

Abstract
The current obesity epidemic and inactive lifestyles of many Americans lead to health problems for millions of Americans and in turn, millions of dollars in medical bills. One aspect of this problem is the lack of physical activity that people engage in. Self-monitoring techniques have been used in the past to increase physical activity. However, there has not been a systematic review of the literature on this research to date. Furthermore, as technology that is user-friendly and assists in self-monitoring physical activity becomes more available to the public, it is important to investigate its use when used in conjunction with self-monitoring. The purpose of this review was to determine how self-monitoring techniques and technology have been applied to increase physical activity across multiple populations. A systematic review of the literature identified 19 articles. Results indicated that the majority of studies used more than one type of self-monitoring intervention. The most popular type of technology used with self-monitoring were fitness trackers. Future research should continue to examine the most effective methodologies that produce lasting behavior change in physical activity.
Keywords: physical activity, self-monitoring, goal-setting, technology, systematic review
The Center for Disease Control and Prevention (CDC) estimates that health-related issues due to inactivity such as higher mortality rate and cardiovascular disease result in $117 billion in medical costs annually (CDC, 2018; Piercy et al., 2018). In 2017, 36% of adults did not meet the minimum guidelines for moderate physical activity (PA) and 63% of adults did not meet the guidelines for vigorous-intense PA (CDC, 2018). Furthermore, the U.S. Department of Health and Human Services found that fewer than a quarter of the children between the years of 12 and 15 met the daily recommended guidelines for moderate-to-vigorous physical activity (Fakhouri, Hughes, Song, Fulton, & Ogden, 2014). According to the CDC, the vigorousness of physical activity is measured by the expenditure of metabolic equivalents (MET), a measure that estimates the level of oxygen used during an activity. An activity is defined as moderate when approximately 3–5.9 METs are burned (e.g., walking, hiking, yoga) and vigorous when METs exceed 6 during any activity (e.g., basketball, jogging, running, tennis; Ainsworth et al., 2000; CDC, 2017).
By applying self-monitoring interventions to the field of physical activity, there is a potential for people to meet these recommended requirements. Self-monitoring, goal-setting, self-recording, and feedback procedures are commonly used interventions in the field of applied behavior analysis (ABA). Self-monitoring is a recording procedure that involves an individual observing and recording his or her target behavior(s) (Cooper, Heron, & Heward, 2007). Self-monitoring has also been referred to as self-recording and self-observation, and is made up of several other self-monitoring interventions like goal-setting and feedback that are commonly used together as a treatment package (Smith & Ward, 2006). Goal-setting refers to creating a behavioral goal, and feedback refers to when an individual receives information from something or someone about a specific behavior or performance (Smith & Ward, 2006).
Self-monitoring procedures have yielded promising results in a variety of fields. For example, Hallahan, Lloyd, Kosiewicz, Kaufman, and Graves (1979) used a self-monitoring procedure with an elementary-age boy who had a learning disability to increase on-task behavior. Foxx and Axelroth (1983) instructed 12 participants to self-record and graph their daily nicotine intake, which resulted in major decreases in nicotine intake for as long as 12 months after the intervention was faded. Self-monitoring has also been used to decrease challenging behaviors, such as stereotypy in people with intellectual disabilities (Fritz, Iwata, Rolider, Camp, & Neidert, 2012).
The benefits of using self-monitoring are that few training sessions are needed, and it can be implemented by individuals without a background in behavior analysis, many of which individuals do daily (e.g., caloric intake, monitoring blood glucose, recording expenses in a checkbook). With advances in technology over the last 20 years, self-monitoring procedures are no longer limited to just pen and paper recordings. Clinicians and professionals can identify target behaviors and create goals with their clients during one session and later that evening can log onto a website or receive an email showing the data of target behavior (VanWormer, 2004). Not only is the availability of the data easier for the clinician or professional, but the recording process is often easier for the client. For example, pedometers were often inaccurate and only recorded steps taken but technology like Fitbits offer a more accurate measure of steps taken (Van Camp & Berth, 2018). Not only are Fitbits more reliable than pedometers, but they also can record more data such as the duration of time slept, percentage of time spent in a heart rate zone during a workout, and caloric intake.
Van Camp and Berth (2018) examined the validity of automated mechanical devices that measure physical activity and found that Fitbits were a reliable measure when compared to pedometers for counting daily steps. In addition, current technology allows the individual to create weight loss goals, such as how many steps are needed and the daily caloric intake that are required to reach a desired goal in a certain period of time. Furthermore, this type of technology allows clinicians to observe their clients’ physical activity data such as daily step count, calories burned, and heart rate, directly from their smartphone. This mode of data collection allows clinicians and professionals to unobtrusively and immediately observe client’s behavior without requiring them to be physically present and can provide immediate feedback via email or messages sent through the application. Finally, the accessibility to this technology for the general population drastically reduces the response effort of the individual to record and track their own behavior
Self-monitoring and technology lend themselves to the individual needs of people who regularly engage in physical activity. Although self-monitoring procedures and treatment packages have been effective at increasing physical activity (Donaldson & Normand, 2009; Kurti & Dallery, 2013), the literature on the use of self-monitoring procedures that use technology to assist in monitoring physical activity has not been systematically reviewed. The aim of this review was to examine how self-monitoring techniques have been used in conjunction with technology to increase physical activity in a variety of populations. In particular, the authors aim to identify trends in the use self-monitoring and technology to increase physical activity and the efficacy of treatments through success estimates.
Method
Inclusionary and Exclusionary Criteria
Articles that met the following criteria were included in the review: (1) published in a peer-reviewed journal, (2) used an experimental single subject design, (3) used original data, (4) the dependent variable (DV) was related to physical activity (e.g., daily step counts, number of circuits completed, pedometer steps), (5) the independent variable (IV) was a self-monitoring procedure, (6) a component of technology was used to either aid in the self-monitoring process or track physical activity (e.g., fitness tracker, pedometer, heart rate monitor, email), (7) the study was published between January 1971–March 29, 2019, and (8) the study was reported in English. Articles that failed to meet all inclusionary criteria were excluded. For example, if a study used a single subject design but could not demonstrate experimental control, such as a reversal to baseline (i.e., A-B design), the study was excluded. The rationale for the large timeframe was that there was no recent review of the literature and the authors wanted to capture anything that may have been used, therefore the 1970s were chosen as a start date. The reason multiple types of technology were chosen was because technology such as email is/was used in the feedback process related to the self-monitoring of participants.
Search Methods
An electronic search was conducted on March 8, 2017, using EBSCO MegaFile, PsychINFO, MEDLINE, SPORTDiscus Academic OneFile, Professional Development Collection, Scopus®, MasterFILE Premier, ERIC, Library, Information Science & Technology Abstracts, Teacher Reference Center, British Library ETHOS, British Source Premier, Alt HealthWatch, Communication & Mass Media Complete, Criminal Justice Abstracts, JSTOR Journals, Directory of Open Access Journals, Minority Health Archive, Digital Access to Scholarship at Harvard (DASH), and MAS Ultra-School Edition with a 45-year, 10-month boundary. The following search string was used: (“self control*” OR “self manage*” OR “self evaluation” OR “self instruct*” OR “self monitor*” OR “self record*” OR “self observ*” OR “self assess*”) AND (“physical activity” OR “exercise” OR “fitness” OR “sports” OR “work out” OR “athletic”) AND (“intervention”).
The search produced 1,685 articles without duplicates. An updated search using the same string was completed on March 29, 2019, using Academic Search elite, Eric, Health and Psychosocial instruments, Medline, PsycARTICLE, PsycINFO, and Sportdiscus with full text. This search produced 689 articles. In addition, the authors hand-searched the Journal of Applied Behavior Analysis from 1968 through 2019 for possible articles that met the inclusion criteria that may have been missed from the electronic search. This yielded no additional results.
Coding
Screening
The authors read the titles and abstracts of all 1,987 articles. Articles were included if their titles and abstracts met the inclusion criteria. This procedure produced 77 articles. After further review, 69 articles were excluded because they failed meet all inclusionary criteria. Eight articles met all inclusionary criteria. Following a forward search and harvesting references of the included articles, 11 articles were added, which resulted in 19 articles and 20 total studies. Kurti and Dallery (2013) included two studies and were coded as Kurti and Dallery (2013a) and Kurti and Dallery (2013b). Seven articles were excluded because they did not demonstrate experimental control (i.e., A-B or pre- and posttest designs). Figure 1 illustrates the screening process.
Fig. 1.
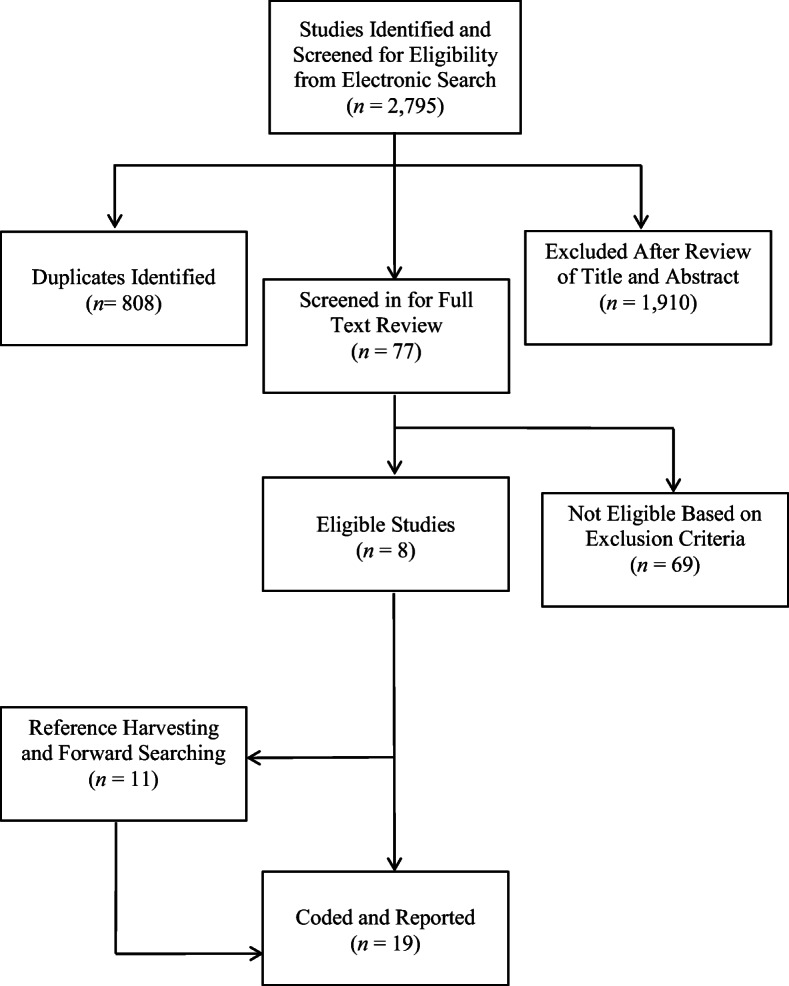
Flow chart of article selection process
Coding
Nineteen articles were coded on the following variables: number of participants, participants age, participants gender, self-monitoring procedure used, dependent variable, type of physical activity, technology, maintenance, and success estimate.
Self-monitoring and technology were coded using categories to capture the different interventions and types of devices. The self-monitoring categories were divided into three groups that are commonly used as self-monitoring interventions in both behavior-analytic literature (see Kazdin, 1974; Normand, 2008) and in ABA textbooks (see Cooper et al., 2007): goal-setting (GS), self-recording (SR), and multiple (M; e.g., goal-setting and feedback). The authors decided to divide self-monitoring into different categories to better define what was being used as an intervention. Not all researchers used the same aspects of self-monitoring, such as goal-setting, but still labeled the program as self-monitoring.
The technology category was divided into four labels: fitness tracker (FT), device (D), heart rate monitor (HRM), and multiple (M). First, the label FT encompassed any type of wearable fitness apparatus (e.g., a Fitbit or Nike Sport Band) that could record multiple forms of variables related to physical activity (e.g., daily steps, heart rate, intensity of workout). The D category refers to larger pieces of technology (e.g., iPods, iPads, computers). Any apparatus that only measured heart rate was coded as HRM. Finally, the label M was given if multiple pieces of technology were used in conjunction (e.g., FT and D).
Success estimates were determined by using visual analysis (i.e., inspection of the trend, variability, and level of the results), and a ratio of successful implementations of the independent variable to the total number of implementations attempted multiplied by 100 was reported (Reichow & Volkmar, 2010). The success estimate was used because it illustrates the consistency of replication of the independent variable in a study. Therefore, a successful intervention would have a high success estimate (e.g., 100%), whereas an unsuccessful intervention would have a low success estimate (e.g., less than 60%).
Interrater Reliability
Interrater reliability (IRR) data were collected by secondary authors. The secondary authors were given a template of all the variables and provided examples. Training was completed in one 30 min session by the first author, who modeled how to use the templated and answered any questions. IRR was calculated by dividing the number of agreements by the number of agreements plus disagreements and multiplied by 100. There were three phases of IRR. First at the screening process, all articles that were included in this review, and all the variables that were coded. Agreement was calculated for 35% (1,100) of the articles during the screening process. IRR for the screening process was 98%. Agreement was then calculated for 100% of all articles included in the review, and the variables that were coded. The IRR for articles included in this review was 99%. Finally, IRR was 95% for the variables that were coded.
Results
A total of 19 articles met all inclusionary criteria, resulting in 20 studies. Table 1 summarizes the coded variables of the included studies. The number of participants ranged from two (Hustyi, Normand, & Larson, 2011) to 30 (Kuhl, Rudrud, Witts, & Schulze, 2015). Participant ages ranged from 4 years old (Hustyi et al., 2011) to 71 years old (Kurti & Dallery, 2013). Studies included a variety of male and female participants. Studies included a combination of only females (Hayes & Van Camp, 2015; Wack, Crosland, & Miltenberger, 2014), only males (Valbuena, Miltenberger, Livingston, & Slattery, 2019), and both (e.g., Donaldson & Normand, 2009; Kuhl et al., 2015). The most common self-monitoring procedure used throughout the studies were multiple forms used in conjunction at 70% of the studies coded. One of the most popular types of technology that was used was FT, with 55% of the articles using them to self-monitor.
Table 1.
Summarized Results
| Citation | Gender of Participants | Age Range (y.o) | Category of Self-Monitoring | Dependent Variable | Type of Physical Activity | Category of Technology | Behavior Maintenance | Success Estimate |
|---|---|---|---|---|---|---|---|---|
| Bassette et al. (2018) | 1M 2F | 18–21 | GS | Percentage of steps completed independently | Squat, hip extension, dumbbell push-up, row | M | - | 100% |
| Cushing et al. (2011) | 3F | 14–18 | M | Percentage of goal attainment | - | D | - | 67% |
| Donaldson & Normand (2009) | 3M 2F | 44–54 | M | Daily caloric expenditure | - | M | Y | 72% |
| Galbraith & Normand (2017) | 8M 9F | 8–9 | M | Average number of steps for class during recess | Steps | FT | N | 80% |
| Hayes & Van Camp (2015) | 6F | 8 | M | Daily steps at recess | - | FT | - | 100% |
| Hustyi et al. (2011) | 1M 1F | 4 | M | Total steps and activity level | Walking, running, and cycling | FT | - | 100% |
| Kuhl et al. (2015) | 14M 16F | 8–9 | M | Daily steps | Steps | FT | - | 89% |
| Kurti & Dallery (2013a) | 1M 5F | 50–71 | M | Daily steps | Steps | M | - | 96% |
| Kurti & Dallery (2013b) | 1M 5F | 60–67 | GS | Daily steps | Steps | M | - | 54% |
| La Londe et al. (2014) | 4M 1F | 21–26 | GS | Daily steps | - | FT | - | 92% |
| Li et al. (2018) | 2M 2F | 21–25 | M | Daily steps | Steps | FT | N | 100% |
| Maki et al. (2008) | 3M 1F | 20–56 | SR | Percentage of 30s intervals engaged in PA | Stretching aerobics, weights | D | - | 100% |
| Miller et al. (2018) | 9M 8F | 5–8 | M | Daily steps | Steps | FT | - | 100% |
| Normand (2008) | 3M 1F | 39–59 | M | Daily steps | Steps | D | - | 100% |
| Valbuena et al. (2019) | 5M | 18–65 | SM | Average rate of steps (min) | Steps per min | FT | - | 100% |
| Valbuena et al. (2015) | 1M 6F | 44–52 | M | Daily steps | Steps | M | - | 50% |
| VanWormer (2004) | 1M 2F | 32–52 | SR | Daily steps, body weight | Steps | M | N | 93% |
| Wack et al. (2014) | 5F | 18–28 | M | Distance per episode | Jogging, running | FT | - | 100% |
| Washington et al. (2014) | 5M 10F | M | Daily steps | Steps | M | - | 90% | |
| Zerger et al. (2017) | 16 | 9–12 | M | Daily steps | Steps | FT | - | 100% |
Note. (-) = variable not reported; GS= goal-setting; M= multiple (i.e., more than one component of self-monitoring procedure implemented; SR= self-recording; M= Multiple (more than one component of technology used); D= Device (e.g., email, text message); FT= Fitness Tracker (e.g., pedometer, Fitbit).
Although the physical activity that the participants engaged in varied, the most common activity was walking or steps (Hustyi et al., 2011; Normand, 2008; VanWormer, 2004). Several studies also used a self-monitoring procedure related to physical activity, but did not explicitly state the type of physical activity monitored (Cushing, Jensen, & Steele, 2011; Donaldson & Normand, 2009; Hayes & VanCamp, 2015; Washington, Banna, & Gibson, 2014). An important aspect of behavior intervention programs is the maintenance of behavior once an intervention is removed. Of the 20 studies, a majority (65%) did not reported whether behavior maintained. Two studies (Bassette, Kulwicki, Titus Dieringer, Zoder-Martell, & Heneisen, 2018; Donaldson & Normand, 2009) reported that behavior was maintained for all participants. Five studies reported that behavior was not maintained (Galbraith & Normand, 2017; Li, Curiel, Ragotzy, & Poling, 2018; Maki, Rudrud, Schulze, & Rapp, 2008; VanWormer, 2004; Washington et al., 2014).
Success estimates were used to determine the effectiveness of the interventions. Of the 20 studies, 10 had a 100% success estimate (Bassette et al., 2018; Hayes & Van Camp, 2015; Hustyi et al., 2011; Li et al., 2018; Maki et al., 2008; Miller, Valbuena, Zerger, & Miltenberger, 2018; Normand, 2008; Valbuena et al., 2019; Wack et al., 2014; Zerger et al., 2017). Four studies fell within 99%–90% (Kurti & Dallery, 2013a; La Londe, Mcneil, Wolfe Eversole, Ragotzy, & Poling, 2014; VanWormer, 2004; Washington et al., 2014). Two studies had a success estimate between 89%–80% (Galbraith & Normand, 2017; Kuhl et al., 2015). Donaldson and Normand (2009) was the lone study that fell within 79%–70%, at a 72% success estimate. Cushing et al. (2011) was the only study to have a success estimate in the range 69%–60%, with a success estimate of 67%. Finally, two studies had a success estimate of 59%–50% (Kurti & Dallery, 2013b; Valbuena, Miltenberger, & Solley, 2015).
Although behavior maintenance may not look promising, success estimates provide strong support for the use of self-monitoring and technology procedures on physical activity. Success estimate ranged from 50% to 100%, with 80% of the studies having a success estimate between 80% and 100%.
Discussion
The purpose of this review was to determine how self-monitoring techniques and technology have been applied using single-subject methodology to increase physical activity throughout the literature. The results of the study indicate that self-monitoring procedures have been successfully used in conjunction with technology in a multitude of ways to increase physical activity. This review found that most of the studies reviewed showed an increase of physical activity when using self-monitoring in conjunction with technology. In addition, few studies reported behavior maintenance, and those that did report maintenance of physical activity reported mixed results. The physical activity topography targeted by many interventions was daily step count or simple topography physical activity. Finally, there seems to be emerging trends in the preference that individuals have on technology (i.e., fitness trackers) and self-monitoring procedures (i.e., multiple).
Self-Monitoring Procedures
The most popular type of self-monitoring intervention used was multiple. However, the type of treatment packages that were used varied across studies. For example, Galbraith and Normand (2017) used goal-setting and feedback as part of the Good Behavior Game whereas Miller et al. (2018) used public posting, goal-setting, and self-monitoring. In addition, success estimate results indicated that self-monitoring treatment packages are highly efficacious at increasing physical activity, with an average of 89%. This finding is consistent with Kazdin’s (1974) report that multiple components of self-monitoring (i.e., self-monitoring, self-recording, goal-setting, feedback) are more effective at producing behavior change than self-monitoring interventions used in isolation.
Although Kazdin (1974) indicated that self-monitoring interventions used in isolation are not as effective as self-monitoring treatment packages, success estimate data somewhat contradicts that notion. Goal-setting was the second most popular intervention and success estimates ranged from 54% (Kurti & Dallery, 2013a) to 100% (Bassette et al., 2018), and two studies implemented a self-recording intervention with an average success estimate of 97% (Maki et al., 2008; VanWormer, 2004). Finally, one study used a self-monitoring intervention (i.e., Valbuena et al., 2019) with a success estimate of 100%.
Type of Physical Activity
For the studies that described the type of physical activity measured, the majority of behaviors could be described as simple topographies (e.g., daily steps). Simple topographical exercises are important, especially for individuals who have not engaged in physical activity for extended periods of time or have had minimal experience with more complex exercises. Furthermore, walking and daily steps are behaviors that many individuals engage in daily and can continue to engage in without significantly changing their lifestyle. For example individuals can take the stairs instead of the elevator or walk to lunch instead of drive.
The simplicity of simple topographical exercises may also be advantageous for individuals to come in contact with reinforcement more quickly if they are just beginning to exercise as well. Of the studies that included a simple topographical exercise, success estimates ranged from 50% to 100% (Valbuena et al., 2015) (e.g., Normand, 2008; Valbuena et al., 2019; Zerger et al., 2017) and averaged 86%.
Technology
The most frequent type of technology used was FT, with 10 studies using some type of FT. Six studies used a pedometer (e.g., Galbraith & Normand, 2017; Hustyi et al., 2014; Kuhl et al., 2015), three used a Fitbit (i.e., Hayes & Van Camp, 2015; La Londe et al., 2014; Li et al., 2018), and one used a Nike SportsBand (Wack et al., 2014). Although success estimates indicate that all three types of FTs were effective (pedometers: 95%; Fitbits: 97%; Nike SportsBand: 100%), available literature contradicts the accuracy of fitness tracking devices. Takacs et al. (2014) and Ferguson, Rowlands, Olds, and Maher (2015) indicated that FT devices such as Fitbits and Nike SportBands often overestimated the number of steps taken, in particular for more vigorous exercises such as running on a treadmill. Van Camp and Berth (2018) investigated the accuracy of fitness tracking devices such as Fitbits and pedometers and found that Fitbits are not only more accurate than pedometers but also accurately record steps taken during vigorous physical activity.
Behavior Maintenance
Despite positive success estimate results of using self-monitoring interventions and technology to increase physical activity, response maintenance data portrays a different result. Of 20 studies, response maintenance data was only reported in 4 studies. Furthermore, physical activity and self-monitoring behavior was maintained in only one study (Donaldson & Normand, 2009). As a science that emphasizes the importance of external validity and lasting behavior change, this statistic is troubling not only because there is a lack of response maintenance, but 80% of the studies did not collect behavior maintenance data. Stokes and Baer (1977) discussed the importance of training for generalization and advocated that for behavioral interventions to be effective, they must not only show external validity, but also lasting behavior change once the intervention is removed. As a result, if researchers or clinicians do not train for maintenance, then they are simply hoping that behavior will generalize and maintain.
The authors also noticed that researchers seldom trained participants prior to the intervention or reported mastery criteria. Although anecdotal, this may be one explanation as to why behavior did not maintain over time. Another explanation is that time restraints did not permit researchers to conduct follow-up sessions. For example, Kuhl et al. (2015) stated that they were unable to collect maintenance data for their class-wide intervention due to the conclusion of the academic school year. The absence of response maintenance data also makes it difficult to determine what type of self-monitoring intervention or type technology either increase the probability or decrease the probability of behavior maintaining. Donaldson and Normand (2009) was the only study that reported that behavior was maintained and used multiple types of self-monitoring interventions and technology. Whereas both Galbraith and Normand (2017) and Li et al. (2018) used self-monitoring treatment packages and FTs, VanWormer (2004) used self-recording and multiple components of technology. It is interesting that Donaldson and Normand (2009) had the lowest success estimate of any of the studies that reported maintenance with 72% compared to Galbraith and Normand (80%), Li et al. (100%), and VanWormer (93%).
Limitations
Although the current review is the first systematic review that investigated how self-monitoring techniques and technology have been used to increase physical activity, it is not without limitations. One limitation is that the authors only captured articles that increased physical activity. Articles that used self-monitoring techniques and technology to decrease sedentary behavior were excluded. Hence, there may be more literature available on self-monitoring techniques, technology, and physical activity. For example, Green, Sigurdsson, and Wilder (2016) used tactile prompts, feedback, and goal-setting to decrease bouts of sedentary behavior in office workers.
Several articles did not report the specific type of physical activity, so results should be interpreted fastidiously (Cushing et al., 2011; Donaldson & Normand, 2009; Hayes & Van Camp, 2015; La Londe et al., 2014). In addition, 70% of the studies included were coded as multiple because more than one component of self-monitoring was used. As a result, it is difficult to determine which self-monitoring procedure was most effective in changing physical activity. Kazdin (1974) stated that self-monitoring, goal-setting, and feedback, when used alone were not effective at changing behavior. Notwithstanding, when all three self-monitoring procedures were used as a treatment package, behavior change was more effective than when used in isolation. Finally, in studies where behavior did not maintain, it cannot readily be determined if it was due to weak experimental control. Many of the participants may have met their goal, but it would be difficult to continue to meet an increased goal for a desired behavior (e.g., ceiling effect).
Results indicate that self-monitoring interventions, when used with technology to increase physical activity are efficacious. However, like all research, researchers should view the literature through a critical lens. Sham and Smith (2014) stressed the importance of researchers being aware of possible publication biases, especially regarding single-subject research where results are typically interpreted by visual analysis and disciplines that do not use single-subject experimental designs may misinterpret the effectiveness of an intervention because of the small sample size. Nonetheless, the effectiveness of the interventions reviewed may not reflect all research because scholarship typically publishes papers on successful interventions. Therefore, additional research and the replication of self-monitoring interventions used in conjuncture with technology to increase physical activity is imperative.
Future Research
Results of this review indicate that the behavior-analytic research is sparse regarding the use of self-monitoring techniques used with technology to increase physical activity. Of the 19 articles that met inclusion criteria, all were published in the past 15 years. In addition, 15 of the 19 articles were published in journals that primarily publish behavior analytic research and are predominately read by behavior analysts. It may be difficult to disseminate the applicability and effectiveness of applied behavior analysis to other disciplines if the research continues to be published in behavior-analytic journals. Future research should investigate interdisciplinary approaches to apply the principles of behavior to increase physical activity and technology across all populations and ages.
Although evaluating the accuracy of FTs is beyond the scope of this review, future research should continue to investigate the accuracy of different FTs due to their widespread use, availability to the public, and applicability to other areas of research such as sport performance. In addition, future research should investigate how self-monitoring procedures and applications of technology can be applied to other health-related behaviors across various populations such as individuals with disabilities, the geriatric population, and individuals enrolled in postsecondary education. Applying these principles to reduce sedentary behavior in the workplace, and systematically increasing the amount of weight lifted for a specific lift may also prove beneficial. Researchers should also investigate interdisciplinary approaches to applying behavior analytic principles and disseminating the research in journals outside of the behavior analytic community.
Baer, Wolf, and Risley (1968) cautiously discussed the use of treatment packages and systematically adding treatment component to demonstrate experimental control. However, 70% of the studies that met inclusion criteria used a self-monitoring treatment package to increase physical activity. In addition, results from Kazdin’s (1974) study of self-monitoring indicated that self-monitoring procedures (i.e., self-monitoring, goal-setting, and feedback) were not as effective at evoking behavior change compared to a treatment package of all three self-monitoring procedures. Thus, future research should investigate what self-monitoring procedure(s) are most effective at producing and maintaining behavior change. An additional recommendation for future research is to collect data and demonstrate that behavior maintains across settings and time. In total, 80% of the studies either did not collect data on maintained behavior or demonstrate that behavior maintained. Although the accessibility of self-monitoring devices such as Fitbits and Apple Watches are available to the general public, research has indicated that habituation must be accounted and controlled for (Stokes & Baer, 1977). Finally, little research has been conducted that has investigated the rigor of physical activity and behavioral persistence. Future research should investigate this possible relationship and if fitness trackers may function as potential motivating operations for exercise.
Compliance with Ethical Standards
Conflict of Interest
Authors report no conflict of interest.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- Ainsworth BA, Haskell WL, Whitt MC, Irwin ML, Swartz AM, Strath SJ, et al. Compendium of physical activities: An update on activity codes and MET intensities. Medicine & Science in Sports & Exercise. 2000;32:498–516. doi: 10.1097/00005768-200009001-00009. [DOI] [PubMed] [Google Scholar]
- Baer DM, Wolf MM, Risley TR. Some current dimensions of applied behavior analysis. Journal of Applied Behavior Analysis. 1968;1:91–97. doi: 10.1901/jaba.1968.1-91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bassette, L., Kulwicki, J., Titus Dieringer, S., Zoder-Martell, K. A., & Heneisen, R. (2018). The use of a multicomponent behavioral intervention to promote physical activity in adolescents with autism spectrum disorders across inclusive community settings. Behavior Analysis in Practice. 11(4), 358–369. 10.1007/s40617-018-00285. [DOI] [PMC free article] [PubMed]
- Centers for Disease Control & Prevention. (CDC). (2017). National health interview survey. Retrieved from https://www-cdc-gov.authenticate.library.duq.edu/nchs/nhis/physical_activity/pa_glossary.htm. Accessed Aug 2018.
- Centers for Disease Control & Prevention. (CDC). (2018). Adult Obesity Causes and Consequences. Retrieved from https://www.cdc.gov/obesity/adult/causes.html. Accessed Aug 2018.
- Cooper JO, Heron TE, Heward WL. Applied behavior analysis. 2. Upper Saddle River, NJ: Pearson; 2007. [Google Scholar]
- Cushing CC, Jensen CD, Steele RG. An evaluation of personal electronic device to enhance self-monitoring adherence in a pediatric weight management program using a multiple baseline design. Journal of Pediatric Psychology. 2011;36:301–307. doi: 10.1093/jpepsy/jsq074. [DOI] [PubMed] [Google Scholar]
- Donaldson JM, Normand MP. Using goal setting, self-monitoring, and feedback to increase calorie expenditure in obese adults. Behavioral Interventions. 2009;24:73–83. doi: 10.1002/bin.277. [DOI] [Google Scholar]
- Fakhouri, T. H., Hughes, J. P., Song, M., Fulton, J. E., & Ogden, C. L. (2014). Physical activity in U. S. youth aged 12–15 years, 2012 (No. 141). Washington, DC: U.S. Department of Health & Human Services. Retrieved from: https://www-cdc-gov.authenticate.library.duq.edu/nchs/data/databriefs/db141.pdf. Accessed Aug 2018.
- Ferguson, T., Rowlands, A. V., Olds, T., & Maher, C. (2015). The validity of consumer-level, activity monitors in healthy adults worn in free-living conditions: A cross-sectional study. International Journal of Behavioral Nutrition & Physical Activity, 1–9. doi:10.1186/s12966-015-0201-9. [DOI] [PMC free article] [PubMed]
- Foxx RM, Axelroth E. Nicotine fading, self-monitoring and cigarette fading to produce cigarette abstinence or controlled smoking. Behaviour Research & Therapy. 1983;21:17–27. doi: 10.1016/0005-7967(83)90122-5. [DOI] [PubMed] [Google Scholar]
- Fritz JN, Iwata BN, Rolider NU, Camp EM, Neidert PL. Analysis of self-recording in self-management interventions for stereotypy. Journal of Applied Behavior Analysis. 2012;45:55–68. doi: 10.1901/jaba.2012.45-55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Galbraith LA, Normand MP. Step it up! using the good behavior game to increase physical activity with elementary school students at recess. Journal of Applied Behavior Analysis. 2017;50:856–860. doi: 10.1002/jaba.402. [DOI] [PubMed] [Google Scholar]
- Green N, Sigurdsson S, Wilder DA. Decreasing bouts of prolonged sitting among office workers. Journal of Applied Behavior Analysis. 2016;49:717–722. doi: 10.1002/jaba.309. [DOI] [PubMed] [Google Scholar]
- Hallahan DP, Lloyd J, Kosiewicz MM, Kaufman JM, Graves AW. Self-monitoring attention as a treatment for a learning disabled boy’s off-task behavior. Learning Disability Quarterly. 1979;2:24–32. doi: 10.2307/1511021. [DOI] [Google Scholar]
- Hayes LB, Van Camp CM. Increasing physical activity of children during school recess. Journal of Applied Behavior Analysis. 2015;48:690–695. doi: 10.1002/jaba.222. [DOI] [PubMed] [Google Scholar]
- Kazdin, A. E. (1974). Reactive self-monitoring: the effects of response desirability, goal setting, and feedback. Journal of consulting and clinical psychology, 42(5), 704. [DOI] [PubMed]
- Kuhl S, Rudrud EH, Witts BN, Schulze KA. Classroom-based interdependent group contingencies increase children’s physical activity. Journal of Applied Behavior Analysis. 2015;48:602–612. doi: 10.1002/jaba.219. [DOI] [PubMed] [Google Scholar]
- Kurti AN, Dallery J. Internet-based contingency management increases walking in sedentary adults. Journal of Applied Behavior Analysis. 2013;46:568–581. doi: 10.1002/jaba.58. [DOI] [PubMed] [Google Scholar]
- La Londe K, McNeil BR, Wolfe Eversole L, Ragotzy SP, Poling A. Increasing physical activity in young adults with autism spectrum disorders. Research in Autism Spectrum Disorders. 2014;8:1679–1684. doi: 10.1016/j.rasd.2014.09.001. [DOI] [Google Scholar]
- Li, A., Curiel, H., Ragotzy, S. P., & Poling, A. (2018). Using a lottery to promote physical activity by young adults with developmental disabilities. Behavior Analysis in Practice. 12, 612–616. 10.1007/s40617-018-00292-8. [DOI] [PMC free article] [PubMed]
- Maki AL, Rudrud EH, Schulze KA, Rapp JT. Increasing therapeutic exercise participation by individuals with acquired brain injury using self-recording and reinforcement. Behavioral Interventions. 2008;23:75–86. doi: 10.1002/bin.255. [DOI] [Google Scholar]
- Miller BG, Valbuena DA, Zerger HM, Miltenberger RG. Evaluating public posting, goal setting, and rewards to increase physical activity during school recess. Behavior Analysis in Practice. 2018;33:237–250. doi: 10.1002/bin.1631. [DOI] [Google Scholar]
- Normand MP. Increasing physical activity through self-monitoring, goal setting, and feedback. Behavioral Interventions. 2008;23:227–236. doi: 10.1002/bin.267. [DOI] [Google Scholar]
- Piercy KL, Troiano RP, Ballard RM, Carlson SA, Fulton JE, Galuska DA, et al. The physical activity guidelines for Americans. JAMA. 2018;320:2020–2028. doi: 10.1001/jama.2018.14854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reichow B, Volkmar FR. Social skills interventions for individuals with autism: Evaluation for evidence-based practices within a best evidence synthesis framework. Journal of Autism & Developmental Disorders. 2010;40:149–166. doi: 10.1007/s10803-009-0842-0. [DOI] [PubMed] [Google Scholar]
- Sham E, Smith T. Publication bias in studies of an applied behavior-analytic intervention: An initial analysis. Journal of Applied Behavior Analysis. 2014;47:663–678. doi: 10.1002/jaba.146. [DOI] [PubMed] [Google Scholar]
- Smith SL, Ward P. Behavioral interventions to improve performance in collegiate football. Journal of Applied Behavior Analysis. 2006;39:385–391. doi: 10.1901/jaba.2006.5-06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stokes, T. F., & Baer, D. M. (1977). An implicit technology of generalization 1. Journal of applied behavior analysis, 10(2), 349–367. [DOI] [PMC free article] [PubMed]
- Takacs J, Pollock CL, Guenther JR, Bahar M, Napier C, Hunt MA. Validation of the Fitbit One activity monitor device during treadmill walking. Journal of Science & Medicine in Sport. 2014;17:496–500. doi: 10.1016/j.jsams.2013.10.241. [DOI] [PubMed] [Google Scholar]
- Valbuena D, Miltenberger R, Livingston C, Slattery L. Self-monitoring and monetary reinforcement increases rate of walking in adults with intellectual disabilities. Journal of Developmental Disabilities. 2019;31:189–203. doi: 10.1007/s10882-018-9627-8. [DOI] [Google Scholar]
- Valbuena D, Miltenberger R, Solley E. Evaluating an Internet-based program and a behavioral coach for increasing physical activity. Behavior Analysis: Research & Practice. 2015;15:122–138. [Google Scholar]
- Van Camp CM, Berth D. Further evaluation of observational and mechanical measures of physical activity. Behavioral Interventions. 2018;33:284–296. doi: 10.1002/bin.1518. [DOI] [Google Scholar]
- VanWormer JJ. Pedometers and brief e-counseling: Increasing physical activity for overweight adults. Journal of Applied Behavior Analysis. 2004;37:421–425. doi: 10.1901/jaba.2004.37-421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wack SR, Crosland KA, Miltenberger RG. Using goal setting and feedback to increase weekly running distance. Journal of Applied Behavior Analysis. 2014;47:181–185. doi: 10.1002/jaba.108. [DOI] [PubMed] [Google Scholar]
- Washington WD, Banna KM, Gibson AL. Preliminary efficacy of prize-based contingency management to increase activity levels in healthy adults. Journal of Applied Behavior Analysis. 2014;47:231–245. doi: 10.1002/jaba.119. [DOI] [PubMed] [Google Scholar]
- Zerger HM, Miller BG, Valbuena D, Miltenberger RG. Effects of student pairing and public review on physical activity during school recess. Journal of Applied Behavior Analysis. 2017;50:529–537. doi: 10.1002/jaba.389. [DOI] [PubMed] [Google Scholar]