

Abstract
Background:
Traditional exercises performed with the shoulder in the position of 90° abduction and external rotation with elbow flexion (90/90) while using a single elastic band showed moderate activity of both the lower trapezius (LT) and infraspinatus (IS) muscle. The purpose of this study was to investigate activity of the teres minor (TMi) and the LT muscles during standing external rotation exercise with the shoulder in the 90/90 position with 2 elastic bands in both the frontal and the scapular plane.
Hypothesis:
TMi, IS, and LT muscle activities will vary depending on whether the shoulder is positioned in the frontal or scapular plane with the application of 2 elastic bands. Also, the serratus anterior (SA) and teres major (TMa) muscles will produce different muscular activity patterns during exercises performed with 2 elastic bands in the frontal plane compared with the TMi and LT muscles.
Study Design:
Controlled laboratory study
Level of Evidence:
Level 4.
Methods:
A total of 21 collegiate baseball players volunteered to participate. The electromyography (EMG) activities of the TMi, IS, LT, SA, TMa, middle deltoid (MD), posterior deltoid, and upper trapezius (UT) muscles were measured with the 90/90 arm position during both isometric and oscillation resistance exercises with 2 elastic bands oriented in the frontal and scapular planes.
Results:
A significant difference was observed in EMG activity of both the TMi and the LT muscles between single and double elastic band applications in the frontal plane (P < 0.05). In contrast, EMG activity of the IS, SA, and TMa muscles was significantly increased in the scapular plane compared with the frontal plane (P < 0.05).
Conclusion:
The standing 90/90 position effectively increased both TMi and LT muscle EMG activity with the double elastic band in the frontal plane while minimizing UT and MD muscle activity. EMG activity of the IS, SA, and TMa muscles increased with exercise in the scapular plane as compared with the frontal plane.
Clinical Relevance:
Oscillation movement under double elastic band application differentiated external rotator muscle and scapular muscle activities between the frontal and scapular plane during the 90/90 exercise in the frontal plane compared with the scapular plane. Clinicians can utilize each of the scapular and frontal positions based on their desired focus for muscular activation.
Keywords: electromyography, teres minor, lower trapezius, elastic resistance exercise, overhead athletes
The modulation of infraspinatus (IS) muscle activity has been identified in a variety of intervention exercises for injury prevention.1-3,9,24,28 However, professional tennis players present with IS atrophy syndrome to which the cause is uncertain.31 Another shoulder external rotator muscle, the teres minor (TMi) muscle, generates up to 45% of external rotation (ER) force compared with the IS muscle.17,30 In contrast to the IS muscle, the TMi muscle produces relatively high activity during the deceleration and follow-through phases of throwing motion,7,10 which may be associated with posterior shoulder tightness identified in glenohumeral horizontal adduction of range of motion.16 Baseball pitchers may also be predisposed to posteroinferior labral lesions, which are associated with the deceleration phase of pitching.22
The lower trapezius (LT) specifically maintains the posterior tilt of the scapula in the late cocking phase of throwing or the tennis serve.13,15 LT muscle activity deficit is associated with scapular dyskinesis, leading to a superior labrum anterior and posterior lesion in a college baseball pitcher.29 Previous studies have measured periscapular muscle activities in intervention exercises with a therapeutic elastic band.12,20,28 The elastic band can minimize the activity of the upper trapezius (UT) and middle deltoid (MD) muscles as it utilizes the tension of elongation with less gravity effect.28 No study has yet investigated TMi and LT muscle activities in different scapular planes using the elastic band. Therefore, the purpose of this study was to compare the modulation of TMi and LT muscle activity using elastic resistance between the frontal and scapular planes during the standing position with double elastic band application and oscillation movement (OSC). This study hypothesized that a second elastic band applied to the distal portion of the arm would independently increase horizontal adduction resistance, leading to an increase in TMi and LT muscle activities. This study also hypothesized that exercises performed in the frontal plane would produce different muscle activities from similar exercises performed in the scapular plane.
Methods
A total of 21 collegiate baseball players belonging to the National Collegiate Athletic Association Division I conference (mean height, 181.4 ± 7.7 cm; mean weight, 87.8 ± 10.0 kg; mean age, 19.0 ± 1.1 years) volunteered to participate in this study. All participants gave informed consent to the procedures as approved by the institutional review board of the university prior to testing. All participants were asymptomatic, competitive baseball players without neurologic or physiologic deficits in the upper body based on the completion of a preliminary screening questionnaire.
Electrode Placement
Raw electromyography (EMG) amplitudes of the TMi, LT, IS, teres major (TMa), and serratus anterior (SA) muscle activities were collected during intervention exercises. This study additionally measured posterior deltoid (PD), MD and UT muscle EMG activities to determine the degree of intensity of each intervention exercise. Bipolar surface silver EMG electrodes with a bar length of 10 mm, width of 1 mm, and a distance of 1 cm between active recording sites (Delsys Bagnoli-8; Delsys Inc) were used. Electrodes were placed on the center of the muscle belly in line with the muscle fibers for the specific manual muscle test as follows: TMi, one-third of the distance from the posterior portion of the acromion process to the inferior angle of the scapula on the lateral aspect of the lateral border of the scapula23; IS, inferior and parallel to the scapular spine on the lateral aspect over the IS fossa3; TMa, the lateral border of the inferior angle of scapula; PD, at an oblique direction parallel to the muscle fibers of the deltoid muscles at the lateral border of the scapular spine26,27; MD, halfway between the tip of the acromion process and deltoid tubercle3; UT, at the halfway point between the C7 spinous process and the acromion process; LT, at an oblique angle from the scapular spine and just outside of the scapular medial border; SA, below the axilla between the latissimus dorsi and pectoralis major at the level of the inferior angle of the scapula.14,25 The reference electrode was placed over the spine of the scapula or between the electrodes of the UT and IS muscles.
Exercise Protocol
Once the electrodes were secured, the athletes performed a maximum voluntary isometric contraction (MVIC) for each muscle using manual muscle testing procedures for normalization of EMG data. The manual pressure was applied by the same examiner for all testing positions.
The athletes performed isometric contractions (ISO) and OSC in both the frontal and scapular planes in a standing position for EMG data collection with the shoulder in the position of 90° abduction (ABD) and ER with elbow flexion to 90° (90/90). Both ISO and OSC exercises were used with an elastic band (Green CLX, 2.1 kg at 100% elongation; TheraBand; Performance Health) at 40% elongation (single band).28 The athletes were also given another elastic band (Blue CLX, 2.6 kg at 100% elongation; TheraBand) at 40% elongation on the distal portion of the arm directly above the elbow (double band). The players oscillated the distal aspect of their upper extremity in the 90/90 arm position while externally rotating the shoulder and releasing the externally rotated shoulder to the original position at a constant pace following a cue from a metronome set at 150 beats per minute.28
To identify the intensity of the elastic resistance exercises, the amount of MVIC force (N·m) of ER was measured in the 90/90 arm position using a handheld dynamometer (MicroFET; Hoggan Scientific, LLC) for each participant in the standing position prior to the exercise protocol. The examiner applied maximal resistance to the distal portion of the pronated forearm on the participant’s dominant side to create shoulder internal rotation while holding the elbow joint with the other hand. The athletes were then given 20% MVIC manual resistance (MR) in an isometric contraction (20% MR) with or without the elastic band above the elbow in both the frontal and the scapular planes. Identical procedures were followed for the scapular and frontal planes for isometric and oscillation conditions. A randomized exercise sequence was used to minimize the systematic effect of motor learning and fatigue for each participant.
Data Analysis
The EMG activities were collected using a data collection program (MP 150 Data Acquisition System; Biopac System Inc) with a sample rate of 1000 Hz; all data were recorded and stored in a computer for offline analysis. The mean EMG activity of the middle 2 seconds of each 4-second maximum isometric contraction was calculated to determine the individual’s MVIC. For the exercises, the mean EMG activity of the middle 5 seconds of each 15-second intervention exercise was calculated. All data were calculated in root-mean-square (RMS) values, normalized to MVIC of the corresponding muscles, and presented as percentage of MVIC (% MVIC).
A 2 × 2 × 3 (Frontal/Scapular × Single/Double × ISO/20% MR/OSC) repeated-measures analysis of variance design was used to determine any significant differences in each of the normalized RMS values. A post hoc test with Tukey honestly significant difference was used to measure any significant difference across the 3 different exercise intensities. The level of significance was set at the 0.05 level of probability.
Results
Teres Minor and Infraspinatus
Mean values and 95% CIs for TMi, IS, LT, TMa, and SA EMG activities (% MVIC) are presented in Table 1. The mean values of TMi EMG activity in the frontal plane were significantly greater with both the single and double elastic bands than those of the scapular plane regardless of exercise conditions (P < 0.05). Also, the mean values of TMi EMG activity were significantly greater with the double elastic band in the frontal plane than those of the single elastic band regardless of exercise conditions (P < 0.05). Figure 1 indicates the marginal mean of TMi EMG activity that is compared between the frontal and scapular planes with 2 different elastic band applications. In contrast, the mean value of IS EMG activity in the scapular plane was significantly greater with the single elastic band than the frontal plane (P < 0.05), while no difference was observed with the double elastic band between the 2 planes.
Table 1.
Mean EMG activity reported as % MVIC (95% CIs) a
| Frontal Plane | Single | Double | ||||
|---|---|---|---|---|---|---|
| ISO | 20% MR | OSC | ISO | 20% MR | OSC | |
| Teres minor | 14.6(10.3, 18.8)*†‡‡ | 19.9(13.9, 24.9)*†‡‡ | 29.7(25.3, 33.9)*†‡‡ | 21.4(14.9, 26.6)*†‡‡ | 28.3(20.8, 34.0)*†‡‡ | 35.5(29.8, 40.3)*†‡‡ |
| Infraspinatus | 31.1(28.1, 34.7)‡ | 36.4(31.8, 40.7)*†‡ | 64.7(58.6, 69.8)‡‡ | 35.1(30.3, 39.5)‡‡ | 45.8(40.2, 50.6)†‡‡ | 68.0(60.2, 73.8)‡‡ |
| Lower trapezius | 34.1(28.7, 38.7)*†‡‡ | 42.7(35.3, 48.5)*‡‡ | 55.4(48.0, 61.1)*‡‡ | 39.8(32.9, 45.2)*†‡‡ | 47.5(42.0, 52.3)*‡ | 58.0(50.4, 63.8)*‡‡ |
| Teres major | 21.2(14.7, 26.4)‡ | 23.2(17.3, 28.1)*†‡ | 46.3(33.8, 54.5)*‡‡ | 21.9(15.8, 27.0)‡ | 30.9(22.0, 37.4)†‡ | 42.8(32.9, 49.8)‡‡ |
| Serratus anterior | 24.3(19.0, 29.0)‡ | 25.0(20.5, 29.3)‡ | 39.6(30.2, 46.3)‡‡ | 22.6(17.0, 27.4)‡ | 24.1(18.7, 28.9)‡ | 38.8(30.9, 44.8)‡‡ |
| Single | Double | |||||
| Scapular Plane | ISO | 20% MR | OSC | ISO | 20% MR | OSC |
| Teres minor | 9.3(6.7, 12.7)*‡ | 13.5(10.1, 17.2)*‡ | 22.1(17.6, 26.3)*‡‡ | 10.6(7.6, 14.0)*‡‡ | 15.9(12.1, 19.8)*‡‡ | 24.9(19.5, 29.6)*‡‡ |
| Infraspinatus | 32.4(26.6, 37.3)‡‡ | 41.9(35.4, 47.2)*†‡‡ | 68.4(60.7, 74.3)‡‡ | 34.0(28.2, 38.9)‡‡ | 47.0(39.5, 52.8)†‡‡ | 66.0(57.9, 72.0)‡‡ |
| Lower trapezius | 26.0(20.9, 30.5)*‡‡ | 36.1(29.3, 41.5)*‡‡ | 46.6(38.6, 52.6)*‡‡ | 28.6(24.1, 32.9)*‡‡ | 35.4(31.0, 39.6)*‡ | 45.5(38.3, 51.1)*‡‡ |
| Teres major | 24.3(17.0, 29.9)‡ | 30.7(21.7, 37.1)*‡ | 51.7(38.0, 60.5)*†‡‡ | 25.6(16.8, 32.0)‡ | 33.6(23.3, 40.8)‡ | 46.4(35.2, 54.0)†‡‡ |
| Serratus anterior | 27.4(21.9, 32.2)‡ | 26.7(22.4, 30.9)‡ | 39.9(30.7, 46.5)‡‡ | 28.0(21.1, 33.4)‡ | 29.0(21.4, 34.7)‡ | 41.3(30.6, 48.7)‡‡ |
EMG, electromyography; ISO, isometric contraction; MR, manual resistance; MVIC, maximum voluntary isometric contraction; OSC, oscillation movement.
The means and 95% CIs (in parentheses) of teres minor, infraspinatus, lower trapezius, teres major, and serratus anterior muscle activities (% MVIC) between the frontal and scapular planes across 3 different intensities with the single and double elastic bands.
Significant difference between the frontal and scapular planes with each band condition at each intensity (P < 0.05).
Significant difference between the single and double elastic bands at each intensity in each plane (P < 0.05).
Significant difference across the different intensities with each band condition in each plane (the critical value of the Tukey honestly significant difference = 5.22% for the teres minor, 9.17% for the infraspinatus, 8.09% for the lower trapezius, 9.66% for the teres major, and 8.56% for the serratus anterior; P < 0.05).
Figure 1.

Marginal mean values of normalized teres minor electromyographic (EMG) activity between the frontal and scapular planes and between the single and double elastic bands. Note that the mean values of the double elastic band were significantly greater than those of the single elastic band for both the frontal and the scapular planes. The error bars denote the SEM. *P < 0.05. MVIC, maximum voluntary isometric contraction; RMS, root mean square.
LT, TMa, and SA
The mean values of LT EMG activity were significantly greater in the frontal plane with both single and double elastic bands than those of the scapular plane regardless of exercise conditions (P < 0.05). Specifically, the mean value of LT EMG activity was significantly greater with the double elastic band during ISO in the frontal plane than that of the single elastic band (P < 0.05). Figure 2 indicates the marginal mean of LT EMG activity that was compared between the frontal and scapular planes with 2 different elastic band applications. LT EMG activity was significantly greater with the double elastic band in the frontal plane than that of the single elastic band, while no difference was observed between the single and double elastic bands in the scapular plane.
Figure 2.
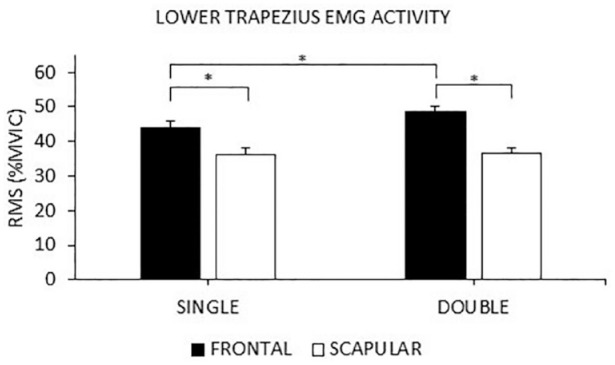
Marginal mean values of normalized lower trapezius electromyographic (EMG) activity between the frontal and scapular planes and between the single and double elastic bands. Note that the mean values of the double elastic band were significantly greater than those of the single elastic band in the frontal plane, while no difference was observed in the scapular planes. The error bars denote the SEM. *P < 0.05. MVIC, maximum voluntary isometric contraction; RMS, root mean square.
The mean values of TMa EMG activity were significantly less in the frontal plane with the single elastic band during both 20% MR and OSC than those of the scapular plane (P < 0.05). The mean value of TMa EMG activity was significantly greater with the single elastic band during OSC in the scapular plane than that of the double elastic band (P < 0.05).
The mean value of SA EMG activity was significantly greater during OSC with both the single and double elastic bands than that of both ISO and 20% MR in both frontal and scapular planes (P < 0.05). No other differences were observed between the single and double elastic bands in either frontal or scapular plane regardless of exercise conditions.
PD, MD, and UT
Mean values for PD, MD, and UT EMG activities (% MVIC) are presented in Table 2. The 3 EMG activities were significantly greater in the frontal plane than those of the scapular plane (P < 0.05). It was clearly observed that the intervention exercises conducted in this study were categorized at the moderate intensity.7
Table 2.
Mean EMG activity reported as % MVIC a
| Frontal Plane | Scapular Plane | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Single | Double | Single | Double | |||||||||
| % MVIC | ISO | 20% MR | OSC | ISO | 20% MR | OSC | ISO | 20% MR | OSC | ISO | 20% MR | OSC |
| Posterior deltoid | 11 | 15 | 18 | 18 | 20 | 27 | 3 | 5 | 7 | 6 | 7 | 13 |
| Middle deltoid | 15 | 18 | 24 | 21 | 23 | 33 | 11 | 11 | 15 | 14 | 12 | 22 |
| Upper trapezius | 21 | 19 | 21 | 25 | 27 | 28 | 16 | 14 | 17 | 17 | 15 | 23 |
ISO, isometric contraction; MR, manual resistance; MVIC, maximum voluntary isometric contraction; OSC, oscillation movement.
The mean values of posterior deltoid, middle deltoid, and upper trapezius activities (% MVIC) between the frontal and scapular planes across 3 different intensities with the single and double elastic bands. Note that based on those 3 electromyographic activities, any of the intervention exercise intensities can be categorized at no further than a moderate level.
Discussion
The mean ratios of TMi to IS muscle activity with the double elastic band in the frontal plane were 0.65, 0.62, and 0.54 for ISO, 20% MR, and OSC, respectively, whereas those mean ratios in the scapular plane were 0.31, 0.35, and 0.40, respectively. This suggests that TMi muscle activity is more involved in the frontal plane, whereas IS muscle activity is more dominant in the scapular plane.
This study demonstrated that OSC with the double elastic band in the frontal plane activated the LT muscle up to 58% MVIC. This finding is in line with the previous study in which the LT muscle activity of 50% MVIC was observed against a manually applied isometric force from the posterior to anterior direction with the arm horizontally abducted at 90° of ABD in the frontal plane.18 Consequently, based on the results of the present study, both the LT and the TMi muscles can be effectively activated in the frontal plane while in the standing 90/90 arm position.
None of the free motion kinetic chain exercises, such as the Lawnmower and Robbery exercises, activated the LT muscle more than 30% MVIC performed with body mass or in unloaded conditions demonstrated in the previous studies.14,19 Our previous studies also demonstrated that the Robbery exercise with different ABD angles of the glenohumeral joint with dumbbell resistance loads up to 7% of the participant’s body weight activated the LT muscle 47% to 59% MVIC while activating the UT muscle up to 82% MVIC.21,27 However, the desired ratio of UT to LT muscle activity should be lower than 1.0 to achieve optimal scapulothoracic kinetic chain motion.4,5 Thus, the OSC exercise coupled with the double elastic band technique may allow the patient to highly activate the LT muscle in the frontal plane while minimizing both UT and MD muscle activities.
With regard to IS muscle activity in the 90/90 arm position with the single elastic band during ISO in the frontal plane, the load of 0.84 kg (40% of 2.1 kg at 100% elongation) activated the IS at a level of 31% MVIC, which was comparable with IS activation level of 27% MVIC with the load of 0.68 kg (40% of 1.7 kg at 100% elongation) found in our previous study.28 Similar IS muscle activity has also been shown in the standing ER isometric exercise achieved by stepping out laterally with 0° of ABD and ER of the glenohumeral joint and the elbow flexed to 90°.20 The present study found that IS muscle activity was increased in the scapular plane compared with the frontal plane. This suggests that IS muscle activity can be associated with the optimal length-tension relationship that occurs in the scapular plane.8
Both TMa and SA muscle activities were increased in the scapular plane compared with the frontal plane as well. However, there was no difference between the single and double elastic band conditions. These findings propose that the double elastic band independently enhances TMi and LT muscle resistance while the athletes maintained the standing 90/90 arm position in the frontal plane and does not have a similar effect on the TMa and SA muscles.
Limitations
TMi muscle activity measured using a surface EMG electrode may not be as accurate as an EMG needle.11,26 One reason for this is that the contamination of crosstalk signals from the PD or long head of the triceps brachii muscle may affect the quantity of TMi muscle activity. This study, however, used an inter-electrode spacing distance of 10 mm for surface EMG, which may reduce contamination of crosstalk signals.6 Also, this study tested highly trained collegiate baseball players with asymptomatic shoulders. Thus, implication of these findings to individuals with differing age, levels of performance, or shoulder symptoms likely has limitations.
Conclusion
The standing 90/90 arm position with double elastic band exercise increased both TMi and LT muscular activation in the frontal plane compared with the scapular plane. This study also identified significant increases in muscle activation using OSC as compared with ISO exercise or 20% MR. The results of this study have clinical implications regarding the careful selection of exercise intensity and arm position when using elastic resistance exercise for the shoulder.
Acknowledgments
The authors thank Deanna Geraci, MA, ATC, for her assistance with data collection during this study.
Footnotes
The authors report no potential conflicts of interest in the development and publication of this article.
References
- 1. Alenabi T, Whittaker RL, Kim SY, Dickerson CR. Arm posture influences on regional supraspinatus and infraspinatus activation in isometric arm elevation efforts. J Electromyogr Kinesiol. 2019;44:108-116. [DOI] [PubMed] [Google Scholar]
- 2. Alpert SW, Pink MM, Jobe FW, McMahon PJ, Mathiyakom W. Electromyographic analysis of deltoid and rotator cuff function under varying loads and speeds. J Shoulder Elbow Surg. 2000;9:47-58. [DOI] [PubMed] [Google Scholar]
- 3. Bitter NL, Clisby EF, Jones MA, Magarey ME, Jaberzadeh S, Sandow MJ. Relative contributions of infraspinatus and deltoid during external rotation in healthy shoulders. J Shoulder Elbow Surg. 2007;16:563-568. [DOI] [PubMed] [Google Scholar]
- 4. Cools AM, Dewitte V, Lanszweert F, et al. Rehabilitation of scapular muscle balance: which exercises to prescribe? Am J Sports Med. 2007;35:1744-1751. [DOI] [PubMed] [Google Scholar]
- 5. Cools AM, Struyf F, De Mey K, Maenhout A, Castelein B, Cagnie B. Rehabilitation of scapular dyskinesis: from the office worker to the elite overhead athlete. Br J Sports Med. 2014;48:692-697. [DOI] [PubMed] [Google Scholar]
- 6. De Luca CJ, Kuznetsov M, Gilmore LD, Roy SH. Inter-electrode spacing of surface EMG sensors: reduction of crosstalk contamination during voluntary contractions. J Biomech. 2012;45:555-561. [DOI] [PubMed] [Google Scholar]
- 7. DiGiovine NM, Jobe FW, Pink M, Perry J. An electromyographic analysis of the upper extremity in pitching. J Shoulder Elbow Surg. 1992;1:15-25. [DOI] [PubMed] [Google Scholar]
- 8. Ellenbecker TS, Davies GJ. The application of isokinetics in testing and rehabilitation of the shoulder complex. J Athl Train. 2000;35:338-350. [PMC free article] [PubMed] [Google Scholar]
- 9. Ellenbecker TS, Sueyoshi T, Bailie DS. Muscular activation during plyometric exercises in 90° of glenohumeral joint abduction. Sports Health. 2015;7:75-79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Gowan ID, Jobe FW, Tibone JE, Perry J, Moynes DR. A comparative electromyographic analysis of the shoulder during pitching. Professional versus amateur pitchers. Am J Sports Med. 1987;15:586-590. [DOI] [PubMed] [Google Scholar]
- 11. Hamada J, Nimura A, Yoshizaki K, Akita K. Anatomic study and electromyographic analysis of the teres minor muscle. J Shoulder Elbow Surg. 2017;26:870-877. [DOI] [PubMed] [Google Scholar]
- 12. Joseph R, Alenabi T, Lulic T, Dickerson CR. Activation of supraspinatus and infraspinatus partitions and periscapular musculature during rehabilitative elastic resistance exercises. Am J Phys Med Rehabil. 2019;98:407-415. [DOI] [PubMed] [Google Scholar]
- 13. Kibler WB, Sciascia A. Evaluation and management of scapular dyskinesis in overhead athletes. Curr Rev Musculoskelet Med. 2019;12:515-526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Kibler WB, Sciascia AD, Uhl TL, Tambay N, Cunningham T. Electromyographic analysis of specific exercises for scapular control in early phases of shoulder rehabilitation. Am J Sports Med. 2008;36:1789-1798. [DOI] [PubMed] [Google Scholar]
- 15. Konda S, Yanai T, Sakurai S. Scapular rotation to attain the peak shoulder external rotation in tennis serve. Med Sci Sports Exerc. 2010;42:1745-1753. [DOI] [PubMed] [Google Scholar]
- 16. Laudner KG, Moline MT, Meister K. The relationship between forward scapular posture and posterior shoulder tightness among baseball players. Am J Sports Med. 2010;38:2106-2112. [DOI] [PubMed] [Google Scholar]
- 17. Melis B, DeFranco MJ, Lädermann A, Barthelemy R, Walch G. The teres minor muscle in rotator cuff tendon tears. Skeletal Radiol. 2011;40:1335-1344. [DOI] [PubMed] [Google Scholar]
- 18. Miyasaka J, Arai R, Ito T, et al. Isometric muscle activation of the serratus anterior and trapezius muscles varies by arm position: a pilot study with healthy volunteers with implications for rehabilitation. J Shoulder Elbow Surg. 2017;26:1166-1174. [DOI] [PubMed] [Google Scholar]
- 19. Moeller CR, Bliven KC, Valier AR. Scapular muscle-activation ratios in patients with shoulder injuries during functional shoulder exercises. J Athl Train. 2014;49:345-355. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Mullaney MJ, Perkinson C, Kremenic I, Tyler TF, Orishimo K, Johnson C. EMG of shoulder muscles during reactive isometric elastic resistance exercises. Int J Sports Phys Ther. 2017;12:417-424. [PMC free article] [PubMed] [Google Scholar]
- 21. Nakamura Y, Tsuruike M, Ellenbecker TS. Electromyographic activity of scapular muscle control in free-motion exercise. J Athl Train. 2016;51:195-204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Park SS, Loebenberg ML, Rokito AS, Zuckerman JD. The shoulder in baseball pitching: biomechanics and related injuries–part 1. Bull Hosp Jt Dis. 2002-2003;61:68-79. [PubMed] [Google Scholar]
- 23. Rathi S, Zacharias A, Green RA. Verification of a standardized method for inserting intramuscular electromyography electrodes into teres minor using ultrasound. Clin Anat. 2015;28:780-785. [DOI] [PubMed] [Google Scholar]
- 24. Reinold MM, Wilk KE, Fleisig GS, et al. Electromyographic analysis of the rotator cuff and deltoid musculature during common shoulder external rotation exercises. J Orthop Sports Phys Ther. 2004;34:385-394. [DOI] [PubMed] [Google Scholar]
- 25. Tsuruike M, Ellenbecker TS. Adaptation of muscle activity in scapular dyskinesis test for collegiate baseball players. J Shoulder Elbow Surg. 2016;25:1583-1591. [DOI] [PubMed] [Google Scholar]
- 26. Tsuruike M, Ellenbecker TS. Scapular muscle electromyographic activity during abduction exercises in the scapular plane in three positions. Int J Sports Phys Ther. 2019;14:935-944. [PMC free article] [PubMed] [Google Scholar]
- 27. Tsuruike M, Ellenbecker TS. Serratus anterior and lower trapezius muscle activities during multi-joint isotonic scapular exercises and isometric contractions. J Athl Train. 2015;50:199-210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Tsuruike M, Ellenbecker TS, Kagaya Y, Lemings L. Analysis of scapular muscle EMG activity during elastic resistance oscillation exercises from the perspective of different arm positions. Sports Health. 2020;12:395-400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Tsuruike M, Ellenbecker TS, Nishime RS. Electromyographic analysis of the scapular dyskinesis test in a baseball pitcher with a SLAP lesion: a case report. Int J Sports Phys Ther. 2020;15:471-477. [PMC free article] [PubMed] [Google Scholar]
- 30. Walch G, Boulahia A, Calderone S, Robinson AH. The “dropping” and “hornblower’s” signs in evaluation of rotator-cuff tears. J Bone Joint Surg Br. 1998;80:624-628. [DOI] [PubMed] [Google Scholar]
- 31. Young SW, Dakic J, Stroia K. High incidence of infraspinatus muscle atrophy in elite professional female tennis players. Am J Sports Med. 2015;43:1989-1993. [DOI] [PubMed] [Google Scholar]