

The ‘lockdown’ of the United Kingdom on 23 March had pronounced impacts on travel patterns. As many millions of people moved to either working at home or were furloughed from their jobs, there were large decreases in trips to workplaces alongside even steeper decreases in recreational journeys.1 Transport is an often overlooked influence on the health of populations and health inequalities, affecting physical activity, road traffic incidents and air pollution, in addition to being a major contributor to climate change. There is ongoing uncertainty around the longer-term trajectory of COVID-19, including risks of a second wave, meaning that the medium-term changes to transport and society are hard to predict. Nevertheless, the current easing of the lockdown in England presents both opportunities and threats to the health impacts of transport.
A key factor is reduced capacity on public transport networks due to social distancing rules, meaning that many people will have to rethink their travel choices. This group faces three broad options: changing to walking or cycling (active travel); staying at home; or using a car or motorcycle. The availability of and ability to use these choices is socio economically patterned, with many low-income workers having fewer options than their higher-income counterparts. Low-income workers are less likely to be able to work at home, as are younger people.2 Physically active travel modes allow people to incorporate physical activity into their daily routines, and systematic review evidence points to health benefits.3 For example, people cycling to work are at reduced risks of death from any cause, people walking to work are at reduced risk of incident cancer, and people who change from driving to work to active modes have a reduced body mass index (BMI).4,5 In addition to these individual impacts on disease, increased walking and cycling reduce air pollution and greenhouse gases. Seventy-seven per cent of distance travelled in 2018 and 61% of trips in England and Wales were by car, meaning that there is considerable scope to increase walking and cycling.6 The potential impacts of changing these patterns are substantial; modelled estimates from a scenario with a quarter of the English population cycling regularly suggest an 11% decrease in all-cause mortality.7
The potential health impacts of large numbers of people staying at home are more difficult to predict. Among the working population, the journey to work can be a significant proportion of daily physical activity, and the average user of public transport for commutes achieves 21 min per day of physical activity by walking to and from transport interchanges.8 This means that 34% of these public transport users achieved recommended levels of physical activity from these journeys alone, ranging from 52% of train users to 21% of bus users. While this varies both across transport modes and socio-demographics, it highlights that, on average, people would need to add another 20 min of physical activity daily if they are going to work at home full-time. The evidence from longitudinal studies to assess the health impacts of public transport use is limited, but a recent systematic review and meta-analysis of available studies suggest a BMI decrease of 0.30 kg/m2 associated with public transport use.9 If people are going to forego this physical activity, other forms of physical activity would have to increase to negate negative impacts on health. Survey data asking participants about their levels of physical activity before and after lockdown indicate that overall levels did not change, which would indicate people were compensating for reduced transport activity.10 However, these population changes may mask differences across socio-economic groups as maintaining physical activity during lockdown was linked to greenspace access and garden ownership, which are both lower in deprived areas. One further potential impact of the COVID-19 lockdown is that there may be a long-term increase in home delivery services. Impacts of this are difficult to predict, but this may increase road use by delivery vehicles with negative impacts on air pollution and emissions, as well as decreasing opportunities for physical activity, i.e. walking to shops.
If public transport journeys are replaced by greater car use, there will be detrimental impacts on individual and population health as well as air pollution and greenhouse gas emissions. Evidence from China suggests that stringent travel restrictions implemented from 25 January have been linked to improved air quality and decreased mortality.11 Transport is a major driver of air pollution in the UK, which account for almost one-quarter of greenhouse gas emissions. Public Health England notes that the costs to society of reliance on car use remain high.12 Data from the Department for Transport (Figure 1) show signs that car use may be returning to pre-lockdown levels. For example, car use in April was close to 30% of that seen in the same time period last year, but by 1 June this had returned to 65%.
Figure 1.
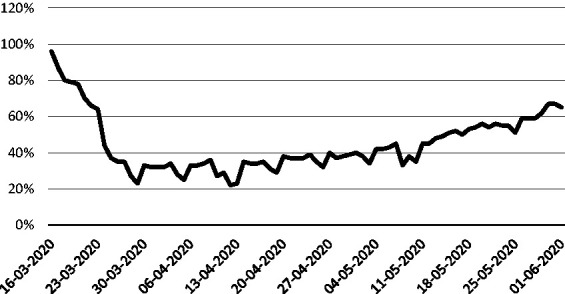
Daily car use in 2020 as percentage of 2019 levels.
Data source: Department for Transport: Transport use during the coronavirus (COVID-19) pandemic data series. Available from https://www.gov.uk/government/statistics/transport-use-during-the-coronavirus-covid-19-pandemic.
Options to increase active travel and decrease car use
With private motor vehicles accounting for most journeys, the UK has some way to go to achieving levels of active travel in neighbouring European countries, especially the Netherlands and Germany. However, lessons can be increasingly learnt from within the UK, with some cities making substantial progress in changing commuting behaviours over recent decades. London has long been an outlier in terms of travel patterns for some time, with far greater proportions of people walking or cycling to work and much less driving. Other areas have also invested in promoting more walking and cycling; Greater Manchester, for example, created the post of Walking and Cycling Commissioner in 2017 after the election of Andy Burnham as Mayor for the region.
Investing in active travel infrastructure is important, especially to address low cycling rates among women, children and ethnic minorities.13 The Government announced a range of measures on transport on 9 May. The first tranche of a £2 billion fund allocated to walking and cycling infrastructure has been released, and the government will publish an updated cycling and walking strategy in the summer.14 New guidance to local authorities has recommended altering roads to allow more dedicated space for walking and cycling, including the closure of streets to cars. Local authorities such as Westminster are introducing a range of measures including closing streets around schools to traffic, while Bath and North East Somerset are additionally working to increase the width of pavements to allow social distancing. Many people will still need to use public transport, and increased government investment will be needed to keep travel operators financially viable, while capacity is reduced due to social distancing. The government has now made it compulsory to wear face coverings on public transport, a policy also used in countries such as South Korea,15 which may allow some relaxation of social distancing rules.
In addition to encouraging people to walk or cycle more, government action is needed to discourage car use, both during the pandemic and after. Price is a key driver of consumer behaviour and people underestimate how much it costs to run a car for a year, and giving them this information may play a role in changing decisions.16 However, providing education and information will likely have limited impact, and bolder action is needed. One policy under active consideration in many local areas in the UK is the introduction of Road User Charging, which is typically considered among a basket of policies aimed at managing transport demand. The case for Road User Charging is premised on its ability to make the costs of driving more closely reflect the true costs to society, if externalities such as accidents and pollution are considered. London led the way here with the first major UK road user-charging system, the Congestion Charge in 2003 and in April 2019 added an extra levy on vehicles not meeting strict emission standards (known as the Ultra-Low Emission Zone – ULEZ). Early evidence has suggested that the ULEZ has reduced pollution, which may add to the popularity of such schemes.17 Local authorities have the legal powers to implement Road User Charges as part of Clean Air Zones, and many such as Sheffield and Bath had well-developed plans to do so. There are signs, however, that some local authorities are considering cancelling these plans in the wake of recent upheaval. The potential role of such policies in shaping post-lockdown travel patterns remains to be seen, but the Parliamentary Transport Committee had recommended the need for a ‘national conversation’ on the issue which is now needed more than ever.
Conclusion
Transport is a fundamental part of the modern world and has profound impacts on health. Prolonged limits to public transport capacity are likely, presenting individuals and governments with an opportunity to change previously detrimental travel patterns which were overly reliant on polluting and dangerous travel modes. Support in the next few weeks and months can ensure that beneficial shifts are made and maintained, which will be crucial to reducing pollutants and addressing the climate emergency.
Declarations
Competing interests
None declared.
Funding
Funded by the National Institute for Health Research (NIHR) School for Public Health Research (grant reference number PD-SPH-2015).
Ethics approval
Not required.
Guarantor
AL.
Contributorship
AL and CM concieved the idea. All authors approved an initial plan, and AL produced a first draft. All authors approved the submitted version.
Acknowledgements
None.
Provenance
Not commissioned; editorial review
ORCID iDs
Anthony A Laverty https://orcid.org/0000-0003-1318-8439 Azeem Majeed https://orcid.org/0000-0002-2357-9858
References
- 1.Google Community Mobility Reports. See https://www.google.com/covid19/mobility/ (last checked 22 May 2020).
- 2.Davenport and Levell. Changes Down the Line: Flattening the Curve of Public Transport Use. IFS Breifing Note. See https://www.ifs.org.uk/uploads/Final-BN287-Changes-down-the-line-Flattening-the-curve-of-public-transport-use.pdf (2020, last checked 19 June 2020).
- 3.Saunders LE, Green JM, Petticrew MP, Steinbach R, Roberts H. What are the health benefits of active travel? A systematic review of trials and cohort studies. PLoS One 2013; 8: e69912–e69912. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Patterson R, Panter J, Vamos EP, Cummins S, Millett C, Laverty AA. Associations between commute mode and cardiovascular disease, cancer, and all-cause mortality, and cancer incidence, using linked Census data over 25 years in England and Wales: a cohort study. Lancet Planet Heal 2020; 4: e186–e194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Flint E, Webb E, Cummins S. Change in commute mode and body-mass index: prospective, longitudinal evidence from UK Biobank. Lancet Public Heal 2017; 1: e46–e55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Department for Transport National Travel Survey: 2018. See www.gov.uk/government/statistics/national-travel-survey-2018 (last checked 19 June 2020).
- 7.Woodcock J, Abbas A, Ullrich A, Tainio M, Lovelace R, Sá TH, et al. Development of the Impacts of Cycling Tool (ICT): a modelling study and web tool for evaluating health and environmental impacts of cycling uptake. PLoS Med 2018; 15(7) :e1002622. [DOI] [PMC free article] [PubMed]
- 8.Patterson R, Webb E, Millett C and Laverty AA. Physical activity accrued as part of public transport use in England. J Public Heal (United Kingdom). 2019; 41(2): 222–230. [DOI] [PubMed]
- 9.Patterson R, Webb E, Hone T, Millett C, Laverty AA. Associations of public transportation use with cardiometabolic health: a systematic review and meta-analysis. Am J Epidemiol 2019; 188: 785–795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Rogers NT, Waterlow N, Brindle E, Enria L, Eggo RM, Lees S, et al. Behavioural Change Towards Reduced Intensity Physical Activity is Disproportionately Prevalent among Adults with Serious Health Issues or Self-perception of High risk During the UK COVID-19 Lockdown. MedRxivhttps://www.medrxiv.org/content/10.1101/2020.05.12.20098921v1. [DOI] [PMC free article] [PubMed]
- 11.Chen K, Wang M, Huang C, Kinney PL and Anastas PT. Air pollution reduction and mortality benefit during the COVID-19 outbreak in China. The Lancet Planetary Health 2020; 4(6): E210–E212. [DOI] [PMC free article] [PubMed]
- 12.Public Health England. Working Together to Promote Active Travel: A briefing for local authorities. See https://goo.gl/SUwmWc (2016, last checked 19 June 2020).
- 13.Department for Transport. Walking and Cycling Statistics, England: 2018. See https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/821842/walking-and-cycling-statistics-2018-accessible.pdf (2019, last checked 19 June 2020).
- 14.Department for Transport. Statutory Guidance Reallocating Road Space in Response to COVID-19: Statutory Guidance for Local Authorities. See https://www.gov.uk/government/publications/reallocating-road-space-in-response-to-covid-19-statutory-guidance-for (2020, last checked 19 June 2020).
- 15.Majeed A, Seo Y, Heo K, Lee D. Can the UK emulate the South Korean approach to covid-19? BMJ 2020; 369: m2084–m2084. [DOI] [PubMed] [Google Scholar]
- 16.Andor MA, Gerster A, Gillingham KT and Horvath M. Running a car costs much more than people think – stalling the uptake of green travel. Nature 2020; 580(7804): 453–455. [DOI] [PubMed]
- 17.Mayor of London. Central London Ultra low Emission Zone –Six Month Report. See https://www.london.gov.uk/sites/default/files/ulez_six_month_evaluation_report_oct19.pdf (2019, last checked 19 June 2020).