

Abstract
Objective
To review current literature and experience with Gore‐TexⓇ implant extrusion following medialization thyroplasty, as well as to report the unique case of Gore‐TexⓇ implant extrusion following revision medialization thyroplasty.
Methods
Review of existing literature and description of personal experience with unique case of Gore‐TexⓇ implant extrusion following revision medialization thyroplasty.
Results
Review of existing literature found no prior reported cases of Gore‐TexⓇ implant extrusion following revision medialization thyroplasty. Risk factors for implant extrusion include the pressure of the implant on insertion and the inability to secure the implant. Cases of implant extrusion can be managed operatively via an endoscopic or via an external open approach.
Conclusion
This is the first reported case of Gore‐TexⓇ implant extrusion following revision medialization thyroplasty. Careful consideration should be given in revision medialization thyroplasty as additional implant material may cause increased pressure, a risk factor for implant extrusion.
Keywords: Complications, Gore‐TexⓇ, Implant extrusion, Laryngoplasty, Medialization thyroplasty, Revision
INTRODUCTION
Medialization thyroplasty (MT) is the most widely used laryngeal framework surgery technique available to treat unilateral vocal fold paralysis (UVFP), enabling improvement in voice and swallowing function, and preventing life‐threatening aspiration events. 1 While other surgical techniques such as injection laryngoplasty, arytenoid adduction (AA), and laryngeal innervation are used to treat UVFP, MT has the unique advantage of intra‐operative manipulation to optimize vocal quality. 2 , 3
A variety of laryngeal implant materials are available for MT, including Gore‐TexⓇ, SilasticⓇ, and hydroxyapatite. A 2010 survey on laryngeal framework surgery by Young et al. 4 revealed a downward trend in the use of SilasticⓇ (76% previously, 24% at the time of survey), and an upward trend in the use of Gore‐TexⓇ (36% previously, 64% at the time of survey). However, all types of laryngeal implants carry the risk of extrusion, with an overall rate of 0.8%. 4 , 5
Here, we describe a case of delayed implant extrusion following a revision Gore‐TexⓇ MT. While implant extrusion following MT is a recognized complication, this case uniquely occurred in both a delayed fashion and following revision Gore‐TexⓇ MT (5 years following the patient's original Gore‐TexⓇ MT, and 4 years following the patient's revision Gore‐TexⓇ MT). This is the first case in the literature of MT implant extrusion following a revision MT.
CASE
The patient is a 59‐year‐old female with history of non‐small cell lung cancer, status post left pneumonectomy in 2013, complicated by left vocal cord paralysis, for which she underwent left Gore‐TexⓇ MT in 2014 and revision Gore‐TexⓇ MT in 2015. She presented to the outpatient clinic with 1 week of sudden onset throat pain and hoarseness. Nasopharyngolaryngoscopy (NPL) revealed Gore‐TexⓇ implant extrusion laryngeally at the level of the false vocal cord, partially obstructing the airway. Imaging was deferred and the patient proceeded emergently to the operating room for direct laryngoscopy and endoscopic implant removal. In the operating room, the extruding Gore‐TexⓇ implant was removed (Figure 1, Figure 2), revealing the second Gore‐TexⓇ implant, which was also extruding and therefore also removed (Figure 3, Figure 4). Following removal of the Gore‐TexⓇ implants, granulation tissue was seen in the left ventricle, which was excised and injected with Decadron (Figure 5, Figure 6). The patient tolerated the procedure well without complication and was discharged home the same day.
Figure 1.
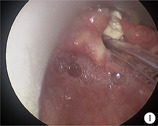
Laryngeal Gore‐TexⓇ implant extrusion
Figure 2.

Endoscopic removal of laryngeal Gore‐TexⓇ implant extrusion
Figure 3.

2nd laryngeal Gore‐TexⓇ implant extrusion
Figure 4.

Endoscopic removal of 2nd laryngeal Gore‐TexⓇ implant extrusion
Figure 5.

Granulation tissue in the left ventricle
Figure 6.

Endoscopic excision of granulation tissue in the left ventricle
At follow‐up the patient was breathing comfortably without any respiratory complaints. Three months after her Gore‐TexⓇ implant removal, she underwent left vocal cord injection laryngoplasty with calcium hydroxylapatite (CaHA), with subsequent vocal improvement and closure of glottic gap on NPL. Her most recent follow‐up has been delayed due to the coronavirus 2019 (COVID‐19) pandemic.
DISCUSSION
Laryngeal framework surgery, including MT and AA, are common treatments for UVFP with glottic incompetence. In the 2010 survey on laryngeal framework surgery by Young et al., 4 the overall complication rate of MT was 15%, airway compromise requiring intervention was observed in 2.2%, suboptimal voice outcome was observed in 4% (3% unchanged, 1% worse voice), and the overall revision rate was 6%. The most common revision surgery was replacement with another implant. 4
Implant extrusion is a recognized postoperative complication (0.8%) and can occur medially into the airway (0.5%) or laterally into the paraglottic space (0.3%). 4 Since the introduction of Gore‐TexⓇ in the 1990s, documentation of Gore‐TexⓇ implant extrusion has been limited to case reports and case series. A total of 13 cases of Gore‐TexⓇ implant extrusion have been described in the literature so far, plus our own case (Table 1). 6 , 7 , 8 , 9 , 10 , 11 , 12 , 13 , 14 , 15 , 16 , 17 Implant extrusion occurred anywhere between 2 months and 10 years postoperatively, and more frequently occurred medially into the airway, with patients presenting with cough, dysphonia, and/or globus sensation. 6 , 7 , 8 , 9 , 10 , 11 , 12
Table 1.
Case summary of Gore‐TexⓇ implant extrusion
| Pt No. | Author | Year | Sex | Surgery | Inner perichondrium | Onset | Treatment |
|---|---|---|---|---|---|---|---|
| 1 | Zeitels | 2003 | NR | MT | Preserved | NR | Removed |
| 2 | Laccourreye | 2003 | F | MT | Removed | 49 months | Removed |
| 3 | Cohen | 2004 | NR | MT | Incised | NR | Removed |
| 4 | Cohen | 2004 | NR | MT | Incised | NR | Removed |
| 5 | Halum | 2005 | F | MT | NA | NR | Removed |
| 6 | Halum | 2005 | NR | MT | NA | NR | Removed |
| 7 | Feinberg | 2010 | F | MT | NA | 6 years | Removed |
| 8 | Sims | 2014 | F | MT | NA | 5 months | Removed |
| 9 | Krane | 2016 | F | MT | Preserved | 5 years | Removed |
| 10 | Morris | 2016 | F | MT | NA | 10 years | Removed |
| 11 | Hardman | 2016 | NR | MT | NA | NR | Removed |
| 12 | Watanabe | 2017 | F | MT/AA | Preserved | 2 months | Removed |
| 13 | Kirke | 2018 | F | MT | Incised | 6 years | Partial removal |
| 14 | Frost* | 2020 | F | Revision MT | NA | 4 years | Removed |
NR: not reported; MT: medialization thyroplasty; AA: arytenoid adduction;
: presented case.
Review of the literature highlighted several factors that may cause a Gore‐TexⓇ implant to extrude. Surgical factors include improper implant placement (removal/violation of the inner perichondrium, pressure of the implant during insertion) and suboptimal implant stabilization (inability to lock the implant to the thyroid cartilage lamina window). 6 , 13 One case reported an unusually large amount of Gore‐TexⓇ needed to achieve medialization, which is another potential risk factor for implant extrusion. 11 Postoperative risk factors include infection and risks associated with subsequent surgeries (size of endotracheal tube (ETT), traumatic intubation, thoracic surgery with double‐lumen ETT, and length of surgery), which may weaken the tissue around the implant. 6 Finally, amongst patient factors, female gender has been noted to be a risk factor due to females having a relatively smaller larynx. 6 , 13
The case presented here has several unique aspects. This is the only published case of Gore‐TexⓇ implant extrusion following revision MT. 14 months after the patient's initial Gore‐TexⓇ MT, her voice continued to be weak and breathy and she was found to have increased left vocal cord atrophy with a persistent glottic gap, for which she underwent revision MT with additional Gore‐TexⓇ implant. The additional implant material may have exerted increased pressure on the laryngeal tissue medial to the implant. In addition, the inevitable vocal cord atrophy in the setting of UVFP, as well as the patient's chronic steroid use given her transplant history, may have weakened the laryngeal tissue medial to the implant. As previously mentioned, female gender has been noted to also be a risk factor. In summary, this was a female patient who underwent revision MT with placement of additional Gore‐TexⓇ, which likely caused increased pressure on the laryngeal surface, which itself weakened in the setting of expected progressive vocal cord atrophy and chronic steroid use. In this case, after suboptimal vocal quality with the initial Gore‐TexⓇ implant, it was believed that a 2nd Gore‐TexⓇ implant would improve her vocal quality, however perhaps the initial Gore‐TexⓇ implant should have been removed completely and replaced with a different implant material or an autogenous implant.
Consistent with the published literature, at our institution MT implant extrusion is managed in the operating room endoscopically or via an external surgical approach. The endoscopic approach is preferred for medial implant extrusion into the airway. The external surgical approach is indicated for lateral implant extrusion. One advantage of the external approach is the ability to perform immediate reimplantation. However previous studies have suggested that reimplantation is often unnecessary following implant extrusion, as many patients retain adequate glottic closure secondary to scar tissue build up in the paraglottic space. 7 , 11 , 13
More recently, ready‐made MT implant systems such as the MontgomeryⓇ Thyroplasty Implant System (Boston Medical Products, MA, USA), which is made of customizable SilasticⓇ, and VoCoM® (GYRUS ACMI, TN, USA), which is made of hydroxyapatite, have been developed to decrease the time involved in implant customization and to reduce complications. 13 In 2018 Chao et al. 17 published on a novel approach to MT with autogenous tissue using tensor fascia lata to improve outcomes and decrease complications such as extrusion or wound infection, particularly in patients that have received prior radiotherapy to the head and neck. Whether these new implant systems improve vocal outcomes and decrease complications long term, such as extrusion, remains to be determined.
CONCLUSIONS
We describe a unique case of Gore‐TexⓇ implant extrusion following revision MT, in which additional Gore‐TexⓇ was added in the revision surgery. The combination of the patient's second Gore‐TexⓇ implant causing increased pressure on the laryngeal surface, which itself weakened in the setting of expected progressive vocal cord atrophy and chronic steroid use, may have contributed to medial implant extrusion. Implant extrusion is a recognized postoperative complication that can be managed endoscopically or via an external open approach based on medial or lateral extrusion. During MT careful attention is given to implant placement and stabilization.
CONFLICTS OF INTEREST
None
ACKNOWLEDGEMENTS
Ariel Frost, contributed to the conception and design of the work, drafting and revising the manuscript, and final approval of the manuscript. Natasha Mirza contributed to the conception and design of the work, revising the manuscript, and final approval of the manuscript.
Frost A, Mirza N. Gore‐Tex implant extrusion following revision medialization thyroplasty: case report and review of the literature. World J Otorhinolaryngol Head Neck Surg. 2022;8:213‐216. 10.1016/j.wjorl.2020.08.001
REFERENCES
- 1. Siu J, Tam S, Fung K. A comparison of outcomes in interventions for unilateral vocal fold paralysis: a systematic review. Laryngoscope. 2016;126:1616‐1624. [DOI] [PubMed] [Google Scholar]
- 2. Harries ML. Unilateral vocal fold paralysis: a review of the current methods of surgical rehabilitation. J Laryngol Otol. 1996;110:111‐116. [DOI] [PubMed] [Google Scholar]
- 3. Benninger MS, Crumley RL, Ford CN, et al. Evaluation and treatment of the unilateral paralyzed vocal fold. Otolaryngol Head Neck Surg. 1994;111:497‐508. [DOI] [PubMed] [Google Scholar]
- 4. Young VN, Zullo TG, Rosen CA. Analysis of laryngeal framework surgery: 10‐year follow‐up to a national survey. Laryngoscope. 2010;120:1602‐1608. [DOI] [PubMed] [Google Scholar]
- 5. Rosen CA. Complications of phonosurgery: results of a national survey. Laryngoscope. 1998;108:1697‐1703. [DOI] [PubMed] [Google Scholar]
- 6. Laccourreye O, Hans S. Endolaryngeal extrusion of expanded polytetrafluoroethylene implant after medialization thyroplasty. Ann Otol Rhinol Laryngol. 2003;112:962‐964. [DOI] [PubMed] [Google Scholar]
- 7. Halum SL, Postma GN, Koufman JA. Endoscopic management of extruding medialization laryngoplasty implants. Laryngoscope. 2005;115:1051‐1054. [DOI] [PubMed] [Google Scholar]
- 8. Sims JR, Lalich IJ, Ekbom DC. Displacement of residual Gore‐Tex thyroplasty implant presenting as a true vocal fold mass. Otolaryngol Head Neck Surg. 2014;150:1090‐1091. [DOI] [PubMed] [Google Scholar]
- 9. Hardman J, Buchanan MA, Riffat F. Case of migrated Gore‐Tex implant following external thyroplasty. BMJ Case Rep. 2016;2016:bcr2016215277. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Morris J, Thomas DM. Delayed airway extrusion of type 1 thyroplasty Gore‐Tex implant. BMJ Case Rep. 2016;2016:bcr2016215704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Krane NA, Hu A, Sataloff RT. Gore‐Tex extrusion following type I thyroplasty. Ear Nose Throat J. 2016;95(4‐5):138‐140. [DOI] [PubMed] [Google Scholar]
- 12. Kirke DN, Blitzer A. Interesting case of late Gore‐Tex extrusion following medialization laryngoplasty. Laryngoscope. 2019;129:1420‐1422. [DOI] [PubMed] [Google Scholar]
- 13. Watanabe K, Hirano A, Honkura Y, Kashima K, Shirakura M, Katori Y. Complications of using Gore‐Tex in medialization laryngoplasty: case series and literature review. Eur Arch Otorhinolaryngol. 2019;276:255‐261. [DOI] [PubMed] [Google Scholar]
- 14. Zeitels SM, Mauri M, Dailey SH. Medialization laryngoplasty with Gore‐Tex for voice restoration secondary to glottal incompetence: indications and observations. Ann Otol Rhinol Laryngol. 2003;112:180‐184. [DOI] [PubMed] [Google Scholar]
- 15. Cohen JT, Bates DD, Postma GN. Revision Gore‐Tex medialization laryngoplasty. Otolaryngol Head Neck Surg. 2004;131:236‐240. [DOI] [PubMed] [Google Scholar]
- 16. Feinberg S, Lopez‐Guerra G, Zeitels SM. Hypopharyngeal extrusion of 2.5 feet (76 cm) of polytetrafluoroethylene (Gore‐Tex): initial laser‐assisted office‐based removal and micropharyngeal completion. Ann Otol Rhinol Laryngol. 2010;119:573‐577. [DOI] [PubMed] [Google Scholar]
- 17. Chao TN, Mahmoud A, Rajasekaran K, Mirza N. Medialisation thyroplasty with tensor fascia lata: a novel approach for reducing post‐thyroplasty complications. J Laryngol Otol. 2018;132:364‐367. [DOI] [PubMed] [Google Scholar]