

INTRODUCTION
Primary cardiac tumors are rare and usually present with non-specific symptoms.1 Alternative diagnosis including metastatic extension of malignancy from extra-cardiac origins should be considered but is often discovered incidentally during an imaging examination. Careful tracking the orifice of lesions and identifying the shunting flow are crucial to differentiate from aortic aneurysms. As the aortic aneurysm is impressed, 3D computed tomography (CT) reconstruction provides additional diagnostic information of the surrounding vasculature, particularly when surgical resection is considered.
CASE
We reported a 64-year-old man with an accidentally identified intra-cardiac tumor at the survey of new onset atrial fibrillation. Without any history of cardiac diseases or cigarette smoking, he was admitted for herniorrhaphy and atrial fibrillation (AF) was observed at the pre-operative electrocardiogram in the absence of palpitation. During the work-up of AF, the initial echocardiography displayed a huge mass (8.3*6.4 cm) locating at the right atrium (RA) with heterogenous characteristics (Figure 1A). Meanwhile, chest CT also supported the diagnosis of intra-cardiac tumor (Figure 1B). He was thereafter transferred to cardiovascular surgeons. However, surprisingly the intra-cardiac mass progressed to be a hypoechogenous cavity with a shunting flow from the aorta in the following transthoracic echocardiography (Figure 1C, supplement video 1 and 2). To differentiate the etiologies, an emergent 3D CT reconstruction was performed and indicated a huge protruding aortic aneurysm origin from the non-coronary sinus of Valsalva (Figure 1D). The intra-operative transesophageal echocardiography also showed an aneurysm with thrombosis. Correspondingly, the operative findings confirmed the diagnosis of a huge aortic aneurysm (above 8 cm). It originated from the sinus of Valsalva and protruded to the RA (Figure 2A). Post the Bentall procedure including the composite graft replacement of the aortic valve, aortic root, and ascending aorta as well as the re-implantation of the coronary arteries into the graft (Figure 2B), the patients recovered well. The histology also displayed no evidence of malignancy but an aortic aneurysm with calcification (Figure 2C).
Figure 1.
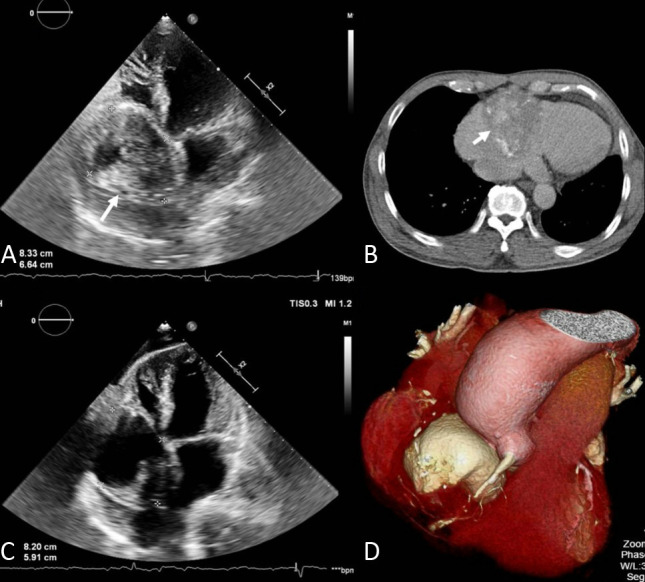
(A) The transthoracic echocardiography representing a huge mass (arrow) locating at the right atrium with heterogenous characteristics; (B) The initial chest computed tomography indicating an intra-cardiac tumor (arrow); (C) The following transthoracic echocardiography indicating the resolution of the intra-cardiac mass to a hypoechogenous cavity with a shunting flow from the aorta; (D) An emergent multidetector computed tomography revealing a huge protruding aortic aneurysm origin from the non-coronary sinus of Valsalva.
Figure 2.
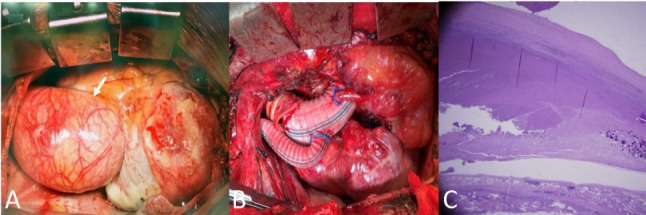
(A) A huge aortic aneurysm in a surgical window; (B) Post a Bentall procedure and coronary graft bypass; (C) The histology also displaying no evidence of malignancy but an aortic aneurysm with calcification.
DISCUSSION
Though an acute rupture of aortic aneurysm is fatal, a slow progression and leak may have a chronic presentation and may mimic other intra-thoracic lesions including a cardiac tumor.1 In previous literature, this anomaly mimicking a primary cardiac tumor or metastatic neoplasm at the initial investigation has been merely reported. Camporrotondo M and colleagues delineated a proximal thoracic aortic aneurysm imitating a mediastinal neoplasm.2 Ortner’s syndrome particularly described as thoracic aortic aneurysm mimicking thoracic malignancy.3 Also, Morris et al. systematically reviewed complications of left atrium compression or fistula formation of thoracic aortic aneurysms.4 In one series of 260 patients, the surgical mortality was 8% for elective resection and 33% for emergency operations.5 Therefore, making the accurate diagnosis prior to the surgical intervention is crucial. Despite two-dimensional echocardiography of the routine equipment for identifying the possible etiology of intra-cardiac lesions, an experience echocardiography performer is the key to detect the true vascular structure of aortic aneurysms. Collectively, this case highlights the diagnostic challenges of a huge sinus of Valsalva aneurysm with external compression to RA mimicking an intra-cardiac tumor.
LEARNING POINTS
1. Despite sinus of Valsalva aneurysm of a well-known pathology, its presence as a cardiac tumor with the RA compression is rare.
2. This case highlights the diagnostic challenges of a huge sinus of Valsalva aneurysm which mimics an intra-cardiac tumor.
CONFLICTS OF INTEREST
All authors have no conflicts of interest.
AUTHOR CONTRIBUTIONS
Conceptualization: NC Wu, JY Shih. Data curation: WT Chang. Project administration: NC Wu, JY Shih. Resources: ZC Chen, BC Cheng. Supervision: ZC Chen, BC Cheng. Writing original draft: WT Chang. Writing review & editing: WT Chang.
FUNDING
This work was supported by Chi-Mei Medical Center.
REFERENCES
- 1.Liao ZY, Tsai JP, Kuo JY, et al. Large aortic aneurysm mimicking a cardiac tumor. Cardiovasc Ultrasound. 2010;8:33. doi: 10.1186/1476-7120-8-33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Wang WP, Yan XL, Ni YF, et al. An unusual cause of dysphagia: thoracic aorta aneurysm. J Thorac Dis. 2013;5:E224–E226. doi: 10.3978/j.issn.2072-1439.2013.11.15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Pathirana U, Kularatne S, Handagala S, et al. Ortner’s syndrome presenting as thoracic aortic aneurysm mimicking thoracic malignancy: a case report. J Med Case Rep. 2015;9:147. doi: 10.1186/s13256-015-0629-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Morris AL, Barwinsky J. Unusual vascular complications of dissecting thoracic aortic aneurysms. Cardiovasc Radiol. 1978;1:95–100. doi: 10.1007/BF02552002. [DOI] [PubMed] [Google Scholar]
- 5.Pressler V, McNamara JJ. Aneurysm of the thoracic aorta. Review of 260 cases. J Thorac Cardiovasc Surg. 1985;89:50–54. [PubMed] [Google Scholar]