

Abstract
Objectives
To assess the association between age, sex, socioeconomic group, weight status and back pain risk in a large general population cohort of children.
Design and setting
A dynamic cohort of children aged 4 years in the Information System for Research in Primary Care (SIDIAP) electronic primary care records data in Catalonia. Multivariable Cox models were fitted to explore the association between back pain and weight status categories according to the WHO 2007 growth reference groups (body mass index for age z-score). Models were adjusted for age, sex, socioeconomic status and nationality.
Participants
Children seen at age 4 years at paediatric primary care clinics between 1 January 2006 and 31 December 2013 and followed up until 31 December 2016 or age 15 years.
Outcome measures
Incident back pain registered by paediatricians at primary care using the International Statistical Classification of Diseases and Health Related Problems, 10th Edition code M54.
Results
466 997 children were followed for a median 5.0 years (IQR 5.1). In multivariable models, overweight and obesity increased back pain risk, with adjusted HRs of 1.18 (95% CI 1.09 to 1.27) and 1.34 (95%CI 1.19 to 1.51) for overweight and obesity, respectively. Females were at greater risk of back pain than males with adjusted HR 1.40 (95%CI 1.35 to 1.46). Adjusted HR was 1.43 (95%CI 1.33 to 1.55) for back pain in children from the most deprived socioeconomic groups compared with the least deprived socioeconomic groups.
Conclusions
Maintaining a healthy weight from an early age may reduce the prevalence of back pain in both children and adults. Overweight female children from deprived socioeconomic groups are at greatest risk of back pain and represent a target population for intervention.
Keywords: primary care, epidemiology, paediatrics
Strengths and limitations of this study.
Large dataset of nearly half a million children.
Generalisable outcome of back pain: when parent believes pain is sufficiently severe to seek input from healthcare professionals.
Study does not address psychometric factors that play important role in the aetiology of back pain.
Long-term follow-up into adulthood not available.
Introduction
Back pain is the greatest cause of disability worldwide, and this burden continues to increase in magnitude.1 It is common among children and adolescents and may affect up to three quarters of individuals before adulthood.2 Childhood back pain results in activity limitation and school absenteeism.3 4 Pain is reported in the cervical, thoracic and lumbar spine,5 and prevalence increases with age,6 reaching levels comparable with adult populations by 18 years.7 Most studies assess self-reported pain, and the number of children and adolescents consulting healthcare professionals with back pain is not known.
There is very limited evidence for primary prevention of back pain.8 In children, only education and ergonomic school furniture have been studied but without robust evidence of benefit.9 Although interventions that incorporate exercise are effective in adults, these have not been investigated in children.8 Interventions are most likely to be successful when targeting specific risk factors in populations predisposed to developing back pain; however, predictive factors are currently not well characterised.10
The prevalence of childhood obesity and back pain are both increasing.7 11 12 Crucially, back pain during youth predicts pain in adulthood,13 14 and obesity during childhood predicts obesity in adolescence.15 Although obesity is associated with chronic back pain in adults,1 there is only limited evidence of an association during childhood.16–18 In addition, the increased prevalence of back pain in females from lower socioeconomic groups in adults1 has not been consistently reproduced in adolescent cohorts.7 Childhood obesity may represent a modifiable risk factor for back pain, and weight optimisation confers benefits beyond musculoskeletal health.
The aims of this study were: (1) to determine the incidence of community paediatrician consultations due to back pain and (w) to explore the association between back pain and age, sex, socioeconomic group and weight status in a large general population cohort of children.
Methods
Data source
Data were obtained from anonymised electronic medical records from the Sistema d’Informació pel Desenvolupament de l’Investigació en Atenció Primària (SIDIAP; www.sidiap.org) (Information System for Research in Primary Care). The database includes longitudinal data on patient demographics, clinical visits to primary care centres and International Statistical Classification of Diseases and Health Related Problems, 10th Edition (ICD-10) coded health problems from 296 primary care centres in Catalonia. Data are available for greater than 80% of the 7.5 million population of Catalonia, totalling more than 1.1 million children under the age of 15 years.
Population
The cohort included all children assessed at age 4 years (±6 months) by a paediatric doctor or nurse in any of the contributing primary care centres between 1 January 2006 and 31 December 2016 with at least one valid height and weight measurement recorded in the SIDIAP database (figure 1). These assessments represent a routine paediatric health surveillance programme within the region.
Figure 1.
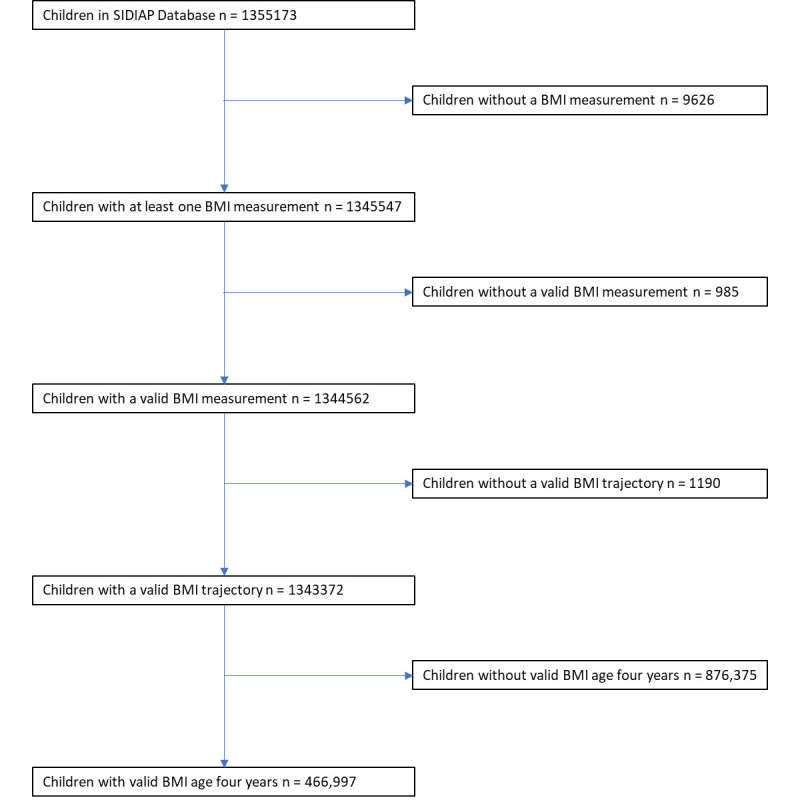
Study population flow chart. BMI, body mass index; SIDIAP the Information System for Research in Primary Care.
Study design
A dynamic cohort study was conducted with longitudinal data extraction for all participants from their index appointment (age 4 years old±6 months) until the earliest of: the date they reached 15 years of age (when individuals transition to adult care), migration away from a Catalan Institute of Health centre, death or end of study (31 December 2016).
Study exposures and outcomes
Recorded exposures included patient demographics measured at the index appointment of a screening programme: age (months), sex, height (metres), weight (kg), socioeconomic group and nationality. Age and sex referenced BMI (body mass index for age z-score (BMIz)) was calculated according to the WHO 2007 guidance, and children were categorised as ‘underweight’, ‘normal weight’, ‘overweight’ or ‘obese’.19 These weight status categories represent the number of SD away from the mean: underweight <−2, normal weight −2 to +2, overweight >+2 and obesity >+3. Biologically implausible values of BMIz were excluded according to WHO Expert Committee 1995 guidance, and implausible values in growth trajectory data up to the age of 10 years were identified using a conditional growth percentile model.20 Socioeconomic group was measured using the MEDEA (Mortalidad en áreas pequeñas Españolas y Desigualdades Socioeconómicas y Ambientales) deprivation index calculated using five census-based socioeconomic indicators: unemployment, manual occupation, temporary employment, illiterate adults and school leavers before 16 years of age. Group 1 represents the least deprivation and group 5 the most deprivation. MEDEA categories also include rural communities and unclassified urban communities.
Outcomes were ascertained from diagnoses recorded in primary care paediatric records during visits to contributing health centres between 1 January 2006 and 31 December 2016 in the Catalan universal healthcare system. Prespecified ICD-10 codes were used to identify first episodes of back pain after 4 years of age: lumbar spine pain (M54.1, M54.3, M54.4 or M54.5), thoracic back pain (M54, M54.6, M54.8 or M54.9) or cervical spine pain (M54.2).
Statistical analysis
Population demographics were expressed as frequencies and percentages for categorical data and means and SD or medians and IQR for continuous data where appropriate. Cumulative incidence was calculated using actuarial lifetables for first time event of a recorded code of interest (lumbar, thoracic or cervical spine pain) and stratified for weight category. Results were tabulated and expressed as Kaplan-Meier plots.
Multivariable Cox models were used to explore the association between back pain and weight categories (BMIz), adjusted for age, sex, nationality (Spanish or other) and socioeconomic group (MEDEA). Weight categories and socioeconomic status groups were treated as factor variables. Age was treated as a continuous variable. MEDEA scores were categorised into quintiles to minimise risk of reidentification.
A prespecified interaction between weight category and sex was tested by introducing a multiplicative term in the Cox equation. Sex-stratified results are reported where the p value for interaction appeared borderline significant (p<0.1). A sensitivity analysis was conducted making further adjustment for birth weight as a marker of genetic and/or in utero conditioning of adiposity.
Patient and public involvement
There was no patient and public involvement in this study.
Results
A total of 466 997 children were included in the study with median follow-up 5.03 years (IQR 5.11). A total of 21 638 and 150 children were transferred out or died during follow-up, respectively. Participant demographics at the initial assessment, stratified by baseline WHO weight categories (BMIz) are summarised in table 1.
Table 1.
Baseline characteristics of the included and excluded study population
| Included | Excluded (no BMI available at age 48±6 months) |
|||||||||
| Total | Normal weight |
Overweight | Obese | Underweight | Total | Normal weight | Overweight | Obese | Underweight | |
| Participants | ||||||||||
| N (%) | 466 997 | 430 681 (92.2) |
26 526 (5.7) |
9 250 (2.0) |
540 (0.1) |
336 924 | 278 030 (82.5) |
37 052 (11.0) |
19 546 (5.8) |
2 296 (0.7) |
| BMIz* | ||||||||||
| Mean (SD) | 0.46 (1.09) |
0.80 (0.88) |
2.40 (0.28) |
3.66 (0.51) |
−3.51 (0.47) |
0.43 (1.17) |
0.11 (0.87) |
1.72 (0.50) |
2.91 (0.73) |
−2.71 (0.64) |
| Age in months | ||||||||||
| Mean (SD) | 49.13 (2.00) |
49.13 (1.99) |
49.13 (2.01) |
49.15 (2.11) |
49.06 (2.50) |
54.30 (36.61) |
49,00 (34.58) |
76,69 (36,85) |
83.53 (31.80) |
85.72 (39,24) |
| Age in months | ||||||||||
| Female N (%) | 226 868 (48.58) |
210 274 (48.8) |
12 455 (47.0) |
3891 (42.1) |
248 (45.9) |
162 842 (48.3) |
136 061 (48.9) |
17 981 (39.8) |
7771 (48.5) |
1029 (44.8) |
| Socioeconomic status | ||||||||||
| Rural N (%) | 94 825 (20.3) |
88 571 (93.4) |
4 666 (4.9) |
1 488 (1.6) |
100 (0.1) |
59 418 (17.6) |
49 898 (84.0) |
6110 (10.3) |
3006 (5.1) |
404 (0.7) |
| Urban quintile 1 (least deprived area) | 57 439 (12.3) |
53 877 (93.8) |
2 750 (4.8) |
761 (1.3) |
51 (0.1) |
50 398 (15.0) |
42 208 (83.7) |
5557 (11.0) |
2284 (4.5) |
349 (0.7) |
| Urban quintile 2 | 68 720 (14.7) |
63 799 (92.8) |
3 715 (5.4) |
1 126 (1.6) |
80 (0.1) |
47 392 (14.1) |
38 886 (82.1) |
5471 (11.5) |
2734 (5.8) |
301 (0.6) |
| Urban quintile 3 | 71 416 (15.3) |
65 660 (91.9) |
4 170 (5.8) |
1 507 (2.1) |
79 (0.1) |
47 313 (14.0) |
38 274 (80.9) |
5564 (11.8) |
3145 (6.6) |
330 (0.7) |
| Urban quintile 4 | 72 801 (15.6) |
66 407 (91.2) |
4 569 (6.3) |
1 746 (2.4) |
79 (0.1) |
49 127 (14.6) |
39 808 (81.0) |
5755 (11.7) |
3239 (6.6) |
325 (0.7) |
| Urban quintile 5 (most deprived area) |
77 129 (16.5) |
69 581 (90.2) |
5 259 (6.8) |
2 172 (2.8) |
117 (0.2) |
55 468 (16.5) |
44 928 (81.0) |
6134 (11.1) |
3962 (7.1) |
444 (0.8) |
| Missing address | 24 667 (5.3) |
22 786 (92.4) |
1 397 (5.7) |
450 (1.8) |
34 (0.1) |
27 808 (8.3) |
24 028 (86.4) |
2461 (8.8) |
1176 (4.2) |
143 (0.5) |
| Nationality | ||||||||||
| Spanish N (%) | 415 829 (89.04) |
383 739 (89.10) |
23 568 (88.80) |
8083 (87.40) |
439 (81.30) |
272 974 (81.0) |
225 915 (81.3) |
29 833 (80.5) |
15 669 (80.2) |
1557 (67.8) |
| Other N (%) | 51 168 (10.96) |
46 942 (10.90) |
2958 (11.20) |
1167 (12.6) |
101 (18.70) |
63 950 (19.0) |
52 115 (18.7) |
7219 (19.5) |
3877 (19.8) |
739 (32.2) |
*BMIz measured age 48±6 months for included participants and measurement closest to age 4 (but <3.5 and >4.5) years available for those included.
BMIz, body mass index for age z-score.
The 11-year cumulative incidence of individuals diagnosed with back pain at any site by a community paediatrician increased with age and reached 8.93% (95% CI 8.61% to 9.25%) by age 15 years (figure 2 and online supplemental figure 1).
Figure 2.

Age-specific cumulative incidence (95% CI) of back pain at any site.
bmjopen-2019-036023supp001.pdf (200.1KB, pdf)
Back pain was most frequently experienced in the lumbar region and the cumulative incidence during childhood (age 4–15 years old) at different sites was 4.33% (95% CI 4.08% to 4.58%) for lumbar pain, 2.46% (95% CI 2.29% to 2.63%) for thoracic pain and 2.86% (95% CI 2.71% to 3.01%) for cervical pain (table 2).
Table 2.
Cumulative incidence of back pain stratified by age, sex and site of pain
| Cumulative incidence (%) | 95% CI | |
| All participants | 8.93 | 8.62 to 9.25 |
| Sex | ||
| Female | 10.31 | 9.82 to 10.80 |
| Male | 7.62 | 7.20 to 8.03 |
| BMIz categories | ||
| Underweight | 4.08 | 1.20 to 6.95 |
| Normal weight | 8.78 | 8.45 to 9.12 |
| Overweight | 10.14 | 8.89 to 11.39 |
| Obese | 11.83 | 9.43 to 14.24 |
| Site of pain | ||
| Cervical | 2.86 | 2.71 to 3.01 |
| Thoracic | 2.46 | 2.29 to 2.63 |
| Lumbar | 4.33 | 4.08 to 4.58 |
BMIz, body mass index for age z-score.
Cumulative risk was higher in females (10.31% (95% CI 9.82% to 10.80%)]) than males (7.62% (95% CI 7.20% to 8.03%)) and increased with weight category: underweight 4.08% (95% CI 1.20% to 6.95%), normal weight 8.78% (95% CI 8.45% to 9.12%), overweight 10.14% (95% CI 8.89% to 11.39%) and obese 11.83% (95% CI 9.43% to 14.24%).
Individuals classified as overweight or obese had an increased risk of developing back pain at any site. This association remains present when adjusting for age, sex, socioeconomic group and nationality. In the multivariable cox regression model, low socioeconomic group, female sex and non-Spanish nationality all increased the risk of back pain (table 3). There was no interaction between sex and weight categories (p=0.86).
Table 3.
Crude and multivariable Cox regression models with HRs for development of back pain at any site
| Univariate | Multivariable* | |||
| HR | 95% CI | HR | 95% CI | |
| Age | ||||
| Months | 1.02 | 1.01 to 1.03 | 1.02 | 1.01 to 1.03 |
| Sex | ||||
| Male | Ref | – | – | – |
| Female | 1.40 | 1.35 to 1.46 | 1.40 | 1.35 to 1.46 |
| BMIz categories | ||||
| Underweight | 0.78 | 0.41 to 1.50 | 0.78 | 0.41 to 1.51 |
| Normal range | Ref | – | – | – |
| Overweight | 1.18 | 1.10 to 1.27 | 1.18 | 1.09 to 1.27 |
| Obese | 1.34 | 1.20 to 1.51 | 1.34 | 1.19 to 1.51 |
| Socioeconomic status | ||||
| Rural area | 1.29 | 1.20 to 1.38 | 1.29 | 1.20 to 1.39 |
| Urban quintile 1 | Ref | – | – | – |
| Urban quintile 2 | 1.16 | 1.07 to 1.25 | 1.16 | 1.07 to 1.25 |
| Urban quintile 3 | 1.28 | 1.18 to 1.38 | 1.27 | 1.18 to 1.38 |
| Urban quintile 4 | 1.32 | 1.23 to 1.43 | 1.33 | 1.23 to 1.44 |
| Urban quintile 5 | 1.41 | 1.31 to 1.52 | 1.43 | 1.33 to 1.55 |
| Urban not classified | 1.32 | 1.19 to 1.47 | 1.32 | 1.18 to 1.47 |
| Nationality | ||||
| Spanish | Ref | – | – | – |
| Other | 0.75 | 0.69 to 0.82 | 0.73 | 0.67 to 0.79 |
*Adjusted for all the variables reported on in this same table.
BMIz, body mass index for age z-score.
The association between weight category and back pain was maintained when stratifying for lumbar, thoracic and cervical spine pain (online supplemental tables 1-3). Obese children had an increased risk of developing pain in all areas of the back compared with individuals with a normal weight status. In each of the lumbar, thoracic and lumbar regions, females remained at greatest risk of back pain, as did individuals in the most deprived socioeconomic groups compared with the least deprived socioeconomic groups.
Birth weight was available for 310 772 (66.55%) of the participants, and inclusion as a covariable in the cox regression model did not modify the observed associations (data not shown). Birth weight was not associated with back pain other than in the cervical region, with adjusted HR of 1.10 (95% CI 1.02 to 1.20) per kg increase in weight at birth (online supplemental table 4).
Discussion
Almost 1 in 10 children develop at least one episode of back pain during childhood, and lower back (lumbar) pain is the most common site. This study demonstrates that children who are overweight or obese at an early age have an increased risk of developing back pain during childhood. The cumulative incidence of back pain diagnosed by community paediatricians increased with age and was almost 9% in children with a normal weight, compared with almost 12% for obese children. Adjusting for age, sex, socioeconomic status and nationality, a child with obesity has a 34% excess risk of developing back pain before the age 15 years. Female children are 40% more likely to develop back pain than males, and children from most deprived socioeconomic groups are at a more than 40% higher risk of developing back pain than those of the least deprived socioeconomic groups.
The incidence of back pain in this study is lower than in other cohorts, where reported lifetime prevalence during adolescence ranges from 4.7% to 74.4%2 with a mean lifetime prevalence of 40% (95% CI 34% to 54%) in 30 studies.7 The large variation in reported prevalence most likely reflects the different tools used to diagnose back pain, which in most studies is self-reported, as well as the population characteristics. Studies to date have recruited individuals from educational or community institutions. In our study, back pain was diagnosed by community paediatricians and only includes children with pain sufficiently severe to seek input from healthcare services.
Existing literature reports inconsistent associations between childhood back pain and BMI.21 22 A systematic review of studies including 5567 participants categorised into normal weight or overweight, concluded that overweight children are at increased risk of lower back pain with a risk ratio of 1.42 (95% CI 1.03 to 1.97); however, the included studies offer only low-quality evidence.17 Our results demonstrate that children who are overweight or obese have an increased risk of developing back pain in the lumbar, thoracic and cervical spine, after adjustment for confounding factors. Furthermore, there is a suggestion of a dose–response relationship between back pain and weight categories.
As with weight categories, there is conflicting evidence regarding the association between sex and childhood back pain. Some studies report no difference between sexes22–24 and others report a higher prevalence in females.25–27 A meta-analysis of 27 studies revealed no statistically significant relationship between sex as lifetime prevalence.7 Our study demonstrates a higher prevalence of back pain in females, as demonstrated in adult cohorts,28 and was the case for the lumbar, thoracic and cervical spine.
Adults with chronic back pain are more likely to have received less education and have lower household income.29 Children of mothers with no educational qualifications are more likely to report frequent complaints of headache, stomach ache or sickness than children of mothers a higher degree (risk ratio of 2.06, 95% CI 1.64 to 2.59).30 Studies have not found an association between socioeconomic status and the prevalence of childhood back pain,31–34 although there is evidence that childhood socioeconomic status may affect the risk of developing back pain as an adult.35 Our cohort demonstrated a clear association between ecological socioeconomic status and childhood back pain with a monotonic association, and studies suggest this trend continues into adulthood.35
Study strengths include the large dataset of nearly half a million children, which to our knowledge is the largest study exploring risk factors for childhood back pain. The outcome is a standardised measure of back pain, which is when a child or their parent believes the back pain is sufficiently severe to seek input from healthcare services. Diagnosis is then confirmed by a community paediatrician. The diagnosis of back pain in this cohort is therefore likely to represent a severe episode of pain, although there are no data on the duration, relief or aggravation of symptoms.
Most epidemiological studies use patient reported outcome measures to diagnose back pain; however, this does not evaluate access to healthcare services, which is key from a health economics perspective. The comprehensive SIDIAP database makes it possible to adjust for salient confounding variables, identified as age, sex, socioeconomic status and nationality, which confirmed overweight or obese weight categories are independent risk factors for back pain. Despite adjustment for confounding factors, there may be other important factors that have not been considered. Psychometric factors play an important role in the aetiology of back pain and have not been evaluated in this study,21 nor have physical activity levels or ergonomics of child’s environment. In addition, weight categories were established based on age and sex referenced BMI using WHO guidance19 but may not accurately reflect cardiometabolic health.36
Long-term follow-up of this cohort into adulthood is not currently available. While this study demonstrates an association between weight status and back pain during childhood, it does not provide evidence of causation. Furthermore, it is not known whether the findings in this cohort are representative of other populations, such as children from USA, where there are higher rates of obesity; however, Spain has among the highest rates of obesity in Europe.37 There were an insufficient number of underweight participants to draw conclusions regarding back pain in this population group, where there is likely to be a higher proportion of patients with systemic medical conditions. Also, a higher proportion of participants were overweight or obese in participants without a valid BMIz at 4-year follow-up assessment. An area not addressed by this study is whether children with back pain at one site are more likely to also present with back pain at a different site. There may also be variation in how clinicians code back pain, particularly when anatomically differentiating the lumbar, thoracic and cervical regions.
Obesity is associated with back pain in adults,38 39 and our study demonstrates that this association is already evident during childhood. Critically, childhood back pain has been shown to predict back pain in adults,13 14 potentially after the initiation of pathology or persistence of risk factors.40 Our study does not quantify the duration of symptoms but chronic pain may continue into adulthood.
A longitudinal study of the British Birth Cohort suggests back pain is unlikely to be a cause of obesity given the absence of a temporal association.24 Reasons for the increased risk of back pain in overweight or obese children are not known, but the aetiology may be mechanical, biological or psychological.1 The absence of an association between birth weight and back pain suggests it is weight gain at a young age that increases the risk of back pain. Crucially, strategies to reduce the prevalence of back pain in adulthood may be most effective when commenced during childhood.
There is very limited evidence for primary prevention of back pain, particularly in children.8 In adolescent populations, only education and ergonomic school furniture have been studied. There is moderate quality evidence that education is not effective and very low quality evidence that ergonomically designed furniture could prevent back pain compared with conventional furniture.9 Exercise, particularly when combined with education, can prevent back pain in adulthood and warrants investigation in child populations.8
The highest risk population for developing back pain is obese females from deprived socioeconomic groups. These individuals should be the priority target for intervention. Tacking childhood obesity may reduce the prevalence of back pain both in children and adults, in addition to conferring other health benefits. The role for early intervention is further supported by a recent study demonstrating that the most rapid gain in weight during childhood is observed between 2 and 6 years of age.15 An improved understanding of how socioeconomic factors influence back pain and obesity may facilitate the development of novel preventative strategies. In addition to physical activity levels, diet and environmental exposures, cultural beliefs and differing thresholds for consulting healthcare practitioners by socioeconomic group may play a role.41 The additional observation that a higher proportion of underweight individuals are of non-Spanish nationality may have implications for migrant health and warrants further investigation.
Conclusion
Children who are overweight or obese are at a significantly increased risk of developing back pain. The incidence of back pain increases with age and is highest in overweight females from deprived socioeconomic groups. Given childhood back pain predicts back pain in adulthood, it is recommended that preventative strategies commence at an early age. Strategies should include ensuring children maintain a normal healthy weight.
Supplementary Material
Footnotes
Twitter: @AJRPalmer, @TDuarte_Salles
Presented at: An abstract entitled ‘Childhood obesity is associated with back pain: a cohort study of 466,997 individuals’ was presented at the International Society for Pharmacoeconomics and Outcomes Research Europe 2018 conference in Barcelona on the 10–14 November 2019 as a poster presentation. The abstract was published in Value in Health, October 2018, Volume 21, Supplement 3, Page S290, DOI: https://doi.org/10.1016/j.jval.2018.09.1729.
Contributors: JLP, DM-L, JdB, TD-S and DP-A designed the study. JLP and DP-A performed the statistical analysis. AJP and DP-A drafted the manuscript. All authors contributed to the data interpretation, revised manuscript drafts, approved the final version and contributed intellectually important content. DP-A attests that all authors meet authorship requirement and that no others meeting the criteria have been omitted. DP-A is the guarantor of the paper and takes responsibility for the integrity of the work from inception to published article.
Funding: Funding was received from La Marató de TV3 Foundation (Grant Number: 2 01 621–30). TD-S is funded by the Department of Health of the Generalitat de Catalunya (Strategic Plan for Research and Innovation in Health (PERIS) 2016–2020 Modality Incorporation of Scientists and Technologists. Grant Number: SLT002/16/00308). DP-A is funded by a National Institute for Health Research Clinician Scientist award (CS-2013-13-012). AJP is funded by a National Institute for Health Research Academic Clinical Lectureship. The research was supported by the National Institute for Health Research (NIHR) Oxford Biomedical Research Centre.
Disclaimer: The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf. No conflicts of interest are declared in relation to the submitted work. Outside of the submitted work, DM-L receives personal fees from Amgen, Lilly, Novartis, Ferrer and Rubió. DP-A received research grants from Les Laboratoires Servier, Amgen and UCB Biopharma SRL. DP-A also received advisory, speaker and consultancy fees paid to his department from UCB and Amgen.
Patient consent for publication: Not required.
Ethics approval: Scientific approval was obtained from the SIDIAP Scientific Committee and ethical approval was granted by CEIC Idiap Jordi Gol (reference number P16/179).
Provenance and peer review: Not commissioned; externally peer reviewed.
Data availability statement: Data may be obtained from a third party and are not publicly available. In accordance with current European and national law, the data used in this study are only available for the researchers participating in this study. Thus, we are not allowed to distribute or make publicly available the data to other parties. However, researchers from public institutions can request data from SIDIAP and other sources (eg, Cancer Registries) if they comply with certain requirements. Further information is available online (https://www.sidiap.org/index.php/menu-solicitudes-en/application-proccedure) or by contacting Anna Moleras (amoleras@idiapjgol.org).
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
References
- 1.Hartvigsen J, Hancock MJ, Kongsted A, et al. What low back pain is and why we need to pay attention. Lancet 2018;391:2356–67. 10.1016/S0140-6736(18)30480-X [DOI] [PubMed] [Google Scholar]
- 2.Jeffries LJ, Milanese SF, Grimmer-Somers KA. Epidemiology of adolescent spinal pain: a systematic overview of the research literature. Spine 2007;32:2630–7. 10.1097/BRS.0b013e318158d70b [DOI] [PubMed] [Google Scholar]
- 3.Skoffer B. Low back pain in 15- to 16-year-old children in relation to school furniture and carrying of the school bag. Spine 2007;32:E713–7. 10.1097/BRS.0b013e31815a5a44 [DOI] [PubMed] [Google Scholar]
- 4.Bejia I, Abid N, Ben Salem K, et al. Low back pain in a cohort of 622 Tunisian schoolchildren and adolescents: an epidemiological study. Eur Spine J 2005;14:331–6. 10.1007/s00586-004-0785-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Aartun E, Hartvigsen J, Wedderkopp N, et al. Spinal pain in adolescents: prevalence, incidence, and course: a school-based two-year prospective cohort study in 1,300 Danes aged 11-13. BMC Musculoskelet Disord 2014;15:187. 10.1186/1471-2474-15-187 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.MacDonald J, Stuart E, Rodenberg R. Musculoskeletal low back pain in school-aged children: a review. JAMA Pediatr 2017;171:280–7. 10.1001/jamapediatrics.2016.3334 [DOI] [PubMed] [Google Scholar]
- 7.Calvo-Muñoz I, Gómez-Conesa A, Sánchez-Meca J. Prevalence of low back pain in children and adolescents: a meta-analysis. BMC Pediatr 2013;13:14. 10.1186/1471-2431-13-14 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Foster NE, Anema JR, Cherkin D, et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet 2018;391:2368–83. 10.1016/S0140-6736(18)30489-6 [DOI] [PubMed] [Google Scholar]
- 9.Michaleff ZA, Kamper SJ, Maher CG, et al. Low back pain in children and adolescents: a systematic review and meta-analysis evaluating the effectiveness of conservative interventions. Eur Spine J 2014;23:2046–58. 10.1007/s00586-014-3461-1 [DOI] [PubMed] [Google Scholar]
- 10.Hill JJ, Keating JL. Risk factors for the first episode of low back pain in children are infrequently validated across samples and conditions: a systematic review. J Physiother 2010;56:237–44. 10.1016/S1836-9553(10)70006-0 [DOI] [PubMed] [Google Scholar]
- 11.Skinner AC, Ravanbakht SN, Skelton JA, et al. Prevalence of obesity and severe obesity in US children, 1999-2016. Pediatrics 2018;141:e20173459. 10.1542/peds.2017-3459 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Cunningham SA, Kramer MR, Narayan KMV. Incidence of childhood obesity in the United States. N Engl J Med 2014;370:403–11. 10.1056/NEJMoa1309753 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Brattberg G. Do pain problems in young school children persist into early adulthood? A 13-year follow-up. Eur J Pain 2004;8:187–99. 10.1016/j.ejpain.2003.08.001 [DOI] [PubMed] [Google Scholar]
- 14.Hestbaek L, Leboeuf-Yde C, Kyvik KO, et al. The course of low back pain from adolescence to adulthood: eight-year follow-up of 9600 twins. Spine 2006;31:468–72. 10.1097/01.brs.0000199958.04073.d9 [DOI] [PubMed] [Google Scholar]
- 15.Geserick M, Vogel M, Gausche R, et al. Acceleration of BMI in early childhood and risk of sustained obesity. N Engl J Med 2018;379:1303–12. 10.1056/NEJMoa1803527 [DOI] [PubMed] [Google Scholar]
- 16.Krul M, van der Wouden JC, Schellevis FG, et al. Musculoskeletal problems in overweight and obese children. Ann Fam Med 2009;7:352–6. 10.1370/afm.1005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Paulis WD, Silva S, Koes BW, et al. Overweight and obesity are associated with musculoskeletal complaints as early as childhood: a systematic review. Obes Rev 2014;15:52–67. 10.1111/obr.12067 [DOI] [PubMed] [Google Scholar]
- 18.Hestbaek L, Leboeuf-Yde C, Kyvik KO. Are lifestyle-factors in adolescence predictors for adult low back pain? A cross-sectional and prospective study of young twins. BMC Musculoskelet Disord 2006;7:27. 10.1186/1471-2474-7-27 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.de Onis M, Onyango AW, Borghi E, et al. Development of a who growth reference for school-aged children and adolescents. Bull World Health Organ 2007;85:660–7. 10.2471/BLT.07.043497 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Yang S, Hutcheon JA. Identifying outliers and implausible values in growth trajectory data. Ann Epidemiol 2016;26:77–80. 10.1016/j.annepidem.2015.10.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Jones GT, Watson KD, Silman AJ, et al. Predictors of low back pain in British schoolchildren: a population-based prospective cohort study. Pediatrics 2003;111:822–8. 10.1542/peds.111.4.822 [DOI] [PubMed] [Google Scholar]
- 22.Mohseni-Bandpei MA, Bagheri-Nesami M, Shayesteh-Azar M. Nonspecific low back pain in 5000 Iranian school-age children. J Pediatr Orthop 2007;27:126–9. 10.1097/BPO.0b013e3180317a35 [DOI] [PubMed] [Google Scholar]
- 23.Petersen S, Bergström E, Brulin C. High prevalence of tiredness and pain in young schoolchildren. Scand J Public Health 2003;31:367–74. 10.1080/14034940210165064 [DOI] [PubMed] [Google Scholar]
- 24.Lake JK, Power C, Cole TJ. Back pain and obesity in the 1958 British birth cohort. cause or effect? J Clin Epidemiol 2000;53:245–50. 10.1016/S0895-4356(99)00155-9 [DOI] [PubMed] [Google Scholar]
- 25.Watson KD, Papageorgiou AC, Jones GT, et al. Low back pain in schoolchildren: occurrence and characteristics. Pain 2002;97:87–92. 10.1016/S0304-3959(02)00008-8 [DOI] [PubMed] [Google Scholar]
- 26.Stanford EA, Chambers CT, Biesanz JC, et al. The frequency, trajectories and predictors of adolescent recurrent pain: a population-based approach. Pain 2008;138:11–21. 10.1016/j.pain.2007.10.032 [DOI] [PubMed] [Google Scholar]
- 27.Kovacs FM, Gestoso M, Gil del Real MT, et al. Risk factors for non-specific low back pain in schoolchildren and their parents: a population based study. Pain 2003;103:259–68. 10.1016/S0304-3959(02)00454-2 [DOI] [PubMed] [Google Scholar]
- 28.Hoy D, Bain C, Williams G, et al. A systematic review of the global prevalence of low back pain. Arthritis Rheum 2012;64:2028–37. 10.1002/art.34347 [DOI] [PubMed] [Google Scholar]
- 29.Shmagel A, Foley R, Ibrahim H. Epidemiology of chronic low back pain in US adults: data from the 2009-2010 National health and nutrition examination survey. Arthritis Care Res 2016;68:1688–94. 10.1002/acr.22890 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Fryer BA, Cleary G, Wickham SL, et al. Effect of socioeconomic conditions on frequent complaints of pain in children: findings from the UK millennium cohort study. BMJ Paediatr Open 2017;1:e000093. 10.1136/bmjpo-2017-000093 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Kristjánsdóttir G. Prevalence of self-reported back pain in school children: a study of sociodemographic differences. Eur J Pediatr 1996;155:984–6. 10.1007/BF02282892 [DOI] [PubMed] [Google Scholar]
- 32.Hestbaek L, Korsholm L, Leboeuf-Yde C, et al. Does socioeconomic status in adolescence predict low back pain in adulthood? A repeated cross-sectional study of 4,771 Danish adolescents. Eur Spine J 2008;17:1727–34. 10.1007/s00586-008-0796-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Jørgensen MB, Nabe-Nielsen K, Clausen T, et al. Independent effect of physical workload and childhood socioeconomic status on low back pain among health care workers in Denmark. Spine 2013;38:E359–66. 10.1097/BRS.0b013e31828435d4 [DOI] [PubMed] [Google Scholar]
- 34.Power C, Frank J, Hertzman C, et al. Predictors of low back pain onset in a prospective British study. Am J Public Health 2001;91:1671–8. 10.2105/AJPH.91.10.1671 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Lallukka T, Viikari-Juntura E, Raitakari OT, et al. Childhood and adult socio-economic position and social mobility as determinants of low back pain outcomes. Eur J Pain 2014;18:128–38. 10.1002/j.1532-2149.2013.00351.x [DOI] [PubMed] [Google Scholar]
- 36.Tomiyama AJ, Hunger JM, Nguyen-Cuu J, et al. Misclassification of cardiometabolic health when using body mass index categories in NHANES 2005-2012. Int J Obes 2016;40:883–6. 10.1038/ijo.2016.17 [DOI] [PubMed] [Google Scholar]
- 37.World Health Organisation Europe Childhood Obsesity surveillance initiative, 2018. [Google Scholar]
- 38.Zhang T-T, Liu Z, Liu Y-L, et al. Obesity as a risk factor for low back pain: a meta-analysis. Clin Spine Surg 2018;31:22–7. 10.1097/BSD.0000000000000468 [DOI] [PubMed] [Google Scholar]
- 39.Shiri R, Karppinen J, Leino-Arjas P, et al. The association between obesity and low back pain: a meta-analysis. Am J Epidemiol 2010;171:135–54. 10.1093/aje/kwp356 [DOI] [PubMed] [Google Scholar]
- 40.Dunn KM, Hestbaek L, Cassidy JD. Low back pain across the life course. Best Pract Res Clin Rheumatol 2013;27:591–600. 10.1016/j.berh.2013.09.007 [DOI] [PubMed] [Google Scholar]
- 41.Vargas CM, Stines EM, Granado HS. Health-equity issues related to childhood obesity: a scoping review. J Public Health Dent 2017;77 Suppl 1:S32–42. 10.1111/jphd.12233 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjopen-2019-036023supp001.pdf (200.1KB, pdf)