

Key Points
Question
Is coronary angiography performed immediately after cardiac arrest associated with improved clinical outcomes at 1 year in patients without signs of ST-segment elevation myocardial infarction?
Findings
In this follow-up of a randomized clinical trial that included 552 patients, there was no significant difference in clinical outcomes at 1 year between patients in the immediate angiography group compared with patients whose angiography was delayed until after neurologic recovery. Survival at 1 year was 61.4% in the immediate group vs 64.0% in the delayed group.
Meaning
The findings of this trial suggest that immediate coronary angiography is not associated with improved clinical outcomes at 1 year in patients after cardiac arrest without signs of ST segment elevation myocardial infarction.
Abstract
Importance
Ischemic heart disease is a common cause of cardiac arrest. However, randomized data on long-term clinical outcomes of immediate coronary angiography and percutaneous coronary intervention (PCI) in patients successfully resuscitated from cardiac arrest in the absence of ST segment elevation myocardial infarction (STEMI) are lacking.
Objective
To determine whether immediate coronary angiography improves clinical outcomes at 1 year in patients after cardiac arrest without signs of STEMI, compared with a delayed coronary angiography strategy.
Design, Setting, and Participants
A prespecified analysis of a multicenter, open-label, randomized clinical trial evaluated 552 patients who were enrolled in 19 Dutch centers between January 8, 2015, and July 17, 2018. The study included patients who experienced out-of-hospital cardiac arrest with a shockable rhythm who were successfully resuscitated without signs of STEMI. Follow-up was performed at 1 year. Data were analyzed, using the intention-to-treat principle, between August 29 and October 10, 2019.
Interventions
Immediate coronary angiography and PCI if indicated or coronary angiography and PCI if indicated, delayed until after neurologic recovery.
Main Outcomes and Measures
Survival, myocardial infarction, revascularization, implantable cardiac defibrillator shock, quality of life, hospitalization for heart failure, and the composite of death or myocardial infarction or revascularization after 1 year.
Results
At 1 year, data on 522 of 552 patients (94.6%) were available for analysis. Of these patients, 413 were men (79.1%); mean (SD) age was 65.4 (12.3) years. A total of 162 of 264 patients (61.4%) in the immediate angiography group and 165 of 258 patients (64.0%) in the delayed angiography group were alive (odds ratio, 0.90; 95% CI, 0.63-1.28). The composite end point of death, myocardial infarction, or repeated revascularization since the index hospitalization was met in 112 patients (42.9%) in the immediate group and 104 patients (40.6%) in the delayed group (odds ratio, 1.10; 95% CI, 0.77-1.56). No significant differences between the groups were observed for the other outcomes at 1-year follow-up. For example, the rate of ICD shocks was 20.4% in the immediate group and 16.2% in the delayed group (odds ratio, 1.32; 95% CI, 0.66-2.64).
Conclusions and Relevance
In this trial of patients successfully resuscitated after out-of-hospital cardiac arrest and without signs of STEMI, a strategy of immediate angiography was not found to be superior to a strategy of delayed angiography with respect to clinical outcomes at 1 year. Coronary angiography in this patient group can therefore be delayed until after neurologic recovery without affecting outcomes.
Trial Registration
trialregister.nl Identifier: NTR4973
This randomized clinical trial examines outcomes after 1 year in patients who received coronary angiography immediately after cardiac arrest vs those with angiography delayed until after neurologic recovery.
Introduction
Out-of-hospital cardiac arrest is a major global health care issue. The outcome of patients after cardiac arrest is poor. A previous study reported that approximately 40% of patients successfully resuscitated from cardiac arrest associated with ventricular fibrillation or pulseless ventricular tachycardia do not survive.1
Because ischemic heart disease is the most frequent cause of cardiac arrest and coronary artery disease has been reported in up to 70% of successfully resuscitated patients,2 it has been suggested that immediate coronary angiography and percutaneous coronary intervention (PCI), if necessary, should be considered in all patients after cardiac arrest, regardless of electrocardiogram (ECG) patterns.
Although, to our knowledge, it has never been studied in a randomized clinical trial, there is little debate about the role of immediate coronary angiography with PCI in patients who present with ST-segment elevation myocardial infarction (STEMI) and cardiac arrest.3,4 However, the role of immediate angiography in patients after cardiac arrest without STEMI is less clear.
The Coronary Angiography After Cardiac Arrest (COACT) trial was designed to test the hypothesis that, in patients successfully resuscitated after cardiac arrest in the absence of STEMI, a strategy of immediate coronary angiography and PCI, if necessary, results in better survival compared with a strategy of coronary angiography delayed until after neurologic recovery. However, no significant difference in 90-day survival was found between the 2 treatment groups.5 Nevertheless, the effects of immediate coronary angiography and PCI may improve long-term outcomes. Immediate PCI may prevent loss of myocardial function and, by doing so, might improve long-term mortality and morbidity. Furthermore, several observational studies have reported long-term benefit of an immediate angiography strategy on survival,6 and it has therefore been advocated that long-term data from randomized clinical trials are needed to further evaluate the role of immediate coronary angiography in this patient group.
Methods
Study Design
The COACT trial was an investigator-initiated, randomized, open-label, multicenter trial comparing immediate vs delayed coronary angiography in patients successfully resuscitated from cardiac arrest without ST-segment elevation on the ECG tracing. The trial design has been published previously.7 The protocol was developed by 3 of us (J.S.L., N.v.R., and H.M.O.-v.S.) and was approved by the steering committee and all relevant ethics committees. The trial protocol is available in Supplement 1. Participants provided informed consent and the study complied with the tenets of the Declaration of Helsinki.8 Participants did not receive financial compensation.
A clinical research organization (Clinical Research Unit Cardiology VUmc) was responsible for maintaining and monitoring the patient data. A data and safety monitoring committee oversaw the trial. An independent core laboratory, blinded to treatment allocation, evaluated all coronary angiography and PCI procedures. This study followed the Consolidated Standards of Reporting Trials (CONSORT) reporting guideline for randomized clinical trials.
Patients and Treatment
Patients were eligible for the study if they had an out-of-hospital cardiac arrest with an initial shockable rhythm and were unconscious after return of spontaneous circulation. Patients were excluded if they had signs of STEMI on the ECG performed in the emergency department, shock, or an obvious noncoronary cause of the arrest. Further inclusion and exclusion criteria and definitions are listed in the eAppendix in Supplement 2. For all enrolled patients, deferred informed consent was obtained with the use of a prespecified procedure (eAppendix in Supplement 2).
Eligible patients were randomized in a 1:1 ratio to either immediate or delayed coronary angiography using a web-based randomization system (Castor EDC). In patients allocated to the immediate coronary angiography group, the procedure was performed as soon as possible and was initiated within 2 hours after randomization. In the delayed coronary angiography group, the procedure was performed after neurologic recovery and, in general, following discharge from the intensive care unit. If a patient initially randomized to the delayed coronary angiography group showed signs of cardiogenic shock, recurrent life-threatening arrhythmias, or recurrent ischemia during their hospitalization, urgent coronary angiography was performed. The choice of anticoagulant and revascularization strategy was left to the discretion of the treating physicians, although it was recommended that treatment should be administered to all coronary lesions suspected of being unstable.
Further postresuscitation care was in line with the resuscitation guidelines.9 Targeted temperature management was initiated as soon as possible and according to local protocol. The approach to withdrawal of life-sustaining treatment for patients with persistent coma was not prespecified but was based on local practice in accordance with Dutch and European guidelines (eAppendix in Supplement 2).
Follow-up data were obtained by telephone interview at 1 year with the patient, family member, or from information acquired from the patient’s general physician. The follow-up was conducted by a member of the research team who was blinded to the treatment allocation. Any potential end point events were verified in a review of original medical records by the research team. In addition, death registries were searched to identify deaths. The primary end point of the trial was survival at 90 days; results associated with this outcome have been reported previously.5 For the 1-year analysis, results are reported for the following prespecified secondary outcomes: death, myocardial infarction since the index hospitalization, repeated revascularization since the index hospitalization, hospitalization for heart failure, and implantable cardiac defibrillator (ICD) shock. In addition, results are reported for the composite of death or myocardial infarction or any revascularization since the index hospitalization. Quality of life was assessed with the RAND-36 questionnaire (range, 0-100, where 0 indicates maximal disability and 100 indicates no limitations) at 1 year.10 A detailed description of the definitions of outcome measures is provided in the eAppendix in Supplement 2.
Statistical Analysis
The design and sample size calculation for the 90-day analysis have been described previously and are summarized in the eAppendix in Supplement 2.5,7 In the 1-year analysis presented herein, data were included for all patients who had the 1-year follow-up and did not retract consent. All analyses were performed according to the intention-to-treat principle. The 1-year event rates were calculated as percentages of patients who had an event within 1 year after randomization.
Effect sizes with 95% CIs are reported for the clinical outcomes, rather than P values, as all analyses presented herein are for secondary end points. Odds ratios (ORs) are reported for dichotomous outcomes. The ratio of geometric means is used as the effect size for skewed continuous data. All effect sizes reported are for immediate relative to delayed coronary angiography. A sensitivity analysis was performed to assess the robustness of the conclusions for the proportion of patients surviving at 1 year. A Kaplan-Meier curve is used to display cumulative survival over time separately in each intervention group with the hazard ratio reported as effect size. Statistical analysis was conducted using SPSS, version 26 (IBM Corp).
Results
Patients
Between January 8, 2015, and July 17, 2018, 552 patients who were successfully resuscitated from cardiac arrest and without ST-segment elevation shown on ECG were enrolled in the trial at 19 participating Dutch centers (Figure 1). Screening data were available during the final period of inclusion, when all centers were enrolling patients (eFigure 1 in Supplement 2). After exclusion of patients for whom informed consent was retrospectively refused, 538 patients (97.5%) were available for analysis of the primary end point of survival at 90 days. In addition, 13 patients refused consent for the 1-year follow-up and 3 patients were lost to follow-up. Data on 1-year vital status were available for 522 of the 552 patients (94.6%), of whom 264 were assigned to the immediate angiography group and 258 to the delayed angiography group. Of the 522 patients with available data, 413 were men (79.1%) and 109 were women (20.9%); mean (SD) age was 65.4 (12.3) years. The baseline characteristics are presented in Table 1.
Figure 1. Study Flowchart.

Inclusion, treatment allocation, informed consent procedure, and lost to follow-up of COACT participants from the start of the trial up to 1 year. COACT indicates Coronary Angiography After Cardiac Arrest; OHCA, out of hospital cardiac arrest; and ROSC, return of spontaneous circulation.
aThese patients received urgent intervention owing to conditions such as cardiogenic shock, recurrent life-threatening arrhythmias, or recurrent cardiac ischemia while waiting for coronary angiography.
Table 1. Baseline Characteristics of the Patients.
| Characteristic | No. (%) | |
|---|---|---|
| Immediate angiography group (n = 264) | Delayed angiography group (n = 258) | |
| Age, mean (SD), y | 65.8 (12.5) | 65.0 (12.2) |
| Sex | ||
| Men | 215 (81.4) | 198 (76.7) |
| Women | 49 (18.6) | 60 (23.3) |
| Hypertension | 128/260 (49.2) | 124/258 (48.1) |
| Previous event | ||
| Myocardial infarction | 70 (26.5) | 74 (28.7) |
| CABG | 41/263 (15.6) | 24/258 (9.3) |
| PCI | 44/263 (16.7) | 59/257 (23.0) |
| Coronary artery disease | 94 (35.6) | 94 (36.4) |
| Cerebrovascular accident | 19/263 (7.2) | 15/258 (5.8) |
| Diabetes | 54/263 (20.5) | 42/258 (16.3) |
| Current smoker | 47/240 (19.6) | 64/242 (26.4) |
| Hypercholesterolemia | 69/261 (26.4) | 76/256 (29.7) |
| Peripheral artery disease | 16/263 (6.1) | 22/258 (8.5) |
| Arrest witnessed | 210 (79.5) | 198 (76.7) |
| Time from arrest to, median (IQR), min | ||
| Basic life support | 2 (1 to 5) | 2 (1 to 5) |
| Return of spontaneous circulation | 15 (8 to 20) | 15 (8 to 20) |
| Signs of ischemia on ECGa | 162/253 (64.0) | 167/241 (69.3) |
| GCS score at admission, median (IQR)b | 3 (3 to 3) | 3 (3 to 3) |
| APACHE IV score, mean (SD)c | 107 (28) | 105 (32) |
| Baseline laboratory values | ||
| pH, mean (SD) | 7.2 (0.1) | 7.2 (0.1) |
| Lactic acid, median (IQR), mEq/L | 5.2 (3.0-8.8) | 4.9 (2.8-8.1) |
| Bicarbonate, mean (SD), mEq/L | 19.4 (4.4) | 19.0 (4.5) |
| Base excess | −7.5 (6.3) | −7.8 (6.2) |
| Partial pressure of oxygen, median (IQR), kPa | 14.7 (9.0-27.2) | 15.4 (10.2-28.8) |
| Creatinine, median (IQR), mg/dL | 1.15 (1.02-1.34) | 1.14 (0.98-1.29) |
| Creatine kinase, median (IQR), U/L | 164 (118-252) | 167 (118-253) |
| Creatine kinase MB, median (IQR), ng/L | 6.1 (4.0-13.8) | 6.3 (3.7-19.9) |
| Troponin T, median (IQR), ng/mL | 0.044 (0.029-0.082) | 0.053 (0.026- 0.117) |
Abbreviations: APACHE, Acute Physiology and Chronic Health Evaluation; CABG, coronary artery bypass graft; ECG, electrocardiography; GCS, Glasgow Coma Scale; IQR, interquartile range; PCI, percutaneous coronary intervention.
SI conversion factors: To convert bicarbonate to millimoles per liter, multiply by 1; creatine kinase to microkatals per liter, multiply by 0.0167; creatine kinase MB fraction to micrograms per liter, multiply by 1; creatinine to micromoles per liter, multiply by 88.4; lactic acid to millimoles per liter, multiply by 1; and troponin T to micrograms per liter, multiply by 1.
Signs of ischemia on ECG are defined as depressions of 1 mm or more in 2 contiguous leads, T-wave inversion in 2 contiguous leads, or both.
GCS scores range from 3 to 15, with lower scores indicating a reduced level of consciousness.
APACHE IV scores range from 0 to 286, with higher scores indicating a higher risk of death.
Treatment
Procedural and treatment characteristics are reported in Table 2 and eTables 1, 2, and 3 in Supplement 2. Coronary angiography was performed in 256 patients (97.0%) in the immediate group and 167 patients (64.7%) in the delayed group. The median time from randomization to coronary angiography was 0.9 (interquartile range [IQR], 0.6-1.2) hours in the immediate group and 119.9 (IQR, 47.7-200.2) hours in the delayed group. An acute thrombotic occlusion was found in 3.1% of patients (8 of 256) in the immediate group and 7.8% of patients (13 of 167) in the delayed group. Chronic total occlusion in one of the coronary arteries was found in 37.5% of patients (96 of 256) in the immediate group and 34.7% of patients (58 of 167) in the delayed group. The rate of PCI was 32.6% (86 of 264) in the immediate group and 24.4% (63 of 258) in the delayed group. Coronary artery bypass graft was performed in 6.1% of patients (16 of 264) in the immediate group and 8.1% of patients (21 of 258) in the delayed group. Patients randomized to the immediate group were more often treated with a glycoprotein IIb/IIIa inhibitor (immediate: 6.4% vs delayed: 2.7%), while patients randomized to delayed angiography were more likely to be treated with salicylates (immediate: 76.1% vs delayed: 87.2%) and/or a P2Y12 inhibitor (immediate: 57.6% vs delayed: 71.3%) (eTable 1 in Supplement 2).
Table 2. Procedural and Treatment Characteristics.
| Characteristic | Angiography group, No. (%) | |
|---|---|---|
| Immediate (n = 264) | Delayed (n = 258) | |
| Coronary angiography performed | 256 (97.0) | 167 (64.7)a |
| Time from arrest to coronary angiography, median (IQR), h | 2.1 (1.5-2.8) | 121.4 (50.4-201.4) |
| Time randomization to coronary angiography, median (IQR), h | 0.9 (0.6-1.2) | 119.9 (47.7-200.2) |
| Coronary artery disease severity | ||
| No clinically significant disease | 92/256 (35.9) | 57/167 (34.1) |
| 1-Vessel disease | 69/256 (27.0) | 48/167 (28.7) |
| 2-Vessel disease | 53/256 (20.7) | 34/167 (20.4) |
| 3-Vessel disease | 42/256 (16.4) | 28/167 (16.8) |
| Acute unstable lesion | 33/256 (12.9) | 27/167 (16.2) |
| Acute thrombotic occlusion | 8/256 (3.1) | 13/167 (7.8)b |
| Chronic total occlusion | 96/256 (37.5) | 58/167 (34.7) |
| Revascularization treatment | ||
| PCI | 86 (32.6) | 63 (24.4) |
| CABG | 16 (6.1) | 21 (8.1) |
| Pharmacologic or conservative treatment | 164 (62.1) | 174 (67.4) |
Abbreviations: CABG, coronary artery bypass graft; IQR, interquartile range; PCI, percutaneous coronary intervention.
Thirty-five of these patients underwent urgent intervention owing to cardiac deterioration.
Six of these patients underwent urgent intervention owing to cardiac deterioration.
Over 90% of patients in each group were treated with targeted temperature management and mechanical ventilation. Median time to target temperature for those receiving this treatment was 5.5 (IQR, 2.9-8.6) hours in the immediate group and 4.7 (IQR, 2.6-7.5) hours in the delayed group. Details on withdrawal of life-sustaining treatment are given in eTable 4 in Supplement 2.
End Points
As reported previously,5 no significant difference was found for the primary outcome of the trial—survival at 90 days—with 176 of 273 patients (64.5%) surviving in the immediate coronary angiography group compared with 178 of 265 patients (67.2%) in the delayed group (OR, 0.89; 0.62-1.27; P = .51). Clinical outcomes at 1 year are reported in Table 3. At 1 year, survival was met in 162 of 264 patients (61.4%) in the immediate group and 165 of 258 patients (64.0%) in the delayed group, yielding an effect size similar to that for survival at 90 days (OR, 0.90; CI, 0.63-1.28) (Table 3). The sensitivity analysis for survival at 1 year showed no significant difference between the groups (eAppendix, eTable 5 in Supplement 2). In a post hoc landmark analysis, the hazard ratio for mortality between 90 days and 1 year was 0.85 (95% CI, 0.26-2.87). Mortality between 90 days and 1 year was 2.2% in our study. Mortality between 90 days and 1 year was 1.90% in the immediate group and 2.3% in the delayed group (Figure 2). In an additional analysis accounting for clustering of patients within hospitals, the OR for 1-year survival was 0.89 (95% CI, 0.62-1.29). Furthermore, in a per protocol analysis that excluded crossovers, the OR for 1 year was 0.92 (95% CI, 0.64-1.32).
Table 3. Clinical Outcomes at 1-Year Follow-up.
| Outcome | Angiography group, No. (%) | Effect size (95% CI)a | |
|---|---|---|---|
| Immediate (n = 264) | Delayed (n = 258) | ||
| Survival | 162 (61.4) | 165 (64.0) | 0.90 (0.63-1.28) |
| Myocardial infarction since index hospitalization | 2/264 (0.8) | 1/258 (0.4) | 1.96 (0.18-21.8) |
| Any revascularization since index hospitalization | 10/264 (3.8) | 10/258 (3.9) | 0.98 (0.40-2.39) |
| Any PCI since index hospitalization | 8/264 (3.0) | 8/258 (3.1) | 0.98 (0.36-2.64) |
| Repeated PCI of the previously treated culprit lesion | 0/264 (0.0) | 3/258 (1.2) | NA |
| Any CABG since index hospitalization | 2/264 (0.8) | 2/258 (0.8) | 0.98 (0.14-6.99) |
| CABG of the previous treated culprit lesion | 1/264 (0.4) | 0/258 (0.0) | NA |
| Hospitalization due to heart failure since index hospitalization | 2/264 (0.8) | 1/258 (0.4) | 1.96 (0.18-21.8) |
| ICD implantation since index hospitalization | 8/264 (3.0) | 4/258 (1.6) | 1.98 (0.59-6.67) |
| ICD shock | 23/113 (20.4) | 17/105 (16.2) | 1.32 (0.66-2.64) |
| If yes, No. of times (different days) | 0.82 (0.56-1.22)b | ||
| Median (IQR) | 1 (1-1) | 1 (1-2) | |
| Geometric means | 1.3 (1.0-1.6) | 1.5 (1.1-2.1) | |
| Appropriate ICD shock | 19/23 (82.6) | 12/17 (70.6) | 1.60 (0.72-3.58) |
| Composite of death, revascularization, or myocardial infarction after index hospitalization | 112/261 (42.9) | 104/256 (40.6) | 1.10 (0.77-1.56) |
Abbreviations: CABG; coronary artery bypass grafting; ICD, implantable cardioverter-defibrillator; IQR, interquartile range; NA, not applicable; PCI, percutaneous coronary intervention.
The effect size is the odds ratio of unless otherwise noted. The delayed angiography group is used as the reference group for odds ratios of geometric means. The 95% CIs for the secondary end points were not adjusted for multiplicity; therefore, inferences drawn from these intervals may not be reproducible.
Ratio of geometric means.
Figure 2. Estimates of Survival Among Patients Who Underwent Immediate or Delayed Coronary Angiography After Cardiac Arrest.
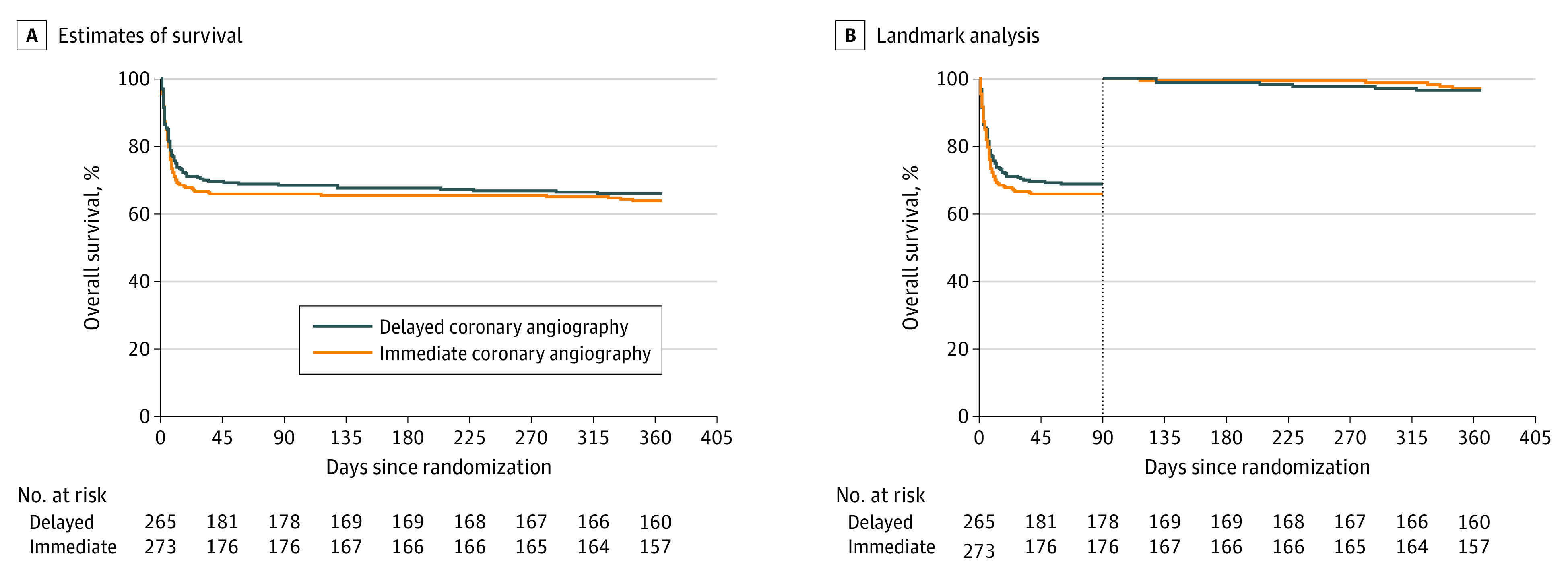
A, Estimates of survival: hazard ratio (HR) for death, 1.09 (95% CI, 0.83-1.45). B, Landmark analysis: HR for death from 0 to 90 days, 1.11 (95% CI, 0.83-1.49), and HR for death from 90 days to 1 year, 0.85 (95% CI, 0.26-2.78).
Myocardial infarction since the index hospitalization occurred in 2 patients (0.8%) in the immediate group and 1 patient (0.4%) in the delayed group. Since the index hospitalization, PCI was performed in 8 patients (3.0%) in the immediate group and 8 patients (3.1%) in the delayed group. Coronary artery bypass grafting of the previously treated lesion since the index hospitalization was performed in 1 patient (0.4%) in the immediate group and none in the delayed group. The end point of hospitalization due to heart failure was met in 2 patients (0.8%) in the immediate group and 1 patient (0.4%) in the delayed group. Twenty-three of 113 patients (20.4%) with an ICD in the immediate group and 17 of 105 patients (16.5%) with an ICD in the delayed group had received a shock. The composite end point of death, myocardial infarction, or repeated revascularization since the index hospitalization was met in 112 of 261 patients (42.9%) in the immediate group and 104 of 256 patients (40.6%) in the delayed group.
Quality-of-life scores were obtained for 235 of the 329 patients who survived until 1 year. Median for the RAND-36 physical component score was 49.2 (IQR, 42.2-55.3) in the immediate group and 50.4 (IQR, 44.9-55.2) in the delayed group. For the RAND-36 mental component score, the medians were 51.3 (IQR, 42.4-56.4) in the immediate group and 50.0 (IQR, 42.8-56.2) in the delayed group (eTable 6 and eFigure 2 in Supplement 2).
Discussion
The COACT multicenter, randomized clinical trial compared immediate coronary angiography with delayed coronary angiography in patients successfully resuscitated from out-of-hospital cardiac arrest without ST-segment elevation on the ECG and in the absence of an obvious noncoronary cause of the arrest. In the COACT trial, 90-day survival did not differ significantly between the 2 treatment strategies.5 In the analyses reported herein, we found no significant difference in survival at 1 year between the immediate and delayed coronary angiography groups. Furthermore, we observed similar rates of myocardial infarction, revascularization, hospitalization for heart failure, or ICD shock since the index hospitalization in the 2 groups.
The results of this study show that mortality primarily occurs during the first 90 days after the arrest. Mortality between 90 days and 1 year was 2.2% in our study. This incidence is in line with a previous report that showed that patients after cardiac arrest have a relatively favorable-long term survival after discharge from hospital.11
Our study, however, could not confirm the findings of previous observational studies,6 which found survival benefit at 1 year for resuscitated patients without STEMI who were treated with immediate coronary angiography. This difference could be related to the observational design of these previous studies, resulting in the risk of potential selection bias by choosing patients with a presumed better prognosis for an immediate angiography strategy.
Our results are consistent with those of randomized clinical trials addressing the role of immediate vs delayed coronary angiography in patients with myocardial infarction without ST-segment elevation and who had not presented with cardiac arrest, which also showed no benefit of immediate angiography on long-term survival.12,13,14
The occurrence of myocardial infarction after index hospitalization was not significantly different and was low in both groups during the 1-year follow-up of our study. This low level can be the result of competing risks. After cardiac arrest resuscitation, patients have a high risk of death before hospital discharge and might, therefore, not survive long enough for heart failure or myocardial infarction to occur. Another explanation is that, although coronary artery disease was found in almost two-thirds of the patients in our study, most patients had stable coronary lesions, with thrombotic occlusions being encountered in only 5% of patients, which might translate to low risk of future coronary events.
Patients in the immediate group were more likely to receive PCI during the index hospitalization than those in the delayed group, but this difference did not result in more PCI in the delayed group in the period following the index hospitalization. The rates of revascularization since the index hospitalization were low in both groups, which is likely related to the relatively stable nature of the atherosclerotic disease in this patient group as discussed above.
Hospitalization for heart failure occurred in similar low rates in the immediate and delayed angiography groups. Myocardial injury and infarct size have shown to be good predictors of subsequent heart failure and long-term outcome.15 In the COACT trial, no significant difference was found in the levels of cardiac markers during the index hospitalization between the 2 treatment groups, which could explain the neutral outcome of the 1-year results with regard to hospitalization for heart failure.5 Still, it is an unexpectedly low rate, confirming the current improved clinical prognosis in patients who survive out-of-hospital cardiac arrest.
In the COACT study, the rate of appropriate ICD shock did not differ significantly between the 2 groups.5 Approximately 14% of patients with an ICD in our trial received an appropriate shock in the first year of follow-up, which is in line with rates reported previously.16 This percentage reflects the high-risk study population of survivors of cardiac arrest but might be increased by the high prevalence of chronic total coronary artery occlusions. Such chronic total occlusions are often accompanied by large areas of myocardial scar and ischemia17 and have been shown to increase the risk of ventricular tachycardia in patients with an ICD after cardiac arrest.18
Limitations
Our trial has several limitations. All of the outcomes in the 1-year analysis are exploratory, as the COACT trial was powered for the 90-day analysis of the primary end point. We acquired data only on patient screening during the final phase of the trial. Owing to the nature of the study, we could not blind physicians to the allocated treatment arm, which might have influenced subsequent treatment. Our results do not apply to patients with shock, severe renal dysfunction, or persistent ST-segment elevation since these conditions were excluded from our trial. No data on medical therapy during follow-up were available. In addition, because of withdrawal of consent, data on 5.4% of randomized patients could not be analyzed at 1 year.
Conclusions
In this randomized clinical trial of patients who were successfully resuscitated from out-of-hospital cardiac arrest and without signs of STEMI, an immediate angiography strategy did not improve 1-year clinical outcomes compared with a delayed angiography strategy.
Trial Protocol
eAppendix. Detailed Trial Characteristics
eFigure 1. Screening Sample
eTable 1. Supplementary Procedural and Treatment Characteristics
eTable 2. Reasons for Crossover
eTable 3. Urgent CAG in Patients From the Delayed Invasive Strategy
eTable 4. Reasons for Withdrawal of Life-Sustaining Treatment
eTable 5. Sensitivity Analysis of Survival at 1 Year
eTable 6. RAND-36 Questionnaire
eFigure 2. RAND-36 Questionnaire: Physical and Mental Summary Scores
eReferences
Supplement 3. Data Sharing Statement
References
- 1.Patel N, Patel NJ, Macon CJ, et al. . Trends and outcomes of coronary angiography and percutaneous coronary intervention after out-of-hospital cardiac arrest associated with ventricular fibrillation or pulseless ventricular tachycardia. JAMA Cardiol. 2016;1(8):890-899. doi: 10.1001/jamacardio.2016.2860 [DOI] [PubMed] [Google Scholar]
- 2.Spaulding CM, Joly LM, Rosenberg A, et al. . Immediate coronary angiography in survivors of out-of-hospital cardiac arrest. N Engl J Med. 1997;336(23):1629-1633. doi: 10.1056/NEJM199706053362302 [DOI] [PubMed] [Google Scholar]
- 3.Ibanez B, James S, Agewall S, et al. . ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2017;2017.27941012 [Google Scholar]
- 4.O’Gara PT, Kushner FG, Ascheim DD, et al. . 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;61(4):e78-e140. doi: 10.1016/j.jacc.2012.11.019 [DOI] [PubMed] [Google Scholar]
- 5.Lemkes JS, Janssens GN, van der Hoeven NW, et al. . Coronary angiography after cardiac arrest without ST-segment elevation. N Engl J Med. 2019;380(15):1397-1407. doi: 10.1056/NEJMoa1816897 [DOI] [PubMed] [Google Scholar]
- 6.Khan MS, Shah SMM, Mubashir A, et al. . Early coronary angiography in patients resuscitated from out of hospital cardiac arrest without ST-segment elevation: a systematic review and meta-analysis. Resuscitation. 2017;121:127-134. doi: 10.1016/j.resuscitation.2017.10.019 [DOI] [PubMed] [Google Scholar]
- 7.Lemkes JS, Janssens GN, Straaten HM, et al. ; COACT investigators . Coronary angiography after cardiac arrest: rationale and design of the COACT trial. Am Heart J. 2016;180:39-45. doi: 10.1016/j.ahj.2016.06.025 [DOI] [PubMed] [Google Scholar]
- 8.World Medical Association World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191-2194. . doi: 10.1001/jama.2013.281053 [DOI] [PubMed] [Google Scholar]
- 9.Nolan JP, Soar J, Cariou A, et al. ; European Resuscitation Council; European Society of Intensive Care Medicine . European Resuscitation Council and European Society of Intensive Care Medicine 2015 guidelines for post-resuscitation care. Intensive Care Med. 2015;41(12):2039-2056. doi: 10.1007/s00134-015-4051-3 [DOI] [PubMed] [Google Scholar]
- 10.Hays RD, Sherbourne CD, Mazel RM. The RAND 36-Item Health Survey 1.0. Health Econ. 1993;2(3):217-227. doi: 10.1002/hec.4730020305 [DOI] [PubMed] [Google Scholar]
- 11.Andrew E, Nehme Z, Wolfe R, Bernard S, Smith K. Long-term survival following out-of-hospital cardiac arrest. Heart. 2017;103(14):1104-1110. doi: 10.1136/heartjnl-2016-310485 [DOI] [PubMed] [Google Scholar]
- 12.Thiele H, Rach J, Klein N, et al. ; LIPSIA-NSTEMI Trial Group . Optimal timing of invasive angiography in stable non-ST-elevation myocardial infarction: the Leipzig Immediate versus early and late PercutaneouS coronary Intervention triAl in NSTEMI (LIPSIA-NSTEMI Trial). Eur Heart J. 2012;33(16):2035-2043. doi: 10.1093/eurheartj/ehr418 [DOI] [PubMed] [Google Scholar]
- 13.Riezebos RK, Ronner E, Ter Bals E, et al. ; OPTIMA trial . Immediate versus deferred coronary angioplasty in non–ST-segment elevation acute coronary syndromes. Heart. 2009;95(10):807-812. doi: 10.1136/hrt.2008.154815 [DOI] [PubMed] [Google Scholar]
- 14.Milasinovic D, Milosevic A, Vasiljevic-Pokrajcic Z, et al. . Three-year impact of immediate invasive strategy in patients with non–ST-segment elevation myocardial infarction (from the RIDDLE-NSTEMI Study). Am J Cardiol. 2018;122(1):54-60. doi: 10.1016/j.amjcard.2018.03.006 [DOI] [PubMed] [Google Scholar]
- 15.Thygesen K, Alpert JS, Jaffe AS, et al. ; Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction . Fourth universal definition of myocardial infarction (2018). J Am Coll Cardiol. 2018;72(18):2231-2264. doi: 10.1016/j.jacc.2018.08.1038 [DOI] [PubMed] [Google Scholar]
- 16.van Welsenes GH, van Rees JB, Borleffs CJ, et al. . Long-term follow-up of primary and secondary prevention implantable cardioverter defibrillator patients. Europace. 2011;13(3):389-394. doi: 10.1093/europace/euq494 [DOI] [PubMed] [Google Scholar]
- 17.Stuijfzand WJ, Biesbroek PS, Raijmakers PG, et al. . Effects of successful percutaneous coronary intervention of chronic total occlusions on myocardial perfusion and left ventricular function. EuroIntervention. 2017;13(3):345-354. doi: 10.4244/EIJ-D-16-01014 [DOI] [PubMed] [Google Scholar]
- 18.Nombela-Franco L, Iannaccone M, Anguera I, et al. . Impact of chronic total coronary occlusion on recurrence of ventricular arrhythmias in ischemic secondary prevention implantable cardioverter-defibrillator recipients (VACTO secondary study): insights from coronary angiogram and electrogram analysis. JACC Cardiovasc Interv. 2017;10(9):879-888. doi: 10.1016/j.jcin.2017.02.008 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Trial Protocol
eAppendix. Detailed Trial Characteristics
eFigure 1. Screening Sample
eTable 1. Supplementary Procedural and Treatment Characteristics
eTable 2. Reasons for Crossover
eTable 3. Urgent CAG in Patients From the Delayed Invasive Strategy
eTable 4. Reasons for Withdrawal of Life-Sustaining Treatment
eTable 5. Sensitivity Analysis of Survival at 1 Year
eTable 6. RAND-36 Questionnaire
eFigure 2. RAND-36 Questionnaire: Physical and Mental Summary Scores
eReferences
Supplement 3. Data Sharing Statement