

Abstract
Background:
The dimensions of oral health-related quality of life (OHRQoL) Oral Function, Orofacial Pain, Orofacial Appearance, and Psychosocial Impact are the major areas where patients are impacted by oral diseases and dental interventions.
Aim:
The aim of this study was to evaluate whether dental patients’ reasons to visit the dentist fit the four OHRQoL dimensions.
Methods:
Dentists (N=1,580) from 32 countries participated in a web-based survey. For their patients with current oral health problems, dentists were asked whether these problems were related to teeth, mouth, and jaws’ function, pain, appearance, or psychosocial impact or whether they do not fit into the previous four categories. Dentists were also asked about their patients who intended to prevent future oral health problems. For both patient groups, the proportions of oral health problems falling into the four OHRQoL dimensions were calculated.
Results:
For 96 out of 100 dental patients, their current oral health problems were related to teeth, mouth, and jaws’ function, pain, appearance, or psychosocial impact. For 92 out of 100 dental patients, the oral health problems they intended to prevent in the future were related to the OHRQoL dimensions. Both numbers increased to 98% or higher when experts analyzed dentists’ explanations of why some oral health problems would not fit these four categories. None of the dentist-provided explanations suggested evidence against the OHRQoL dimensions as the concepts that capture dental patients’ suffering.
Conclusion:
Oral Function, Orofacial Pain, Orofacial Appearance, and Psychosocial Impact capture dental patients’ oral health problems worldwide. These four OHRQoL dimensions offer a psychometrically sound and practical framework for patient care and research, identifying what is important to dental patients.
Keywords: Oral Health, Quality of life, Surveys and Questionnaires, Dentistry, Problem-Oriented Medical Records, WHO
Introduction
Dental patients have current oral health problems, or they want to prevent them from occurring
Patients visit the dentist because of two main concerns – they either have current oral health problems, or they want to prevent them in the future. These problems are caused by 1,323 oral conditions or a combination of them (oral diseases represent the majority of these conditions, and we will use this term henceforth).1 Patients’ perceived oral health problems are not a deterministic reflection of the physical oral health situation, but rather they are shaped by personal, e.g., personality characteristics, and environmental factors, e.g., societal factors such as attitudes and laws. Conceptually, an infinite number of oral health problem situations results. Perceived oral health is a complex and multidimensional personal experience for each dental patient.
Dental patients’ oral health problems can be grouped
While the number of oral health problems is infinite, some problems are more related than others are. One reason for relationships among oral health problems is the oral disease that caused these problems. Typically, a disease creates not only one but several oral health problems for the patient. Consequently, the infinite number of oral health problems cluster into a smaller number of larger problem groups. These problem clusters are of practical importance for public health and clinical oral health care because they represent the major reasons why dental patients seek care. For example, Rosenstiel et al. mentioned that patients’ chief complaints or the reasons for treatment seeking typically belong to one of four categories (comfort, function, social, appearance).2
Dimensions of OHRQoL - A framework to group dental patients’ oral health problems
The entirety of the patient’s oral health problems is often described as the patient’s oral health-related quality of life (OHRQoL). Oral Function, Orofacial Pain, Orofacial Appearance, and Psychosocial Impact were identified as psychometrically sound and clinically intuitive OHRQoL dimensions.3 Exploratory4 and as well as confirmatory studies5 support the dimensions, and these studies were performed in diverse international dental patients as well as on general population subjects.6 Conceptually, OHRQoL can be seen as an umbrella concept with these four major components, and the patient’s oral health problems are situated in these components. If oral health problems lead patients to seeking care, then the four OHRQoL dimensions are also related to why dental patients visit the dentist.
Aim
The aim of this study was to evaluate whether dental patients’ reasons to visit the dentist fit the four OHRQoL dimensions Oral Function, Orofacial Pain, Orofacial Appearance, and Psychosocial Impact.
Materials and Methods
Participants
We targeted a convenience sample of international dentists, representing all six World Health Organization (WHO) regions with at least three countries per region. The WHO regions are (i) African Region, (ii) Region of the Americas, (iii) South-East Asia Region, (iv) European Region, (v) Eastern Mediterranean Region, and (vi) Western Pacific Region. To cover dental patients globally (through their dentists) was a major objective for this study.
Dentists from 32 countries participated. Each of the 32 countries was represented by one dentist, whom we called the “center dentist.” Center dentists were known to the first or the last author of the article or recommended by other center dentists. After the study was explained to them, we asked them to recruit at least ten dentists from their country to complete the web-based survey. They also received weekly reports on how many colleagues provided study data. Inclusion criteria for participating dentists were that they should be able to read and respond to an English-language questionnaire, and they should have treated dental patients in the past year. A total number of 1,580 dentists from 32 countries participated in the study.
Web-based survey about patients’ oral health problems
Data were collected with an anonymous electronic survey in the English language between June 10, 2017, and July 27, 2018. The questionnaire about patients’ oral health problems consisted of three main questions:
-
Why did patients typically visit you when they had problems with their teeth (including dentures), mouth, or jaws?
The patients visited me because of [% of patients]:- Impaired oral function (eating, chewing, talking, etc.)
- Pain (dental, oral, facial, etc.)
- Impaired dental, oral, or facial appearance
- Broader psychosocial impacts/distress because of their oral health situation
-
Other problems not mentioned above(if dentists responded here, they were asked to write down the most important problem, which does not fit into any of the four listed categories Function, Pain, Appearance, Psychosocial Impact)
-
To assess how your typical patients match your most recent patients, please check the dental records or think of your last 10 patients with oral health problems.
How many patients came because of [number of patients]?- Impaired oral function (eating, chewing, talking, etc.)
- Pain (dental, oral, facial, etc.)
- Impaired dental, oral, or facial appearance
- Broader psychosocial impacts/distress because of their oral health situation
-
Other problems not mentioned above(if dentists responded here, they were asked to write down the most important problem, which does not fit into any of the four listed categories Function, Pain, Appearance, Psychosocial Impact)
-
Dentists were also asked whether they perform preventative interventions. If they responded positively, they were asked: You mentioned that some patients visited you primarily for a preventative check-up. Why did they typically visit you when they came for a preventative check-up regarding their teeth (including dentures), mouth, or jaws?
They visited me because they wanted to prevent [% of patients]:- Impaired oral function (eating, chewing, talking, etc.)
- Pain (dental, oral, facial, etc.)
- Impaired dental, oral, or facial appearance
- Broader psychosocial impacts/distress because of their oral health situation
- Other problems not mentioned above (if dentists responded here, they were asked to write down the most important problem, which does not fit into any of the four listed categories (Function, Pain, Appearance, Psychosocial Impact)
Dentists were also asked for demographic and professional characteristics:
a country where dentist currently works (grouped in the six WHO regions)
years since graduation from a school of dentistry
age
gender
whether the majority of patients came to visit the dentist because of current suffering
whether the majority of patients were referred by other dentists
whether the dentist was the general/primary dentist for the majority of his/her patients
fields where dentist regularly diagnoses and treats patients ((i) Restorative Dentistry (including Endodontics and Prosthodontics), (ii) Periodontics, (iii) Oral and/or Maxillofacial Surgery, (iv) Pediatric Dentistry, (v) Orthodontics, (vi) Oral Medicine and/or Temporomandibular Disorders)
The questionnaire was generated using Qualtrics software. All questions asked for mutually exclusive responses, except for question No 8 about the dental fields. Study participants received the electronic link to the questionnaire, and their anonymous responses were collected online. Dentists could use several attempts to complete the survey, but only complete response sets were analyzed. The entire questionnaire can be found in the web appendix.
Data Analysis
The proportion of patients with problems related to teeth, mouth, and jaws’ function, pain, appearance, or psychosocial impact, also called four-dimensional (4D) oral health problems (and often simply referred to as 4D problems), was derived by summing the first four response categories in question 1, 2, or 3.
The proportion of 4D problems among recent patients who suffered from oral diseases (question 2) and a proportion of 4D problems among patients who wanted to prevent this suffering in the future (question 3) were the study’s main outcomes. The proportion of all patients with current 4D problems (question 1) was used for validation analyses.
First, we calculated these proportions. Second, we took dentists’ free-text responses into account and recalculated proportions. The reported free-text problems were checked whether they represented current patient suffering or not and whether they represented a 4D problem or not. When dentists mentioned a combination of problems, e.g., “Function and esthetics”, we only consider the first problem, in this case “Function.” Then, the proportions were changed accordingly. Three authors (MTJ, KRS, SS) independently performed these assessments. Third, we considered two factors when calculating the proportions: WHO region (where the dental care was provided - demographic question No. 1 was categorized into the six WHO regions) and dental field (what dental care was provided for the patients - demographic/professional characteristics question No 8 about the dental fields).
We graphically presented the results using stacked bar charts for all patients and stratified them also by WHO region or dental field. For the analysis of current patients’ suffering, using Stata7 software with maximum likelihood estimation with adaptive quadrature, we performed mixed-effects logistic regression analyses.8 The analysis was used to model the binary outcome variable (4D problem yes/no) with 15,800 patients nested within 1,580 dentists, assuming a dentist-level random effect which considered the interdependencies among patients seen by the same dentists. We estimated three models. While model #1 was a null model with no predictor variables in the fixed part and a random variance component for dentists, model #2 and #3 presented estimates for dental field or WHO region as predictor variables (both variables used as indicators variables) in the fixed part model and a random variance component for dentists. Using the models, we obtained predicted probabilities of a positive response, i.e., the patient has a 4D problem. An intraclass correlation coefficient (ICC) described the proportion of between cluster (dentist) variation in the total variation.
For the analysis of patients preventing future suffering, we performed linear regression analyses with bootstrap standard errors (1,000 replications). Bootstrapping is a distribution-independent method to derive standard errors.9 Including 1,065 dentists who provided preventive interventions for their patients, we estimated a model without any predictor variable and two other models with WHO region or dental field as predictor variables (both variables were used as indicator variables).
In validation analyses, we studied how well findings for dentists’ ten most recent patients approximated findings for all patients. A Pearson correlation coefficient was calculated and “large” effect sizes (r=0.5 and larger), according to guidelines for Cohen’s r, were expected.10
Ethical approval
The study was submitted to the Institutional Review Board (IRB) of the University of Minnesota, USA. The IRB determined (IRB ID: STUDY00000864) that “the proposed activity is not research involving human subjects as defined by DHHS (Department of Health and Human Services) and FDA (Federal Drug Administration) regulations since the questions are about a dental practice.”
Results
Participant characteristics
In this global survey, 1,580 dentists from 32 countries participated (Table 1). Slightly more female dentists participated. Dentists were typically around 40 years of age with two-thirds of dentists being between 30 and 50 years of age. Approximately half of the dentists had practiced dentistry for ten years or less. Dentists were typically the primary dentists for their patients, and the majority of patients were not referred to them for treatment. One-third of the dentists responded that their patients visited them only when they currently suffer from an oral health problem. Typically, dentists were active in multiple dental fields with restorative dentistry being the most frequent field of dentistry, in which more than two-thirds of the dentists performed diagnosis and treatment. The European Region was represented by the highest number of dentists with slightly more than 60% of all participating dentists coming from this region. On average, a participating country contributed 49 dentists to the project with four countries (Slovenia, Austria, Saudi-Arabia, and Italy), contributing more than 100 participants per country.
Table 1.
Characteristics of the 1,580 participating dentists
| Characteristic | N (%) or Mean (SD) |
|---|---|
| Age [years] | 38.6 (10.6) |
| Female gender | 848 (53.7) |
| Years since graduation | |
| 0–10 years | 772 (48.9) |
| 11–20 years | 453 (28.7) |
| 21 or more years | 355 (22.5) |
| Dentist is primary (general) dentist for patients | 988 (62.5) |
| Patients visit the dentist only because of current oral health problems (as compared to current and future problem prevention) | 515 (32.6) |
| Majority of dentist’s patients are referred | 563 (35.6) |
| Diagnosis and treatment performed in the following fields# | |
| Restorative Dentistry | 1122 (71.0) |
| Periodontics | 666 (42.2) |
| Oral & Maxillofacial Surgery | 440 (27.9) |
| Pediatric Dentistry | 523 (33.1) |
| Orthodontics | 243 (15.4) |
| Oral Medicine and/or TMD | 338 (21.4) |
| Region | |
| African Region | 111 (7.0) |
| Region of the Americas | 118 (7.5) |
| South-East Region | 113 (7.2) |
| European Region | 962 (60.9) |
| Eastern Mediterranean Region | 174 (11.0) |
| Western Pacific Region | 102 (6.5) |
| Country | |
| Australia | 29 (1.8) |
| Austria | 178 (11.3) |
| Bosnia & Herzegovina | 30 (1.9) |
| Brazil | 17 (1.1) |
| Chile | 36 (2.3) |
| China | 28 (1.8) |
| Colombia | 23 (1.5) |
| Croatia | 52 (3.3) |
| Denmark | 24 (1.5) |
| Germany | 99 (6.3) |
| Ghana | 32 (2.0) |
| India | 70 (4.4) |
| Iran | 18 (1.1) |
| Italy | 121 (7.7) |
| Japan | 34 (2.2) |
| Northern Macedonia | 78 (4.9) |
| Morocco | 12 (0.8) |
| Nigeria | 66 (4.2) |
| Panama | 18 (1.1) |
| Russia | 15 (1.0) |
| Saudi Arabia | 130 (8.2) |
| Serbia | 39 (2.5) |
| Singapore | 11 (0.7) |
| Slovenia | 223 (14.1) |
| South Africa | 13 (0.8) |
| Sri Lanka | 32 (2.0) |
| Sudan | 14 (0.9) |
| Sweden | 56 (3.5) |
| Switzerland | 33 (2.1) |
| Thailand | 11 (0.7) |
| United Kingdom | 14 (0.9) |
| United States | 24 (1.5) |
TMD Temporomandibular Disorders,
dentists could mark one or more fields
Patients suffering currently from oral health problems
The vast majority of the dentists (78%, n=1,237), reported that all their recent patients’ suffering was related to teeth, mouth, and jaws’ function, pain, appearance, or psychosocial impact (Figure 2, left panel).
Figure 2.
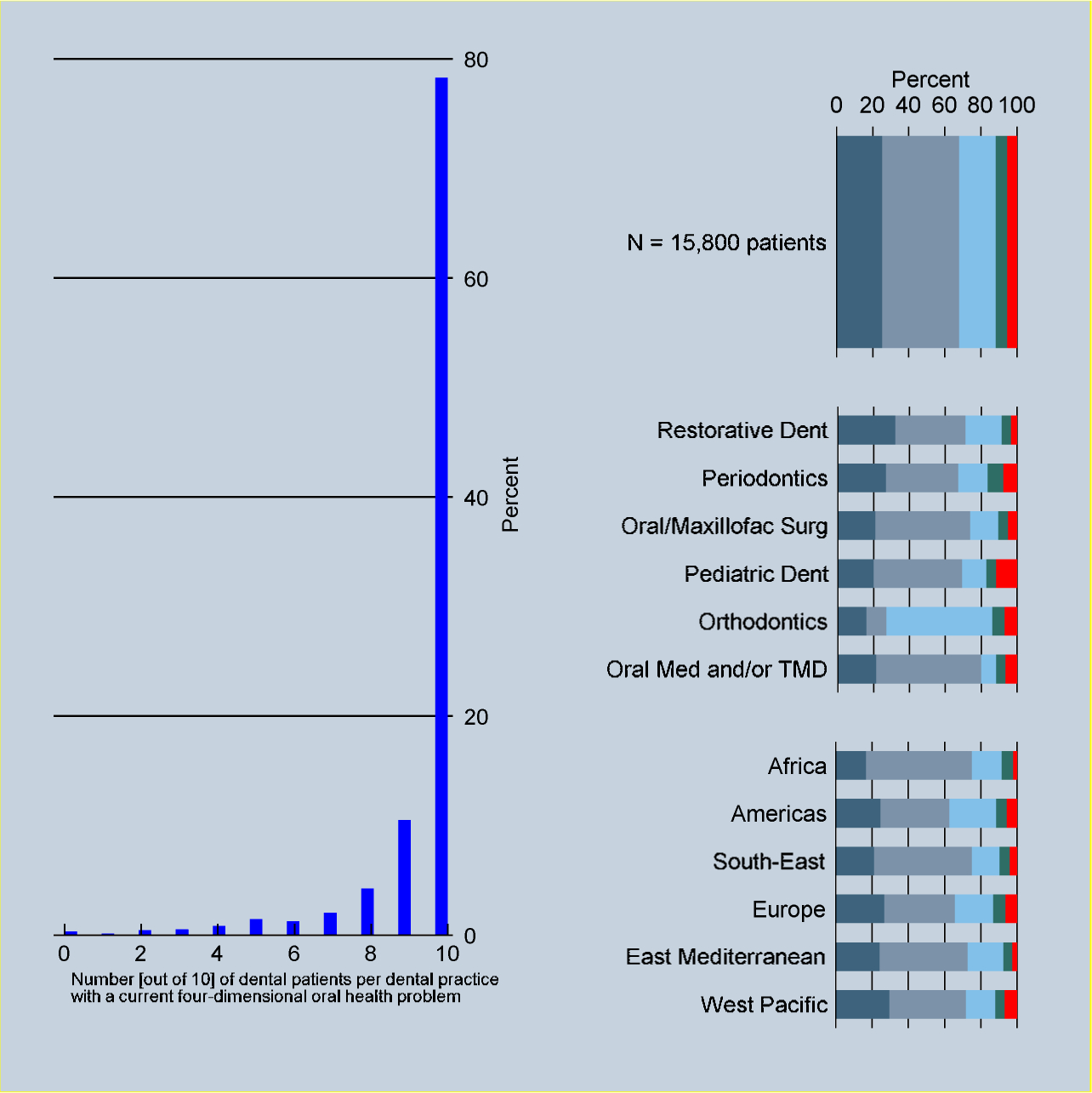
Number [out of 10] of dental patients per dental practice with a current four-dimensional oral health problem [left panel] and distribution of oral health problems related to function [dark grey], pain [light grey], appearance [light blue], psychosocial impact [green], and other reasons [red] for 15,800 international patients and stratified by dental field and WHO region [right panel]
Among patients with current suffering (Figure 2, right panel), 14,951 of the 15,800 (95%) patients had a 4D problem (for results by country, see web appendix Table 1). Taking into account that patients were clustered in dentists, the model-derived probability of a 4D oral problem was 96%. The ICC was 0.69, which means that slightly more than two-thirds of the total variation of the outcome was due to variation between dentists.
When the free-text responses given by the dentists as an explanation for “other” oral health problems were analyzed, the model-derived probability of a 4D problem increased to 99%, and the ICC increased to 0.90. Among the 343 free-text responses, 30% were too vague to be confidently interpreted as to whether the “other” oral health problem represented indeed current suffering not covered by the four OHRQoL dimensions. However, none of these vague free-text responses contained evidence contradicting the four dimensions as the concepts that capture dental patients’ suffering. That is, while some “other” oral health problems were only vaguely described, all these problems could potentially be related to teeth, mouth, and jaws’ function, pain, appearance, or psychosocial impact. When the free-text responses were independently assessed by another expert (sensitivity analysis), the model-derived probability of a 4D problem was almost identical.
When dental field or WHO region was included in two statistical models, model-derived probabilities were 94% or higher for 4D problems in any dental field or any WHO region. All results were precise with widths of 95% confidence intervals for predicted probabilities of 5% or less.
In a validation analysis, the correlations between recent patients’ and all patients’ problems related to teeth, mouth, and jaws’ function, pain, appearance, or psychosocial impact were “large” (range: 0.62 to 0.81). We interpreted these results as evidence that a dentist’s recent patients seemed to be similar to all patients as far as their oral health problems were concerned.
Patients intending to prevent future suffering from oral health problems
About two-thirds of the 1,580 dentists (n=1,065), provided preventive oral health care. Among them, more than 80% (n=889) mentioned that all their patients’ future oral health problems were related to teeth, mouth, and jaws’ function, pain, appearance, or psychosocial impact (Figure 3).
Figure 3.
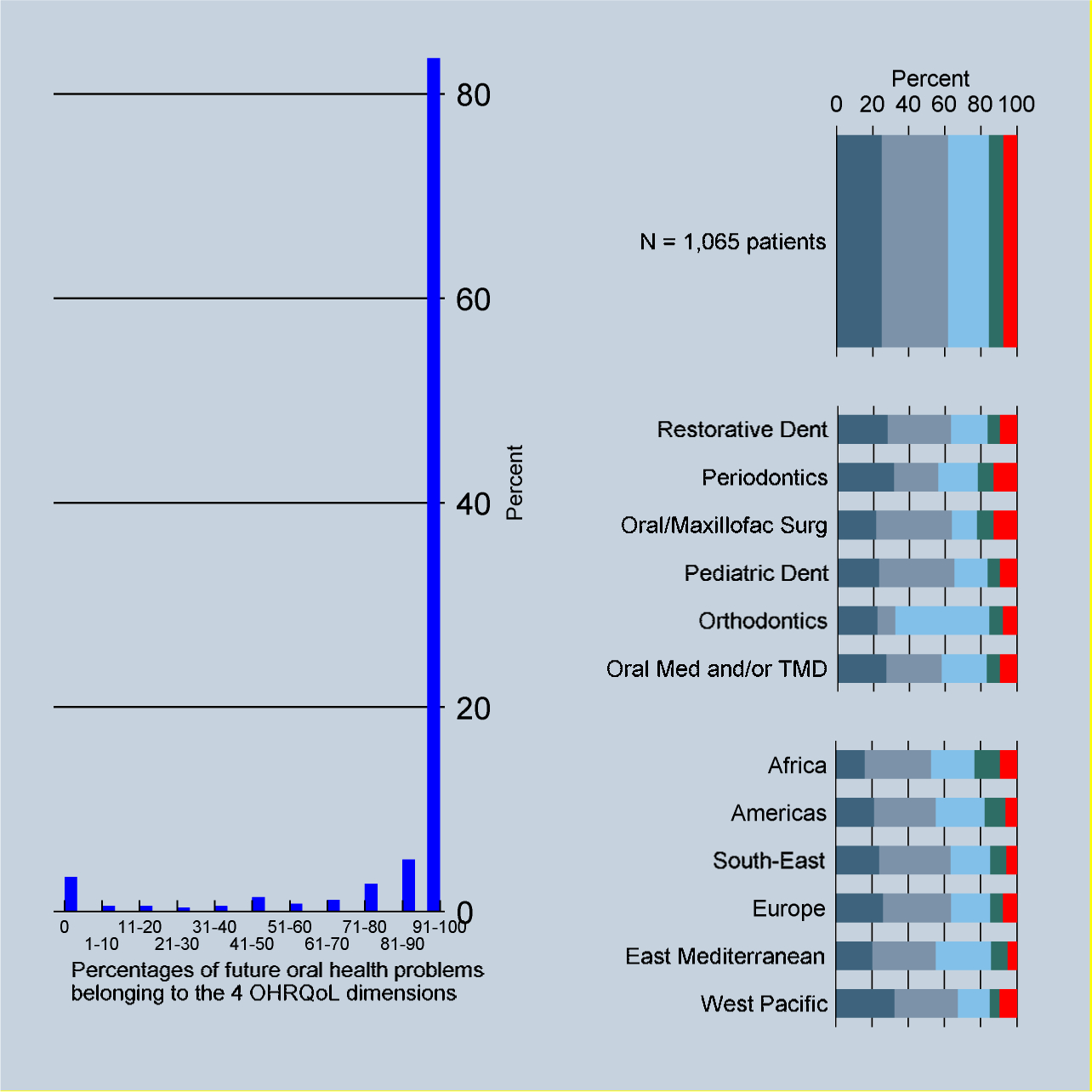
Eleven proportion brackets of patients intending to prevent a future 4D problem among all preventive patients per dental practice [left panel]. Distribution of oral health problems related to function [dark grey], pain [light grey], appearance [light blue], psychosocial impact [green], and other reasons [red] these patients intended to prevent for 1,065 international dentists and stratified by dental field and WHO region [right panel]
The vast majority of problems patients wanted to prevent by visiting their dentists (92%) was a 4D problem (for results by country, see web appendix Table 2). When experts assessed free-text responses, this number increased to 98%. When adjusted for the dental field and WHO region, all model-derived probabilities of a 4D problem for any dental field and any WHO region were 90% and higher. All results were precise with widths of 95% confidence intervals for predicted probabilities of 7% or less.
Discussion
Patients’ reasons why they seek oral health care align very well with the four dimensions of OHRQoL. The findings confirm the validity of OHRQoL as a comprehensive concept that captures the patient’s oral health suffering and supports the OHRQoL dimensions as the primary building blocks within the umbrella concept OHRQoL.
According to 1,580 dentists from 32 countries from all WHO world regions, approximately 95% of their patients’ oral health problems fell into the four OHRQoL dimensions. Neither practice profile of the dentist, i.e., what type of dental care the dentist provided, nor where the dentist (and patients) were from, changed these findings. Findings indicate that OHRQoL dimensions were, not unexpectedly, a global concept for oral health.
When oral health problems mentioned by the participating dentists as being “other problems,” i.e., problems not falling into the four dimensions, were re-assessed by two experts, this percentage increased to 99%. While some dentists’ responses were too vague to be confidently evaluated as belonging to the four dimensions or not, these vague responses, such as “complex patients,” did not provide any evidence against the four dimensions. Again, findings indicated that the four OHRQoL dimensions are, not unexpected, a broad concept describing dental patient’s oral health.
Overall, these findings support that the four OHRQoL dimensions are the underlying framework of patients’ oral health problems caused by oral diseases, regardless of whether patients visited the dentist due to current oral health suffering or because they want to prevent future suffering from oral diseases.
Literature findings that dental patients’ suffering falls into the four OHRQoL dimensions
Our survey study design recruited international dentists to report their patients’ oral health problems. This study design was not used before to investigate this research question. However, it is not unusual to study international dentists. The World Dental Federation (FDI) performs such surveys regularly targeting international dentists.11 In addition to organized dentistry, researchers like us used global surveys to provide a perspective about topics such as the International Classification of Functioning, Disability, and Health12 or its Health Children and Youth version (ICF-CY.)13
The uniqueness of our research question paired with a particular international survey design limits the comparability of our results. However, the approach to use experts to assign items (in our case, patients’ oral health problems) to oral health attributes (in our case, OHRQoL dimensions) has been applied frequently. For the 49-item Oral Health Impact Profile (OHIP) the two OHIP instrument authors originally grouped the questionnaire’s 49 items, i.e., patient problems, into seven domains (Functional limitation, Physical disability, Psychological discomfort, Physical disability, Psychological disability, Social disability, and Handicap).14 Later, when 14 health care experts tried to replicate these findings, they found only four dimensions were needed to account for all OHIP items when assigning OHIP items to each of the original seven domains.15 For this group of experts, it could also be shown that a stable problem-to-dimensions assignment in a test-retest part of the study was achieved, indicating that experts agreed and that item-attribute assignment is not arbitrary.15 However, how consistent this assignment is across experts and for experts’ repeated assignment over time is typically not studied. For example, when the instruments assessing dental Patient-Reported Outcomes (dPROs), also called dental Patient-Reported Outcomes Measures (dPROMs)1, were comprehensively identified and analyzed in two systematic reviews,16,17 the review authors concluded that many questionnaire developers just assigned items to domains or dimensions without a more formal analysis. Obviously, for these dPROMs, authors relied on their clinical expertise for item assignment. When analyses were performed, most often factor analysis -a technique revealing the unobserved structure underlying the variation of observed questionnaire variables and their interrelationships18 - was used to investigate how individual questionnaire items, often patient’s oral health problems, are related to dimensions of the targeted construct.
Dimensions of OHRQoL – a comprehensive set of major patient problems
The finding that the four OHRQoL dimensions work well as a grouping for dental patients’ concern is not surprising. The OHRQoL dimensions were studied in several previous studies using the OHIP. The OHIP is the instrument with the largest number of OHRQoL items, and thus being able to characterize patients’ oral health problems most comprehensively. This instrument is also the most widely used OHRQoL instrument, as dentists and researchers find it to be the best fit for their patients’ or research subjects’ oral health problems. Different methodological approaches such as exploratory factor analysis,4 confirmatory factor analysis,5 validation analyses6, correlation analyses19 all support OHRQoL dimensions as the major attributes underlying the patient’s oral health experience. Even for multi-item dPROMs, in general, this seems to be the case. In two recent systematic reviews, the four OHRQoL dimensions were the major attributes measured by 53 oral health-generic16 as well as 103 oral health-specific dPROMs.17 That international dental patients’ oral health problems fit these dimensions as well, was expected; however, the clear findings using a different methodological approach compared to previous OHRQoL dimension studies provides strong confirmatory evidence for the concept of OHRQoL dimensions.
Strengths and limitations
This study has several strengths. The sample size of participating international dentists was large, and the number of 32 participating countries was substantial. All WHO regions were represented by a minimum of three countries. The three most populous countries were included and, except for Canada, the seven largest countries in the world were included. The number of 10 patients per dentist and the number of 32 countries are based on feasibility and sample size calculation. Less than 250 patients (without taking into account that they are clustered within dentists) allow estimation of a proportion of 0.80 with a 95% confidence interval width of 0.1.
This study also has limitations. Our three questions’ five response options were mutually exclusive, i.e., the dentist could only choose one answer. Reflecting the clinical reality that patients often present with multiple problems of equal importance, many dentists mentioned such combinations of oral health problems, e.g., “function and esthetics”, and reported them as “other” oral health problems. Because we aimed to study only the patients’ primary problems to not exceed 100% as the sum of the five categories, we only considered the first of several mentioned problems in our analysis of corrected responses.
We were not able to calculate a response rate for the participating dentists because we assured them that their responses were anonymous and that we did not even know whether they participated or not because we did not ask center dentists to report the number of invited dentists. If study participation were related to the prevalence of 4D problems, our findings would be biased. We believe this situation is unlikely because we did not identify any factor, including the dentist’s sociodemographic characteristics, that were relevantly related to prevalence of 4D problems (results not shown).
We used a convenience sample of countries and within a particular country, a convenience sample of dentists. While convenience samples are more prone to bias than random or large consecutive samples, it seems unlikely that our sampling strategies substantially biased the finding that dental patients’ problems fit into the four OHRQoL dimensions. From a clinical point of view, the distribution of patients’ dimensional oral health problems varies by dental field, e.g., more patients with appearance problems visit orthodontists than other dentists or more patients with orofacial pain problems visit TMD and Orofacial Pain specialists than other dentists. While a particular dimension of dental patient suffering may be more frequent in a particular setting, we did not see any reason why the cumulative proportion of all dimensions should vary across settings. This clinically plausible statement is supported by the multivariable analysis in this study. Neither WHO region, i.e., where patients came from nor dental field, i.e., what treatments were performed for patients, influenced OHRQoL dimensions’ coverage of patients’ oral health problems. The cumulative proportion of all dimensional problems was relatively constant.
Finally, we did not ask patients directly about their reasons why they visited the dentist. Instead we used an indirect approach asking dentists about their patients’ reasons, assuming dentists know their patients’ oral health problems. Both approaches should provide the same answer. In fact, dental patients were asked about their oral health problems in previous research studies. For example, OHIP developers asked patients and recorded their experiences of dental disorders” in Australia14 and other researchers repeated this approach in de novo instrument developments of the OHIP in Germany,20 Japan,21 Malaysia,22 and Saudi-Arabia.23 A remarkable similarity of patient problems across these different cultures was found. When such international OHIP data were analyzed with latent variable analyses, as discussed above, OHIP data had four dimensions – a finding attesting to the complementarity of studying patient’s oral health problems directly by asking patients or indirectly by asking dentists about their patients.
Implications
The four OHRQoL dimensions Oral Function, Orofacial Pain, Orofacial Appearance, and Psychosocial Impact offer a robust and practical framework for oral health care and research, identifying what is important to patients. Consequently, the level of a patient suffering in these four areas needs to be quantified with psychometrically sound dPROMs by deriving a score. After applying oral interventions, the change in scores would represent the treatment effect of the interventions. The treatment that reduces patient suffering the most (or prevents the suffering from occurring) would be the preferred treatment for the patient in an evidence-based dentistry framework. Such general principles of providing optimal care for patients that emphasize the importance of four-dimensional dPROMs have been already pointed out in dental fields such as prosthodontics24 and orthodontics.25 Value-based oral health care, relating treatment outcomes to costs, also relies on dPROM scores.26
The four OHRQoL dimensions and their measures, e.g., the OHIP-527,28 - a practical five-item tool applicable in all practice and research settings - are essential for global evidence-based dentistry, that is, applying oral interventions that work best for dental patients.
Conclusion
Oral Function, Orofacial Pain, Orofacial Appearance, and Psychosocial Impact capture dental patients’ oral health problems worldwide and regardless of whether the patient currently suffers from oral diseases or intends to prevent them in the future.
Supplementary Material
Figure 1.
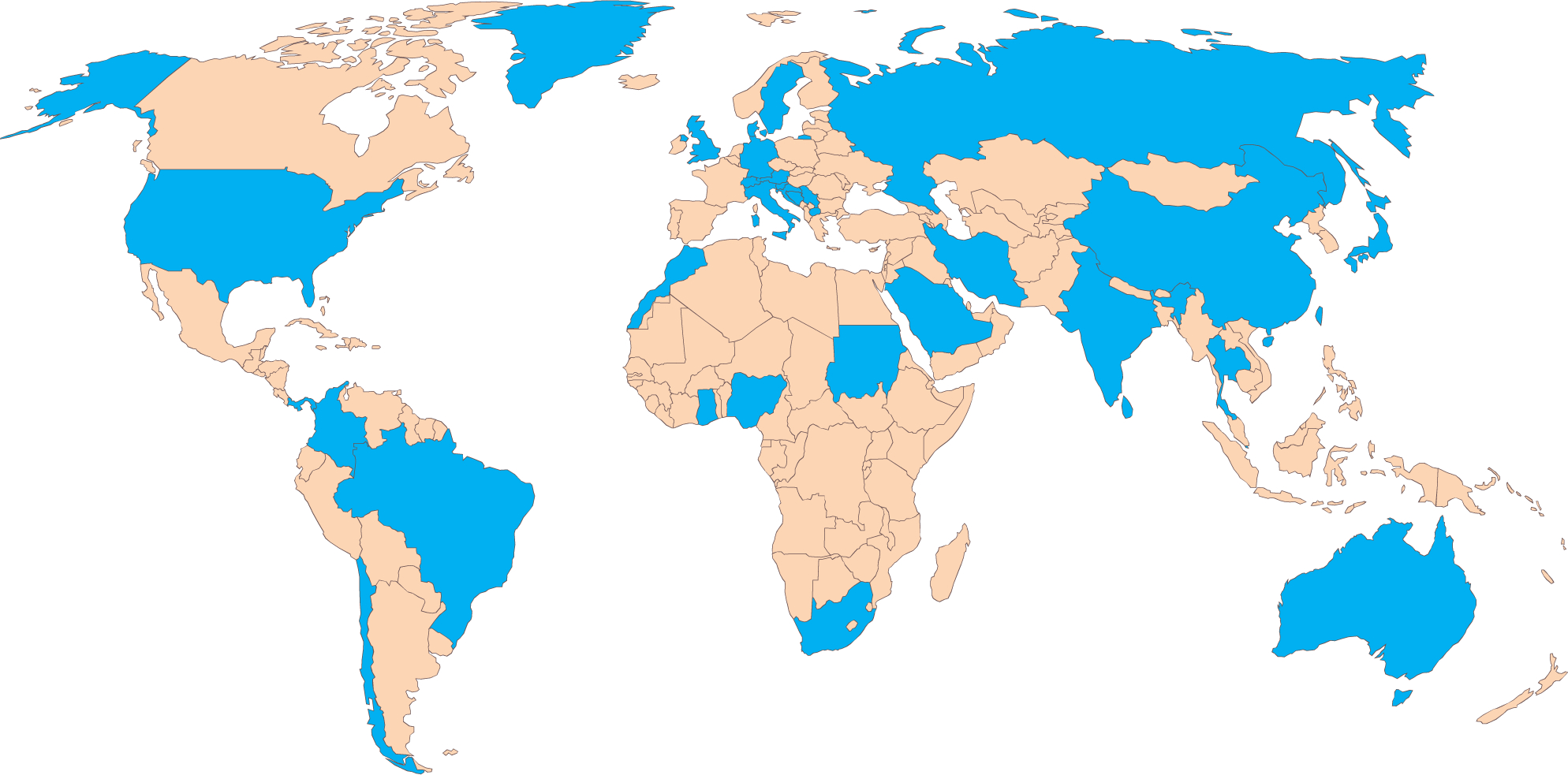
Countries participating in the study (N=32, in blue) from six World Health Organization regions
Acknowledgments
We thank Ms. Kathleen M. Patka, Executive Office and Administrative Specialist, Division of Oral Medicine, School of Dentistry, University of Minnesota, Minneapolis, MN, USA, for proofreading the manuscript.
The research reported in this publication was supported by the National Institute of Dental and Craniofacial Research of the National Institutes of Health, USA, under the Award Numbers R01DE022331 and R01DE028059.
List of Abbreviations:
- OHRQoL
Oral Health-Related Quality of Life
- WHO
World Health Organization
- 4D
Four-Dimensional
- ICC
Intraclass Correlation Coefficient
- TMD
Temporomandibular Disorders
- OHIP
Oral Health Impact Profile
- dPRO
Dental Patient-Reported Outcome
- dPROM
Dental Patient-Reported Outcome Measure
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Declarations of interest:
None.
References
- 1.John MT. Health outcomes reported by dental patients. J Evid Based Dent Pract. 2018;18(4):332–335. [DOI] [PubMed] [Google Scholar]
- 2.Stephen Rosenstiel, Martin Land, Junhei Fujimoto. Comtemporary Fixed Prosthodontics. 4th ed. St. Louis: Mosby; 2006. [Google Scholar]
- 3.John MT, Hujoel P, Miglioretti DL, LeResche L, Koepsell TD, Micheelis W. Dimensions of oral-health-related quality of life. J Dent Res. 2004;83(12):956–960. [DOI] [PubMed] [Google Scholar]
- 4.John MTT, Reissmann DRR, Feuerstahler L, et al. Exploratory factor analysis of the Oral Health Impact Profile. J Oral Rehabil. 2014;41(9):635–643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.John MTT, Feuerstahler L, Waller N, et al. Confirmatory factor analysis of the Oral Health Impact Profile. J Oral Rehabil. 2014;41(9):644–652. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.John MT, Reißmann DR, Feuerstahler L, et al. Factor analyses of the Oral Health Impact Profile - Overview and studied population. J Prosthodont Res. 2014;58(1):26–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.StataCorp. 2019. Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC. [Google Scholar]
- 8.McCulloch CE, Searle SR, Neuhaus JM. Generalized, Linear, and Mixed Models. 2nd ed. Hoboken, NJ: Wiley; 2008. [Google Scholar]
- 9.Efron B, Tibshirani R. An Introduction to the Bootstrap. New York: Chapman & Hall; 1993. [Google Scholar]
- 10.Cohen J Statistical power analysis for the behavioral sciences. 1988, Hillsdale, NJ: L. Erlbaum Assoc; xxi 567. [Google Scholar]
- 11.World Dental Federation. Surveys. https://www.fdiworlddental.org/resources/surveys. Published 2019. Accessed April 22, 2020.
- 12.Dougall A, Molina GF, Eschevins C, Faulks D. A Global Oral Health Survey of professional opinion using the International Classification of Functioning, Disability and Health. J Dent. 2015;43(6):683–694. [DOI] [PubMed] [Google Scholar]
- 13.Faulks D, Molina G, Eschevins C, Dougall A. Child oral health from the professional perspective - a global ICF-CY survey. Int J Paediatr Dent. 2016;26(4):266–280. [DOI] [PubMed] [Google Scholar]
- 14.Slade GD, Spencer AJ. Development and evaluation of the Oral Health Impact Profile. Community Dent Heal. 1994;11(1):3–11. [PubMed] [Google Scholar]
- 15.John MTT. Exploring dimensions of oral health-related quality of life using experts’ opinions. Qual Life Res. 2007;16(4):697–704. [DOI] [PubMed] [Google Scholar]
- 16.Mittal H, John MT, Sekulić S, Theis-Mahon N, Rener-Sitar K. Dental patient-reported outcome measures for adults: a systematic review. J Evid Based Dent Pract. 2019;1(19):53–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Rener-Sitar K, John MT, Truong V, Tambe S, Theis-Mahon N. Systematic Review of Nonmalignant Oral Disease-specific dPROMs for Adult Patients. J Evid Based Dent Pract. 2019;submitted. [DOI] [PubMed] [Google Scholar]
- 18.Gorsuch RL. Factor Analysis. Hillsdale, N.J.: Erlbaum Associates; 1983. [Google Scholar]
- 19.John MT, Reissmann DR, Čelebić A, et al. Integration of oral health-related quality of life instruments. J Dent. 2016;53:38–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.John MTMT, Patrick DLDLL, Slade GDGDD. The German version of the Oral Health Impact Profile–translation and psychometric properties. Eur J Oral Sci. 2002;110(6):425–433. [DOI] [PubMed] [Google Scholar]
- 21.Yamazaki M, Inukai M, Baba K, John MTT. Japanese version of the Oral Health Impact Profile (OHIP-J). J Oral Rehabil. 2007;34(3):159–168. [DOI] [PubMed] [Google Scholar]
- 22.Saub R, Locker D, Allison P. Derivation and validation of the short version of the Malaysian Oral Health Impact Profile. Community Dent Oral Epidemiol. 2005;33(5):378–83. [DOI] [PubMed] [Google Scholar]
- 23.Al-Jundi MA, Szentpétery A, John MT. An Arabic version of the Oral Health Impact Profile: Translation and psychometric properties. Int Dent J. 2007;57(2):84–92. [DOI] [PubMed] [Google Scholar]
- 24.Reissmann DR. Dental patient-reported outcome measures are essential for evidence-based prosthetic dentistry. J Evid Based Dent Pract. 2019;19(1):1–6. [DOI] [PubMed] [Google Scholar]
- 25.Hua F Increasing the Value of Orthodontic Research Through the Use of Dental Patient-Reported Outcomes. J Evid Based Dent Pract. 2019;19(2):99–105. [DOI] [PubMed] [Google Scholar]
- 26.Listl S Value-based oral health care: moving forward with dental patient-reported outcomes. J Evid Based Dent Pract. 2019;19(3):255–259. [DOI] [PubMed] [Google Scholar]
- 27.John MT, Miglioretti DL, LeResche L, Koepsell TD, Hujoel P, Micheelis W. German short forms of the Oral Health Impact Profile. Community Dent Oral Epidemiol. 2006;34(4):277–288. [DOI] [PubMed] [Google Scholar]
- 28.Naik A, John MT, Kohli N, Self K, Flynn P. Validation of the English-language version of 5-item Oral Health Impact Profile. J Prosthodont Res. 2016;60(2):85–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.