

Introduction
The most prevalent form of atrioventricular nodal reentrant tachycardia (AVNRT) is the slow-fast type, with a 1:1 atrioventricular (AV) ratio. Cases of AVNRT with 2:1 AV ratio have been reported. In this case report, we present a case of syncopal episode and a supraventricular tachycardia with different degrees of AV block.
Case report
A 48-year-old woman with a history of multiple episodes of paroxysmal supraventricular tachycardia converted to sinus rhythm with intravenous adenosine presented to our emergency department with syncope not preceded by palpitations and without vasovagal characteristics.
The resting electrocardiogram was normal. The carotid sinus massage and active standing test were negative for the diagnosis of carotid sinus hypersensitivity and orthostatic hypotension, respectively. Transthoracic echocardiogram ruled out structural heart disease. An electrophysiological study was indicated.
With the use of conventional fluoroscopy, 3 multipolar catheters (4-polar, 10-polar, and 4-polar) were introduced, which were initially placed in the His region, inside the coronary sinus, and in the right ventricle.
The baseline conduction intervals were normal (PA = 35 ms, AH = 53 ms, and HV = 41 ms). The atrial stimulation protocol with programmed extrastimulation demonstrated a decremental and discontinuous AV conduction with the presence of AH jump and nodal echoes. We were able to induce, reproducibly, a regular narrow QRS tachycardia with a cycle length of 310 ms, with 1:1 AV conduction with concentric retrograde atrial activation and a septal ventriculoatrial (VA) interval less than 60 ms. Tachycardia spontaneously terminated with an atrial event. The same tachycardia was able to be induced with burst pacing from the right ventricle. During tachycardia the AV conduction spontaneously changed and the AV ratio became 2:1, maintaining a fixed VA interval of less than 60 ms and without changes in the sequence of atrial activation or cycle length. This ruled out the possibility of an AV reentrant tachycardia by an accessory pathway. The fusion between the blocked P wave and the previous T wave on surface electrocardiogram configured an electrocardiographic sign known as “the kiss of the girl from Ipanema”1 (Figure 1). During the presence of the blocked P waves, only the presence of the atrial electrogram was observed without the presence of the His electrogram.
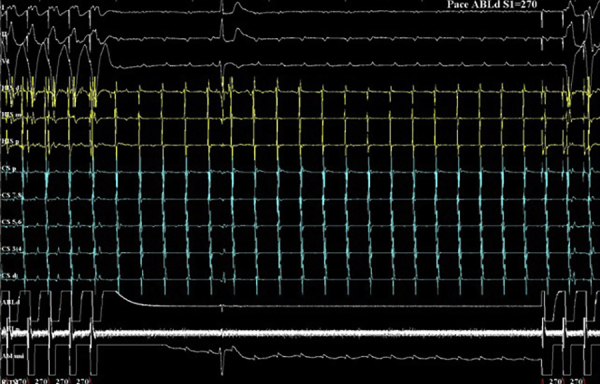
Figure 1.

Supraventricular tachycardia with 2:1 atrioventricular ratio and maintaining a ventriculoatrial interval less than 60 ms. Tachycardia cycle length of 312 ms. Red circle marks the sign of “the kiss of the girl from Ipanema.”
Subsequently there was a dissociation between atrial and ventricular activity, with the presence of His electrogram always preceding the ventricular activity and with variable HA and VA intervals (Figure 2A), with return to a 1:1 AV ratio seconds later. Faster ventricular stimulation was performed to entrain the tachycardia in order to assess the V-A-V response, to eliminate the possibility of atrial tachycardia; however, the response was an AV block, with a single escape for 6 seconds. Owing to the absence of ventricular escape rhythm, brief ventricular stimulation was performed with subsequent maintenance of the tachycardia and return of the 1:1 AV ratio (Figure 3).
Figure 2.

A: Tachycardia with dissociation of atrial and ventricular activity, and variable ventriculoatrial intervals. His electrogram always preceding the ventricular activity. B: Schematic representation of the atrioventricular block mechanism during supraventricular tachycardia. A = atrium; LCP = lower common pathway; UCP = upper common pathway; V = ventricle.
Figure 3.
Continuation of tachycardia after attempted of entrainment from the right ventricle. Tachycardia with atrioventricular (AV) block with pause of 6 seconds with subsequent ventricular stimulation and return of the 1:1 AV ratio. ABLd = right ventricle.
Owing to the findings compatible with slow-fast AVNRT, radiofrequency lesions were created between coronary sinus ostium and tricuspid annulus, in the “P2” region where high-frequency potentials were recorded, where accelerated junctional beats were induced during the delivery of the radiofrequency current. Ablation of the slow pathway was performed, with the absence of induction of arrhythmias after the ablation. The patient remained asymptomatic for the next 3 months.
Discussion
This case describes a patient with supraventricular tachycardia with a VA interval of less than 60 ms and with various degrees of AV block during tachycardia, suggesting as possible causes focal atrial tachycardia and slow-fast AVNRT. However, the reproducible induction of tachycardia following the presence of AH jump and nodal echo, the ability to be induced with ventricular burst pacing, and the spontaneous termination with atrium as the last event define AVNRT as the mechanism causing tachycardia. This case also shows alternation in the AV ratio, from a tachycardia with a 2:1 AV block to the absence of ventricular activity triggered by an attempt to entrain tachycardia from the right ventricle. The available evidence supports that it could be a functional block at level of the His bundle (HB), owing to the following characteristics:
-
(1)
The HB block may or may not show the presence of His potential. Man and colleagues2,3 demonstrate that in cases of blockage at the HB (intrahisian level), His potential can be a very low amplitude and have no apparent signal.
-
(2)
The 2:1 AV block during tachycardia could be caused by a functional phase 3 block at the HB and this behavior is maintained owing to the phenomenon known as the long-short activation sequence, typical of the HB.4
-
(3)
There is evidence that ventricular stimulation or spontaneous ventricular activity may change the AV ratio of tachycardia from 2:1 to 1:1, because the retrograde depolarization of the HB by the ventricular stimulus eliminates the long-short activation sequence in the HB by peeling back and shortening the effective refractory period, and thus recovers the antegrade conduction to 1:1.4,5
However, the case described shows other findings that differ from previously published cases. As is the case in spontaneous AV dissociation with the presence of His potential exclusively when ventricular activity is present (Figure 2A), this is probably because the initial portion of HB activated, during intrahisian block, is so small that it produces an unrecognizable low-voltage potential in the intracavitary registry; or owing to the presence of a lower common pathway that causes a changing relationship between the His potential and the atrial electrogram, sometimes producing an atrial electrogram that precedes the His potential until a block, probably functional, occurs without the presence of His potential6 (Figure 2B). The presence of common pathways is less likely to be present due to a variable histological architecture and the scant expression of connexin isoforms in the AV node. Thus the presence of AV block during AVNRT is just an expression of longer refractory period below the arrhythmia circuit.7
Another finding is the presence of a total AV block with a long pause after ventricular stimulation (Figure 3), which is probably due to a refractoriness of the right and left bundle branches, produced by the retrograde activation of these structures compatible with functional block. The restoration of the 1:1 AV ratio post a new ventricular pacing could be due to a peeling-back phenomenon of the refractory period of the right and left bundle branches, indicating a probable location of the functional blockade at the intrahisian level.4
Another interesting finding is the presence of the electrocardiographic sign known as the kiss of the girl from Ipanema,1 typical of AVNRT with a 2:1 AV ratio.
Conclusion
The findings described demonstrate the presence of a slow-fast AVNRT with atypical presentation, owing to the presence of several degrees of AV block.
The available evidence is consistent with the findings observed, describing a provable functional phase 3 block at the intrahisian level maintained for the long-short activation sequence, typical of the HB. The recovery of 1:1 conduction after ventricular stimulation can be explained by the elimination of the long-short activation sequence in the HB by peeling back of the refractory period of the right and left bundle branches. After the slow pathway ablation, no more supraventricular arrhythmias were induced. At present the evidence is limited on the exact phenomenon that produces this behavior; however, the presence of a probable lower common pathway or an intrahisian functional block are the most accepted theories so far.
Key Teaching Points.
-
•
The electrocardiographic sign known as the kiss of the girl from Ipanema is an electrocardiographic manifestation of typical atrioventricular nodal reentrant tachycardia (AVNRT) with a 2:1 atrioventricular (AV) block.
-
•
There are 2 theories to explain the presence of AV block during AVNRT: the presence of a lower common pathway or an intrahisian functional phase 3 block.
-
•
According to current evidence, AV block during AVNRT just defines a longer refractory period below the circuit.
Footnotes
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The authors have no conflicts of interest to disclose.
References
- 1.Evertz R., Brugada J. The kiss of the girl from Ipanema. Neth Heart J. 2013;21:374–376. doi: 10.1007/s12471-013-0434-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Man K.C., Brinkman K., Bogun F. 2:1 atrioventricular block during atrioventricular node reentrant tachycardia. J Am Coll Cardiol. 1996;28:1770–1774. doi: 10.1016/S0735-1097(96)00415-9. [DOI] [PubMed] [Google Scholar]
- 3.Lee S.H., Tai C.T., Chiang C.E. Spontaneous transition of 2:1 atrioventricular block to 1:1 atrioventricular conduction during atrioventricular nodal reentrant tachycardia: evidence supporting the intra-Hisian or infra-Hisian area as the site of block. J Cardiovasc Electrophysiol. 2003;14:1337–1341. doi: 10.1046/j.1540-8167.2003.03198.x. [DOI] [PubMed] [Google Scholar]
- 4.Kaneko Y., Nakajima T., Tamura S. Superior-type fast slow atrioventricular nodal reentrant tachycardia with a 2:1 atrioventricular block. J Cardiovasc Electrophysiol. 2019;30:1696–1698. doi: 10.1111/jce.14054. [DOI] [PubMed] [Google Scholar]
- 5.Sorgente A., Chierchia G.B., De Asmundis C. Stepwise transition of 2:1 atrio-ventricular block to 1:1 conduction induced by ventricular premature beats in a patient with atypical AVNRT. Pacing Clin Electrophysiol. 2010;33:e20–e23. doi: 10.1111/j.1540-8159.2009.02584.x. [DOI] [PubMed] [Google Scholar]
- 6.Issa Z.F., Miller J.M., Zipes D.P. 3rd ed. Elsevier; Philadelphia: 2019. Clinical Arrhythmology and Electrophysiology: A Companion to Braunwald's Heart Disease. [Google Scholar]
- 7.Katritsis D.G., Josephson M.E. Classification of electrophysiological types of atrioventricular nodal re-entrant tachycardia: a reappraisal. Europace. 2013;15:1231–1240. doi: 10.1093/europace/eut100. [DOI] [PubMed] [Google Scholar]