo L, Pavan A, Stivali L, Stivali G, . . . Sani G (2017). Body image and eating disorders are common among professional and amateur athletes using performance and image enhancing drugs: A cross-sectional study. Journal of Psychoactive Drugs, 49(5), 373–384. doi: 10.1080/02791072.2017.1359708 [DOI] [PubMed] [Google Scholar]
- Piran N, & Robinson SR (2006). Associations between disordered eating behaviors and licit and illicit substance use and abuse in a university sample. Addictive Behaviors, 31(10), 1761–1775. doi: 10.1016/j.addbeh.2005.12.021 [DOI] [PubMed] [Google Scholar]
- Pope HG Jr, Wood RI, Rogol A, Nyberg F, Bowers L, & Bhasin S (2014). Adverse health consequences of performance-enhancing drugs: An endocrine society scientific statement. Endocrine Reviews, 35(3), 341–375. doi: 10.1210/er.2013-1058 [doi] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith RN, Agharkar AS, & Gonzales EB (2014). A review of creatine supplementation in age-related diseases: More than a supplement for athletes. F1000Research, 3, 222. doi: 10.12688/f1000research.5218.1 [doi] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Thiblin I, Garmo H, Garle M, Holmberg L, Byberg L, Michaelsson K, & Gedeborg R (2015). Anabolic steroids and cardiovascular risk: A national population-based cohort study. Drug and Alcohol Dependence, 152, 87–92. doi: 10.1016/j.drugalcdep.2015.04.013 [doi] [DOI] [PubMed] [Google Scholar]
- Young S, Touyz S, Meyer C, Arcelus J, Rhodes P, Madden S, . . . Hay P (2017). Validity of exercise measures in adults with anorexia nervosa: The EDE, compulsive exercise test and other self-report scales. The International Journal of Eating Disorders, 50(5), 533–541. doi: 10.1002/eat.22633 [DOI] [PubMed] [Google Scholar]