

Abstract
Neck circumference is quick and simple to measure and thus an attractive proxy of neck strength, a putative mechanism underlying risk of sport-related concussion (SRC). Research, however, is limited on the relationship of neck circumference to SRC. Our study examined differences in neck circumference based on sex, concussion history, concussions experienced subsequent to college entry, and participation in sports with high versus low risk for contact. Neck circumference was measured in incoming NCAA Division I athletes (N = 324) from a large northeastern university during athlete pre-participation physicals. Sex, sport team, and self-reported concussion history were obtained from retrospective pre-participation questionnaires and medical chart review. Concussion diagnoses during college were collected subsequent to neck measurements from medical chart review. Proportional neck circumference (normalized by body-mass index) was computed. Each sport was categorized as involving high or low risk of contact (as a proxy of risk for injury). Sex differences in neck circumference and proportional neck circumference were assessed. Differences in neck circumference and proportional neck circumference were also characterized by contact risk and SRC history (with biological sex included as a covariate). Differences in neck circumference and proportional neck circumference were explored among those who did versus did not experience subsequent SRC diagnosis. Males had significantly larger neck circumference and proportional neck circumference than females. Neck circumference and proportional neck circumference were not related to SRC history or subsequent SRC. Neck circumference is a quick and simple measure; however, even when considered in proportion to body mass, it was unrelated to SRC. Future studies are needed to assess whether this is due to a lack of relationship between the neck and injury or limitations in circumference as a proxy measure of cervical spine characteristics and biomechanics.
Keywords: Concussion, Athletes, Sex differences, Neck circumference, Contact Sports, Neck Girth
Introduction
Stronger necks may reduce the magnitude of linear and rotational head acceleration upon impact, a potential mechanism of sport-related concussion (SRC; Guskiewicz & Mihalik, 2011). Neck circumference has been proposed as a simple proxy measure of other features of the cervical spine, such as neck strength (Tierney et al., 2005), yet research on neck strength is limited. One study of male and female high school athletes found that those who experienced a concussion during a season had smaller neck circumference, neck-to-head circumference ratio, and overall strength than uninjured athletes (Collins et al., 2014). The statistically significant differences in neck circumference, however, were modest (< 1 centimeter), and the neck-to-head circumference ratio difference was only significant for male athletes (Collins et al., 2014).
Female versus male athletes show greater head acceleration when purposefully heading a soccer ball (Bretzin, Mansell, Tierney, & McDevitt, 2017; Caccese, Buckley, Tierney, Rose, et al., 2018) and typically have smaller neck circumferences than males (Bretzin et al., 2017; Tierney et al., 2008). Reduced neck strength may be one mechanism that confers higher risk for female athletes sustaining a SRC in sex-comparable sports (Covassin, Moran, & Elbin, 2016). Understanding factors that increase risk of SRC in women is understudied and has significant public health implications as women may have worse cognitive outcomes (Covassin, Elbin, Harris, Parker, & Kontos, 2012; Sandel, Schatz, Goldberg, & Lazar, 2017), more complex symptom profiles (Sandel et al., 2017), and longer recovery timelines (Iverson et al., 2017; Tator et al., 2016) post-SRC.
Neck circumference was examined in relation to a history of SRC and contact sport-risk (collision/contact versus limited/non-contact athletes) while controlling for sex differences. In addition, exploratory analyses compared neck circumference in participants who had versus had not experienced a SRC subsequent to college entry. We predicted that female versus male athletes, on average, would have smaller neck circumferences (Bretzin et al., 2017; Tierney et al., 2005). We predicted that male athletes who experienced an SRC would have smaller neck circumferences compared to those who did not (Collins et al., 2014). We tentatively hypothesized that high contact sport-risk athletes would have larger neck circumferences as upper body strength training may differ by sports that involve purposeful contact.
Methods
Participants
Prospective or incoming collegiate student-athletes (N=324; 51% female) from 22 NCAA Division I teams (9 male) at a major U.S. university were recruited during standard pre-participation physicals (2013–2016). Informed consent was obtained from all individual participants included in the study and was approved by the university’s Institutional Review Board. All athletes were uninjured at the time of testing and medically cleared for athletic participation.
Materials
We measured neck circumference in inches (converted to centimeters) during the pre-participation physicals by a sports-medicine physician or athletic trainer. Circumference was measured over the thyroid cartilage (Streifer et al., 2019). Height (inches) and weight (pounds) were used to compute body mass index (BMI=(weight/height2)*703 = BMI in kg/m2; missing from 18 participants). Proportional neck circumference was calculated by dividing BMI by neck circumference to account for an individual’s overall body mass.
Biological sex (male/female), height, weight, and sport were collected from self-report questionnaires routinely administered to all incoming athletes. Sport teams were classified as high (collision/contact) or low (limited/non-contact) contact risk based on prior recommendations for relative risk of sustaining an acute injury (Rice, American Academy of Pediatrics Council on Sports, & Fitness, 2008).
Concussion history (yes/no) was determined from one self-report questionnaire item (“Have you ever had a head injury or concussion?”) that was completed as part of a research survey administered to prospective incoming student athletes during the summer prior to entry and from supplementary physician notes from standard medical chart completed by sports-medicine personnel. Data from 5 participants were not available in and were not included in the analyses; however, they were included in figures for reference. Subsequent concussion diagnosis (i.e., during college, subsequent to neck measurement) was determined from standard medical charts. All medical charts were retrospectively reviewed by research staff in December 2018 and double entered (i.e., by two study staff) into a structured survey; data were matched to check for consistency and ensure data entry accuracy.
Statistical Analyses
Univariate analysis of variance (ANOVA) and analysis of covariance (ANCOVA) were performed using SPSS 25 (IBM Corporation, Armonk, NY). Two dependent variables were used: neck circumference in centimeters and proportional neck circumference (BMI/neck circumference). Athletes with neck circumference (n = 1) or proportional neck circumference (n = 2) greater than three standard deviations above the group mean were identified as outliers; analyses were computed with and without outliers. Effect sizes (η2) were calculated to estimate magnitude of clinical effects. Post-hoc analyses were completed using independent sample t tests to characterize sex differences. Analyses were considered significant at p<0.05.
First, we assessed sex differences in neck circumference. Then, controlling for sex differences, we compared neck circumferences between individuals with and without SRC history and individuals in sports considered at high versus low contact risk. Finally, we compared neck circumferences in individuals who did versus did not experience a SRC subsequent to college entry. These latter analyses did not include sex due to the small sample size.
Results
Thirty-six male (23%) and 20 female (12%) athletes reported an SRC history (see Table 1). During college, 13 athletes (9 males) were subsequently diagnosed with an SRC.
Table 1.
Sample characteristics by group.
| Age | BMI | Neck Circumferenceb | Proportional Neck Circumference | |
|---|---|---|---|---|
|
All N = 324; N = 306a |
18.34 (0.97) | 23.82 (3.96) | 35.73 (4.45) | 1.51 (0.19) |
|
Male n = 159; n = 143a |
18.45 (1.05) | 25.53 (4.32) | 39.58 (2.74) | 1.57 (0.17) |
|
Female n = 165; n = 163a |
18.22 (0.87) | 22.31 (2.87) | 32.02 (1.87) | 1.45 (0.19) |
|
Low Contact Risk Sports n = 168; n = 161a |
18.29 (0.90) | 22.88 (3.76) | 34.38 (3.67) | 1.52 (0.21) |
|
High Contact Risk Sports n = 156; n = 145a |
18.38 (1.04) | 24.86 (3.93) | 37.18 (4.75) | 1.50 (0.17) |
|
No Concussion - Pre-college n = 263; n = 247a |
18.34 (0.98) | 23.72 (3.97) | 35.46 (4.45) | 1.50 (0.19) |
|
Concussion - Pre-college n = 56; n = 54a |
18.36 (0.98) | 24.23 (3.87) | 36.97 (4.42) | 1.53 (0.17) |
|
No Concussion - During college n = 311; n = 293a |
18.35 (0.98) | 23.80 (4.00) | 35.67 (4.45) | 1.51 (0.19) |
|
Concussion - During college n = 13 |
18.08 (0.64) | 24.29 (2.94) | 37.17 (4.18) | 1.54 (0.13) |
Note. Mean (Standard Deviation) reported. BMI = Body Mass Index.
represents number of participants with BMI measure.
Circumference measured in inches, reported in centimeters.
Neck Circumference.
Males had significantly larger neck circumference than females, F(1,322)=844.73, p<0.001, η2=0.72. Controlling for sex, there were no differences in neck circumference associated with to SRC history, F(1,316)=0.072, p=0.789, η2=0, or associated with sport contact risk group, F(1,321)=3.03, p=0.083, η2=0.009. Figure 1 depicts neck circumferences of individual athletes by sport and SRC history. Preliminary analyses of athletes who did (n=13) versus did not (n=311) experience a subsequent SRC during college also were not significant when looking at neck circumference, F(1,322)=1.42, p=0.235, η2=0.004.
Figure 1.
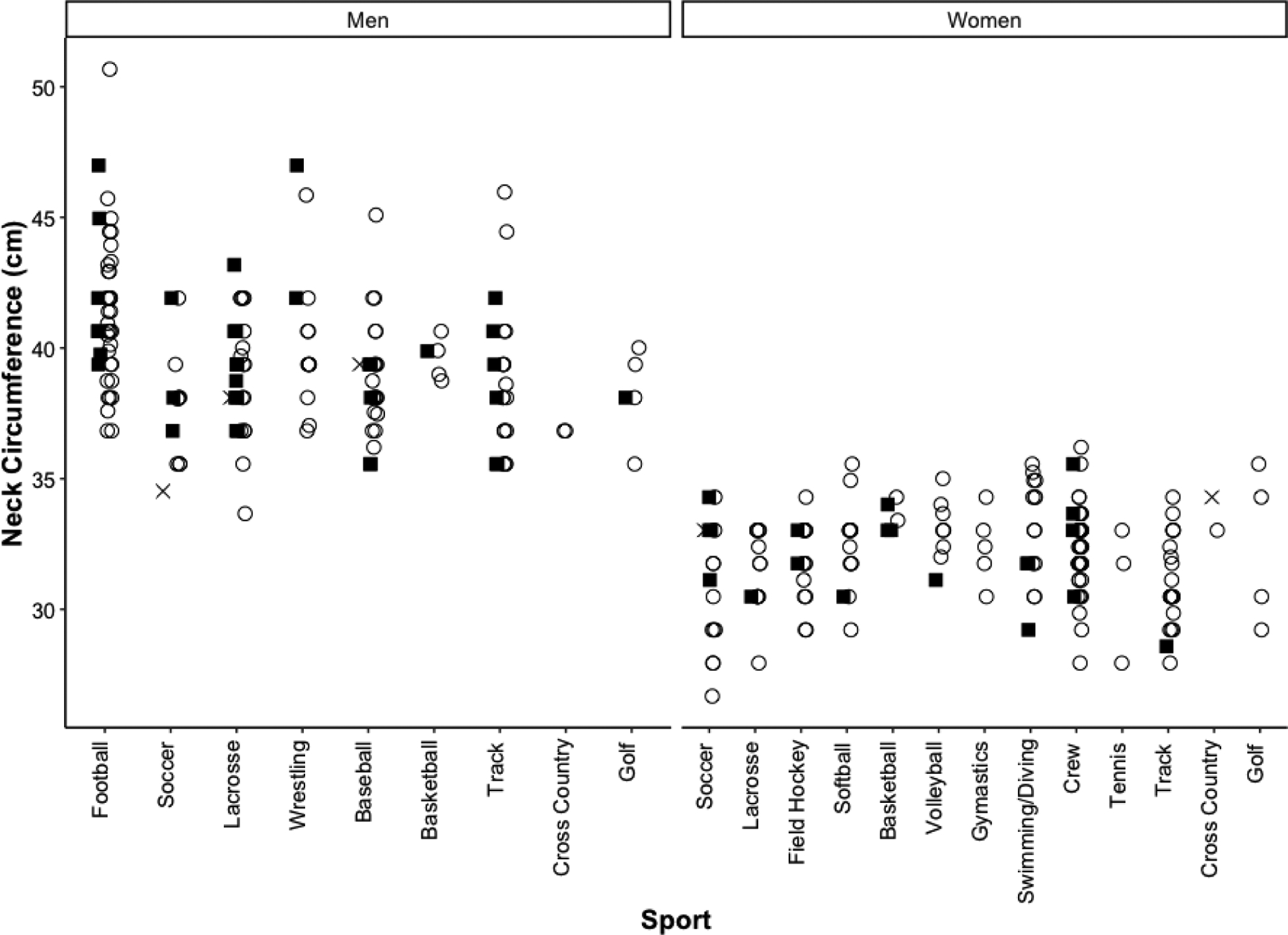
Neck circumference in centimeters (measured in inches) plotted for male and female athletes with a history of SRC (solid black box) and without a history of SRC (open circle) for each collegiate sport; missing SRC data are indicated by an x.
Proportional Neck Circumference.
Males had a significantly larger proportional neck circumference than females, F(1,304)=34.62, p<0.001, η2=0.102. Controlling for sex, proportional neck circumference did not significantly differ between athletes with versus without a history of SRC, F(1,298)= 0.01, p=0.909, η2=0.000. However, differences between high and low contact risk athletes were significant, F(1,303)=8.64, p=0.004, η2=0.028. Post-hoc analyses revealed that this was due to female high-risk sport athletes having smaller proportional neck circumferences than female low-risk sport athletes, F(1,161)=6.83, p=0.01, η2=0.041. There were no differences in high- and low-risk male athletes F(1,141)=2.12, p=0.139, η2=0.015. Figure 2 depicts proportional neck circumferences of individual athletes by sport and SRC history. Preliminary analyses of athletes who did (n=13) versus did not (n=293) experience a subsequent SRC during college were not significant, F(1,304)=0.26, p=0.613, η2=0.001.
Figure 2.
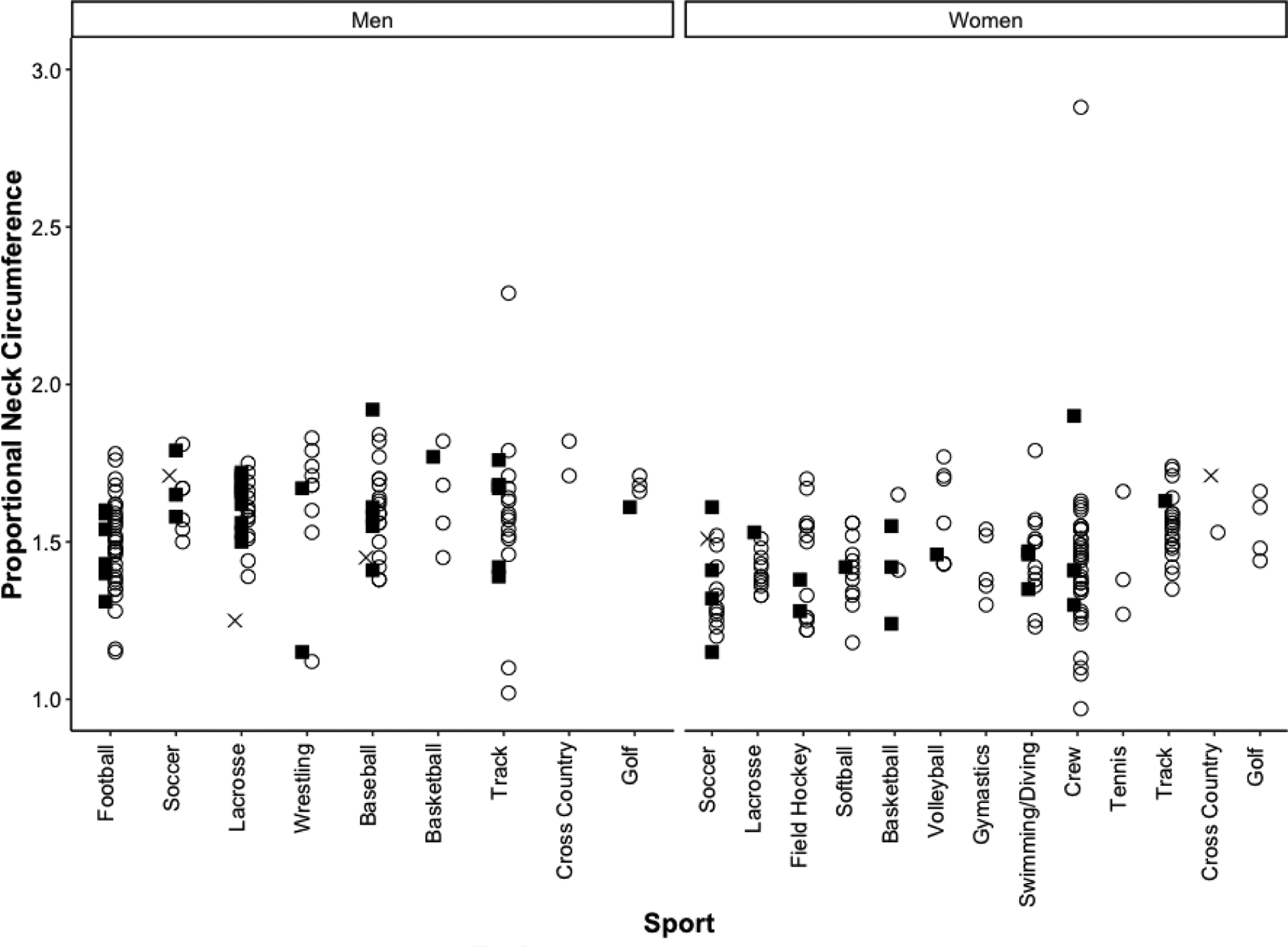
Proportional neck circumference is plotted for male and female athletes with a history of SRC (solid black box) and without a history of SRC (open circle) for each collegiate sport; missing SRC data are indicated by an x.
Discussion
This study collected neck circumference from a large sample of incoming college athletes and assessed its relationship to sex, contact risk, and self-reported prior and subsequent concussions. Consistent with past work and our hypothesis, male athletes had significantly larger neck circumferences than female athletes. However, there were no significant differences in relation to contact risk and history of SRC. A prior study of neck circumference in high school soccer, lacrosse, and basketball athletes likewise found no significant differences related to concussion when male and female athletes were analyzed separately (Collins et al., 2014). The present study extends those results to athletes from a full range of sports who had been invited to participate in a NCAA Division I collegiate program.
When neck circumference was considered in relation to overall body mass, male athletes still showed a higher proportional neck circumference than female athletes. In other words, males had a greater neck circumference per unit of body mass (i.e., proportionally larger necks) than females. Proportional neck circumference was not related to history of SRC or subsequent SRC. This is in contrast to a prior study that showed proportionally larger necks among male, but not female, athletes who subsequently experienced a concussion (Collins et al., 2014). The reason for these differences may stem from the small number of SRCs diagnosed in this sample subsequent to neck measurement or the present sample’s inclusion of nine male sports teams.
We observed a small effect difference that suggested that female athletes in low- versus high-contact risk sports had higher proportional neck circumferences. We initially posited the opposite – that the strength training protocols of sports with high-contact risk contact would promote neck strength that would be measurable as differences in neck circumference. However, it may be that athletes from sports that have greater upper body involvement, which may include low-contact risk sports such as crew as well as high-contact risk sports such as gymnastics, have larger proportional neck circumferences. There were two athletes with large proportional neck circumference, possibly due to a low BMI; however, these scores did not influence the results.
Athletics is actively seeking objective biomarkers of SRC risk; neck circumference is quick and simple to measure, and thus an attractive proxy of neck strength (Streifer et al., 2019). Past work suggests that a stronger neck can buffer the brain against the biomechanical forces elicited by an acute head impact (Caccese, Buckley, Tierney, Arbogast, et al., 2018; Collins et al., 2014; Tierney et al., 2008); however, this study suggests that neck circumference is not sufficient to determine SRC risk, likely due to the complexity of the relationship between neck circumference, musculature, and function. This study must be considered in light of the limited number of past and subsequent concussions, the use of self-report and chart review, and limited information about the timing and frequency of prior concussions. Neck circumference can change across adolescence and emerging adulthood (Katz et al., 2014); thus, timing of prior SRCs and mechanisms of injury may be important. All NCAA Division I sports at this university were included to ensure generalizability of our findings; however, some teams included only a few athletes and even within teams, physical requirements of different play positions may influence upper body strength, and possibly neck circumference. Nonetheless, these results point to a need for additional studies to determine whether neck circumference is sufficient as a proxy for neck strength and whether it can help predict who is at risk for SRC.
Acknowledgements
Financial support was provided to J.F.B. by the National Institutes of Health (K02AA025123) and New Jersey Commission on Brain Injury Research (NJCBIR13IRG0280). Financial support was provided to C.E. through Rutgers University School of Health Professions.
Footnotes
Publisher's Disclaimer: This Author Accepted Manuscript is a PDF file of an unedited peer-reviewed manuscript that has been accepted for publication but has not been copyedited or corrected. The official version of record that is published in the journal is kept up to date and so may therefore differ from this version.
Compliance with Ethical Standards: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee (Rutgers ArtSci IRB approval # 12–607M) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants.
Informed consent: Informed consent was obtained from all individual participants included in the study.
Conflict of Interest: The authors declare that they have no conflict of interest.
Ethical Approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee Rutgers ArtSci IRB approval # 12–607 and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
References
- Bretzin AC, Mansell JL, Tierney RT, & McDevitt JK (2017). Sex differences in anthropometrics and heading kinematics among Division I soccer athletes. Sports Health, 9(2), 168–173. doi: 10.1177/1941738116678615 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Caccese JB, Buckley TA, Tierney RT, Arbogast KB, Rose WC, Glutting JJ, & Kaminski TW (2018). Head and neck size and neck strength predict linear and rotational acceleration during purposeful soccer heading. Sports Biomechanics, 17(4), 462–476. doi: 10.1080/14763141.2017.1360385 [DOI] [PubMed] [Google Scholar]
- Caccese JB, Buckley TA, Tierney RT, Rose WC, Glutting JJ, & Kaminski TW (2018). Sex and age differences in head acceleration during purposeful soccer heading. Research in Sports Medicine, 26(1), 64–74. doi: 10.1080/15438627.2017.1393756 [DOI] [PubMed] [Google Scholar]
- Collins CL, Fletcher EN, Fields SK, Kluchurosky L, Rohrkemper MK, Comstock RD, & Cantu RC (2014). Neck strength: A protective factor reducing risk for concussion in high school sports. Journal of Primary Prevention, 35(5), 309–319. doi: 10.1007/s10935-014-0355-2 [DOI] [PubMed] [Google Scholar]
- Covassin T, Elbin RJ, Harris W, Parker T, & Kontos A (2012). The role of age and sex in symptoms, neurocognitive performance, and postural stability in athletes after concussion. American Journal of Sports Medicine, 40(6), 1303–1312. doi: 10.1177/0363546512444554 [DOI] [PubMed] [Google Scholar]
- Covassin T, Moran R, & Elbin RJ (2016). Sex differences in reported concussion injury rates and time loss from participation: An update of the National Collegiate Athletic Association Injury Surveillance Program from 2004–2005 through 2008–2009. Journal of Athletic Training, 51(3), 189–194. doi: 10.4085/1062-6050-51.3.05 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guskiewicz KM, & Mihalik JP (2011). Biomechanics of sport concussion: Quest for the elusive injury threshold. Exercise and Sport Science Reviews, 39(1), 4–11. doi: 10.1097/JES.0b013e318201f53e [DOI] [PubMed] [Google Scholar]
- Iverson GL, Gardner AJ, Terry DP, Ponsford JL, Sills AK, Broshek DK, & Solomon GS (2017). Predictors of clinical recovery from concussion: A systematic review. British Journal of Sports Medicine, 51(12), 941–948. doi: 10.1136/bjsports-2017-097729 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Katz SL, Vaccani JP, Clarke J, Hoey L, Colley RC, & Barrowman NJ (2014). Creation of a reference dataset of neck sizes in children: Standardizing a potential new tool for prediction of obesity-associated diseases? BMC Pediatrics, 14, 159. doi: 10.1186/1471-2431-14-159 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rice SG, American Academy of Pediatrics Council on Sports, M., & Fitness. (2008). Medical conditions affecting sports participation. Pediatrics, 121(4), 841–848. doi: 10.1542/peds.2008-0080 [DOI] [PubMed] [Google Scholar]
- Sandel NK, Schatz P, Goldberg KB, & Lazar M (2017). Sex-based differences in cognitive deficits and symptom reporting among acutely concussed adolescent lacrosse and soccer players. American Journal of Sports Medicine, 45(4), 937–944. doi: 10.1177/0363546516677246 [DOI] [PubMed] [Google Scholar]
- Streifer M, Brown AM, Porfido T, Anderson EZ, Buckman J, & Esopenko C (2019). The potential role of the cervical spine in sports-related concussion: Clinical perspectives and considerations for risk reduction. Journal of Orthopaedic and Sports Physical Therapy, 49(3), 202–208. doi: 10.2519/jospt.2019.8582 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tator CH, Davis HS, Dufort PA, Tartaglia MC, Davis KD, Ebraheem A, & Hiploylee C (2016). Postconcussion syndrome: demographics and predictors in 221 patients. Journal of Neurosurgery, 125(5), 1206–12016. doi: 10.3171/2015.6.JNS15664 [DOI] [PubMed] [Google Scholar]
- Tierney RT, Higgins M, Caswell SV, Brady J, McHardy K, Driban JB, & Darvish K (2008). Sex differences in head acceleration during heading while wearing soccer headgear. Journal of Athletic Training, 43(6), 578–584. doi: 10.4085/1062-6050-43.6.578 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tierney RT, Sitler MR, Swanik CB, Swanik KA, Higgins M, & Torg J (2005). Gender differences in head-neck segment dynamic stabilization during head acceleration. Medicine and Science in Sports and Exercise, 37(2), 272–279. doi: 10.1249/01.MSS.0000152734.47516.AA [DOI] [PubMed] [Google Scholar]