

Abstract
Accurately diagnosing urinary tract infections (UTIs) in hospitalized patients remains challenging, requiring correlation of frequently non-specific symptoms and laboratory findings. Urine cultures (UCs) are often ordered indiscriminately, especially in patients with urinary catheters, despite the Infectious Diseases Society of America guidelines recommending against routine screening for asymptomatic bacteriuria (ASB).1,2 Positive UCs can be difficult for providers to ignore, leading to unnecessary antibiotic treatment of ASB.2,3 Using diagnostic stewardship to limit UCs to situations with a positive urinalysis (UA) can reduce inappropriate UCs since the absence of pyuria suggests absence of infection.4–6 We assessed the impact of the implementation of a UA with reflex to UC algorithm (“reflex intervention”) on UC ordering practices, diagnostic efficiency, and UTIs using a quasi-experimental design.
Methods:
We retrospectively studied three hospitals (one 300-bed community, one 500-bed academic-community tertiary care, and one 500-bed academic tertiary care) in the same healthcare network, using a single electronic medical record (EMR) (PowerChart Millennium, Cerner Corporation, North Kansas City, MO). For socialization prior to implementation, the reflex UC order was available alongside the routine UC order starting 4/2017 as a soft rollout. On 8/1/2017, all hospitals implemented the reflex intervention, where the default inpatient UC order was replaced with an order set with two options: 1) a pre-checked (except for orders within obstetric, neutropenic fever, neonatal, renal transplant or pre-urology procedure order sets) order for UA with microscopy which reflexes to UC only if the UA has ≥10 white blood cells per high-power field and 2) a UC without a UA (non-reflex UC). Embedded clinical decision support suggested non-reflex UC orders be limited to patients who were pregnant, neutropenic, aged <1-year, renal transplant recipients or undergoing a urologic procedure.
The primary outcomes were the change in rates of non-reflex and total UCs ordered per 1000 patient-days, before (10/1/2015–7/31/2017) and after (8/1/2017–7/31/2018) the intervention. The secondary outcomes assessed the change in UTIs per 1000 patient-days and diagnostic efficiency (proportion of UCs with bacterial growth). UTIs were determined by pooling catheter-associated UTIs (CAUTIs) as defined by the National Healthcare Safety Network (NHSN) and admissions with an ICD-10 code adapted from the Agency for Healthcare Research and Quality (AHRQ) Prevention Quality Indicator (PQI) 12 for UTI or UTI in pregnancy (Supplemental Table 1). We compared median monthly rates and interquartile ranges (IQR) with Wilcoxon rank sum tests and proportions using χ2 tests. An interrupted time series (ITS) analysis using an autoregressive segmented linear regression model estimated the change in monthly UC and UTI rates associated with the intervention while controlling for unmeasured trends in time. The potential monthly decrease in UCs and UTIs attributable to the intervention was calculated by multiplying the adjusted rate difference by the median number of patient-days (32,892.5).
Results:
UC order rates
The median monthly rate of non-reflex UC orders/1,000 patient-days decreased by 75.6% after implementing the reflex initiative (35.2 [IQR: 33.1–35.7] pre-intervention vs. 8.6 [IQR: 8.2–9.0] post-intervention, p <0.001) (Supplemental Table 1). Total UC orders/1,000 patient-days also decreased from 35.2 (IQR: 33.1–35.7) to 18.6 (IQR: 18.1–19.6, p<0.001), a decrease of 47.2%. In an ITS analysis, the intervention decreased the monthly non-reflex UC rate by 16.8 cultures/1000 patient-days (p<0.001, Figure 1) and the total UC rate by 12.4 cultures/1000 patient-days (p<0.001, Figure 1), corresponding to a potential monthly decrease of 408 UCs.
Figure 1:
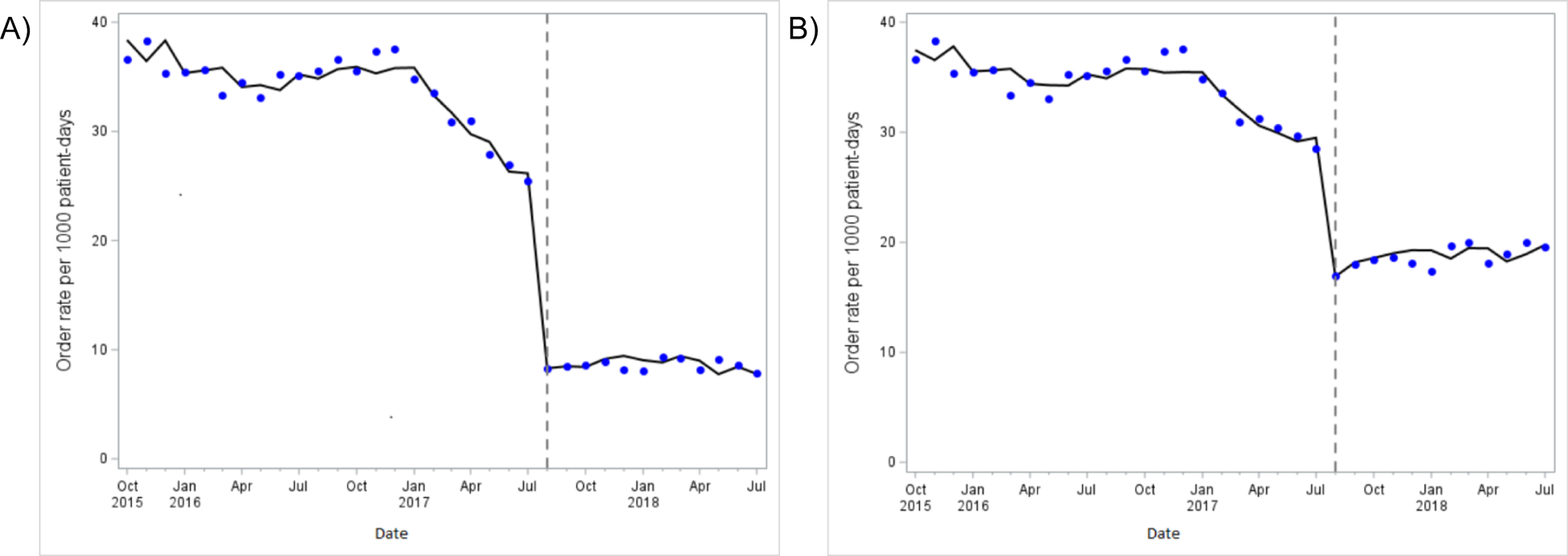
Monthly rates of non-reflex urine cultures (A) and total urine cultures (B) ordered per 1,000 patient-days before and after the intervention (dashed line). The data points represent the observed monthly rates and the solid line represents the autoregressive model.
Diagnostic efficiency
Post-intervention the proportion of UCs performed with bacterial growth increased (22.2% vs. 30.5%, p<0.001) and reflex UCs were more likely to yield bacterial growth than non-reflex UCs (41.0% vs. 18.2%, p<0.001).
UTI rates
The median monthly rate of UTIs/1,000 patient-days decreased after the intervention (16.1 [IQR:15.4–17.4] vs. 14.7 [IQR: 14.5–15.3], p<0.001). In the ITS analysis, the intervention decreased monthly UTIs/1,000 patient-days by 1.5 (p=0.04) for a potential monthly decrease of 49 UTIs.
Discussion:
Implementing a reflex UC intervention significantly decreased potentially inappropriate UCs ordered without a UA and total UCs ordered per month by almost 50%. With an estimated decrease of 408 UCs/month at a cost of $15 per culture7 our healthcare system saved $6,120/month in laboratory costs and increased diagnostic efficiency.
Our results are consistent with prior studies demonstrating that diagnostic stewardship can decrease UC orders,7,8 and CAUTIs in intensive care units.9 To our knowledge, our study is the first to demonstrate that UTIs in hospitalized patients may decrease following a reflex UC intervention. We postulate the decrease in UTIs may reflect more accurate diagnoses, as asymptomatic patients without pyuria could no longer be incorrectly diagnosed with a UTI. Alternatively, the intervention may have increased awareness of inappropriate UTI diagnoses and led to changes in coding behavior. Similar interventions may reduce the number of patients at risk for adverse events from receiving antibiotics for ASB.3,10 However, pyuria alone should not be used as a surrogate for ordering a UC or antibiotic treatment. Limitations to this study include: 1) we could not assess appropriateness of non-reflex UC orders, 2) UTI rates were determined primarily from administrative and not clinical data, and 3) due to the soft rollout of the reflex order prior to the full implementation, we may have underestimated the effect of the intervention.
In conclusion, a reflex UC intervention can be an effective diagnostic stewardship tool to reduce unnecessary UCs, improve diagnostic efficiency, and limit inappropriately diagnosed UTIs. Improved clinical decision support to determine when to order a UC using readily available clinical data may help to further reduce potentially inappropriate UC orders.
Supplementary Material
Acknowledgements
Financial support: JHA was partly supported by the National Center for Advancing Translational Sciences of the National Institutes of Health [UL1TR002378 and TL1TR002382]. JTJ was partly supported by the Centers for Disease Control and Prevention Epicenters (U01CK00054). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the Centers for Disease Control and Prevention.
The authors would like to acknowledge information technology, infection prevention, nursing and hospital leadership at Emory Healthcare who helped to implement and support this study initiative.
Footnotes
Potential conflicts of interest: All authors report no conflicts of interest relevant to this article.
Previous presentation: A preliminary version of this work was presented at the Society to Improve Diagnosis in Medicine Annual International Conference (October 2018)
References:
- 1.Nicolle LE, Gupta K, Bradley SF, et al. Clinical Practice Guideline for the Management of Asymptomatic Bacteriuria: 2019 Update by the Infectious Diseases Society of America. Clin Infect Dis 2019;68:e83–e110. [DOI] [PubMed] [Google Scholar]
- 2.Leis JA, Gold WL, Daneman N, Shojania K, McGeer A. Downstream Impact of Urine Cultures Ordered without Indication at Two Acute Care Teaching Hospitals. Infect Control Hosp Epidemiol 2013;34:1113–1114. [DOI] [PubMed] [Google Scholar]
- 3.Spivak ES, Burk M, Zhang R, et al. Management of Bacteriuria in Veterans Affairs Hospitals. Clin Infect Dis 2017;65:910–917. [DOI] [PubMed] [Google Scholar]
- 4.Kayalp D, Dogan K, Ceylan G, Senes M, Yucel D. Can routine automated urinalysis reduce culture requests? Clinical Biochemistry 2013;46:1285–1289. [DOI] [PubMed] [Google Scholar]
- 5.Stovall RT, Haenal JB, Jenkins TC, et al. A negative urinalysis rules out catheter-associated urinary tract infection in trauma patients in the intensive care unit. J Am Coll Surg 2013;217:162–166. [DOI] [PubMed] [Google Scholar]
- 6.Simerville JA, Maxted WC, Pahira JJ. Urinalysis: A Comprehensive Review. AFP 2005;71:1153–1162. [PubMed] [Google Scholar]
- 7.Munigala S, Rojek R, Wood H, et al. Effect of changing urine testing orderables and clinician order sets on inpatient urine culture testing: Analysis from a large academic medical center. Infect Control Hosp Epidemiol 2019;40:281–286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Munigala S, Jackups RR, Poirier RF, et al. Impact of order set design on urine culturing practices at an academic medical centre emergency department. BMJ Qual Saf 2018;27:587–592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Epstein L, Edwards JR, Halpin AL, et al. Evaluation of a Novel Intervention to Reduce Unnecessary Urine Cultures in Intensive Care Units at a Tertiary Care Hospital in Maryland, 2011–2014. Infect Control Hosp Epidemiol 2016;37:606–609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Zalmanovici Trestioreanu A, Lador A, Sauerbrun-Cutler M-T, Leibovici L. Antibiotics for asymptomatic bacteriuria. Cochrane Database Syst Rev 2015;4:CD009534. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.