

Abstract
Sexual minority (lesbian, gay, bisexual, and same-sex attracted) youth and adults report elevated rates of excessive alcohol abuse relative to their heterosexual peers; these differences are strongest for sexual minority girls and women. Although preliminary evidence suggests that unsupportive parenting and maladaptive parent-child relationship qualities are associated with concurrent substance use among sexual minority youth, questions remain about the long-term implications of these early familial experiences on sexual minority drinking behaviors. Nationally-representative prospective data (n = 14,800; 53.1% female; Wave 1 Mean age = 15.61; Wave 4 Mean age = 28.51) were used to test the longitudinal association between parent-child relationships and parental autonomy granting between the ages of 13-18, and sexual-orientation-related disparities in abuse during adulthood. The findings showed that adolescent same-sex attraction was associated with alcohol abuse during adulthood for sexual minority women and that deficits in parent-child relationship quality statistically mediated this association. No sexual orientation differences in alcohol abuse were found among men. The findings suggest that the quality of relationships with parents in early adolescence has long-lasting impact on sexual minority women’s vulnerability for alcohol abuse. Early interventions that bolster supportive parent-child relationship qualities may have enduring consequences for sexual minority women’s alcohol use across the life course.
Keywords: sexual minority youth, LGB youth, parenting, parental support, alcohol abuse, longitudinal
Introduction
Sexual minority (lesbian, gay, bisexual, and same-sex attracted) youth and adults have consistently higher rates of alcohol use, abuse, and dependence when compared to their heterosexual counterparts (Marshal et al., 2008; McCabe et al., 2009), and these disparities are typically wider for sexual minority girls (Marshal et al., 2008). These disparities are often attributed to unique stressors that sexual minority people experience such stigma, discrimination, and rejection due to their marginalized sexual identities (Meyer, 2003). General population-based studies demonstrate the association between, parent-child relationship quality, parental autonomy granting, and alcohol-related behaviors during the transition to adulthood (Ohannessian, Flannery, Simpson & Russell, 2016). At the same time, studies document that sexual minority youth report a lack of familial support and acceptance relative to their heterosexual peers, particularly sexual minority girls (Fish & Russell, 2018). Much less is known, however, about the long-term health implications of strained parental relationships for sexual minorities as they age into adulthood. As scholars address this scarcity in research, developmental perspectives of sexual minority health are necessary to help identify the timing and focus of prevention and intervention strategies. Motivated by this gap in the literature and the compelling public health concern therein, the current study assessed whether youth reports of same-sex attraction were related to alcohol abuse during adulthood and if parent-child relationship quality and autonomy granting help to explain these disparities across the transition to adulthood using national representative longitudinal panel data.
Parenting, Parent-child Relationships, and Trajectories of Alcohol Use
Risk-taking tends to increase over the course of adolescence, including increased alcohol and other substance use (Steinberg, 2007). Family science research on adolescent risk behavior indicates that family dynamics have an appreciable influence on these behaviors, and indicates that specific qualities of the parent-child relationship may have particular salience. For example, relationship dynamics that characterize the parent-adolescent bond or connection – such as attachment security or perceived familial support – are protective factors against maladaptive outcomes across adolescence and through the transition to adulthood (Dixon, Graber, & Brooks-Gunn, 2008).
Developmental theories describe individuation processes as a central developmental task of adolescence, whereby adolescents – informed by connections to their families and communities – strive to build a sense of self apart from their parents (Steinberg, 2007). During this period, parents’ active pursuit of knowledge about their child’s behaviors to identify and intervene against perceived inappropriate or risky behaviors decreases, whereas autonomy granting practices increase (Abar et al. 2015; Russell & Gordon, 2017). As this process unfolds, adolescents independently encounter a complex social landscape, one that expands to include more information about socially accepted behavior and the attitudes that shape individuals’ choices as they seek a sense of belonging—including whether and to what extent youth engage in risk behavior like substance use (Rogers & McKinney, 2019). In particular, supportive parent-child relationship qualities that convey information about closeness and approval are associated with fewer risks (Kerr, Stattin & Burk, 2010; Padilla-Walker, & Son, 2019). Adolescents are more likely to share details of their lives with parents with whom they shared a supportive bond characterized by open communication.
Supportive parenting that is warm and responsive seems to play a mechanistic role in buffering youth against risk, perhaps because it fosters spontaneous open communication during interactions that may convey encouragement to youth about their competence as communicators and decision makers. Thus, the extent to which adolescents should be granted freedom to make their own choices with regards to friends, unscheduled free time, and risk-taking should not be uncoupled from other supportive parenting behaviors that scaffold decision making skills needed for adolescents’ ability to assess risk (Best & Miller, 2010) and convey parents’ support for and affection towards their adolescent thus reinforcing or strengthening a sense of positive connection between parent and child.
Parenting that scaffolds adolescents’ independence across the transition to adulthood reflects a degree of sensitivity and developmental awareness characterize a supportive parenting approach (Baumrind, 2013). Despite mixed findings regarding the association between adolescent alcohol use outcomes and a parenting style that balances controlling and demanding with warm and nurturing qualities (Koning et al. 2012), there is evidence that particular practices common to this authoritative style may be more consistent predictors of lower adolescent alcohol use (Minaie Hui, Leung, Toumbourou, & King, 2015). A supportive, warm, cohesive relationship between parent and child including reports of perceived closeness and nurturance is associated with adaptive psychosocial development including lower levels of internalized adolescent distress, positive parent-child relationships, and lower rates of substance use and delinquency (Fletcher, Steinberg, & Williams-Wheeler, 2004). Supportive parenting is also associated with parental autonomy granting that affords youth significant opportunities to develop self-efficacy and decision-making skills, thus promoting adaptive outcomes over time including lower alcohol use (Patock-Peckham & Morgan-Lopez, 2009). The extant literature on the protective influence of autonomy granting during adolescence is nuanced; some studies report that the greatest benefit to youth risk outcomes is only seen when autonomy granting is coupled with other features of authoritative parenting (e.g., responsivity, warmth, and affection; Lanza et al., 2013).
Sexual Minority Youth, Parent-Child Relationships, and Alcohol Use
Relying on the minority stress model (Meyer, 2003), research often attributes sexual minority youth’s disproportioned burden of health problems to the unique stressors they experience (Goldbach & Gibbs, 2017). Much less is known about how parent-child relationship quality and parenting practices contribute to alcohol-related behavior during adolescence or the transition to adulthood for sexual minority youth. Research consistently documents elevated alcohol use among sexual minority youth (Marshal et al., 2008; Ploderl & Tremblay, 2015) and some research has linked these higher levels of alcohol use to unsupportive social relationships (Coulter et al., 2019). Sexual minority youth are no different from their heterosexual peers in their need for supportive parenting to promote adaptive outcomes, yet sexual minority young people are more likely to report strained relationships with parents compared to their heterosexual counterparts (Fish & Russell, 2018; Watson, Barnett, & Russell, 2016). Although studies have linked a lack of parental support to negative outcomes (Needham & Austin, 2010; Ryan, Huebner, Diaz, & Sanchez, 2009), relatively few studies have attempted to test these associations over time and across different developmental periods of life (i.e., adolescent through adulthood).
An exception addresses the gap in this scholarship: A recent study estimated profiles of both familial and non-familial warmth during childhood and adolescence and assessed whether these support profiles were related to elevated risk for heavy alcohol use and alcohol us disorder during young adulthood (ages 18-25; Coulter et al., 2019). Their results showed that sexual minority women, but not sexual minority men, were more likely to be members of classes characterized by low or moderate support relative to heterosexual women and men, respectively. Importantly, these support profiles, which include characteristics of parental support, explained in part sexual orientation differences in young adult alcohol abuse for women. The findings by Coulter and colleagues hint at how early experiences of support, or lack thereof, among sexual minority adolescence may lead to elevated risk for alcohol abuse shortly thereafter.
Finally, although studies indicate that sexual minority youth report more compromised relationships with parents, there has been a dearth of research investigating how other prominent and developmentally-specific parent-child relationship dynamics, such as autonomy granting may differ for sexual minority youth. For example, if parents sense or know about their child’s same-sex sexuality and are unsupportive, they may restrict autonomy by limiting exposure to sexual minority peers or settings. Emerging research focused on parental monitoring show that greater parental monitoring among young men who have sex with men is associated with less alcohol use (Mustanski, Swann, Newcomb, & Prachand, 2017). Yet, studies that compare heterosexual and sexual minority girls suggest that parental monitoring does not curb substance use among sexual minority girls in the same what it does for heterosexual girls (Montano, McCauley, Miller, Chisolm & Marshal, 2017).
Current Study
The current study aims to extend and integrate the aforementioned literatures by testing how youth same-sex attraction is associated with parenting in the form of parent-child relationship quality and autonomy granting, and whether these processes may be associated with alcohol abuse during adulthood. Specifically, data are from the National Longitudinal Study of Adolescent to Adult Health (Add Health) – the largest and longest running nationally-representative prospective panel study to include measures of sexual minority status – to test whether the association between adolescent same-sex attraction and adult alcohol abuse is mediated by adolescent reports of parent-child relationship quality and parental autonomy granting. It was hypothesized that youth same-sex attraction would be related to later alcohol abuse (Hypothesis 1). It was also anticipated that same-sex attraction would show lower rates of parental-child relationship quality and less parental autonomy granting than their exclusively other-sex attracted peers during adolescence, and that these differences in parenting-child processes would mediate the relationship between adolescent same-sex attraction and adult alcohol abuse (Hypothesis 2). All analytic models were sex-stratified given (1) a robust body of literature which documents sex differences in sexual-orientation-related alcohol abuse disparities (Hughes et al., 2016; Marshal et al., 2008) and (2) a growing set of studies that document sex differences in sexual minority youth reports of parental support (Fish & Russell, 2018; Needham & Austin, 2010).
Method
Data Source and Sample
Started in 1994, Add Health (Harris, 2009) is one of the most comprehensive, prospective studies following youth from adolescence into adulthood. The core sample – which was selected from a larger school-based survey of 80 high schools that represented the US population – included 20,745 7-12th graders and their parents who were interviewed at baseline (Wave 1) in 1994-1995. One year later, Wave II included 14,738 of the original participants. Wave III occurred 5-6 years later, when participants were young adults (ages 18-24; n = 15,197 from Wave I) and Wave IV was conducted 7-8 years after Wave III when participants were approximately ages 24 to 32 (2007-2008) and included 15,701 of the original participants. The current study included participants who were assigned a valid weight and participated in Waves 1 and 4 (n = 14,800; n = 7,864 girls/women and n = 6,936 boys/men). Demographic characteristics for the current sample are presented in Table 1. This secondary data analysis was approved by the University of Texas and University of Maryland Institutional Review Board.
Table 1.
Sample Characteristics
| Full Sample | Males | Females | ||||||
|---|---|---|---|---|---|---|---|---|
| n | %w | n | %w | %m | n | %w | %m | |
| DSM IV alcohol abuse (W4) | 0.03 | 0.03 | ||||||
| No | 11,093 | 72.69 | 6,296 | 77.96 | 4,797 | 67.57 | ||
| Yes | 3,701 | 27.31 | 1,568 | 22.04 | 2,133 | 32.43 | ||
| Same-sex attraction (W1) | 0.81 | 0.79 | ||||||
| No SSA | 13,792 | 93.62 | 7,386 | 94.67 | 6406 | 92.6 | ||
| Any SSA | 887 | 6.38 | 416 | 5.33 | 471 | 7.4 | ||
| Same-sex attraction (W2) | 25.42 | 26.31 | ||||||
| No SSA | 10,484 | 94.48 | 5606 | 95.57 | 4878 | 95.39 | ||
| Any SSA | 509 | 4.52 | 279 | 4.43 | 230 | 4.61 | ||
| Same-sex attraction (W3) | 15.69 | 19.46 | ||||||
| No SSA | 11,065 | 90.65 | 5801 | 86.97 | 5264 | 94.44 | ||
| Any SSA | 1,158 | 9.35 | 839 | 13.03 | 319 | 5.56 | ||
| Same-sex attraction (W4) | 0.34 | 0.25 | ||||||
| No SSA | 13,718 | 93.17 | 7,120 | 90.43 | 6598 | 95.82 | ||
| Any SSA | 1,036 | 6.83 | 719 | 9.57 | 317 | 4.18 | ||
| LGB Identity (W4) | 0.89 | 0.81 | ||||||
| No | 14,119 | 96.47 | 7,471 | 95.83 | 6,648 | 97.1 | ||
| Yes | 553 | 3.53 | 325 | 4.17 | 228 | 2.9 | ||
| Race/ethnicity (W1) | 0.09 | 0.04 | ||||||
| White | 8,119 | 67.33 | 4,266 | 67.37 | 3,853 | 67.28 | ||
| Black | 3,154 | 15.82 | 1,790 | 16.12 | 1,364 | 15.53 | ||
| Latino | 2,213 | 11.29 | 1,151 | 11.25 | 1,062 | 11.34 | ||
| Other | 1,302 | 5.56 | 652 | 5.26 | 650 | 5.85 | ||
| Education (W4) | 0.03 | 0.03 | ||||||
| < High school | 1,142 | 9.23 | 488 | 7.77 | 654 | 10.64 | ||
| High school | 2,396 | 17.94 | 1,070 | 14.38 | 1,326 | 21.39 | ||
| Some college | 6,520 | 42.89 | 3,503 | 44.44 | 3,017 | 41.39 | ||
| ≥ College | 4,736 | 29.94 | 2,803 | 33.4 | 1,933 | 26.58 | ||
| Family structure (W1) | 1.87 | 1.99 | ||||||
| Biological, two-parent | 8,135 | 56.74 | 4,225 | 56.3 | 3,910 | 57.17 | ||
| Single parent | 3,807 | 25.29 | 2,127 | 25.93 | 1,680 | 24.66 | ||
| Step-family/Other | 2,571 | 17.97 | 1,367 | 17.77 | 1,204 | 18.18 | ||
| Receipt of public assistance (W1) | 14.59 | 13.47 | ||||||
| No | 11,618 | 90.6 | 6,082 | 89.91 | 5,536 | 91.27 | ||
| Yes | 1,098 | 9.40 | 636 | 10.09 | 462 | 8.73 | ||
| M, SD | M, SD | M, SD | ||||||
| Adolescent alcohol use (W1) | 1.44 | 2.69 | 1.25 | 2.35 | 0.75 | 1.65 | 3.01 | 1.27 |
| Age (W1) | 15.61 | 1.72 | 15.71 | 1.73 | 0.07 | 15.53 | 1.72 | 0.04 |
| Age (W4) | 28.51 | 1.76 | 28.41 | 1.75 | 0.04 | 28.62 | 1.76 | 0.07 |
| Parent-child relationship quality (W1) | 4.38 | 0.60 | 4.45 | 0.53 | 1.50 | 4.31 | 0.65 | 2.16 |
| Parent-child relationship quality (W2) | 4.27 | 0.61 | 4.33 | 0.54 | 28.01 | 4.21 | 0.67 | 27.82 |
| Parental autonomy granting (W1) | 0.73 | 0.01 | 0.73 | 0.01 | 1.50 | 0.73 | 0.01 | 2.17 |
Note. %w = weighted percentages; %m = % missing
Measures
Adult alcohol abuse (Wave 4).
The Add Health Wave 4 data file includes a constructed variable that reflects participants’ alcohol abuse and dependence. Adult alcohol abuse was assessed using an index of five items that reflect Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV) abuse symptoms (American Psychiatric Association, 2013). Alcohol abuse symptoms were measured by asking questions about functional impairment and continued use in the presence of negative consequences, such as work and relationship impairment. Response options include “never”, “1 time”, or “more than 1 time”. Participants met the criteria for each symptom if they reported that a symptom occurred “more than 1 time”. Items were summed to reflect the number of alcohol abuse symptoms and dichotomized to reflect whether the participant met the criteria for adult alcohol abuse (yes = 1, no = 0), which was one or more symptoms.
Adolescent same-sex attraction (Wave 1).
Adolescent participants were asked about their romantic attraction to both boys and girls via two questions: Have you ever had a romantic attraction to a female?” and “Have you ever had a romantic attraction to a male?” Responses were yes = 1 and no = 0. By referencing participants’ own sex, items were recoded into a single-item that reflected same-sex attraction (yes = 1 and no = 0).
Parent-child relationship quality (Wave 1 and 2).
Parent-child relationship quality was measured using ten items that ask youth to report on mothers/mother-like figures (5 items) and fathers/father-like figures (5 items). These items have been previously used, and show adequate reliability (Driscoll, Russell, & Crockett, 2008; Ream & Savin-Williams, 2005; Watson et al., 2016; Wave 1 α = .873, Wave 2 α =.858). In the case where mother or father did not reside in the home, these items assess “mother” and “father” like figures (e.g., stepparents, grandparents, uncles, aunts, foster parents, etc.) that reside with and are determined by the adolescent. Items include: “How close do you feel to your mother/father” (not at all = 1, very much = 5); “How much do you think s/he cares about you?” (not at all = 1, very much = 5); and “Overall, you are satisfied with your relationship with your mother/father?” (strongly disagree = 1, strongly agree = 5). Items were summed and averaged so higher scores reflect closer parental relationships and account for the presence of one or two parents. Parent-child relationship quality indicators are not available in Wave 4.
Parent-child autonomy granting (Wave 1 and 2).
Parent-child autonomy granting was assessed using seven yes/no items that ask youth to reflect on whether their parents allow them to make decisions about curfew, friends, television, and bedtime. Items asked youth, “Do your parents let you make your own decisions about…”, “the time you must be home on weekend nights?” and “the people you hang around with?”. Items were summed and averaged to reflect the degree to which parents scaffold child autonomy. Given a lack of literature on this particular scale in the Add Health data, a confirmatory factor analysis was conducted; the results of which indicated good model fit to the data with a single factor structure (X2=3289.94, df=15, p <.001, CFI=.915, RMSEA=.049, 95% CI: .044, .053, SRMR=.040; see Kline, 2016).
Time invariant covariates.
Based on a wealth literature highlighting sociodemographic differences in alcohol abuse (Delker et al., 2016). Models adjusted effects for endogenous variables across waves to include several covariates measured at Wave 1: race/ethnicity (White [reference], Black/African American, Latinx, and Other), family structure (two-parent [reference], single-parent, and stepfamily/other), receipt of public assistance (via parental report: yes = 1, no = 0) , and adolescent reported alcohol use at Wave 1, which was quantified as an average of three items that include frequency of alcohol use, average quantity when drinking, and frequency of heavy episodic drinking (see Fish, Pollitt, Schulenberg & Russell, 2018). Models also adjust for several Wave 4 covariates of alcohol abuse including same-sex attraction (yes = 1 and no = 0), education (high school [reference], less than high school, college, or professional degree), and age, in years. Models also adjusted for Wave 4 LGB identity (LGB = 1, heterosexual = 0), given that sexual minority identity is uniquely associated with alcohol abuse (via heightened discrimination) above and beyond same-sex attracted heterosexuals (see Fish & Krueger, 2020). All categorical covariates were dummy coded.
Time-varying covariates.
Adolescence and young adulthood are developmental periods characterized by the awareness and development of same-sex attraction (Mustanski, Kuper, & Green, 2014). Studies often demonstrate the developmental nature of same-sex attraction and thus, same-sex attraction was modeled as a time varying covariate to adjust for the influence of fluid same-sex attraction on substance use (see Fish & Pasley 2015). Similar to Wave 1 reports, participants indicated whether they were attracted to men and women at all waves. Items were recoded to reflect same-sex attraction as yes = 1 and no = 0.
Analytic Approach
Model 1 tested whether Wave 2 reports of parent-child relationship quality and parental autonomy granting mediated the association between Wave 1 same-sex attraction and Wave 4 alcohol abuse. As a follow-up, a developmental cascade model (Model 2) was estimated to assess whether Wave 1 same-sex attraction is associated with concurrent deficits in parental relationship quality and differential parental autonomy granting play a role in the mediational pathway between Wave 1 same-sex attraction and adult alcohol abuse.
All data management and preliminary analyses were conducted in Stata 15.1 (StataCorp, 2017). Longitudinal associations and mediating effects for Model 1 and 2 were estimated using path analysis in Mplus 7.4 (Muthén & Muthén, 1998-2017). Add Health’s longitudinal sampling weights were applied to adjust for non-response across waves (Chen & Chantala, 2014). Missing data (see Table 1) were accounted for by using full-information likelihood (FIML) estimation procedures in Mplus (see Enders, 2010). All models were run using maximum likelihood estimation with robust standard errors to assist in the estimation of indirect effects and to apply FIML procedures to account for missing data. For this reason, traditional fit indices such as chi-square test of model fit, TLI, and CLI and statistically test differences between nested and alternative models were unavailable. The use of FIML also prevented the estimations of bootstrapped indirect effects.1
Results
There were no significant associations between adolescent same-sex attraction and adult alcohol abuse among boys/men in the sample (see Supplemental Table 1). Therefore results are limited to girls/women. Initial main effects (i.e., non-mediational) models among women showed that there was a significant association between adolescent-same sex attraction and DSM-IV alcohol abuse after accounting for all covariates aOR = 2.11, p < .001 (Hypothesis 1; see Supplemental Table 1).
Among women, results from Model 1 showed that same-sex attraction at Wave 1 was inversely associated with Wave 2 parent-child relationship quality (β = −.05, p = .002) and that Wave 2 parent-child relationship quality was inversely related to alcohol abuse at Wave 4 (aOR = 0.80, p = .001). Wave 1 same-sex attraction was unrelated to Wave 2 parental autonomy granting (β = −.02, p = .313), which was also unrelated to Wave 4 alcohol abuse (aOR = 1.54, p = .112). Testing of indirect effects showed a small but statistical mediating effect between adolescent same-sex attraction and alcohol abuse in adulthood via youth-reported parent-child relationship quality b= .032, se = .014, 95% CI (.005, .059), p = .013 (Hypothesis 2; see Figure 1; Table 4).
Figure 1: Path analysis models testing the mediating influence of parent-child relationship quality and parental-child autonomy granting in the association between adolescent same-sex attraction and adult alcohol abuse among females.
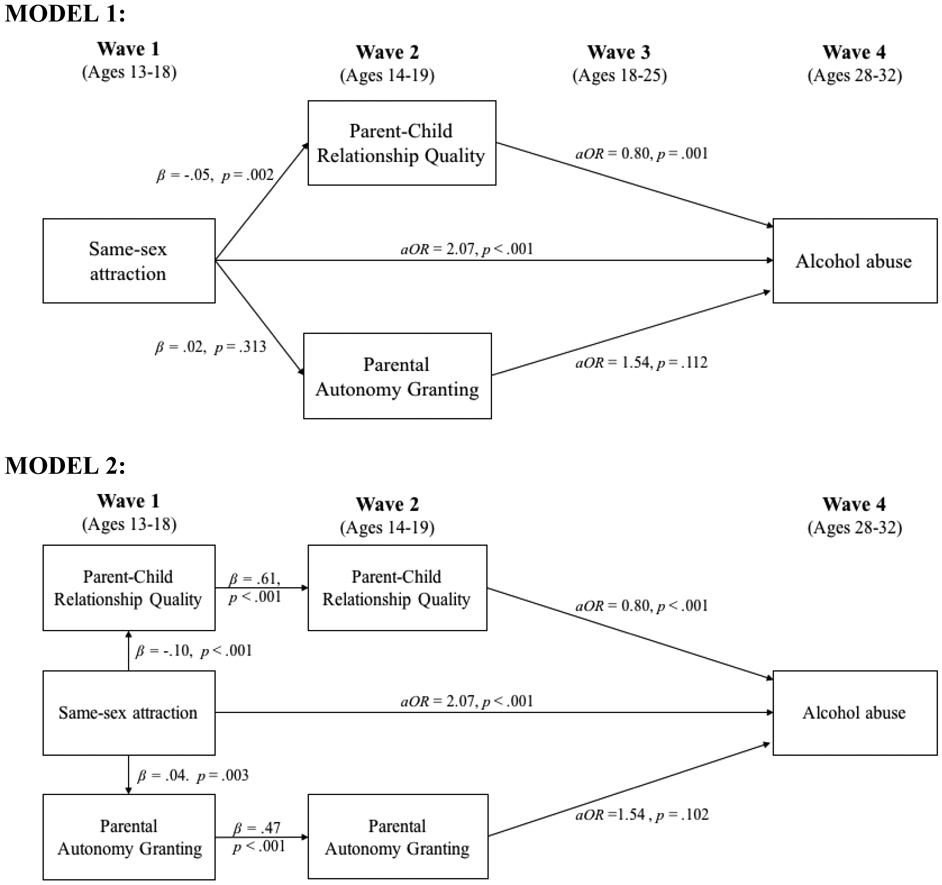
Parent-child relationship quality and parental autonomy granting were regressed on Wave 1 covariates and alcohol abuse was regressed on all Wave 1 and 4 covariates (not shown). Models were estimated with maximum likelihood estimation with robust standard errors to accurately test indirect effects and to account for missing data. For this reason, it was not possible to provide traditional fit indices such as chi-square test of model fit, TLI, CLI, RMSEA, and SRMR, or statistically test differences between nested and alternative models. The Mplus bootstrap option also does not work with this estimator nor the integration statement that are required to estimate indirect effects with weighted survey data. It was also therefore unable to provide bootstrapped confidence intervals for indirect effects.
Table 4.
Total, indirect, and direct effects of adolescent same-sex attraction on adult alcohol abuse via adolescent and young adult parent-child relationship quality and parental autonomy granting
| b | se | 95% CI | p-value | |
|---|---|---|---|---|
| MODEL 1: | ||||
| Total | 0.774 | 0.162 | (.460, 1.09) | <.001 |
| Total indirect | 0.040 | 0.018 | (.005, .074) | .022 |
| Indirect (via relationship quality) | 0.032 | 0.014 | (.005, .059) | .019 |
| Indirect (via autonomy granting) | 0.007 | 0.008 | (−.008, .023) | .355 |
| Direct | 0.734 | 0.160 | (.420, 1.049) | <.001 |
| MODEL 2: | ||||
| Total | 0.774 | 0.165 | (.450, 1.10) | <.001 |
| Total indirect | 0.048 | 0.017 | (.015, .081) | .004 |
| Indirect (via relationship quality) | 0.039 | 0.014 | (.012, .067) | .004 |
| Indirect (via autonomy granting) | 0.009 | 0.006 | (−.003, .020) | .154 |
| Direct | 0.726 | 0.161 | (.410, 1.04) | <.001 |
Results from Model 2 (Table 3) showed that adolescent same-sex attraction at Wave 1 was negatively associated with concurrent parent-child relationship quality (β = −.10, p < .001), which was positively associated with Wave 2 parent-child relationship quality (β = .61, p < .001). Wave 2 parent-child relationship quality was negatively associated with Wave 4 alcohol abuse (aOR = .80, p < .001). Wave 1 same-sex attraction was positively associated with Wave 1 parental autonomy granting (β = .04, p = .003), which was strongly associated with Wave 2 parental autonomy granting (β = .47, p < .001). Wave 2 parental autonomy granting, however, was not statically related to adult alcohol abuse (aOR = 1.54, p = .102). The testing of indirect effects support a cascading mediational effect, whereby adolescent same-sex attraction and alcohol abuse in adulthood are sequentially mediated by parent-child relationship quality in Wave 1 and 2 respectively (see Figure 1, Table 3), b = .039, se = .014, 95% CI (.012, .067), p = .004. There was no evidence of indirect effect through parental autonomy granting.
Table 3.
Model 2: Parent-child relationship quality cascade mediation between adolescent same-sex attraction and adult alcohol abuse among Females.
| b | se | OR/B | 95% CI | p-value | |
|---|---|---|---|---|---|
| Wave 4 DSM-IV alcohol abuse regressed on: | |||||
| Same-sex attraction (W1) | 0.73 | 0.16 | 2.07 | (1.51, 2.83) | < .001 |
| Parent-child relationship quality (W2) | −0.22 | 0.06 | 0.80 | (0.71, 0.90) | < .001 |
| Parental autonomy granting (W2) | 0.43 | 0.26 | 1.54 | (0.92, 2.58) | .102 |
| Race/ethnicity | |||||
| White [ref] | |||||
| Black/African American | −1.19 | 0.11 | 0.31 | (0.24, 0.38) | < .001 |
| Latinx | −0.50 | 0.17 | 0.61 | (0.44, 0.84) | .003 |
| Other | −0.43 | 0.16 | 0.65 | (0.48, 0.88) | .006 |
| Family Structure (W1) | |||||
| Two-parent [ref] | |||||
| Single-parent | 0.07 | 0.09 | 1.07 | (0.90, 1.28) | .458 |
| Step-family/other | 0.24 | 0.11 | 1.28 | (1.03, 1.59) | .029 |
| Adolescent alcohol use (W1) | 0.14 | 0.02 | 1.15 | (1.10, 1.20) | < .001 |
| Receipt of public assistance (W1) | −0.16 | 0.19 | 0.85 | (0.58, 1.25) | .418 |
| Education (W4) | |||||
| High school [ref] | |||||
| Less than high school | 0.87 | 0.25 | 2.40 | (1.48, 3.90) | < .001 |
| Some college | 1.28 | 0.25 | 3.60 | (2.21, 5.88) | < .001 |
| College or more | 1.59 | 0.26 | 4.88 | (2.95, 8.08) | < .001 |
| Age (W4) | −0.16 | 0.03 | 0.85 | (0.81, 0.90) | < .001 |
| Sexual identity (W4) | |||||
| Heterosexual [ref] | |||||
| LGB | −0.01 | 0.22 | 0.99 | (0.64, 1.54) | .969 |
| Same-sex attraction (W4) | 0.63 | 0.15 | 1.88 | (1.40, 2.53) | < .001 |
| Wave 2 Parent-Child Relationship Quality Regress on: | |||||
| Parent-child relationship quality (W1) | 0.61 | 0.02 | 0.61 | (0.57, 0.64) | < .001 |
| Same-sex attraction (W2) | −0.04 | 0.05 | −0.01 | (−0.09, 0.02) | .440 |
| Race/ethnicity | |||||
| White [ref] | |||||
| Black/African American | 0.03 | 0.01 | 0.01 | (−0.01, 0.04) | .220 |
| Latinx | 0.00 | 0.00 | 0.00 | (−0.04, 0.04) | .960 |
| Other | −0.12 | −0.04 | −0.04 | (−0.08, −0.00) | .041 |
| Family Structure (W1) | |||||
| Two-parent | |||||
| Single-parent | −0.04 | −0.03 | −0.03 | (−0.06, 0.01) | .128 |
| Step-family/other | −0.08 | −0.04 | −0.04 | (−0.07, −0.02) | .001 |
| Adolescent alcohol use (W1) | −0.01 | 0.01 | −0.03 | (−0.06, 0.01) | .117 |
| Receipt of public assistance (W1) | 0.04 | 0.04 | 0.02 | (−0.02, 0.06) | .332 |
| Wave 2 Parental Autonomy Granting Regressed on: | |||||
| Parental autonomy granting (W1) | 0.45 | 0.02 | 0.47 | (0.44, 0.51) | < .001 |
| Same-sex attraction (W2) | 0.02 | 0.01 | 0.02 | (−0.00, 0.05) | .067 |
| Race/ethnicity | |||||
| White [ref] | |||||
| Black/African American | −0.02 | 0.01 | −0.03 | (−0.07, 0.01) | .102 |
| Latinx | −0.04 | 0.01 | −0.05 | (−0.09, −0.01) | .006 |
| Other | −0.03 | 0.02 | −0.03 | (−0.07, 0.01) | .125 |
| Family Structure (W1) | |||||
| Two-parent | |||||
| Single-parent | 0.02 | 0.01 | 0.05 | (0.01, 0.08) | .014 |
| Step-family/other | 0.01 | 0.01 | 0.02 | (−0.02, 0.05) | .302 |
| Adolescent alcohol use (W1) | 0.01 | 0.00 | 0.06 | (0.02, 0.10) | .002 |
| Receipt of public assistance (W1) | −0.03 | 0.01 | −0.04 | (−0.07, −0.01) | .013 |
| Wave 1 parent-child relationship quality regressed on: | |||||
| Same-sex attraction (W1) | −0.29 | 0.06 | −0.10 | (−0.13, −0.06) | < .001 |
| Wave 1 parental autonomy granting regressed on: | |||||
| Same-sex attraction (W1) | 0.04 | 0.02 | 0.04 | (0.02, 0.07) | .003 |
Discussion
Sexual minority youth and adults – and sexual minority females in particular – are at greater risk for substance use relative to their heterosexual peers (Marshal et al, 2008; Plöderl & Tremblay, 2015). These disparities are often attributed to minority stressors that include compromised familial relationships as a result of having a sexual minority identity (Goldbach & Gibbs, 2017; Russell & Fish, 2016). Despite preliminary evidence that unsupportive parenting and strained parent-child relationships are associated with substance use among sexual minority youth (Needham & Austin, 2010; Ryan et al., 2009), questions remain about the long-term implications of these early familial experiences on sexual minority drinking behaviors (Mereish, 2020).
The findings presented here are among the first to document the enduring health consequences of compromised parent-child relationships during adolescence for sexual minority girls/women. Among sexual minority women, youth same-sex attraction was associated with reduced parent-child relationship quality, which in turn was associated with adult alcohol abuse. These findings both support and extend current literature on sexual minority health trajectories across the transition to adulthood. Similar to cross-sectional studies, the findings here show that sexual minority youth, and sexual minority girls in particular, demonstrated deficits in parent-child relationship quality (Fish & Russell, 2018; Needham & Austin, 2010). The findings presented here also corroborate work by Coulter et al. (2019): Our findings show how, for women, adolescent deficits in parent-child relationship quality help to explain, in part, sexual orientation differences in alcohol abuse in adulthood. These results add to and extend these findings by isolating parent-child relationship quality as a key mechanism of risk for alcohol abuse across the life course for sexual minority women, and assess how early awareness of same-sex attraction are temporally associated with decreased support from parents, which in turn are prospectively associated with alcohol abuse at later periods in the life course.
There were no sexual orientation differences in alcohol abuse among men. Research generally supports that sexual-orientation-related disparities in substance abuse, and excessive alcohol use and abuse in particular, are more consistent and robust for sexual minority women relative to sexual minority men (Hughes et al., 2016; Plöderl & Tremblay, 2016). These gender differences are not well understood, but have been attributed to a number of factors, including sexual minority women’s rejection of traditional gender norms, the fact that heterosexual men drink at higher rates than heterosexual women, and sexual minority women’s elevated rates of physical and sexual victimization across the life course (Hughes et al., 2016). Still, other research highlights that sexual minority men may be more susceptible to elevated rates of substance abuse outside of alcohol (e.g., cigarette use, club drugs; McCabe et al., 2009; Plöderl & Tremblay, 2015). Future research should consider how parental and familial relationships may play a unique role for risk across different substances given that there appear to be unique patterns of risk among sexual minority youth and adults on the basis of sex.
Our results provide mixed evidence for differential autonomy granting for sexual minority youth and its ability to help explain, in part, sexual orientation differences in alcohol abuse in adulthood. Our cascade model (Model 2) showed a statistical relationship between same-sex attraction and parental autonomy granting, whereby sexual minority girls reported more autonomy-granting from parents relative to their heterosexual peers in Wave 1 and this effect carried forward, but was unrelated to adult alcohol abuse. These findings are consistent with a previous study on parental monitoring, which found that sexual minority girls were less likely than heterosexual girls to report parental solicitation of knowledge about their location and activities (Montano et al., 2017). This same article also noted that sexual minority girls were less likely to share accurate information with parents. Together these findings suggest that there may be something unique about the relationship between parents and their sexual minority female children with respect to monitoring or sharing information. Although results showed no longitudinal association between autonomy-granting and alcohol abuse in adulthood, further studies should continue to explore intervening mechanisms that may link processes of autonomy-granting with health and risk behaviors later in adulthood. More generally, the results call attention to the fact that there are other relevant parent-child processes that deserve attention in the context of sexual minority youth development and health (see also Newcomb, LaSala, Bouris, Mustanski, Prado, Schrager, & Huebner, 2019). Autonomy granting is an important construct for assessing trajectories of substance use across adolescence and the transition to adulthood in the general population (Minaie Hui et al., 2015; Gordon et al., 2019) and should, alongside other familial process, be a focus of research when assessing the development and health of sexual minority young people.
Our findings with regard to parent-child relationship quality and risk for alcohol abuse among sexual minority women are consistent with minority stress theory (Meyer, 2003). Poor mental health and maladaptive coping strategies among sexual minority people, such as alcohol abuse, emanate from chronic stressors that arise in response to a stigmatized sexual orientation. Although minority stressors are often operationalized as discrete experiences of stigma such as LGB-specific instances of discrimination, bullying, and rejection, minority stress theory also emphasizes how sexual minority people may also experience elevated rates of everyday stressors, which include strained interpersonal relationships (Krueger, Fish, & Upchurch, 2020; Meyer, 2003). In the case of our study, these chronic stressors are related to deficits in parental-relationship quality. The results are consistent with previous research which highlights compromised familial relationships as a result of sexual minority status (D’Augelli et al., 2008), and adjacent research that elucidates the negative health consequences of parental rejection (Ryan et al., 2009). This study links these two processes and extends them to demonstrate how they work in concert to influence the long-term health of sexual minority women. That is, same-sex attracted girls reported lower levels of parental warmth, closeness, and caring than their other-sex attracted peers, and these difference in parental relationship quality carried forward across adolescence and were associated with elevated odds of alcohol abuse in adulthood. As such, policies, programs, and practices that address both overt forms of discrimination, but also more subtle but enduring stress are necessary to combat and address sexual orientation-related health disparities.
With regard to the practical implications of this work, our findings are largely relevant to programs and practices for sexual minority young people. Prevention and intervention programs and strategies for sexual minority youth should consider the importance of including a focus on strengthening parent-child relationships, as they appear (not surprisingly) to have long-lasting impact on the health of sexual minority adults. Even with the overwhelming agreement that parents matter for the health and wellness of youth, there is a relatively small literature on the role of family in the positive, health, and development of sexual minority young people (Newcomb et al., 2019). Parental support cannot be assumed in the context of sexual minority young people, nor can one assume that supportive parents display an absence of other behaviors that are simultaneously undermining and harmful. For example, a parent can say that they are support of a young person’s sexual identity, but undermine these statements by policing their clothing, who they hang out with, and disclosure of this identity to other family members. Family programs have shown to be effective and often times more effective that individual treatment for supporting youth and altering maladaptive or risky behavior (Brody, Chen, Kogan, Murry, & Brown, 2010; Prado et al., 2012) – but these perspectives have yet to gain significant traction in the sexual minority youth health promotion scholarship (Newcomb et al., 2019). An exception are individual therapeutic approaches: Attachment-Based Family Therapy (Diamond, Russon, & Levy, 2016) models with sexual minority young people have shown to be an effective strategy for supporting sexual minority youth mending ruptures that occur in the family system as a result of rejecting parental behaviors in reaction to adolescent same-sex attraction. In short, there is much work to be done in this area, both in the degree to which family dynamics influence sexual minority youth health, but also the strategies that bolster and repair parent-child relationships in ways that support the positive development and health of sexual minority youth.
Despite the contributions, there are several limitations to note. First, it was not possible to know whether parents were aware of youth’s same-sex attraction (i.e., if they were out) during adolescence or if youth identified as LGB given that Add Health did not include items assessing sexual identity until adulthood. Second, global measures of parenting and relationship quality provide important information, but the Add Health study does not assess sexuality-specific parenting practices. Other studies have documented cross-sectional links between parental rejection of sexual minority identities and substance use behaviors for both sexual minority males and females (Ryan et al., 2009); sexuality-specific parenting practices could make a lasting difference for sexual minority youth in ways that general measures of parenting and relationships do not. Third, the data on parenting behaviors were limited to youth reports. Future studies would benefit from using multisource data on parenting practices, and its impact on sexual minority youth substance use and wellbeing. Finally, given the analytic approach it was not possible to assess model fit, or to compare fit across our two models – this is a regrettable limitation but does not discount the gravity of our findings. With more analytic advancements for estimating model fit with complex data, future studies that are able to address these limitations will be necessary to help validate the associations documented here. Finally, Add Health participants were adolescents in the 1990s, and thus their experiences as young sexual minorities would likely differ from today’s youth. Yet despite significant social change toward legal and policy inclusion for sexual minorities, there is evidence that compromised relationships between parent and sexual minority youth are not improving over time: A recent study found a growing disparity in the perception of family connectedness and parent support among sexual minority youth compared to their heterosexual counterparts (Watson, Rose, Doull, Adjei, & Saewyc, 2019). Given the continued or even growing sexual orientation disparity in parent-adolescent relationships, our findings continue to be relevant for contemporary sexual minorities, and these associations deserve investigation among contemporary cohorts.
Conclusion
The current study aimed to understand the degree to which adolescent family processes are associated with later vulnerability for substance use among sexual minority adults. Our findings suggest that same-sex attracted adolescents experience deficits in parent-child relationship quality, and those deficits are implicated in in well-established disparities in alcohol abuse between sexual minority and heterosexual women. As the quality and quantity of data on the experiences of sexual minority youth continues to expand, it is critical for us to understand the factors that shape the health of sexual minority people. Prospective studies in particular have the capacity to not only inform the contextual factors that should be addressed, but equally importantly when they seem most salient for shaping health and wellness across the life course.
Supplementary Material
Table 2.
Model 1: Parent-child relationship mediation between adolescent same-sex attraction and DSM-IV alcohol abuse among Females
| b | se | aOR | 95% CI / se | p | |
|---|---|---|---|---|---|
| Wave 4 DSM-IV alcohol abuse regressed on: | |||||
| Same-sex attraction (W1) | 0.73 | 0.16 | 2.07 | (1.52, 2.85) | < .001 |
| Parent-child relationship quality (W1) | −0.21 | 0.06 | 0.80 | (0.72, 0.92) | .001 |
| Parental autonomy granting (W1) | 0.41 | 0.26 | 1.54 | (0.90, 2.50) | .112 |
| Race/ethnicity | |||||
| White [ref] | |||||
| Black/African American | −1.19 | 0.12 | 0.31 | (0.24, .38) | < .001 |
| Latinx | −0.51 | 0.17 | 0.61 | (0.43, .84) | .003 |
| Other | −0.43 | 0.16 | 0.65 | (0.48, .88) | .006 |
| Family Structure (W1) | |||||
| Two-parent [ref] | |||||
| Single-parent | 0.07 | 0.09 | 1.07 | (0.90, 1.29) | .408 |
| Step-family/other | 0.25 | 0.11 | 1.28 | (1.03, 1.60) | .024 |
| Adolescent alcohol use (W1) | 0.14 | 0.02 | 1.15 | (1.10, 1.20) | .000 |
| Receipt of public assistance (W1) | −0.17 | 0.19 | 0.85 | (0.57, 1.23) | .381 |
| Education (W4) | |||||
| High school [ref] | |||||
| Less than high school | 0.86 | 0.25 | 2.40 | (1.46, 3.84) | < .001 |
| Some college | 1.27 | 0.25 | 3.60 | (2.90, 5.79) | < .001 |
| College or more | 1.57 | 0.26 | 4.88 | (2.92, 7.94) | < .001 |
| Age (W4) | −0.16 | 0.03 | 0.85 | (0.81, 0.90) | < .001 |
| Sexual identity (W4) | |||||
| Heterosexual [ref] | |||||
| LGB | −0.01 | 0.22 | 0.99 | (0.64, 1.53) | .968 |
| Same-sex attraction (W4) | 0.64 | 0.15 | 1.88 | (1.41, 2.54) | < .001 |
| Wave 2 parent-child relationship quality regressed on: | |||||
| Same-sex attraction (W1) | −0.15 | 0.05 | −0.05 | (−0.08, −.02) | .002 |
| Wave 2 parental autonomy granting regressed on: | |||||
| Same-sex attraction (W1) | 0.02 | 0.02 | 0.02 | (−.02, .06) | .313 |
Acknowledgements
This research uses data from Add Health, a program project directed by Kathleen Mullan Harris and designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill, and funded by grant P01-HD31921 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, with cooperative funding from 23 other federal agencies and foundations. Information on how to obtain the Add Health data files is available on the Add Health website (http://www.cpc.unc.edu/addhealth). No direct support was received from grant P01-HD31921 for this analysis.
Funding
This study was funded in part by the National Institute on Alcohol Abuse and Alcoholism (awarded to Fish) grant number F32AA023138. This research was also supported by grant P2CHD041041, Maryland Population Research Center, and P2CHD042849, awarded to the Population Research Center at The University of Texas at Austin by the Eunice Kennedy Shriver National Institute of Child Health and Human Development. Additionally, the study was funded in part by the National Institutes of Drug Abuse (awarded to Watson) grant number K01DA047918. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The authors acknowledge generous support from the Communities for Just Schools Fund Project at the New Venture Fund, and for Russell from the Priscilla Pond Flawn Endowment at the University of Texas at Austin. Fish would also like to acknowledge support from the the University of Maryland Prevention Research Center cooperative agreement U48DP006382 from the Centers for Disease Control and Prevention (CDC). Any interpretations and opinions expressed herein are solely those of the authors and may not reflect those of the CDC.
Footnotes
Publisher's Disclaimer: This Author Accepted Manuscript is a PDF file of an unedited peer-reviewed manuscript that has been accepted for publication but has not been copyedited or corrected. The official version of record that is published in the journal is kept up to date and so may therefore differ from this version.
Data Sharing Declaration.
The data that support the findings of this study are available from Add Health, a program project directed by Kathleen Mullan Harris and designed by J. Richard Udry, Peter S. Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill team, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. However, data are available from the authors upon reasonable request and with permission of the Add Health program.
Conflict of Interest
The authors report no conflict of interests.
Ethical Approval
The University of Texas and the University of Maryland Institutional Review Boards granted exemption from human subjects review for the current study given that data are anonymous and publically available.
Informed Consent
The current study design uses secondary data; therefore, informed consent was not necessary. Informed consent was obtained as part of the original study.
The Mplus bootstrap option does not work with the FIML missing data procedure nor the integration statement requirements to estimate the indirect effects with weighted survey data (Muthen, 2015).
References
- Abar CC, Jackson KM, Colby SM & Barnett NP (2015). Parent-child discrepancies in reports of parental monitoring and their relationship to adolescent alcohol-related behaviors. Journal of Youth and Adolescence, 44, 1688–701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- American Psychiatric Association (2000). Diagnostic and statistical manual of mental disorders (4th ed., Text Revision). Washington, DC: Author. [Google Scholar]
- Baumrind D (1991). The influence of parenting style on adolescent competence and substance use. Journal of Early Adolescence, 11, 56–95. [Google Scholar]
- Baumrind D (2013). Authoritative parenting revisited: History and current status In Larzelere RE, Morris AS, & Harrist AW (Eds.), Authoritative parenting: Synthesizing nurturance and discipline for optimal child development (pp. 11–34). Washington, DC: American Psychological Association. [Google Scholar]
- Best JR, & Miller PH (2010). A developmental perspective on executive function. Child Development, 81, 1641–1660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brody GH, Chen YF, Kogan SM, Murry VM, & Brown AC (2010). Long-term effects of the strong African American families program on youths’ alcohol use. Journal of consulting and clinical psychology, 78, 281–285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen P, & Chantala K (2014). Guidelines for analyzing Add Health data. Carolina Population Center: University of North Carolina at Chapel Hill [Google Scholar]
- Coulter RWS, Jun H-J, Truong N, Mair C, Markovic N, Friedman MR, … Corliss HL (2019). Effects of familial and non-familial warmth during childhood and adolescence on sexual-orientation disparities in alcohol use trajectories and disorder during emerging adulthood. Drag and Alcohol Dependence, 205, 107643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- D’Augelli AR, Grossman AH, & Starks MT (2008). Families of gay, lesbian, and bisexual youth: What do parents and siblings know and how do they react? Journal of GLBT Family Studies, 4, 95–115. [Google Scholar]
- Delker E, Brown Q, & Hasin DS (2016). Alcohol Consumption in Demographic Subpopulations. Alcohol Research: Current Reviews, 38(1), 7–15. [PMC free article] [PubMed] [Google Scholar]
- Diamond G, Russon J, & Levy S (2016). Attachment-based family therapy: A review of the empirical support. Family Process, 55, 595–610. [DOI] [PubMed] [Google Scholar]
- Dixon SV, Graber JA, & Brooks-Gunn J (2008). The roles of respect for parental authority and parenting practices in parent–child conflict among African American, Latino, and European American Families. Journal of Family Psychology, 22, 1–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Driscoll AK, Russell ST, & Crockett LJ (2008). Parenting Styles and Youth Well-Being Across Immigrant Generations. Journal of Family Issues, 29, 185–209. [Google Scholar]
- Enders CK (2010). Applied missing data analysis. New York, NY: Guilford Press. [Google Scholar]
- Fletcher AC, Steinberg L, & Williams-Wheeler M (2004). Parental influences on adolescent problem behavior: Revisiting Stattin and Kerr. Child development, 75, 781–796. DOI: 10.1111/j.1467-8624.2004.00706.X [DOI] [PubMed] [Google Scholar]
- Fish JN, & Baams L (2018). Trends in alcohol-related disparities between heterosexual and sexual minority youth from 2007 to 2015: Findings from the Youth Risk Behavior Survey. LGBT Health, 5, 359–637 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fish JN, Hughes TL, Russell ST (2018). Sexual identity differences in high-intensity binge drinking: Findings from a US National Sample. Addiction, 113, 749–758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fish JN, Pollitt AM, Schulenberg JE, & Russell ST (2017). Alcohol use from adolescence through early adulthood: an assessment of measurement invariance by age and gender. Addiction, 112(8), 1495–1507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fish JN, Schulenberg JE, & Russell ST (2019). Sexual minority youth report high-intensity binge drinking: The critical role of school victimization. Journal of Adolescent Health, 64, 186–193 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fish JN, & Russell ST (2018). Have mischievous responders misidentified sexual minority youth disparities in the National Longitudinal Study of Adolescent to Adult Health? Archives of Sexual Behavior, 47, 1053–1067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldbach JT, & Gibbs JJ (2017). A developmentally informed adaptation of minority stress for sexual minority adolescents. Journal of Adolescence, 55, 36–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gordon M, Russell BS, & Finan L (2020). The influence of parental support and community belonging on socioeconomic status and adolescent substance use over time. Substance Use and Misuse, 55, 23–36. [DOI] [PubMed] [Google Scholar]
- Harris Kathleen Mullan. 2009. The National Longitudinal Study of Adolescent to Adult Health (Add Health), Waves I & II, 1994–1996; Wave III, 2001–2002; Wave IV, 2007–2009 [machine-readable data file and documentation]. Chapel Hill, NC: Carolina Population Center, University of North Carolina at Chapel Hill. [Google Scholar]
- Hughes TL, Wilsnack SC, & Kantor LW (2016). The influence of gender and sexual orientation on alcohol use and alcohol-related problems. Alcohol Research: Current Reviews, 38, 121–132. [PMC free article] [PubMed] [Google Scholar]
- Kerr M, Stattin H, & Burk WJ (2010). A reinterpretation of parental monitoring in longitudinal perspective. Journal of research on Adolescence, 20, 39–64. [Google Scholar]
- Kline R (2016). Principles and practice of structural equation modeling. New York, NY: The Guilford Press. [Google Scholar]
- Koning IM, van den Eijnden RJJM, Verdurmen JEE, Engels RCME, & Vollebergh WAM (2012). Developmental alcohol specific parenting profiles in adolescence and their relationships with adolescents’ alcohol use. Journal of Youth and Adolescence, 41, 1502–1511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Krueger EA, Fish JN, & Upchurch DM (2020). Sexual Orientation Disparities in Substance Use: Investigating Social Stress Mechanisms in a National Sample. American journal of preventive medicine, 58, 59–68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lanza HI, Huang DYC, Murphy DA, & Hser YI (2013). A latent class analysis of maternal responsiveness and autonomy-granting in early adolescence: Prediction to later adolescent sexual risk-taking. Journal of Early Adolescence, 33, 404–428 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marshal MP, Friedman MS, Stall R, King KM, Miles J, Gold MA, … Morse JQ (2008). Sexual orientation and adolescent substance use: a meta-analysis and methodological review. Addiction, 103, 546–556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCabe SE, Hughes TL, Bostwick WB, West BT, & Boyd CJ (2009). Sexual orientation, substance use behaviors and substance dependence in the United States. Addiction, 104, 1333–1345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mereish EH (2019). Substance use and misuse among sexual and gender minority youth. Current Opinion in Psychology, 30, 123–127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meyer IH (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychological Bulletin, 129, 674–697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Minaie MG, Hui KK, Leung RK, Toumbourou JW, & King RM (2015). Parenting style and behavior as longitudinal predictors of adolescent alcohol use. Journal of Studies on Alcohol and Drugs, 76, 671–679. [DOI] [PubMed] [Google Scholar]
- Montano GT, Marshal MP, McCauley HL, Miller E, Chung T, & Hipwell AE (2018). Group-based trajectories of parent-child communication and parental knowledge between sexual minority and heterosexual girls and their associations with substance use. Journal of Adolescence, 69, 150–162 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Montano GT, McCauley HL, Miller E, Chisolm DJ, & Marshal MP (2017). Differences in Parental Monitoring Components and Their Associated Health Indicators Between Sexual-Minority and Heterosexual Girls. Journal of GLBT Family Studies, 13(3), 211–235. 10.1080/1550428X.2016.1200507 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mustanski B, Kuper L, & Greene GJ (2014). Development of sexual orientation and identity In Tolman DL, Diamond LM, Bauermeister JA, George WH, Pfaus JG, & Ward LM (Eds.), APA handbook of sexuality and psychology, Vol. 1: Person-based approaches, (pp. 597–628). Washington: American Psychological Association. [Google Scholar]
- Mustanski B, Swann G, Newcomb ME, & Prachand N (2017). Effects of Parental Monitoring and Knowledge on Substance Use and HIV Risk Behaviors Among Young Men Who have Sex with Men: Results from Three Studies. AIDS and Behavior, 21(7), 2046–2058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK (2015, March 11). Path analysis with a binary outcome variable [Online forum comment]. Retrieved from http://www.statmodel.com/discussion/messages/23/12916.html?1499400666 [Google Scholar]
- Muthén LK, & Muthén BO (1998–2011). Mplus User's Guide. Sixth Edition. Los Angeles, CA: Muthén & Muthén. [Google Scholar]
- Needham BL, & Austin EL (2010). Sexual orientation, parental support, and health during the transition to young adulthood. Journal of Youth and Adolescence, 39, 1189–1198. [DOI] [PubMed] [Google Scholar]
- Newcomb ME, LaSala MC, Bouris A, Mustanski B, Prado G, Schrager SM, & Huebner DM (2019). The influence of families on LGBTQ youth health: A call to action for innovation in research and intervention development. LGBT Health, 6, 139–145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ohannessian CM, Flannery KM, Simpson E, & Russell BS (2016). Family functioning and adolescent alcohol use: A moderated mediation analysis. Journal of Adolescence, 49, 19–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Padilla-Walker LM, & Son D (2019). Longitudinal associations among routine disclosure, the parent–child relationship, and adolescents’ prosocial and delinquent behaviors. Journal of Social and Personal Relationships, 36, 1853–1871. [Google Scholar]
- Patock-Peckham JA, & Morgan-Lopez AA (2009). Mediational links among parenting styles, perceptions of parental confidence, self-esteem, and depression on alcohol-related problems in emerging adulthood. Journal of Studies on Alcohol and Drugs, 70, 215–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Plöderl M, & Tremblay P (2015). Mental health of sexual minorities. A systematic review. International Review of Psychiatry, 27, 367–385. [DOI] [PubMed] [Google Scholar]
- Prado G, Pantin H, Huang S, Cordova D, Tapia MI, Velazquez MR, … & Jimenez GL (2012). Effects of a family intervention in reducing HIV risk behaviors among high-risk Hispanic adolescents: A randomized controlled trial. Archives of pediatrics & adolescent medicine, 166, 127–133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ream GL, & Savin-Williams RC (2005). Reciprocal associations between adolescent sexual activity and quality of youth-parent interactions. Journal of Family Psychology, 19, 171–179. [DOI] [PubMed] [Google Scholar]
- Rogers MM, & McKinney C (2019). Emerging adult risky sexual behavior predicted by parental overprotection: Moderated mediation analysis. Family Process, 58, 972–985. [DOI] [PubMed] [Google Scholar]
- Russell BS & Gordon M (2017). Parenting and adolescent substance use: Moderation effects of community engagement in a nationally representative sample. International Journal of Mental Health and Addiction, 15(5), 1023–1036. DOI 10.1007/s11469-017-9728-0 [DOI] [Google Scholar]
- Russell ST, & Fish JN (2016). Mental Health in lesbian, gay, bisexual, and transgender (LGBT) youth. Annual Review of Clinical Psychology, 12, 465–487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Russell ST, & Fish JN (2019). Sexual minority youth, social change, and health: A developmental collision. Research in Human Development, 16, 5–20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Russell ST, & Toomey RB (2013). Protective factors for suicidal thoughts among sexual minority youth: evidence from the add health study. Journal of Gay & Lesbian Mental Health, 17, 132–149. [Google Scholar]
- Russell ST, Toomey RB, Ryan C, & Diaz RM (2014). Being out at school: The implications for school victimization and young adult adjustment. American Journal of Orthopsychiatry, 84(6), 635–643. [DOI] [PubMed] [Google Scholar]
- Ryan C, Huebner D, Diaz RM, & Sanchez J (2009). Family rejection as a predictor of negative health outcomes in White and Latino lesbian, gay, and bisexual young adults. Pediatrics, 123(1), 346–352. 10.1542/peds.2007-3524 [DOI] [PubMed] [Google Scholar]
- StataCorp. 2017. Stata Statistical Software: Release 15 College Station, TX: StataCorp LLC [Google Scholar]
- Steinberg L (2007). Risk taking in adolescence new perspectives from brain and behavioral science. Current Directions in Psychological Science, 16(2), 55–59. DOI [Google Scholar]
- Steinberg L, Blatt-Eisengart I, & Cauffman E (2006). Patterns of competence and adjustment among adolescents from authoritative, authoritarian, indulgent, and neglectful homes: A replication in a sample of serious juvenile offenders. Journal of Research on Adolescence, 16, 47–58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steinberg L, Darling NE, & Fletcher AC (1995). Authoritative parenting and adolescent adjustment: An ecological journey In Moen P, Elder GH, & Luscher K (Eds.), Examining lives in context: Perspectives on the ecology of human development (pp. 423–466). Washington, DC: American Psychological Association. [Google Scholar]
- Steinberg L, & Silk JS (2002). Parenting adolescents In Bornstein MH (Ed.), Handbook of parenting: Children and parenting (pp. 103–133). Mawah, NJ: Lawrence Earlbaum Associates [Google Scholar]
- Talley AE, Gilbert PA, Mitchell J, Goldbach J, Marshall BDL, & Kaysen D (2016). Addressing gaps on risk and resilience factors for alcohol use outcomes in sexual and gender minority populations. Drug and Alcohol Review, 35, 484–493. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Watson RJ, Barnett M, & Russell ST (2016). Parent support matters for the educational success of sexual minorities. Journal of GLBT Family Studies, 12, 188–202. doi: 10.1080/1550428X.2015.1028694 [DOI] [Google Scholar]
- Watson RJ, Rose H, Doull M, Adjei J, & Saewyc E (2019). Worsening perceptions of family connectedness and parent support for lesbian, gay, and bisexual adolescents. Journal of Child and Family Studies, 28, 3121–3131. doi: 10.1007/s10826-019-01489-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.