

Abstract
Objectives
This study aims to evaluate the effects of local adipose stem cell injection on non-union and diabetic non-union of rat femurs.
Materials and methods
Forty-eight female Wistar albino rats (weighing mean 200 g and aged 8 weeks) were used in this study. The rats were divided into six groups. Group 1 was chosen as a reference for receptor activator of nuclear factor-kappa (k) B (RANK), receptor activator of nuclear factor-k B ligand (RANKL) and osteoprotegerin (OPG) genes and no femur osteotomy was performed in this group. Group 2 underwent femur osteotomy, the osteotomy was fixed with a 1.5 mm K-wire as retrograde from the knee joint, and no gap was left in the osteotomy line. In order to induce non-union, femurs underwent osteotomy fixed with K-wires in groups 3, 4, 5 and 6. In addition, the osteotomy line was measured as 1.8 mm gap with electronic calipers and the gap was fixed with U staple. Before osteotomy, streptozocin was injected intraperitoneally at a dose of 60 mg/kg in 0.1 mol/L citrate buffer solution (Ph 4.4) in groups 4 and 6, in order to induce diabetes mellitus. Left femur anteroposterior and lateral X-rays were taken 10 weeks after the operation and the union in group 2 and non-union in groups 3, 4, 5, and 6 were confirmed. To see if injection of adipose stem cells into the non-union site increases bone union, 2 mL 0.9% sodium chloride (NaCl) in groups 3 and 4 and 2×106 adipose stem cell in groups 5 and 6 were locally injected into the non-union area with fluoroscopy. Femur X-rays were taken eight weeks after the injection and all rats were sacrificed. Femurs of rats were removed for histopathological and gene expression evaluation.
Results
There were significant differences between the groups injected 0.9% NaCI and adipose stem cells in terms of bone healing according to radiological and histopathological evaluations (p<0.05). No statistically significant difference was observed between the groups in terms of gene expression levels.
Conclusion
According to the results of our study, local adipose stem cell injection has positive radiological and histopathological effects in diabetic and non-diabetic femoral non-unions, independently of RANK, RANKL, or OPG gene expression pathways.
Keywords: Adipose stem cell, non-union, osteoprotegerin, receptor activator of nuclear factor-kappa B, receptor activator of nuclear factor-kappa B ligand
Introduction
Fracture non-union is a chronic condition characterized by pain and functional disability. According to the diagnostic criteria established by the United States Food and Drug Administration, a non-union occurs when a fracture fails to union over a period of nine or more months or fails to prove any radiographic clues of healing response in an osseous environment within the previous three months of the follow-up.[1]
Non-unions are seen in a small percentage of cases in which the biological process of fracture repair cannot overcome the local biology and mechanics of bony injury. This leads to a large number of procedures to treat non-healing fractures, increasing morbidity for patients and costs.
Non-union of fractures have become an important health problem. Non-union still remains as a problem in some fractures despite the developments in surgical techniques and materials used in fracture repair. Delayed healing or non-union is an expected situation particularly in the fractures with wide soft tissue, bony tissue and periosteal damage.[2,3]
A higher rate of non-union has been found in different risk groups after ankle arthrodesis including diabetic patients compared to non-diabetic patients.[4]
Although autologous bone grafts are recognized as the gold standard for the conditions of non-healing fracture or non-union, there are negative aspects such as leading to damage in the body region where the graft was taken and the removed part being limited.[5-7] An alternative is the use of stem cells on bone.[8] Studies have focused on diabetic non-union, adipose stem cell and genetic mechanisms of healing.[9-19]
A literature screening revealed that numerous non-union models have been described in rats, mice and rabbits, and the use and effects of stem cells have been investigated in a large number of fracture healings.[9-14] However, to our knowledge, there is no study using stem cell application in a diabetic non-union model.
Mesenchymal stem cells can also be obtained from muscle tissue, adipose tissue and synovium.[15] More recently, the advent of induced pluripotent stem cells obtained through genetic engineering of somatic cells, and possessing high proliferation and differentiation capabilities have offered additional promising alternative sources for bone regeneration.[16,17]
Nowadays, with the introduction of genetic therapy and diagnostic tools in medicine, each tissue, disease and treatment have been addressed again, and their correlations with genes have been studied. The genes particularly known for bony tissue include receptor activator of nuclear factor-kappa (κ) B (RANK), receptor activator of nuclear factor-κ B ligand (RANKL) and osteoprotegerin (OPG) genes.[18,19] In our hypothesis, localization of adipose stem cell injection for non-union will provide positive effect on union by activation of RANK, RANKL, and OPG gene expression. Therefore, in this study, we aimed to evaluate the effects of local adipose stem cell injection on non-union and diabetic non-union of rat femurs.
Patients and Methods
This study was conducted at Erciyes University Medical Faculty between May 2015 and December 2016. A total of 48 female Wistar albino rats (weighing mean 200 g and aged 8 weeks) were included. Rats were randomly divided into six groups with eight subjects in each group. Before surgery, groups were intraperitoneally injected with 3 mg/kg xylazine hydrochloride and 90 mg/kg ketamine hydrochloride for anesthesia under protection of animal rights. All experimental protocols were approved by the Erciyes University Medical Faculty Ethics Committee for Experimental Animal Research (approval: 12.11.2014- 14/138).
Group 1 was chosen as a reference for RANK, RANKL and OPG genes and no femur osteotomy was performed in this group. Group 2 underwent femur osteotomy, the osteotomy was fixed with 1.5 mm Kirschner wires (K-wires) as retrograde from the knee joint.[20,21] Left femur anteroposterior and lateral X-rays were taken 10 weeks after the operation and the union was confirmed.
Streptozocin (STZ) was injected intraperitoneally at a dose of 60 mg/kg in 0.1 mol/L citrate buffer solution (Ph 4.4)[22] in order to induce diabetes mellitus (DM) in groups 4 and 6. Following the STZ injection, 12-hour fasting blood glucose levels were measured on the third day. Rats with fasting blood glucose levels ≥200 mg/dL at each measurement were accepted to have DM,[23] and these rats were included in the diabetic groups.
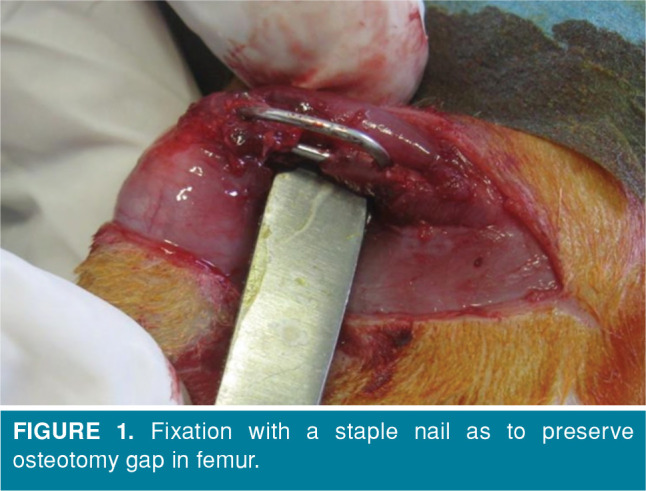
In order to induce non-union for groups 3, 4, 5 and 6, after femur osteotomy fixation with K-wires, osteotomy line was measured as 1.8 mm gap as described by Garcia et al.[13] with electronic calipers and the gap was fixed with a U staple (Figure 1). Femurs’ X-rays were taken 10 weeks after the operation and the non-union was confirmed.[13,14]
Figure 1. Fixation with a staple nail as to preserve osteotomy gap in femur.
Mesenchymal stem cells (MSCs) were prepared and determined to have a typical fusiform appearance Erciyes University, Genome and Stem Cell Center (GENKOK) (Figure 2). Morphology of the cells was found to have typical fusiform, fibroblast like MSC character. The desired number of cells was easily reached at the third passage. As a result of flow cytometric study, adipose MSCs were found to express MSC markers. Cluster of differentiation (CD)11b/c was found as 4.7%, CD45 as 0.9%, CD29 as 91.7%, CD73 as 90%, CD90 as 92.7%, and CD44 as 90.4% (Figure 3).
Figure 2. Morphologic image of adipose mesenchymal stem cell, light microscope.
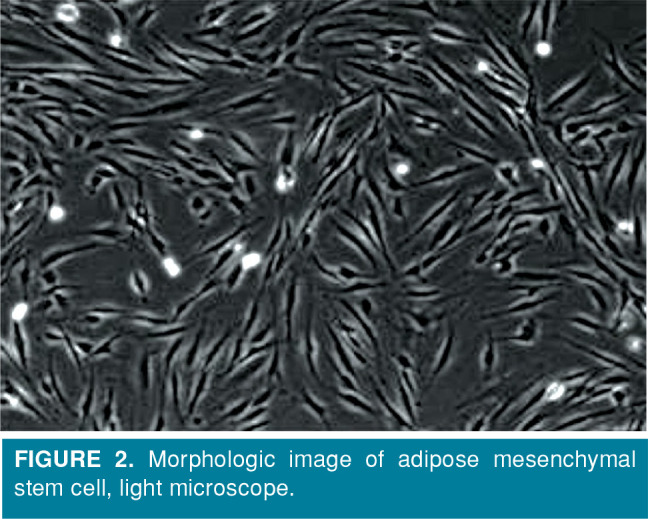
Figure 3. Adipose mesenchymal stem cells cluster of differentiation (CD) 29, CD44, CD73, and CD90 were positive, while CD 11b/c and CD45 were negative in flow cytometry.

Non-union lines were accessed through approximately 2 cm incision from the lateral femur of the subjects and 2×106 adipose stem cells were given to the non-union line in feeding solution in the 10th week in groups 5 and 6. In order to see if injection of adipose stem cells into the non-union site increases bone union, all rats were sacrificed at eight weeks post-injection.[24] Left femurs of the rats were dissected from the soft tissue for histopathological examination and gene expression.
Statistical analysis
Data were analyzed using the PASW for Windows version 17.0 (SPSS Inc., Chicago, IL, USA) software. Normality of quantitative variables was analyzed with Kolmogorov-Smirnov test. In the comparison of the data of two different groups, t-test was used for normally distributed variables, while Mann- Whitney U test was used for non-normally distributed variables. One-way analysis of variance was used in the comparison of multiple group data. When the difference between group data was significant, Tukey test was used in post-hoc test in subgroup analysis. Chi-square test was used in the comparison of categorical data. P values <0.05 were considered statistically significant.
Results
The formation of non-union and union grades were evaluated by mentor authors. The evaluation was performed by Lane-Sandhu classification.[25]
In group 2, complete bone union was observed in five rats (62.5%), invisible fracture line in two rats (25%), and union onset in one rat (12.5%), while in group 3, callus was seen in four rats (50%), and union onset in two rats (25%). There was a statistically significant difference between groups 2 and 3 (p<0.05).
In group 3, union onset was observed in two rats (25%), and callus in four rats (50%), while in group 5, complete bone union was found in one rat (12.5%), invisible fracture line in one rat (12.5%), and union onset in six rats (75%). There was a statistically significant difference between groups 3 and 5 in radiological outcomes (p<0.05) (Figures 4 and 5).
Figure 4. Radiographs of a subject from group 3. Non-union is observed in 10 weeks. In group 3, 2 mL 0.9% sodium chloride was locally injected into non-union area with fluoroscopy. Eight weeks after injection, femur X-rays were taken. No improvement was observed in non-union line.

Figure 5. Radiograph of a subject from group 5. Non-union was seen in X-rays at 10th week. In group 5, 2x106 adipose stem cells were locally injected to non-union area with fluoroscopy. Eight weeks after injection, femur X-rays were taken. Injection of adipose stem cells to fracture zone increased bone union seen in X-rays at 18th week.

Callus was seen in four rats (50%) and no union was seen in group 4. In group 6, callus was seen in two rats (25%) and union was seen in four rats (50%).
The histological samples were taken from paraffin blocks which were prepared as 4-6 micron. Evaluation of non-union and union grades of the samples was performed as described by Hou et al.[26]
Comparison of the histological findings between the groups is given in Table I. According to the results of histological examination, there was a statistically significant difference between groups 3, 4 injected sodium chloride and groups 5, 6 injected adipose stem cell (p<0.05) (Table II).
Table 1. Comparison of radiological scores of groups in 10<sup>th</sup> and 18<sup>th</sup> weeks.
| Group 1 | Group 2 | Group 3 | Group 4 | Group 5 | Group 6 | p | |
| 4 | 2.5 | 0 | 0 | 0 | 0 | ||
| 10th week | (4-4) | (2-4) | (0-0) | (0-0) | (0-0) | (0-0) | <0.001 |
| Radiology (n) | 8 | 8 | 8 | 8 | 8 | 8 | |
| 4 | 4 | 1 | 0 | 2 | 1,5 | ||
| 18th week | (4-4) | (2-4) | (0-2) | (0-1) | (2-4) | (0-2) | <0.001 |
| Radiology (n) | 8 | 8 | 8 | 8 | 8 | 8 | |
| Group 1: Was not performed any surgery; Group 2: With union; Group 3: With non-union; Group 4: Diabetic, with non-union; Group 5: With stem cell and non-union; Group 6: Diabetic with stem cell and non-union. | |||||||
Table 2. Comparison of histological findings between groups.
| Group 1 | Group 2 | Group 3 | Group 4 | Group 5 | Group 6 | p | |
| 10 | 10 | 2.5 | 3 | 7 | 3 | ||
| Histological | (10-10) | (6-10) | (1-6) | (1-7) | (6-8) | (0-8) | <0.001 |
| Outcomes (n) | 8 | 8 | 8 | 8 | 8 | 8 | |
| Group 1: Was not performed any surgery; Group 2: With union; Group 3: With non-union; Group 4: Diabetic, with non-union; Group 5: With stem cell and non-union; Group 6: Diabetic with stem cell and non-union. | |||||||
In group 2, union of the fracture was observed in the radiological examination for all rats. In the histological evaluation, mature-immature bone healing was observed in the osteotomy line.
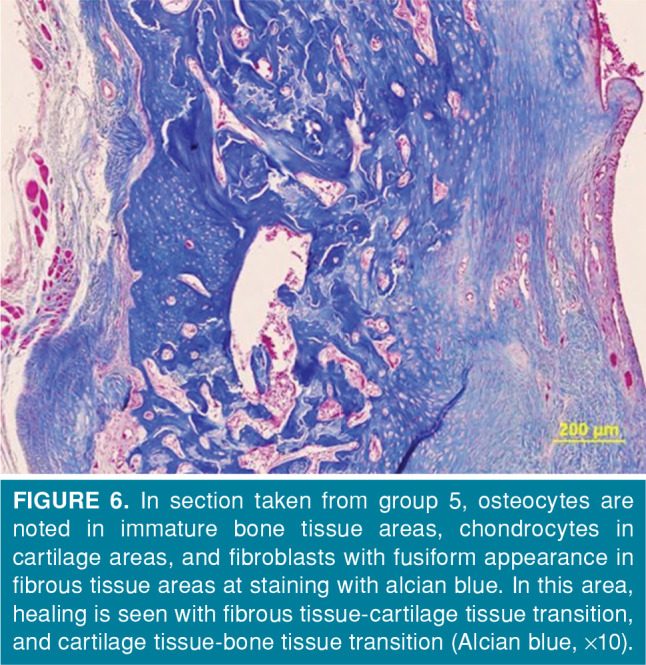
In the microscopic evaluation of group 5, predominantly cartilage tissue and less fibrosis tissue were observed in two rats, immature bone healing was observed in two rats, and mature bone healing in four rats. Histopathological image of a rat from group 5 is presented in Figure 6.
Figure 6. In section taken from group 5, osteocytes are noted in immature bone tissue areas, chondrocytes in cartilage areas, and fibroblasts with fusiform appearance in fibrous tissue areas at staining with alcian blue. In this area, healing is seen with fibrous tissue-cartilage tissue transition, and cartilage tissue-bone tissue transition (Alcian blue, x10).
In the microscopic evaluation of group 6, predominantly cartilage tissue and less fibrous tissue were seen in three rats, and immature bone healing was seen in five rats.
The histological evaluation showed that the injection of stem cells is effective in the non-union model even in diabetic rats.
The RANK, RANKL, and OPG gene expression analyses were carried out utilizing real time- polymerase chain reaction (PCR). Comparison of genetic parameters between the groups is given in Table III. Group A1 was taken as the control group in terms of the reference gene expression values for PCR.
Table 3. Comparison of genetic parameters between groups.
| Group 1 | Group 2 | Group 3 | Group 4 | Group 5 | Group 6 | p | |
| 0.94 | 0.25 | 0.57 | 1.94 | 0.69 | 0.36 | ||
| 22 | (0.16-30.4) | (0.02-9.0) | (0.05-8.11) | (0.53-36.0) | (0.20-56.10) | (0.12-56.1) | 0.334 |
| RANK (n) | 8 | 8 | 8 | 8 | 8 | 8 | |
| 0.59 | 0.39 | 0.93 | 2.05 | 0.67 | 0.61 | ||
| 22 | (0.12-7.84) | (0.03-3.34) | (0.19-17.51) | (0.24-9.65) | (0.00-10.48) | (0.02-13.5) | 0.758 |
| RANK (n) | 6 | 6 | 8 | 8 | 5 | 7 | |
| 0.28 | 0.16 | 0.37 | 0.51 | 0.00 | 0.35 | ||
| 22 | (0.05-6.96) | (0.00-0.47) | (0.00-046020.85) | (0.02-3.07) | (0.00-0.31) | (0.07-5.31) | 0.444 |
| RANK (n) | 6 | 4 | 7 | 4 | 3 | 6 | |
| Group 1: Was not performed any surgery; Group 2: With union; Group 3: With non-union; Group 4: Diabetic, with non-union; Group 5: With stem cell and non-union; Group 6: Diabetic with stem cell and non-union; RANK: Receptor activator of nuclear factor-kappa B. | |||||||
In the measurements of gene expression levels using PCR techniques, first, the correlation of these genes with fracture healing was examined. PCR expression image of RANK gene is shown in Figure 7.
Figure 7. Polymerase chain reaction expression image of receptor activator of nuclear factor-kappa B gene.
No statistical correlation could be demonstrated between gene expression and fracture healing (groups 1-2), non-union (groups 2-3), adipose stem cell administration (groups 3-5), and diabetes (groups 4-6) formation (p>0.05 in all comparisons).
Discussion
In the present study, we tried to demonstrate the effectiveness of adipose stem cell therapy in a non-union model induced in non-diabetic group 5 and diabetic group 6 rats, and effects of the genes thought to play a role in fracture healing such as RANK, RANKL, and OPG.
According to the results of our study, local adipose stem cell injection has a positive radiological and histopathological effect in femoral non-unions, independent of RANK, RANKL and OPG genes expression pathways.
The RANKL, which is expressed primarily by osteoblasts and bone marrow stromal cells and occurs membrane bound on the surface of these cells, exerts an important effect on the activation of osteoclasts.[27,28] RANK, which is the receptor for RANKL, is significant for osteolysis.[29] The expression of OPG and RANKL has been shown to be related to the regulation of osteoclast differentiation controlled by osteoblasts.[30] On the other hand, we could not find any statistical correlation between gene expression and fracture healing (groups 1-2), non-union (groups 2-3), adipose stem cell administration (groups 3-5), and diabetes (groups 4-6) formation (p>0.05 for all). For these findings, we aimed to explain the mechanism of action of stem cells in non-union with pathways of these genes. However, we could not statistically show the relationship between stem cells healing, diabetic non-union, non-union and fracture healing with the genes. We thought that stem cells might use another gene pathway.
Several factors such as age, smoking, drugs and various systemic diseases play an important role in the development of delayed union or non-union. Diabetes mellitus is among the systemic diseases which are known to negatively affect bone healing.[4] We supported these findings in our study. Nondiabetic group 3 with non-union has been shown to heal faster than diabetic group 4 with non-union. Adipose stem cells injected nondiabetic group 5 with non-union was shown to heal faster than adipose stem cell applied diabetic group 6 with non-union. Diabetes was shown to reduce the effects of bone healing and adipose stem cell therapy to union.
For the success of non-union therapy, first, a non- union model should be created. Common causes of non-unions developed after lower extremity fractures such as the femur and tibia include diabetes, infections, open fractures, fractures due to gunshot injuries, defective segmental fractures, periosteal injuries and fixation failure. In this study, we used a non-union model by creating bone gap in rats with and without diabetes induced, as described by Garcia et al.[13] After osteotomy was performed in the left femurs of the rats, periosteal was proximally and distally dissected. The fracture line was fixed so as to leave a 1.8 mm gap and waited for 10 weeks. The formation of non-union was confirmed with radiological examination.
Group 2 was shown to have fracture healing faster than group 3. These results indicated that fractures with bone defect and damaged periosteal were the only factors in the development of non-union. Thus, it can be said that the non-union model used in the study described by Garcia et al.[13] was successful.
Although autologous bone grafts are considered the gold standard for the conditions where fracture healing is not observed or may be problematic in terms of union, these grafts have some disadvantages such as leading to damage in the body region where they are taken, and the amount of removed graft being limited.[5-7] Therefore, researchers have proposed various alternatives in order to accelerate fracture healing, and eliminate delayed union and non-union.[31] One of these alternatives is the use of stem cells on bony tissue.[9] Taguchi et al.[10] have evaluated in vivo migration of bone marrow cells and their contribution to bone repair and shown that MSCs were definitely associated with bone healing.
In our study, adipose stem cells were shown to be effective in diabetic and nondiabetic rat non-union model. Group 5 with adipose stem cell and non-union was shown to heal faster than group 3 with non- union. Group 6 with adipose stem cell and diabetic non-union was shown to heal faster than group 4 with diabetic non-union.
Numerous authors have used only histopathology, which relies on firm evidence.[3,10] In the current study, we preferred the histopathological grading system developed by Huo et al.[26] Although more fibrous tissue and less cartilage were seen in the light microscope in the control groups, the amount of immature and mature bony tissue was higher in the stem cell groups. Therefore, subjective radiologic examination was supported with histopathological examination, which is more objective.
In the present study conducted using adipose stem cells, it was found that adipose stem cell application showed a positive effect in the treatment of non-union in non-diabetic subjects, and the differences were significant in terms of the radiological and histopathological results.
This study has some limitations including being based on animal experiments with small-sized study groups and having a limited gene diversity analysis.
In conclusion, although today there are different treatment options for non-union, local adipose stem cell injection has positive radiological and histopathological effects in diabetic and non-diabetic femoral non-unions, independently of RANK, RANKL, or OPG gene expression pathways. The findings of our study need to be supported with further future studies.
Footnotes
Conflict of Interest: The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Financial Disclosure: This study was funded by the Scientific Research Projects of University of Erciyes. Number of approval: TTU-2015-5780.
References
- 1.Pountos I, Georgouli T, Pneumaticos S, Giannoudis PV. Fracture non-union: Can biomarkers predict outcome. Injury. 2013;44:1725–1732. doi: 10.1016/j.injury.2013.09.009. [DOI] [PubMed] [Google Scholar]
- 2.Kabak S, Halici M, Tuncel M, Avsarogullari L, Karaoglu S. Treatment of midclavicular nonunion: comparison of dynamic compression plating and low-contact dynamic compression plating techniques. J Shoulder Elbow Surg. 2004;13:396–403. doi: 10.1016/j.jse.2004.01.033. [DOI] [PubMed] [Google Scholar]
- 3.Ozaki A, Tsunoda M, Kinoshita S, Saura R. Role of fracture hematoma and periosteum during fracture healing in rats: interaction of fracture hematoma and the periosteum in the initial step of the healing process. J Orthop Sci. 2000;5:64–70. doi: 10.1007/s007760050010. [DOI] [PubMed] [Google Scholar]
- 4.Azad V, Breitbart E, Al-Zube L, Yeh S, O'Connor JP, Lin SS. rhBMP-2 enhances the bone healing response in a diabetic rat segmental defect model. J Orthop Trauma. 2009;23:267–276. doi: 10.1097/BOT.0b013e31819f290e. [DOI] [PubMed] [Google Scholar]
- 5.Fillingham Y, Jacobs J. Bone grafts and their substitutes. Bone Joint J. 2016;98-B:6–9. doi: 10.1302/0301-620X.98B.36350. [DOI] [PubMed] [Google Scholar]
- 6.Emara KM, Diab RA, Emara AK. Recent biological trends in management of fracture non-union. World J Orthop. 2015;6:623–628. doi: 10.5312/wjo.v6.i8.623. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Barba M, Cicione C, Bernardini C, Campana V, Pagano E, Michetti F, et al. Spinal fusion in the next generation: gene and cell therapy approaches. ScientificWorldJournal. 2014;2014:406159–406159. doi: 10.1155/2014/406159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Watanabe Y, Harada N, Sato K, Abe S, Yamanaka K, Matushita T. Stem cell therapy: is there a future for reconstruction of large bone defects. S47-51Injury. 2016;47 doi: 10.1016/S0020-1383(16)30012-2. [DOI] [PubMed] [Google Scholar]
- 9.Chen G, Fang T, Qi Y, Yin X, Di T, Feng G, et al. Combined Use of Mesenchymal Stromal Cell Sheet Transplantation and Local Injection of SDF-1 for Bone Repair in a Rat Nonunion Model. Cell Transplant. 2016;25:1801–1817. doi: 10.3727/096368916X690980. [DOI] [PubMed] [Google Scholar]
- 10.Taguchi K, Ogawa R, Migita M, Hanawa H, Ito H, Orimo H. The role of bone marrow-derived cells in bone fracture repair in a green fluorescent protein chimeric mouse model. Biochem Biophys Res Commun. 2005;331:31–36. doi: 10.1016/j.bbrc.2005.03.119. [DOI] [PubMed] [Google Scholar]
- 11.Senos R, Roberto-Rodrigues M, Fernandes RMP, Santos TMP, Viana LP, Lima I, et al. Nandrolone decanoate in induced fracture nonunion with vascular deficit in rat model: morphological aspects. Musculoskelet Surg. 2019 doi: 10.1007/s12306-019-00621-2. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 12.SunL , LiZ , XueH , MaT , RenC , LiM , etal MiR-26a promotes fracture healing of nonunion rats possibly by targeting SOSTDC1 and further activating Wnt/β-catenin signaling pathway. Mol Cell Biochem. 2019;460:165–173. doi: 10.1007/s11010-019-03578-9. [DOI] [PubMed] [Google Scholar]
- 13.Garcia P, Holstein JH, Maier S, Schaumlöffel H, Al-Marrawi F, Hannig M, et al. Development of a reliable non-union model in mice. J Surg Res. 2008;147:84–91. doi: 10.1016/j.jss.2007.09.013. [DOI] [PubMed] [Google Scholar]
- 14.Orth M, Kruse NJ, Braun BJ, Scheuer C, Holstein JH, Khalil A, et al. BMP-2-coated mineral coated microparticles improve bone repair in atrophic non-unions. Eur Cell Mater. 2017;33:1–12. doi: 10.22203/eCM.v033a01. [DOI] [PubMed] [Google Scholar]
- 15.Yoo JU, Barthel TS, Nishimura K, Solchaga L, Caplan AI, Goldberg VM, et al. The chondrogenic potential of human bone-marrow-derived mesenchymal progenitor cells. J Bone Joint Surg [Am] 1998;80:1745–1757. doi: 10.2106/00004623-199812000-00004. [DOI] [PubMed] [Google Scholar]
- 16.Lou X. Induced Pluripotent Stem Cells as a new Strategy for Osteogenesis and Bone Regeneration. Stem Cell Rev Rep. 2015;11:645–651. doi: 10.1007/s12015-015-9594-8. [DOI] [PubMed] [Google Scholar]
- 17.Wu Q, Yang B, Hu K, Cao C, Man Y, Wang P. Deriving osteogenic cells from ınduced pluripotent stem cells for bone tissue engineering. Tissue Eng Part B Rev. 2017;23:1–8. doi: 10.1089/ten.TEB.2015.0559. [DOI] [PubMed] [Google Scholar]
- 18.de Amorim FP, Ornelas SS, Diniz SF, Batista AC, da Silva TA. Imbalance of RANK, RANKL and OPG expression during tibial fracture repair in diabetic rats. J Mol Histol. 2008;39:401–408. doi: 10.1007/s10735-008-9178-x. [DOI] [PubMed] [Google Scholar]
- 19.Baud’huin M, Lamoureux F, Duplomb L, Rédini F, Heymann D. RANKL, RANK, osteoprotegerin: key partners of osteoimmunology and vascular diseases. Cell Mol Life Sci. 2007;64:2334–2350. doi: 10.1007/s00018-007-7104-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Koçkara N, Sofu H, Issin A, Çetinkaya M, Tayfur M, Süleyman B. Pregabalin does not affect fracture healing adversely. Eklem Hastalik Cerrahisi. 2017;28:19–24. doi: 10.5606/ehc.2017.50897. [DOI] [PubMed] [Google Scholar]
- 21.Baki ME, Aldemir C, Duygun F, Doğan A, Kerimoğlu G. Comparison of non-compression and compression interlocking intramedullary nailing in rabbit femoral shaft osteotomy model. Eklem Hastalik Cerrahisi. 2017;28:7–12. doi: 10.5606/ehc.2017.54333. [DOI] [PubMed] [Google Scholar]
- 22.Liu SH, Chang YH, Chiang MT. Chitosan reduces gluconeogenesis and increases glucose uptake in skeletal muscle in streptozotocin-induced diabetic rats. J Agric Food Chem. 2010;58:5795–5800. doi: 10.1021/jf100662r. [DOI] [PubMed] [Google Scholar]
- 23.Wang F, Xi Y, Liu W, Li J, Zhang Y, Jia M, et al. Sanbai Melon Seed Oil Exerts Its Protective Effects in a Diabetes Mellitus Model via the Akt/GSK-3β/Nrf2 Pathway. J Diabetes Res. 2019;2019:5734723–5734723. doi: 10.1155/2019/5734723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Mir SA, Azam MQ, Al-Dakheel DA, Acharya S. Healing of Experimentally Created Non-Union of Femur in Rats Using Bone Precursor Cells from Mesenchymal Stem Cells (MSCs) J Stem Cells. 2015;10:91–96. [PubMed] [Google Scholar]
- 25.Lane JM, Sandhu HS. Current approaches to experimental bone grafting. Orthop Clin North Am. 1987;18:213–225. [PubMed] [Google Scholar]
- 26.Huo MH, Troiano NW, Pelker RR, Gundberg CM, Friedlaender GE. The influence of ibuprofen on fracture repair: biomechanical, biochemical, histologic, and histomorphometric parameters in rats. J Orthop Res. 1991;9:383–390. doi: 10.1002/jor.1100090310. [DOI] [PubMed] [Google Scholar]
- 27.Wu R, Li Q, Pei X, Hu K. Effects of Brucine on the OPG/ RANKL/RANK Signaling Pathway in MDA-MB-231 and MC3T3-E1 Cell Coculture System. Evid Based Complement Alternat Med. 2017;2017:1693643–1693643. doi: 10.1155/2017/1693643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Kong YY, Yoshida H, Sarosi I, Tan HL, Timms E, Capparelli C, et al. OPGL is a key regulator of osteoclastogenesis, lymphocyte development and lymph-node organogenesis. Nature. 1999;397:315–323. doi: 10.1038/16852. [DOI] [PubMed] [Google Scholar]
- 29.Li J, Sarosi I, Yan XQ, Morony S, Capparelli C, Tan HL, et al. RANK is the intrinsic hematopoietic cell surface receptor that controls osteoclastogenesis and regulation of bone mass and calcium metabolism. Proc Natl Acad Sci U S A. 2000;97:1566–1571. doi: 10.1073/pnas.97.4.1566. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Goto H, Hozumi A, Osaki M, Fukushima T, Sakamoto K, Yonekura A, et al. Primary human bone marrow adipocytes support TNF-α-induced osteoclast differentiation and function through RANKL expression. Cytokine. 2011;56:662–668. doi: 10.1016/j.cyto.2011.09.005. [DOI] [PubMed] [Google Scholar]
- 31.Gürbüz K, Yerer MB, Gürbüz P, Halıcı M. Icariin promotes early and late stages of fracture healing in rats. Eklem Hastalik Cerrahisi. 2019;30:282–288. doi: 10.5606/ehc.2019.66796. [DOI] [PubMed] [Google Scholar]