

Abstract
Cholesterol granuloma (CG) is a rare condition histological consisting of a foreign body, giant cell reaction to cholesterol crystals and haemosiderin derived from the ruptured of the erythrocytes. A 25-year-old man came to our Department presenting signs and symptoms of tympano-mastoid cholesterol granuloma. He showed all the specific sign and symptoms of the disease. However, considering the lack of literature regarding TMCG, this study was performed with the aim of presenting the main characteristics of tympano-mastoid CG, describing the case report and reviewing the literature.
Keywords: Cholesterol granuloma, middle ear, mastoid, cholesterol crystal, review
Introduction
Cholesterol granuloma (CG) is a histological definition used to describe foreign body, giant cell reaction to cholesterol crystals and haemosiderin derived from the rupture of the erythrocytes.
This condition involves diverse temporal bone sites: middle ear, mastoid and petrous apex.
In the literature, it is considered the most common benign pathological lesion of the petrous apex, involving about 40% of the lesions in that area.1 On the contrary, tympano-mastoid CGs are rare.
To our knowledge, over the last decades, principally case reports of tympano-mastoid CG have been reported, but no review of the literature.
The aim of this study was to present the main characteristics of tympano-mastoid CG describing a case report and reviewing the literature.
Materials and Methods
Case report
A 25-year-old man came to our Department presenting a progressive impairment and fullness of the left ear. Otoscopy showed a bluish, non-pulsing, retro-tympanic mass that caused a bulging (Figure 1).
Figure 1.

Otoscopy. Blue retrotympanic mass that involves external auditory channel.
Preoperative Magnetic Resonance Imaging (MRI) revealed high signal intensity in T1- and T2-weighted images with a high suspicion of CG.2
Tympano-mastoid canal wall up surgery was performed under general anaesthesia in order to remove the presumed CG (Figure 2). Histological examination of the bioptic sample revealed the typical features of cholesterol granuloma (Figure 3).
Figure 2.
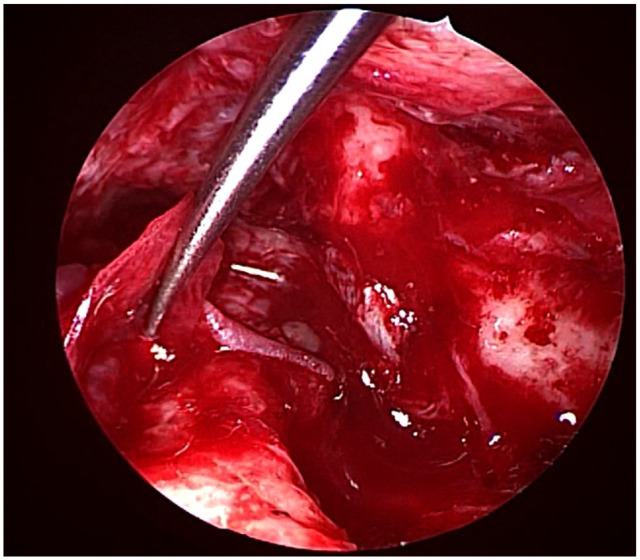
Intraoperative view after the removing of tympano mastoid cholesterol granuloma (TMCG).
Figure 3.
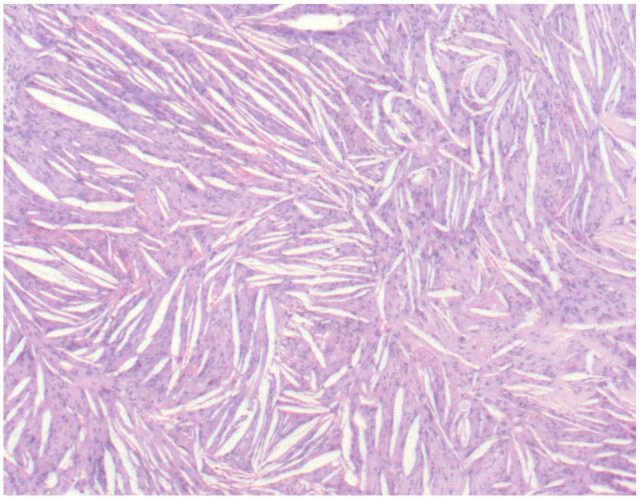
Low power magnification of the bioptic sample shows a typical cholesterol granuloma. Bar: 200 microns.
High power magnification of the latter, highlighted the clefts of cholesterol crystals resulting from cholesterol dissolution during tissue processing, associated with foreign body multinucleated giant cells and haemorrhage1 (Figure 4).
Figure 4.
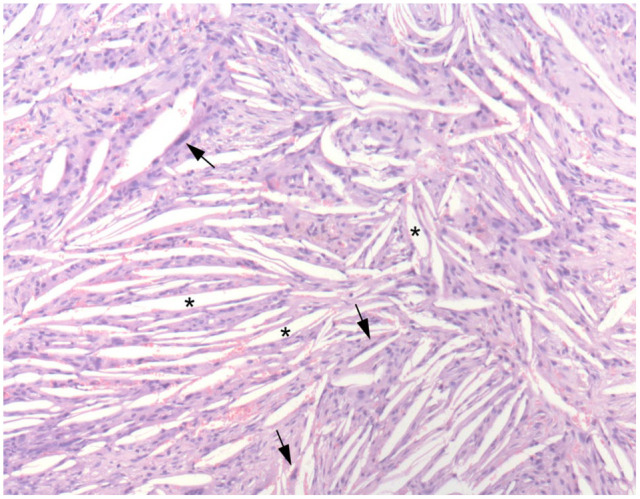
High power magnification of the bioptic sample highlights the clefts of cholesterol crystals (asterisks) resulting from the dissolution of cholesterol during tissue processing associated with foreign body multinucleated giant cells (arrows) and haemorrhage. Bar: 100 microns.
Immunohistochemistry showed that endothelial cells presented an increased expression of angiogenetic growth factor receptors. High vascular density and increased angiogenesis were found together with high levels of VEGF and CD34 expression.
Review
Research was conducted using PubMed and reference list, identifying articles for inclusion. Two reviewers independently screened literature search results and extracted data from included studies. The keywords used for the research were: tympanic cholesterol granuloma, mastoid cholesterol granuloma, middle ear cholesterol granuloma. Descriptive analysis was conducted.
Results
In the literature few articles have described tympano-mastoid CG. Sixteen were considered the most relevant and were analysed. Fourteen were included in this review. The exclusion criterion was the presence of different disease (eg, cholesteatoma) contemporarily to CG. The total number of cases of isolated TMCG reported in literature regarded 53 patients.
Discussion
Epidemiology and pathophysiology of TMCG
Cholesterol granuloma was described, for the first time, in Manassé’s study of 1894. It is not a specific disease of the temporal bone, but is reported in other locations too: central nervous system, frontal bone, orbital cavity, paranasal sinus, infratemporal fossa, thyroid gland, mediastinum, ovary and peritoneum.3,4
In the temporal bone it could be present in different sites: middle ear, mastoid and petrous apex. It is considered to be the most common benign pathological lesion of the petrous apex, accounting for about 40% of the lesion of that area,1 whereas tympano-mastoid CG has an unknown incidence.
Petrous Apex (PA) CG has been related with 2 hypotheses of formation: the obstruction-vacuum-theory and the exposed marrow theory.5-7
Tympano-mastoid (TM) CG could be either a primary disease of the middle ear and mastoid or a secondary disease due to surgery of these regions.8,9
In 1964, MacNaughton mentioned the herpes virus as a possible pathogen of TMCG. He proposed that haematoma of the tympanic membrane is smoothly absorbed, except for in some pathological conditions in which absorption can be greatly impeded (closed spaces poorly ventilated and poorly vascularised).10
In the same years, many studies revealed that in chronic secretory otitis media the lamina propria is thickened and consists of a broad fibrous layer. This anatomical change could be responsible for the poor absorption of mucus and eventual blood, in the middle ear, causing haematoma. The latter, not disintegrated, produces cholesterol granuloma.11
However, it has been observed that CG is usually associated with cholesteatoma. Friedmann believed that cholesterol granuloma was not the predecessor of cholesteatoma. He proposed that the cholesteatoma tissue, liquefying, deposited the cholesterol which stimulated tissue to form cholesterol granuloma.12 Recent literature has described cholesteatoma and cholesterol granuloma as different processes of the same disease. According to evidence that cholesteatoma possesses a component of cholesterol, it was suggested that CG could be formed by the ruptured epithelium covering of the cholesteatoma. The content flows outward into the interstitia, leading to the foreign body reaction of macrophages and inflammatory cell infiltration.
According to this theory, Luo et al, in 2002, considered the pathophysiological etiology of both cholesteatoma and cholesterol granuloma, to be related to occlusion of ventilation and disturbance of drainage.13
Clinical examination and differential diagnosis
Cholesterol granuloma is slow growing and is usually asymptomatic. It is typically observed as primary disease of the middle ear and mastoid in the form of idiopathic haemotympanum. However, it may be secondary to surgery of the tympanomastoid compartments in the form of so-called ‘blue domed cyst’, sometimes observed in a canal wall down procedure.2 CG is pain-free, but could lead to transmission deafness, vertigo and facial palsy.1
Otoscopy showed a bluish tympanic membrane, non-pulsing, that sometimes caused a bulging. Differential diagnosis is difficult. Farrior et al described all the possible differential diagnoses with TMCG. The most important to consider are: high jugular bulb; aberrant carotid artery and vascular abnormality; tympanic and tympano-jugular glomus; the Shwartze sign of otosclerosis; same types of TORPS and implants in the mastoid; osteoma and bony exostosis; pigmentary changes in external auditory channel and middle ear, chronic serous otitis media; chronic serous mastoiditis; brain hernia; haemotympanum; barotrauma; haemorrhagic otitis media.14 Cochlear invasion is rare and, in the literature, only 2 cases are reported.12,15,16
Imaging
Today, imaging used to diagnose cholesterol granuloma consists of CT and MRI.2,17
Computed Tomography (CT) associated with contrast material is a poor specific test for TMCG, unable to make a differential diagnosis. It is more useful for diagnosis petrous apex cholesterol granuloma (PACG), evaluating possible bone erosion. However, CT could reduce doubt because it rarely causes bony erosion, on the contrary to other lesions (eg, glomus tumour) that cause bone erosion in the middle ear and mastoid.18,19
For diagnosis and localisation of cholesterol granuloma, MRI is the most accurate exam. The MRI findings of cholesterol granuloma are, in fact, unique. CG typically appears with a high signal intensity on T1- and T2-weighted images. Moreover, it can exhibit high signal intensity on fluid attenuated inversion recovery (‘FLAIR’) MRI and low signal intensity on diffusion-weighted MRI. This is useful for preoperative planning and could be helpful for making differential diagnosis with non-contrast-enhanced masses and cholesteatoma.
Histological examination
Histological evidence of cholesterol granuloma is characterised by foreign body, giant cell reaction to cholesterol crystals and haemosiderin derived from the ruptured of the erythrocytes.7,12 Iannella et al, in 2017, investigated the immunohistochemical expression of VEGF and CD34 in a group of patients surgically treated for CGs. They demonstrated that, if conducted, immunohistochemistry shows that endothelial cells present an increased expression of angiogenetic growth factor receptors (VEGF and CD34).20
Surgical management and approach
In the literature only a few studies have described the surgery of isolated TMCGs.
In small TMCGs involving only middle ear, without symptomatology, some authors have reported that tube insertion is not needed.21 On the contrary, others authors, have recommended conservative treatment.14,22
For small CGs confined to the middle ear a canal wall up or down tympanoplasty associated with ventilation tube insertion are usually performed.
The aim of surgical therapy is to achieve reaeration of the mastoid cavity and of the Eustachian tube.23 To date, no authors have described TMCG removed by exclusive endoscopic approach.
Prognosis and hearing results
Hearing prognosis for patients with TMCG is poor. Inagi et al, believed that poor post-hearing results in TMCG surgery was related to different factors: age 35 years or older; symptoms for more than 15 years; pre-operative otorrhoea within 1 month of operation; tympanic membrane perforation; granulations around the ossicular chain. Moreover, bone conduction worsened from 25.6 to 42.3 dB during the early postoperative period in cholesterol granuloma patients.24,25
In 2003, Matsuda et al, presented relatively good hearing results 2 weeks after surgery (an overall hearing success rate of 75%), but some patients worsened postoperatively. They affirmed that patients’ hearing prognosis is determined during the first 2 post-operative weeks and that no subsequent hearing improvement can be expected.26
Conclusion
Tympano-mastoid CG is rare disease of the middle ear and mastoid. Few articles have been written about it and no review has been published during the last decades. It is important to be aware of the characteristics of TMCGs because is essential to make a correct differential diagnosis to permit correct management of this disease.
Footnotes
Funding:The author(s) received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting Interests:The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Authors’ Contributions: AP and GM: made a substantial contribution to the concept and design of the work; approved the version to be published. GI, MR and AC: acquisition, analysis and interpretation of data.
Informed Consent: Appropriate consent to publish case details was obtained from the patient.
ORCID iDs: Alessandro Corsi  https://orcid.org/0000-0001-6896-4509
https://orcid.org/0000-0001-6896-4509
Giuseppe Magliulo
https://orcid.org/0000-0003-3052-1969
References
- 1. Mitchell RG, Zanation AM, Ebert CS, Senior BA. Cholesterol granuloma of the petrous apex. Otolaryngol Clin North Am. 2011;44:1043-1058. doi: 10.1016/j.otc.2011.06.005. [DOI] [PubMed] [Google Scholar]
- 2. Iannella G, Stasolla A, Pasquariello B, Re M, Magliulo G. Tympanomastoid cholesterol granuloma: radiological and intraoperative findings of blood source connection. Eur Arch Otorhinolaryngol. 2016;273:2395-2401. doi: 10.1007/s00405-015-3820-5. [DOI] [PubMed] [Google Scholar]
- 3. Rinaldo A, Ferlito A, Cureoglu S, Devaney KO, Schachern PA, Paparella MM. Cholesterol granuloma of the temporal bone: a pathologic designation or a clinical diagnosis? Acta Otolaryngol. 2005;125:86-90. doi: 10.1080/00016480310017036. [DOI] [PubMed] [Google Scholar]
- 4. Campos A, Armengot M, Zapater E, Hostalet F, Basterra J. Cholesterol granuloma of the middle ear: report of 5 cases. Acta Otolaryngol. 1996; 50:125-129. [PubMed] [Google Scholar]
- 5. Graham MD, Kemink JL, Latack JT, Kartush JM. The giant cholesterol cyst of the petrous apex: a distinct clinical entity. Laryngoscope. 1985;95:1401-1406. doi: 10.1288/00005537-198511000-00021. [DOI] [PubMed] [Google Scholar]
- 6. Jackler RK, Cho M. A new theory to explain the genesis of petrous apex cholesterol granuloma. Otol Neurotol. 2003;24:96-106. doi: 10.1097/00129492-200301000-00020. [DOI] [PubMed] [Google Scholar]
- 7. Altes K. Cholesterol- Granuloma in the middle ear. Pract Otorhinolaryngol (Basel). 1965;27:324. [Google Scholar]
- 8. Albakheet N, Al-Shawi Y, Bafaqeeh M, Fatani H, Orz Y, Shami I. Familial hypercholesterolemia with bilateral cholesterol granuloma: a case series. Int J Surg Case Rep. 2019;62:135-139. doi: 10.1016/j.ijscr.2019.07.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Olcott C, Strasnick B. A blue middle ear mass: cholesterol granuloma mimicking a glomus tumor and endolymphatic sac tumor. Am J Otolaryngol. 2017;38:100-102. doi: 10.1016/j.amjoto.2016.09.013. [DOI] [PubMed] [Google Scholar]
- 10. Macnaughton IPJ. The chronic ear. The aetiology and treatment of cholesterol granuloma in the middle ear. Proc R Soc Med. 1964;57:767-769. [PMC free article] [PubMed] [Google Scholar]
- 11. Altes AJ. Cholesterol granuloma in the tympanic cavity. J Laryngol Otol. 1966;80:691-698. doi: 10.1017/s0022215100065865. [DOI] [PubMed] [Google Scholar]
- 12. Friedmann I. The patology of secretory otitis media. Proc R Soc Med. 1963;56:695-699. [PMC free article] [PubMed] [Google Scholar]
- 13. Luo L, Gong S, Bai G, Wang J. A retrospective study on cholesteatoma otitis media coexisting with cholesterol granuloma. J Huazhong Univ Sci Technolog Med Sci. 2002;22:168-170. doi: 10.1007/BF02857685. [DOI] [PubMed] [Google Scholar]
- 14. Farrior B, Kampsen E, Farrior JB. The positive pressure of cholesterol granuloma idiopathic blue eardrum. Differential diagnosis. Laryngoscope. 1981;91:1286-1297. doi: 10.1288/00005537-198108000-00011. [DOI] [PubMed] [Google Scholar]
- 15. Murugasu E, Yong TT, Yoon CP. Invasive middle ear cholesterol granuloma involving the basal turn of the cochlea with profound sensorineural hearing loss. Otol Neurotol. 2004;25:231-235. doi: 10.1097/00129492-200405000-00005. [DOI] [PubMed] [Google Scholar]
- 16. Martin C, Faye M-B, Bertholon P, Veyret C, Dumollard J-M, Prades J-M. Cholesterol granuloma of the middle ear invading the cochlea. Eur Ann Otorhinolaryngol Head Neck Dis. 2012;129:104-107. doi: 10.1016/j.anorl.2011.10.009. [DOI] [PubMed] [Google Scholar]
- 17. Sakurai T. CT scan findings in blue ear drum. Acta Otolaryngol Suppl. 1987;435:117-121. doi: 10.3109/00016488709107360. [DOI] [PubMed] [Google Scholar]
- 18. Raghavan D, Lee TC, Curtin HD. Cholesterol granuloma of the petrous apex: a 5-year review of radiology reports with follow-up of progression and treatment. J Neurol Surg B Skull Base. 2015;76:266-2271. doi: 10.1055/s-0034-1396600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Mosnier I, Cyna-Gorse F, Grayeli AB, et al. Management of cholesterol granulomas of the petrous apex based on clinical and radiologic evaluation. Otol Neurotol. 2002;23:522-528. doi: 10.1097/00129492-200207000-00022. [DOI] [PubMed] [Google Scholar]
- 20. Iannella G, Di Gioia C, Carletti R, Magliulo G. Tympanomastoid cholesterol granulomas: immunohistochemical evaluation of angiogenesis [published online ahead print of February 3, 2017]. Laryngoscope. doi: 10.1002/lary.26458. [DOI] [PubMed] [Google Scholar]
- 21. Ikeda M, Watanabe I. Post-operative evaluation of cholesterol granuloma. Ear Res Jpn. 1997;90:8. [Google Scholar]
- 22. Plester D. Cholesterol granuloma. Otolaryngol Clin North Am. 1982;15:665-667. [PubMed] [Google Scholar]
- 23. Maeta M, Saito R, Nakagawa F, Miyahara T. Surgical intervention in middle-ear cholesterol granuloma. J Laryngol Otol. 2003;117:344-348. doi: 10.1258/002221503321626366. [DOI] [PubMed] [Google Scholar]
- 24. Inagi K, Shitara T, Okamoto M, Sano H. Clinical study of cholesterol granuloma of middle-ear. Ear Res Jpn. 1989;16:6-13. [Google Scholar]
- 25. Yoshida S, Tomita H. The surgical indications and hearing prognosis of middle ear cholesterol granuloma with blue ear drums. Otol Jpn. 1994;4:172–176. [Google Scholar]
- 26. Matsuda Y, Kurita T, Ueda Y, Ito S, Nakashima T. Analysis of surgical treatment for middle-ear cholesterol granuloma. J Laryngol Otol Suppl. 2009;123:90. doi: 10.1017/S0022215109005167. [DOI] [PubMed] [Google Scholar]