

Background:
Attaining a straight dorsum in patients with deviated nose is a main task in rhinoplasty. The basis of this difficulty is the presence of multiple anatomical abnormalities; hence, many methods are used to correct such a deformity. In this study, a sequential comprehensive surgical approach is proposed for the correction of deviated nose.
Methods:
Seventy-six patients who presented with developmental or posttraumatic external nasal deviation were enrolled in this study. All patients were subjected to open septorhinoplasty using a systematic approach. The outcome was assessed throughout for patient satisfaction.
Results:
The postoperative course was uneventful. Minor complications were encountered as transient hypoesthesia in the nasal tip in 4 patients and as prolonged tip edema in 10 patients. Residual significant nasal deviation was observed in 3 patients, and only 1 of them necessitated revision. All patients reported improvement of their nasal airway, and the percentages of their aesthetic satisfaction were as follows: very satisfied (n = 57, 75%), satisfied (n = 18, 23.7%), and unsatisfied (n = 1, 1.3%).
Conclusions:
A simple and comprehensive approach for correction of deviated nose is presented, which resulted in a better long-term cosmetic and functional outcome. This approach could correct the deviations in various anatomic locations, and helps the surgeon to deal with nasal deviation in an effective and straightforward manner wherever the pathology of deviation.
INTRODUCTION
Nasal deviation is one of the most challenging disfigurements faced in rhinoplasty. It represents a set of several anatomical distortions, the most severe and complex form of which is the deformation of the nasal septum.1,2 Deviation of the dorsal portion of the septum gives rise to both functional and aesthetic problems.3
The entire nasal pyramid could be involved in nasal deviation. Occasionally, deviations may be localized, with varying degrees of deformity to the upper, middle, or lower portion. Classification of the deviations would be of great benefit to analyze and categorize the pathologic deformities. Ellis and Gilbert4 used 3 classes for nasal deviation: at the nasion, at the level of rhinion, and a combination of both. Rohrich et al1 suggested 3 basic types of deviations: (1) caudal septal deviation, (2) concave dorsal deformity, and (3) concave/convex dorsal deformity. Nasal deviation is frequently related to nasal trauma5,6 but may be present since birth or may be associated with a cleft lip nasal deformity. Minor cartilage trauma early in life can lead to noticeable deformation with cartilage growth. Because of the complex and intimate relationship of the bony and cartilaginous framework of the nose, the effects of fractured nasal bones may spread to involve cartilaginous and bony septum, the upper lateral cartilages (ULC), and the alar cartilages, as well “dynamic concept.”7
Deviated nasal septum represents the foremost element in the deviated nose, as it forms the underpinning upon which the external nasal osseocartilaginous framework is built.2 As a result, septum surgery typically plays a vital role in the successful management of the externally deviated nose, and hence, combined septal and corrective rhinoplasty should be done in a single procedure. Even in the absence of functional problems, septal surgery may still be indicated to correct minor septal deviations that may hamper the correct configuration of external nasal pyramid.8
A deviated nose can typically be improved surgically, but the achievement of a perfectly straight nose is occasionally difficult. This is simply because of the diversity of nasal structures that are usually involved in this deformity. Furthermore, the force of scar contracture together with long-standing natural force offered in the cartilaginous structures and soft tissues influence the result. An extra factor that may cause recurrence of deviation even with complete and symmetric osteotomies is the imperfect correction of the nasal structures, particularly the deviated septum responsible for the original deviation.9–12
The objective of the study was to present our experience in treating deviated nose along with presenting an algorithm to address its management. Because of the dynamicity of septorhinoplasty procedure with our aim for standardization of the corrective techniques, we introduce this comprehensive approach. This approach could be efficiently used as a standard of care for correction of deviated nose.
PATIENTS AND METHODS
This is a retrospective study on 76 patients who presented with nasal deviation with variable degrees of nasal obstruction (Table 1). All patients were subjected to open septorhinoplasty using the same approach. Detailed medical history and physical examination were performed. A routine computed tomography scan was done. During follow-up visits, patients were assessed, stressing on the dorsum shape, position, or any residual deviation of the nose.
Table 1.
Demographic and Clinical Characteristics of Patients
| Characteristics | |
|---|---|
| Age | |
| Range | 18–55 y |
| Mean | 29 y |
| Sex | |
| Male | 43 patients |
| Female | 33 patients |
| Etiology of ND | |
| History of trauma | 35 patients (46%) |
| No history of trauma | 41 patients (54%) |
| Types of ND | |
| C-shaped | 42 patients (55.3%) |
| Straight | 20 patients (26.3%) |
| S-shaped | 14 patients (18.4%) |
| Airway obstruction | All patients complaining from obstruction with variable degrees |
| Sites of graft harvest | |
| Septal cartilage | 57 patients (75%) |
| Conchal cartilage | 11 patients (14.5%) |
| Costal cartilage | 8 patients (10.5%) |
| Follow-up duration | |
| Range | 6–50 mo |
| Mean | 15 mo |
ND, nasal deviation.
The patients’ postoperative satisfaction was assessed for 2 components: correction of deviation and improvement of airway. The data were documented and categorized into 3 categories, including very satisfied, satisfied, and unsatisfied. All patients provided a written consent for usage of their photographs in scholarly publications.
A sequential and comprehensive approach for management of nasal deviation was proposed (Fig. 1). Successful correction of nasal deviation requires all anatomic gears involved in this deformity to be effectively recognized and surgically realigned. For this reason, our approach to this difficult deformity is through these successive 6 steps. First is caudal septoplasty to manage caudal septal deviation. In our view, this is the key and the most vital building block in treating the deviated nose, as the caudal septum is a decisive structure providing support to the nasal tip. The second step is central septoplasty for correction of middle septal deviation. Excision involves the central part of quadrangular cartilage, with preservation of an “L-shaped” strut about 1–1.5 cm for nasal dorsum and tips support.3,13 The third step is cephalic septoplasty to correct the deviated upper vault. Optimal handling of osseocartilagenous junction is mandatory. This is simply obtained by excision of a deviated part of bony septum or by performing a green stick fracture to level it. The fourth step is straightening the bony nasal vault through osteotomies to produce controlled fractures in the nasal bones. Fifth step is scoring of the concave side of the dorsal and caudal L-strut to uncurl the deviated cartilage.3,14 The final step is cartilage grafting to support and maintain the straightened structures. Two types of grafts are used: spreader grafts15–18 and columellar strut.19–21 Spreader grafts can be considered the “workhorse” grafts, as they straighten and buttress weakened L-struts in a high dorsally deviated septum, recreate dorsal aesthetic lines, reconstruct a narrow middle vault, and restore the internal nasal valve function.17
Fig. 1.

Schematic diagram of the comprehensive approach used for correction of deviated nose. A, Exposure through marginal and stair-step incisions. B, Caudal, central, and cephalic septoplasty. C, Medial and lateral osteotomies. D, Scoring of the dorsal and caudal L-strut. E, Grafting in the form of spreader. F, Columellar strut.
Surgical Technique
A stair-step columellar incision, combined with bilateral marginal incisions, is made (Fig. 1A). Skin and soft tissues are elevated in the sub-SMAS (Superficial Musculo-Aponeurotic System) plane. The soft tissues over the bone vault are elevated in supra-periosteal plane. Next, component dorsal hump reduction for any coexisting hump is performed.22
The interdomal ligament and medial crura had to be separated (the area of membranous septum between the medial crura and caudal septum should be left intact as much as possible). The anterior septal angle is identified with soft tissue removal from between the medial crura down to the premaxilla. This provides excellent exposure of the caudal septum. Beginning at the anterior septal angle, strict submucoperichondrial and submucoperiosteal septal flaps are elevated bilaterally, then the ULCs are separated from the septum. Wide dissection of fibrous connections and ligaments around the anterior nasal spine allows the access to the caudal septum from the anterior septal angle to the nasal spine, maxillary crest, and nasal floor in this area. This also releases the buckling effects of the dense fascia over the septum, creates a pocket to accommodate the caudal septum in its new position, and affords an excellent exposure to the whole cartilaginous and bone septum. If the caudal septum needs shortening, then excision of overhanging part of cartilaginous septum is performed. A wedge resection from the posterior aspect of the caudal septum will disengage it from the maxillary crest and will liberate the tension on the cartilage. This will allow it to swing back to the midline (Figs. 1B, 2).23 Freeing the caudal septum from its attachments, including the maxillary crest even in the absence of caudal septal deviation, helps in straightening the deviated septum above by breaking its spring action.
Fig. 2.
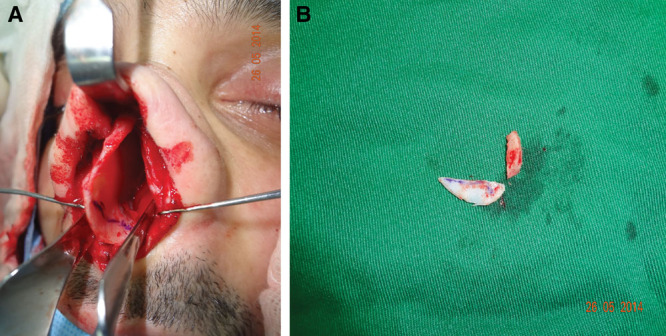
Caudal septoplasty involves disengaging the septum from the maxillary crest, excision of overhanging part of cartilaginous septum and a wedge from the posterior aspect, and release of tension in the cartilage to allow it to swing back to the midline. A, Marking of the overhanging caudal and posterior parts of the septum. B, The excised parts.
Central septoplasty of the middle septum is done. Typical resection of the deflected cartilage and osseocartilaginous junction with preservation of dorsal and caudal L-strut is performed (Figs. 1B, 3). In the absence of major mid-septal deviation, limited excision, cartilage weakening, and splinting might be used to correct these minimal deformities. The remaining deviated posterosuperior portion of perpendicular plate of ethmoid is corrected by judicious green stick fracture, with careful mobilization of the ethmoid plate to the midline, taking care not to fracture it superiorly. A long, straight, and broad instrument, as straight 10–15 mm osteotome, could be used for mobilization. In presence of severe deviation or spurs, it could be partially excised by Takahashi forceps. This is an important step not only for the correction of perpendicular plate of ethmoid but also to aid in aligning the bone pyramid. This will allow the free mobility of the nasal bone after osteotomy. We termed this step as “cephalic septoplasty”.
Fig. 3.

Central septoplasty involves resection of an appropriate amount of the deflected cartilage (A), and osseocartilaginous junction between quadrangular cartilage and perpendicular plate of ethmoid bone (B).
Alignment of the bone nasal vault is performed via medial and lateral osteotomies. Medial osteotomies are to be started at the junction of the upper lateral cartilage and nasal bones. A gentle fade of the osteotome by 15 degrees toward the medial canthus is advised. This safeguards the osteotome from passing through the frontal bone. Also, it avoids contour irregularities and formation of a “rocker deformity”.24 Then, lateral perforating osteotomies are completed percutaneously in a high–low–high fashion. Initially, the osteotomy should start high along the pyriform aperture (preserving the Webster triangle), then pass low along the ascending maxilla, and should go high again along the nasal bones superiorly (Fig. 1C). After osteotomies, slight ridges and asymmetries along the nasal bone can be reduced by rasping.
The residual deviation in the dorsal and caudal septum is corrected by scoring of the L-strut (Fig. 1D). Grafting is done after being prepared from the excised septal cartilage (Fig. 1E, F). If the septal cartilage is not enough, conchal or costal cartilages would be the alternative. Bilateral spreader grafts are used to provide stronger opposition to the cartilaginous memory. Asymmetric grafts are also used when indicated. The grafts are first secured to the septum using 5/0 monofilament absorbable horizontal mattress sutures and then secondarily to the ULCs. It is essential to gently spring the ULCs toward the anterior septal angle before reattaching them. This will guard against the risk of buckling of the ULCs during reattachment (Fig. 1E).
The second type of graft is the columellar strut, which is considered as an integral step in the open-surgery approach.19 The desired length from the anterior nasal spine to the columellar-lobular angle is about 15–20 mm. The pocket between the 2 medial crura should be narrow and just reaching the anterior nasal spine to accept the graft tightly. The base of the strut should touch the anterior nasal spine. With the strut in this position, the 2 medial crurae are advanced in posteroanterior and cephalo-caudal direction to the necessary position and projection. This technique allows precise, independent positioning, shaping, and stabilization of the medial crura for optimal contour and dome height symmetry (Fig. 1F).
Tip shaping and refinement with conservative cephalic trim of both lower lateral cartilages might be performed if there is any supratip fullness. Tip suturing to improve tip definition and correct intrinsic asymmetries are routinely done.25,26
Wound closure in a regular fashion is done. Bilateral extramucosal septal silicone splints are fixed in position with a through-and-through suture to support the cartilage while it heals.3 A small nonadherent nasal pack and nasal cast are applied as usual.
RESULTS
The postoperative course was uneventful. Minor complications were encountered as transient hypoesthesia in the nasal tip in 4 patients and as prolonged tip edema for up to 1 year in 10 patients (Table 2). Residual significant deviation was present in 3 patients, only one necessitated revision.
Table 2.
Satisfaction and Complications
| Patient satisfaction | |
| Very satisfied | 57 patients (75%) |
| Satisfied | 18 patients (23.7%) |
| Unsatisfied | 1 patient (1.3%) |
| Complications | |
| Transient hypoesthesia of nasal tip | 4 patients |
| Prolonged tip edema | 10 patients |
| Residual nasal deviation | 3 patients |
In terms of patient satisfaction, all patients reported improvement of their nasal airway and an almost straight, symmetrical nose. The percentages of their aesthetic satisfaction were as follows: very satisfied (n = 57, 75%), satisfied (n = 18, 23.7%), and unsatisfied (n = 1, 1.3%). In all patients, an almost straight nose with consistent tip support and adequate tip projection was achieved (Figs. 4, 5).
Fig. 4.

A and B, Preoperative views of a patient with posttraumatic right nasal deviation. C and D, Postoperative views of the patient’s face after 1 year, showing consistent satisfactory results.
Fig. 5.

A and B, Preoperative views of a patient with recurrent left nasal deviation. C and D, Postoperative views of the patient after 6 months, showing pleasing results.
DISCUSSION
Even though septoplasty is originally performed to treat breathing difficulties, it now becomes essential for correcting external nasal deviation. It represents a vital step in rhinoplasty surgery: septorhinoplasty. Even in patients with no functional problems, septoplasty may correspond to one solution for obtaining a proper realignment of the external nasal shape.27 If the numerous variables that contribute to nasal deviation are not properly identified and addressed, there is a high possibility of postoperative disappointment.28 Though there is an abundance of surgical techniques described to date that are aiming to straighten the nose and maximize nasal function with a stable long-term correction, correcting nasal deviation remains a difficult problem, and the recurrence rate of deviation remains high.
It is evident from the literature review that the abnormalities present in deviated nose can differ significantly from one patient to another. Hence, there is no universal technique that could be used for every case.29 Based on these notions, with expansion of our knowledge, in addition to an increased number of patients presented with nasal deviation, we suggested this comprehensive approach. It is considered an anatomical correction of deviated nose in a systematic way in all patients regardless of the etiology, location, and/or severity of the deviation.
Open approach is used as it provides direct and excellent access to the entire septum, with release of all mucoperichondrial and mucoperiosteal attachments to the septum, especially the deviated part. Furthermore, it allows separation of ULC from the dorsal septal cartilage under vision. All septal corrections and straightening techniques, including all harvesting procedures and graft insertion, can be easily accomplished.30,31 Our approach allows the surgeon to correct all anatomic components involved in the nasal deviation in a single stage, as the septoplasty constitutes a key element in surgical management of the deviated nose.32 This approach involves at least 4 steps to tackle the deviated septum: caudal septoplasty, central septoplasty, cephalic septoplasty, and spreader grafts. Consequently, it will produce an appropriate and consistent correction of the deviation.
In this study, the first and most important element toward correction of deviated nose was the caudal septoplasty, which involved a wide dissection and mobilization of the caudal septum to the midline in a “swinging door” fashion,33 with excision of the overhanging part. The described technique calls for creation of a wide pocket in the area of the anterior nasal spine and maxillary crest to allow the caudal septum to move toward the midline without any type of suture. Pastorek described his “modified swinging door” technique in which the caudal septum is flipped over the nasal spine, which acts as a doorstop holding the septum in the midline. A suture is then used to secure the septum to the nasal spine.34 Kridel describes the “tongue in groove” technique for the management of caudal deviations.35 This procedure would tend to shorten the nose and make stiffness in the area of membranous septum.
The second and third steps in our approach are central septoplasty and cephalic septoplasty. Cephalic septoplasty is as important as caudal septoplasty in correcting and preventing the recurrence of the deformity, especially in the upper third of the nose. It corrects deviated posterosuperior portion of perpendicular plate of ethmoid. When performing septoplasty in a deviated nose, we must free all the structures to avoid recurrence. We had to emphasize that we are performing 3 types of septoplasties: cephalic, central, and caudal. Each septoplasty type has its own implication for correction of the deviation, but if whichever missed it will typically end by recurrence.
The ULCs are affected to a greater degree than the nasal bones by high septal deviations. Grafting in the form of precise placement of spreader grafts will effectively lateralize the ULCs, widen the nasal valve areas and stenting the scored dorsal septal cartilage. Likewise, it can address concavities by boosting the concave side.31
Using open approach usually destabilizes the major supporting structures of the nasal tip. The use of columellar struts as an integral step in all patients is highly recommended, as it re-supports, improves, and maintains the tip shape, projection, and position in relation to the nasal dorsum without compromising the structural integrity or introducing additional visible grafts.19
Some authors have recommended the extracorporeal septum reconstruction.36–38 However, this technique has a problem: it compromises the structural role of the septum in nasal dorsum and tip support. If the septum can be straightened outside the nose, it could be straightened in situ as well.8 Using our technique, all septal jobs could be accurately tackled while the septum is in place, without affecting its structural integrity.
In the current study, all patients reported an improvement in breathing, with patient satisfaction around 98.7%. Secondary corrective procedures were minimized with this approach. The revision surgery was necessary in only 1 patient (1.3%). This is merely because of the checklist-minded approach by the operating surgeon using this technique. Moreover, it deals with the external nasal deviation found in the upper, middle, and lower thirds of the nose.
The main limitation of this study is the lack of an objective assessment of the outcome as we could not recall the whole study patients. By applying this technique, the surgeon will be organized to address all components of deviation. Nothing will be missed then. So, it will be easy to do the required steps according to the existing deformity. Certainly, it is not mandatory to perform the 6 steps in every single patient rather than to tailor the procedure according to the existing situation.
CONCLUSIONS
Deviated nose is a complex problem with a diversity of anatomical distortions. Management of deviated nose should involve recognition and correction of these underlying deformities. A simple and comprehensive 6-step approach is introduced here with improved cosmetic and functional outcomes. This sequential approach can alleviate the problems in each part involved in the deviation, which helps the surgeon to deal with it in an effective and straightforward manner. Based on this series, we would consider this technique as a standard systematic approach in the treatment of nasal deviation.
PATIENT CONSENT
Patients provided written consent for the use of their images.
Footnotes
Published online 20 August 2020.
Disclosure: The authors have no financial interest to declare in relation to the content of this article.
REFERENCES
- 1.Rohrich RJ, Gunter JP, Deuber MA, et al. The deviated nose: optimizing results using a simplified classification and algorithmic approach. Plast Reconstr Surg. 2002;110:1509. [DOI] [PubMed] [Google Scholar]
- 2.Dulcic Y, Hilger PA. Surgical correction of the deviated septum. Facial Plast Surg. 1999;7:319–331 [Google Scholar]
- 3.Gunter JP, Rohrich RJ. Management of the deviated nose. The importance of septal reconstruction. Clin Plast Surg. 1988;15:43–55 [PubMed] [Google Scholar]
- 4.Ellis DA, Gilbert RW. Analysis and correction of the crooked nose. J Otolaryngol. 1991;20:14–18 [PubMed] [Google Scholar]
- 5.Ramirez OM, Pozner JN. The severely twisted nose. Treatment by separation of its components and internal cartilage splinting. Clin Plast Surg. 1996;23:327–340 [PubMed] [Google Scholar]
- 6.Stucker JF., Jr Management of scoliotic nose. Laryngoscope. 1982;92:128–134 [DOI] [PubMed] [Google Scholar]
- 7.Guyuron B. Dynamics of rhinoplasty. Plast Reconstr Surg. 1991;88:970–978; discussion 979 [PubMed] [Google Scholar]
- 8.Foda HM. The role of septal surgery in management of the deviated nose. Plast Reconstr Surg. 2005;115:406–415 [DOI] [PubMed] [Google Scholar]
- 9.Antunes MB, Goldstein SA. Surgical approach to nasal valves and the midvault in patients with a crooked nose. Facial Plast Surg. 2011;27:422–436 [DOI] [PubMed] [Google Scholar]
- 10.Okur E, Yildirim I, Aydogan B, et al. Outcome of surgery for crooked nose: an objective method of evaluation. Aesthetic Plast Surg. 2004;28:203–207 [DOI] [PubMed] [Google Scholar]
- 11.Kim JK, Lee JS, Lee HM, et al. A simple technique for correcting the hump on a deviated nose. Aesthetic Plast Surg. 2006;30:686–688 [DOI] [PubMed] [Google Scholar]
- 12.Porter JP, Toriumi DM. Surgical techniques for management of the crooked nose. Aesthetic Plast Surg. 2002;26:suppl 118. [DOI] [PubMed] [Google Scholar]
- 13.Killian G. Die submukose Fensterresektion der Nasenscheidewand. Arch Laryng Rhin (Berlin). 1904;16:326–326 [Google Scholar]
- 14.Murakami WT, Wong LW, Davidson TM. Applications of the biomechanical behavior of cartilage to nasal septoplastic surgery. Laryngoscope. 1982;92:300–309 [DOI] [PubMed] [Google Scholar]
- 15.Sheen JH. Spreader graft: a method of reconstructing the roof of the middle nasal vault following rhinoplasty. Plast Reconstr Surg. 1984;73:230–239 [PubMed] [Google Scholar]
- 16.Sheen JH, Sheen AP. Aesthetic Rhinoplasty. 1987;St. Louis, Miss.: CV Mosby; [Google Scholar]
- 17.Rohrich RJ, Hollier LH. Use of spreader grafts in the external approach to rhinoplasty. Clin Plast Surg. 1996;23:255–262 [PubMed] [Google Scholar]
- 18.André RF, Paun SH, Vuyk HD. Endonasal spreader graft placement as treatment for internal nasal valve insufficiency: no need to divide the upper lateral cartilages from the septum. Arch Facial Plast Surg. 2004;6:36–40 [DOI] [PubMed] [Google Scholar]
- 19.Abu El-Wafa AM. Columellar strut: is it an integral step in primary rhinoplasty? Plast Reconstr Surg. 2013;131:119e–121e [DOI] [PubMed] [Google Scholar]
- 20.Rohrich RJ, Hoxworth RE, Kurkjian TJ. The role of the columellar strut in rhinoplasty: indications and rationale. Plast Reconstr Surg. 2012;129:118e–125e [DOI] [PubMed] [Google Scholar]
- 21.Anderson JR. New approach to rhinoplasty: a five-year reappraisal. Arch Otolarynol. 1971;93:284–291 [DOI] [PubMed] [Google Scholar]
- 22.Rohrich RJ, Muzaffar AR, Janis JE. Component dorsal hump reduction: the importance of maintaining dorsal aesthetic lines in rhinoplasty. Plast Reconstr Surg. 2004;114:1298–1308, discussion 1309 [DOI] [PubMed] [Google Scholar]
- 23.Wright WK. Principles of nasal septum reconstruction. Trans Am Acad Ophthalmol Otolaryngol. 1969;73:252–255 [PubMed] [Google Scholar]
- 24.Harshbarger RJ, Sullivan PK. The optimal medial osteotomy: a study of nasal bone thickness and fracture patterns. Plast Reconstr Surg. 2001;108:2114–2119; discussion 2120 [DOI] [PubMed] [Google Scholar]
- 25.Rohrich RJ, Adams WP., Jr The boxy nasal tip: classification and management based on alar cartilage suturing techniques. Plast Reconstr Surg. 2001;107:1849–1863; discussion 1864 [PubMed] [Google Scholar]
- 26.Rohrich RJ, Griffin JR. Correction of intrinsic nasal tip asymmetries in primary rhinoplasty. Plast Reconstr Surg. 2003;112:1699–1712, discussion 713 [DOI] [PubMed] [Google Scholar]
- 27.Parrilla C, Artuso A, Gallus R, et al. The role of septal surgery in cosmetic rhinoplasty. Acta Otorhinolaryngol Ital. 2013;33:146–153 [PMC free article] [PubMed] [Google Scholar]
- 28.Guyuron B, Behmand RA. Caudal nasal deviation. Plast Reconstr Surg. 2003;111:2449–2457; discussion 2458 [DOI] [PubMed] [Google Scholar]
- 29.Akbaş H, Keskin M, Güneren E, et al. Unilateral osteotomies for externally deviated noses. Aesthetic Plast Surg. 2002;26:413–415 [DOI] [PubMed] [Google Scholar]
- 30.Gunter JP. The merits of the open approach in rhinoplasty. Plast Reconstr Surg. 1997;99:863–867 [DOI] [PubMed] [Google Scholar]
- 31.Toriumi DM, Ries WR. Innovative surgical management of the crooked nose. Facial Plast Surg Clin North Am. 1993;1:63–78 [Google Scholar]
- 32.Vuyk HD. A review of practical guidelines for correction of the deviated, asymmetric nose. Rhinology. 2000;38:72–78 [PubMed] [Google Scholar]
- 33.Metzenbaum M. Dislocation of the lower end of the nasal septum cartilage. Arch Otolaryngol. 1936;24:78 [Google Scholar]
- 34.Pastorek NJ, Becker DG. Treating the caudal septal deflection. Arch Facial Plast Surg. 2000;2:217–220 [DOI] [PubMed] [Google Scholar]
- 35.Kridel RW, Scott BA, Foda HM. The tongue-in-groove technique in septorhinoplasty. A 10-year experience. Arch Facial Plast Surg. 1999;1:246–256; discussion 257 [DOI] [PubMed] [Google Scholar]
- 36.Vilar-Sancho B. Rhinoseptoplasty. Aesthetic Plast Surg. 1984;8:61–65 [DOI] [PubMed] [Google Scholar]
- 37.Rees TD. Surgical correction of the severely deviated nose by extramucosal excision of the osseocartilaginous septum and replacement as a free graft. Plast Reconstr Surg. 1986;78:320–330 [DOI] [PubMed] [Google Scholar]
- 38.Gubisch W. The extracorporeal septum plasty: a technique to correct difficult nasal deformities. Plast Reconstr Surg. 1995;95:672–682 [DOI] [PubMed] [Google Scholar]