

Once a vaccine for coronavirus disease 2019 becomes available, it will be important to maximize vaccine uptake and coverage. This national survey explores factors associated with vaccine hesitancy. The results suggest that multipronged efforts will be needed to increase acceptance of a coronavirus disease 2019 vaccine.
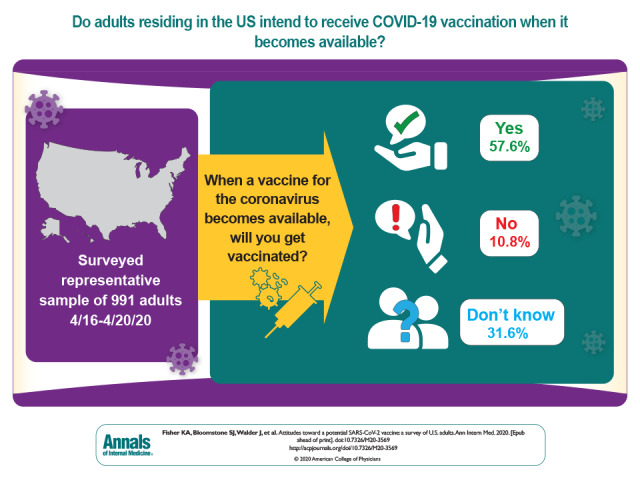
Visual Abstract. Attitudes Toward a Potential SARS CoV-2 Vaccine Among U.S. Adults.
Once a vaccine for coronavirus disease 2019 becomes available, it will be important to maximize vaccine uptake and coverage. This national survey explores factors associated with vaccine hesitancy. The results suggest that multipronged efforts will be needed to increase acceptance of a coronavirus disease 2019 vaccine.
Abstract
Background:
Coronavirus disease 2019 (COVID-19) has rapidly instigated a global pandemic. Vaccine development is proceeding at an unprecedented pace. Once available, it will be important to maximize vaccine uptake and coverage.
Objective:
To assess intent to be vaccinated against COVID-19 among a representative sample of adults in the United States and identify predictors of and reasons for vaccine hesitancy.
Design:
Cross-sectional survey, fielded from 16 through 20 April 2020.
Setting:
Representative sample of adults residing in the United States.
Participants:
Approximately 1000 adults drawn from the AmeriSpeak probability-based research panel, covering approximately 97% of the U.S. household population.
Measurements:
Intent to be vaccinated against COVID-19 was measured with the question, “When a vaccine for the coronavirus becomes available, will you get vaccinated?” Response options were “yes,” “no,” and “not sure.” Participants who responded “no” or “not sure” were asked to provide a reason.
Results:
A total of 991 AmeriSpeak panel members responded. Overall, 57.6% of participants (n = 571) intended to be vaccinated, 31.6% (n = 313) were not sure, and 10.8% (n = 107) did not intend to be vaccinated. Factors independently associated with vaccine hesitancy (a response of “no” or “not sure”) included younger age, Black race, lower educational attainment, and not having received the influenza vaccine in the prior year. Reasons for vaccine hesitancy included vaccine-specific concerns, a need for more information, antivaccine attitudes or beliefs, and a lack of trust.
Limitations:
Participants' intent to be vaccinated was explored before a vaccine was available and when the pandemic was affecting a narrower swath of the United States. Questions about specific information or factors that might increase vaccination acceptance were not included. The survey response rate was 16.1%.
Conclusion:
This national survey, conducted during the coronavirus pandemic, revealed that approximately 3 in 10 adults were not sure they would accept vaccination and 1 in 10 did not intend to be vaccinated against COVID-19. Targeted and multipronged efforts will be needed to increase acceptance of a COVID-19 vaccine when one becomes available.
Primary Funding Source:
Agency for Healthcare Research and Quality.
Coronavirus disease 2019 (COVID-19) is caused by the β-coronavirus severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). This virus has rapidly become a major global threat, instigating a pandemic affecting more than 185 countries and 3 500 000 people and leading to nearly 250 000 deaths worldwide (1). The pandemic has overwhelmed hospital systems, undermined economic activity worldwide, and instilled fear into the general populace (2, 3). An international poll conducted in April 2020 found that 61% of those surveyed identified COVID-19 as the most concerning national issue, overtaking unemployment, health care, and poverty (4). In a separate survey conducted at the same time in the United States, more than 80% of participants were very or somewhat concerned about being infected with coronavirus (5). In response to the massive global effects of COVID-19, multiple laboratories worldwide are working to create an effective vaccine. The possibility that one will be available in 12 to 18 months is seen by many as the most promising means of controlling the COVID-19 pandemic.
Over the past century, vaccinations have become a routine and effective preventive measure in reducing the rate of and eradicating or nearly eradicating certain viral illnesses (6). Besides providing direct immunity and preventing disease among vaccinated individuals, vaccines have been shown to reduce infections even among individuals who are not vaccinated, through herd immunity, if a sufficient proportion of the population is immune (7). Many pharmaceutical companies and research labs are currently working with messenger RNA, DNA, subunit, virus-like particles, and viral vectors to discover an effective vaccine for the COVID-19 pandemic (8, 9). On an unprecedented timeline, multiple vaccines have been developed and are currently being tested in large-scale phase 3 trials (10), suggesting that a vaccine may be available in the foreseeable future. The great potential of a vaccine against COVID-19 is tempered by rising vaccine skepticism in the United States and worldwide, which may present challenges to widespread vaccine uptake when a vaccine becomes available (11–14). It is unknown whether the unprecedented and severe effects of COVID-19 in the United States will overcome vaccine skepticism and foster widespread acceptance of and demand for vaccination.
Although the timeline for having a safe, effective COVID-19 vaccine ready for distribution is uncertain, it is important to anticipate and mitigate barriers to its widespread use. We assessed intent to be vaccinated against COVID-19 among a nationally representative sample of adults in the United States. To inform and target future efforts to encourage vaccine uptake, we sought to identify predictors of intent to decline or delay acceptance of a vaccine (“vaccine hesitancy”) and reasons for doing so.
Methods
Participants and Survey Administration
We surveyed a nationally representative sample of adults residing in the United States via the National Opinion Research Center (NORC) AmeriSpeak Omnibus survey. The AmeriSpeak Panel is a probability-based research panel that provides coverage of approximately 97% of the U.S. household population. Panel members were contacted and enrolled via telephone, mail, and in-person field interviews by using a multistage process. Informed consent was obtained at the time of panel enrollment. Panel members provide demographic and other information upon enrollment. The AmeriSpeak Omnibus survey combines questions from multiple entities and is fielded twice monthly to a national sample of panel members to achieve approximately 1000 responses. Panel members receive an initial invitation via email, SMS, or phone, followed by 1 or 2 reminders to nonresponsive members. Households without Internet access are included and complete the survey via smartphone or telephone interview. Data for the present study were collected via the AmeriSpeak Omnibus survey fielded from 16 through 20 April 2020. In addition to the COVID-19 vaccine-related questions reported here, other COVID-19–related questions were included elsewhere on this survey; we do not have access to these questions or responses. The only COVID-19 vaccine–related questions on this survey are the ones we report here. Participants were informed that the survey would cover “a variety of topics.” They were not informed about the specific topic of the survey before they agreed to participate.
Measures
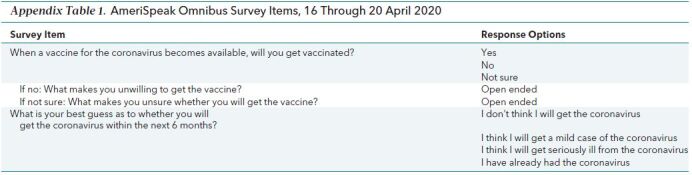
We assessed intent to be vaccinated for the novel coronavirus with the question, “When a vaccine for the coronavirus becomes available, will you get vaccinated?” followed by the response options “yes,” “no,” and “not sure.” Participants who responded “no” or “not sure” were asked one of the following open-ended questions, respectively: “What makes you unwilling to get the vaccine?” or “What makes you unsure whether you will get the vaccine?.” To assess perceived risks of infection, we asked, “What is your best guess as to whether you will get the coronavirus within the next 6 months?”; response options were “I don't think I will get the coronavirus,” “I think I will get a mild case of the coronavirus,” “I think I will get seriously ill from the coronavirus,” or “I have already had the coronavirus.” Survey items are shown in Appendix Table 1 (available at Annals.org). We conducted 2 rounds of pilot testing of the main question assessing intent to be vaccinated among a convenience sample of over 100 individuals and did not detect any problems.
Appendix Table 1. AmeriSpeak Omnibus Survey Items, 16 Through 20 April 2020.
Data on participant characteristics were provided by NORC and included age, sex, race/ethnicity, educational attainment, household income, household size, marital status, employment status, geographic location, urban or rural location (addresses within a metropolitan statistical area were categorized as urban), receipt of influenza vaccination in the prior year, and self-rated overall health status. NORC collects data on health-related variables (such as receipt of influenza vaccination and self-rated overall health status) upon enrollment or soon after for most panel members; if a panel member has not responded to a specific item, that item may be included on subsequent surveys. All data provided to the investigators were fully deidentified.
Statistical Analysis
Participant characteristics were summarized by using frequencies and percentages. We used cross-tabulations and χ2 tests to estimate unadjusted associations of participant characteristics and perceived personal risk for coronavirus with the 3-category outcome intent to get vaccinated. To better distinguish characteristics associated with responses of “not sure” versus “yes” and characteristics associated with responses of “no” versus “yes,” we also calculated separate χ2 tests and associated P values for these 2 sets of comparisons.
To estimate corresponding adjusted (multivariate) associations, we used multinomial logistic regression, an extension of binomial logistic regression that compares each of 2 or more nonordered outcome categories to the reference category. In particular, we modeled both natural log [Pr (Not sure)/Pr (Yes)] and natural log [Pr (No)/Pr (Yes)] as a function of participant characteristics. This approach allows different associations with covariates for the 2 comparisons while providing overall P values for covariates. Whereas coefficients from a binomial logistic regression model are typically exponentiated to obtain odds ratios, exponentiated coefficients from a multinomial logistic regression model are interpreted as relative risk ratios (RRRs). An illustrative calculation is provided in the footnote to Table 3.
Characteristics that were not statistically significant (P < 0.05) in the multivariate multinomial modeling were omitted in the final model; these characteristics were found to be correlated with predictors retained in the final model (for example, household income was related to education). We considered the possibility that inclusion of prior receipt of influenza vaccine in the model may obscure other predictors of COVID-19 vaccine hesitancy owing to overlap in the reasons for reluctance to get an influenza or COVID-19 vaccine. We therefore repeated the primary analysis after removing receipt of influenza vaccine from the model. Adjusted percentages were calculated for each predictor category by fixing all other predictors at their observed distributions. To assess model performance, we calculated C-statistics and Hosmer–Lemeshow statistics separately for binomial logistic regressions for “not sure” versus “yes” and “no” versus “yes.”
All analyses incorporated survey sampling weights based on gender, age, education, race/ethnicity, and region. Analyses were conducted by using SAS, version 9.4.
We used thematic analysis to inductively generate codes and identify themes in the responses to the open-ended query soliciting reasons for vaccine hesitancy (15). The coding team included investigators with backgrounds in health communication, health literacy, patient–provider communication, clinical medicine, and clinical social work; all coding team members had prior experience in qualitative analysis. A coding framework was created on the basis of initial review of all responses. Codes and associated definitions were revised and refined through iterative application and discussion. Two analysts (K.F., S.B.) then independently coded all responses. More than 1 code could be assigned to a response if applicable. Coding discrepancies were discussed until agreement was reached; the third member of the coding team was available to adjudicate but was not needed. Codes were assigned in Excel; final codes were merged into SPSS, version 25, to facilitate data manipulation and summarization.
Our study was determined to be exempt by the University of Massachusetts Medical School Institutional Review Board.
Role of the Funding Source
Dr. Fisher is supported by Agency for Healthcare Research and Quality grant K08HS024596. The funder had no role in the design, conduct, or analysis of this study.
Results
The AmeriSpeak Omnibus survey was released to 6247 panel members, and a total of 1003 (16.1%) responded. Most participants (91.2%) completed the survey via the Web; the remainder (8.8%) completed it via telephone interview. Twelve participants did not respond to the question on intent to be vaccinated; all results presented here are based on the 991 participants who responded to this question.
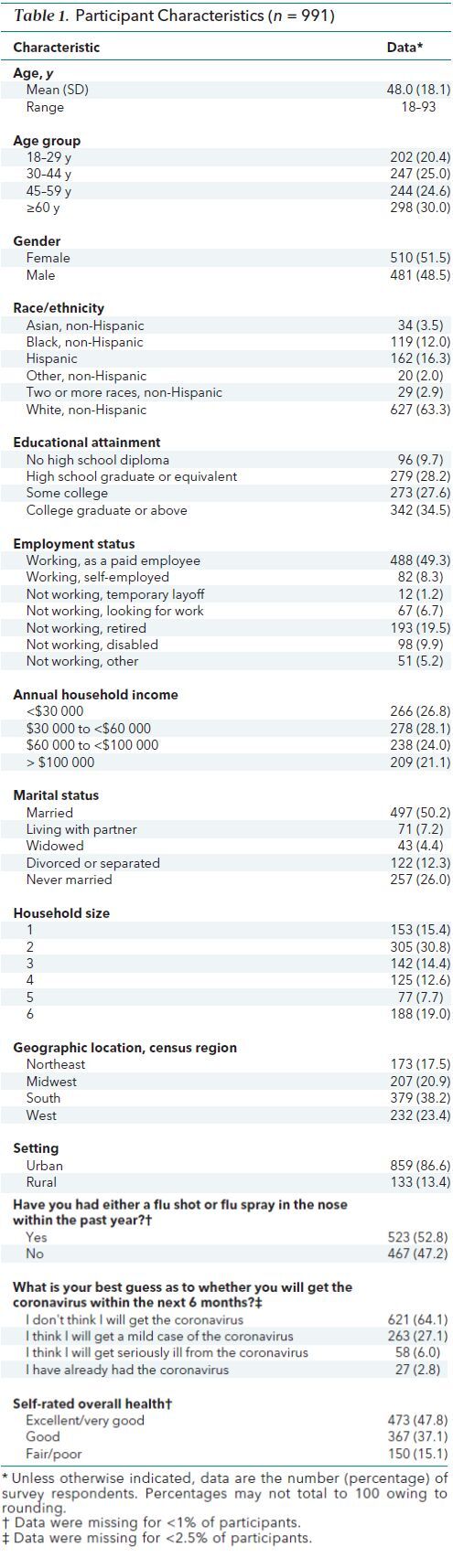
A majority of participants (63.3%) were White, approximately one third (30.0%) were 60 years of age or older, and 51.5% were female. Participants had varied levels of educational attainment, with more than one third (37.8%) having a high-school diploma or less. Most participants perceived their risk for coronavirus to be low, predicting that they will either not get the coronavirus (64.1%) or that they will get a mild case of the coronavirus (27.1%) in the next 6 months. Only 58 participants (6.0%) predicted they will get seriously ill from the coronavirus. Approximately one half (52.8%) of participants reported having received the influenza vaccine previously. Additional participant characteristics are shown in Table 1.
Table 1. Participant Characteristics (n = 991).
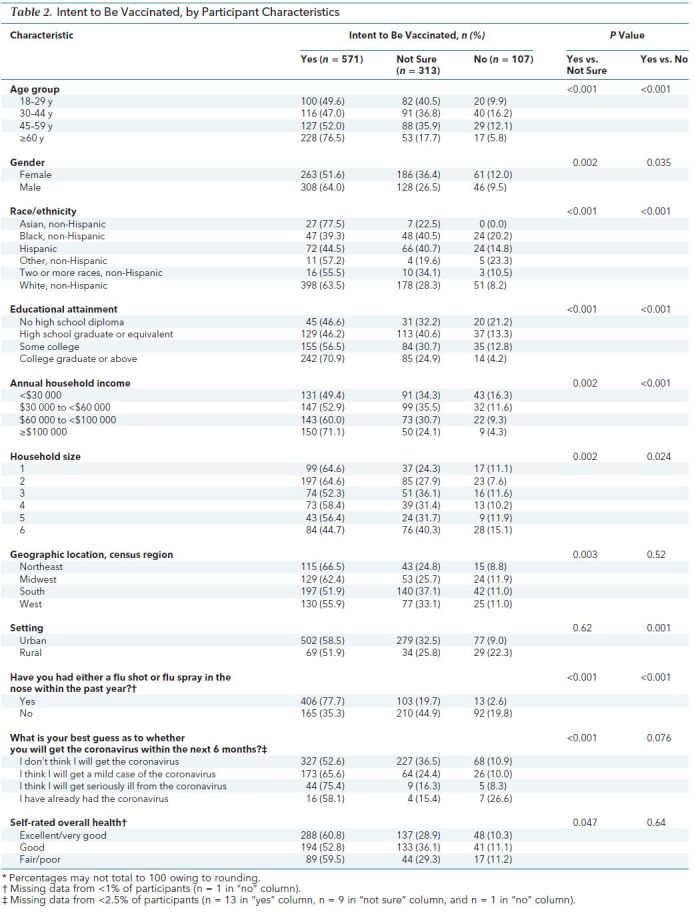
Overall, 57.6% of participants (n = 571) intended to be vaccinated, 31.6% (n = 313) were not sure whether they would be vaccinated, and 10.8% (n = 107) did not intend to be vaccinated. Participant characteristics associated with a higher chance of responding “no” or “not sure” versus “yes” were being younger (<60 years), female, or Black or Hispanic; having lower educational attainment, lower household income, or larger household size, and being less likely to report having received an influenza vaccine. In addition to these differences, participants who responded “not sure” were more likely to live in the South or West and to believe they were at less personal risk for coronavirus despite providing lower ratings of their overall health. Participants who responded “no” were more likely to live in a rural setting (Table 2).
Table 2. Intent to Be Vaccinated, by Participant Characteristics.
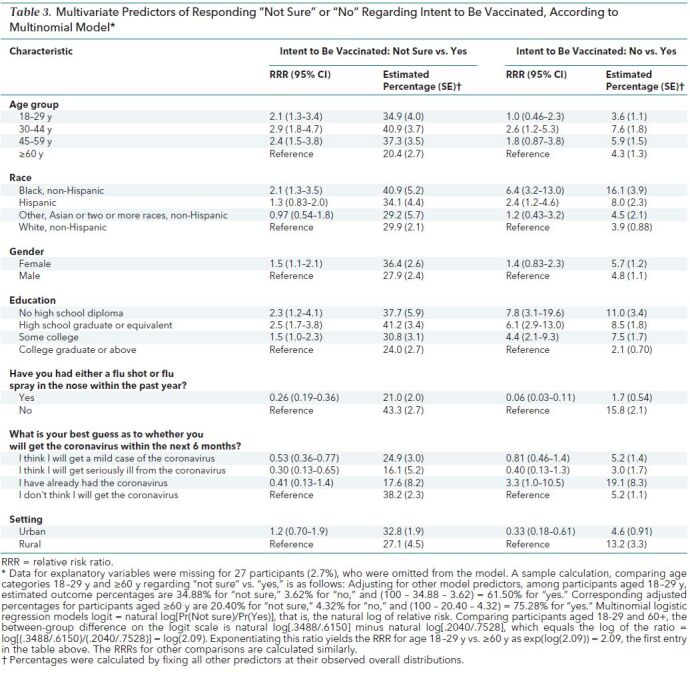
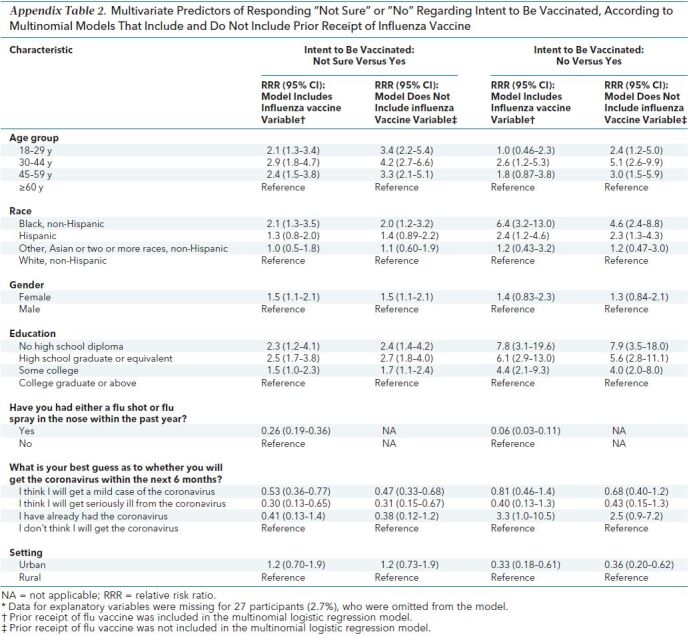
After adjustment for differences in participant characteristics (Table 3), factors that were independently associated with vaccine hesitancy (response of “no” or “not sure”) include younger age (<60 years), Black race, educational attainment of less than a college degree, and not receiving an influenza vaccine in the prior year. Participants who did not have a high school diploma had a nearly 8-fold higher relative likelihood of responding “no” versus “yes” compared with those who had a college degree or higher (RRR, 7.8 [95% CI, 3.1 to 19.6]). Black race was associated with a more than 6-fold higher chance (RRR, 6.4 [CI, 3.2 to 13.0]) of not intending to be vaccinated versus intending to be vaccinated compared with White race. Participants who had previously received an influenza vaccine had a 94% lower relative likelihood of responding “no” versus “yes” (RRR, 0.06 [CI, 0.03 to 0.11]) compared with those who had not received an influenza vaccine. Other characteristics, such as female sex, some age strata, Hispanic ethnicity, and perceived personal risk for coronavirus, were associated with vaccination intent but did not consistently achieve statistical significance for both response categories (“not sure” and “no”). Living in a rural area was strongly associated with responding “no” when asked about intent to be vaccinated, but not with responding “not sure.” Household income, household size, region, and self-reported health were not significantly associated with vaccination intent after adjustment for the characteristics in Table 3. Results including these as model predictors were similar (data not shown). Removal of prior receipt of influenza vaccine from the multinomial model resulted in an increase in the relative risk ratios comparing “no” versus “yes” for 2 age groups (18 to 29 years and 45 to 59 years), such that the CI no longer included 1 while other results remained similar (Appendix Table 2, available at Annals.org). Because one of the main goals of our study was to predict who may be hesitant to be vaccinated against COVID-19 and prior receipt of influenza vaccine offers a pragmatic way to identify these individuals, we report the findings from the model that included prior receipt of influenza vaccine. Hosmer–Lemeshow statistics for “not sure” versus “yes” and for “no” versus “yes” were not statistically significant (P = 0.37 and 0.50, respectively), and corresponding C-statistics were 0.74 and 0.89, indicating excellent model fit and performance.
Table 3. Multivariate Predictors of Responding “Not Sure” or “No” Regarding Intent to Be Vaccinated, According to Multinomial Model*.
Appendix Table 2. Multivariate Predictors of Responding “Not Sure” or “No” Regarding Intent to Be Vaccinated, According to Multinomial Models That Include and Do Not Include Prior Receipt of Influenza Vaccine.
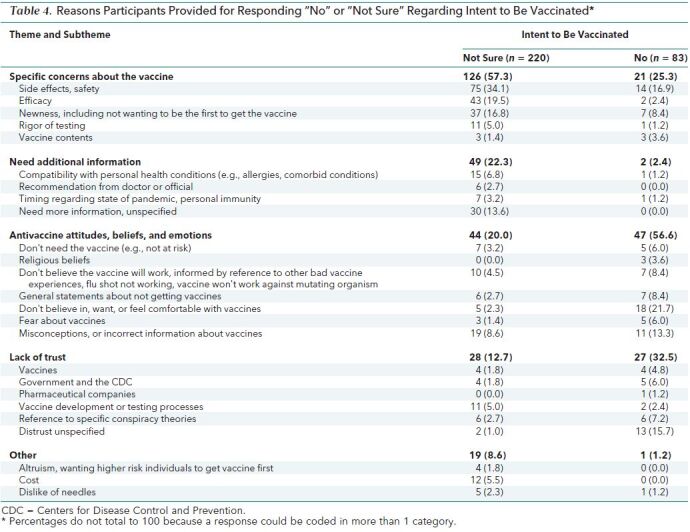
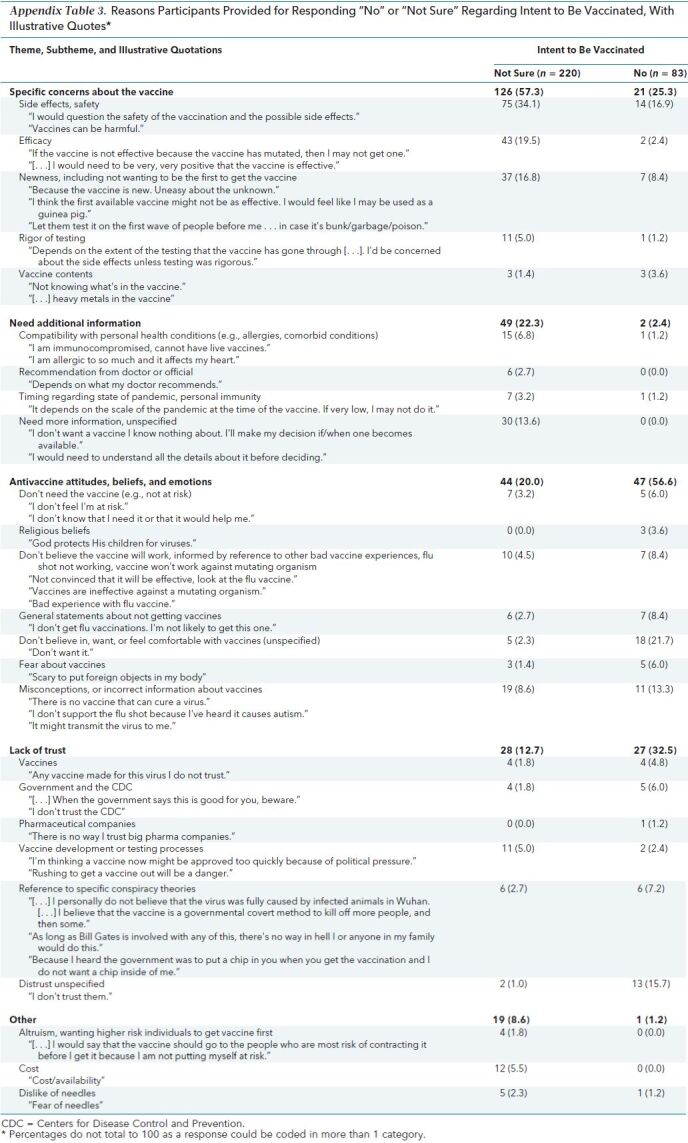
Of the 420 participants who were unsure or did not intend to be vaccinated, 303 (72.1%) provided a reason for their response and constitute the sample for the qualitative analysis. The 118 remaining participants who answered “not sure” or “no” (28.1%) did not provide a reason for their hesitancy (for example, they did not respond, responded simply “don't know,” or provided an uninterpretable response). Participants' reasons for being unsure or not intending to be vaccinated are broadly categorized as having specific concerns about the vaccine; needing additional information; holding antivaccine attitudes, beliefs, or emotions; and not trusting entities involved in vaccine development, testing, or dissemination (Table 4). The most common reasons cited by participants who were not sure whether they will be vaccinated included specific concerns about the vaccine (such as safety or effectiveness) or a need for more information. In contrast, the most common reasons provided by participants who did not intend to be vaccinated included antivaccine attitudes, beliefs, or emotions, and lack of trust. Illustrative quotes are provided in Appendix Table 3 (available at Annals.org).
Table 4. Reasons Participants Provided for Responding “No” or “Not Sure” Regarding Intent to Be Vaccinated*.
Appendix Table 3. Reasons Participants Provided for Responding “No” or “Not Sure” Regarding Intent to Be Vaccinated, With Illustrative Quotes*.
Discussion
In this large, nationally representative sample, nearly one half (42.4%) of participants indicated hesitancy to be vaccinated against COVID-19 when a vaccine becomes available. This finding is especially striking considering that the survey was conducted during mid-April 2020, when the number of deaths per day due to COVID-19 were at or near peak levels of the initial surge in the United States (16). The percentage of individuals who intend to be vaccinated (57%) is only slightly higher than the percentage of adults who received the influenza vaccination (45%) during the 2018–2019 influenza season (17); this is surprising, given the increased severity, death rate, societal disruption, and resultant media coverage associated with the COVID-19 pandemic.
Increasing vaccination rates are expected to confer substantial benefits, including reductions in COVID-19–related hospitalizations, strain on hospital capacity, and deaths. For example, it has been estimated that increasing influenza vaccination coverage by 5 percentage points could have prevented 4000 to 11 000 hospitalizations in the 2017–2018 influenza season (18). The increased severity of COVID-19 compared with influenza suggests that the magnitude of benefit of increased coronavirus vaccination coverage could be even greater. The percentage of individuals who will need to be vaccinated to achieve herd protection is not yet defined for COVID-19 because it depends on vaccine effectiveness, patterns of population mixing, vaccination patterns, and the basic reproduction number (R0) (7) of the novel coronavirus. Using a pooled estimate of the R0 of 3.32 (19) and assuming a best-case scenario in which a vaccine has perfect effectiveness yields a projection that at least 70% of the population will need to be vaccinated to achieve herd protection. In fact, a newly developed coronavirus vaccine is unlikely to be perfectly effective, so the coverage required to achieve herd immunity will almost certainly be higher than 70%. Considering that intent as assessed in our study does not account for incomplete follow-through and barriers to vaccine access, it is likely that a substantial gap will exist in the number needed to be vaccinated to achieve herd protection and the number who receive vaccination. Concerted efforts will be needed to persuade the large percentage of individuals who are unsure about or opposed to being vaccinated against COVID-19 if we are to realize the substantial benefits afforded by high immunization coverage rates.
We found several independent predictors of being hesitant to be vaccinated against COVID-19; the strongest were lower educational attainment, Black race, not having had a recent influenza vaccination, and perceived personal risk for coronavirus, consistent with the findings of a national survey conducted by RTI (20). Evidence that these characteristics are predictive of vaccine hesitancy could be useful in targeting vaccine messaging and outreach to populations at risk for not being vaccinated. Our findings highlight the importance of social determinants of health, such as educational status (a close proxy for health literacy [21]) and race/ethnicity, and their influence on preventive health behaviors (22). Racial disparities in vaccination rates have been described for other vaccinations. For example, rates of influenza vaccination among African American persons (39.4%) and Hispanic persons (37.1%) were substantially lower than among White persons (48.7) during 2018–2019 (17). These differences are particularly concerning given the disproportionately high toll of COVID-19 among African American communities (23–26). The confluence of increased COVID-19 disease burden and potential for decreased receipt of vaccination has the potential to substantially magnify health-related disparities experienced by African American persons. Our findings highlight the need for vaccine implementation strategies that anticipate racial gaps in COVID-19 vaccination. These strategies could draw on the approaches used to successfully close racial disparities in measles vaccination while being mindful of persistently lower rates of influenza vaccination rates among minority adults stemming from lack of trust in health care (27). Prior research has demonstrated the importance of social norms and perceived disease risk in influencing vaccination decisions among African American persons and could be explored as a means of fostering coronavirus vaccine acceptance among this population (28, 29). The association between intent to be vaccinated and perceived risk for coronavirus suggests this may be a particularly important lever for promoting vaccination.
In addition to being targeted for populations least likely to be vaccinated, such as members of racial and ethnic minority groups and individuals of low health literacy, successful vaccination campaigns will need to leverage an understanding of why individuals may be hesitant to be vaccinated in order to tailor messaging to mitigate these concerns. Concern about vaccine safety was one of the most commonly cited reasons for being unsure about accepting vaccination in the present study, consistent with studies of other vaccines (30). A Reuters poll found that approximately 75% of Americans would agree to be vaccinated against COVID-19 if they received assurances about the safety of the vaccine (31). Collectively, these findings suggest that transparent reporting of vaccine safety in a way that people of all educational levels can understand is likely to be an effective strategy to increase public uptake of vaccination. However, many participants in our study and the Reuters poll indicated hesitancy to be among the first to be vaccinated, which will probably delay achievement of high vaccination coverage rates for COVID-19.
Over one half (56.6%) of respondents who provided a reason for not intending to be vaccinated referred to antivaccine attitudes, beliefs, or emotions. Of these, many indicated only that they did not like, want, or believe in vaccines, whereas others made explicit reference to scientifically inaccurate information, such as the association between vaccines and autism and that it is not possible to vaccinate against a virus. These beliefs and essentially emotional responses to vaccination are likely to be among the hardest to overcome, because information alone is unlikely to have an effect. It may be that messages designed to engage and influence emotions, such as narratives or stories, will be more effective than expository or informational health messages (32).
Lack of trust was the second most common reason for responding “no” to intent to be vaccinated. Trust has been shown to be a determinant of vaccine uptake (33), suggesting this finding is likely to be of consequence and indicating a need for strategies aimed at increasing trust among individuals with greater degrees of vaccine skepticism. We found that circulating conspiracy theories about the coronavirus vaccination have taken hold among a small percentage of participants, in addition to more common misconceptions about vaccines. Further research is needed to develop effective strategies to combat conspiracy theories and misinformation (34). Some participants in our study also cited prior experience with the influenza vaccine “not working” as a reason to believe a vaccine against the coronavirus will not be effective, demonstrating the negative effects of perceived ineffective vaccines on overall vaccine acceptance. Given the real possibility for variable rates of effectiveness among the COVID-19 vaccines currently in development and the possible need for revaccination, public health officials might consider proactively acknowledging this possibility to avoid further loss of trust if or when this happens.
Surprisingly, very few vaccine-hesitant participants indicated a need or desire for a recommendation from a physician. However, there is evidence that patients whose physicians recommend a vaccine are more likely to be vaccinated than patients who do not (35). It has been argued that physicians are well-positioned to address misinformation, discuss risk, and convey the seriousness of COVID-19 in a way that is tailored to the unique needs of the individual patient during an encounter (36). Such conversations may be the ideal but may be difficult to implement in time-limited primary care encounters, where there are typically many competing priorities. In addition, the effectiveness of such conversations will almost certainly depend on the patient having trust in the physician and the physician having the requisite time, skills, and comfort to address the emotion-laden topic of vaccine hesitancy. Given the time constraints of primary care and the potential need for physicians to receive additional training to enable them to successfully address vaccine-related concerns, health systems might consider an alternative strategy in which trained vaccine counselors use motivational interviewing to engage vaccine-hesitant individuals. This approach has been effective at increasing rates of infant vaccine coverage and adolescent human papillomavirus vaccination (37, 38). We have identified characteristics, such as not previously receiving an influenza vaccine, that are readily available in the electronic health record and could easily be used to identify COVID-19 vaccine–hesitant individuals who might especially benefit from the motivational interviewing approach. Our findings suggest that a multipronged approach may be needed in which trusted physicians promote vaccine uptake against a backdrop of innovative approaches and channels to combat vaccine misinformation, consistent with the body of literature of strategies to address vaccine hesitancy (39).
A strength of our study is that the large, nationally representative sample allows generalization of our findings. In addition, the timing of the survey administration coincided with a peak time of the pandemic in many parts of the United States, making the findings particularly timely and salient.
Our study also has limitations. First, we queried individuals about their intent to be vaccinated at a time when a vaccination is not yet available. It is possible that as more details regarding a potential vaccine are known, some participants who indicated their response depended on additional information may change their response. In addition, our study was not designed to determine what additional information is needed, or how best to deliver it. Future research is needed to better delineate the types of assurances needed and the messengers most likely to be trusted (for example, community leaders and religious leaders).
In conclusion, we found that a substantial proportion (42.2%) of participants in a national survey conducted during the coronavirus pandemic would be hesitant to accept vaccination against COVID-19. Black race was one of the strongest independent predictors of not accepting vaccination; this is especially alarming, given the outsized impact of COVID-19 among African-Americans. Our findings suggest that many of the individuals who responded “not sure” may accept vaccination if given credible information that the vaccine is safe and effective. As vaccine development proceeds at an unprecedented pace, parallel efforts to proactively develop messages to foster vaccine acceptance are needed to achieve control of the COVID-19 pandemic.
Footnotes
This article was published at Annals.org on 4 September 2020
References
- 1. World Health Organization. Coronavirus disease (COVID-19): situation report 106. World Health Organization; 2020. Accessed at www.who.int/docs/default-source/coronaviruse/situation-reports/20200505covid-19-sitrep-106.pdf?sfvrsn=47090f63_2 on 9 May 2020.
- 2. Nicola M, Alsafi Z, Sohrabi C, et al. The socio-economic implications of the coronavirus pandemic (COVID-19): a review. Int J Surg. 2020;78:185-93. [PMID: 32305533] doi:10.1016/j.ijsu.2020.04.018 [DOI] [PMC free article] [PubMed]
- 3. Phua J, Weng L, Ling L, et al; Asian Critical Care Clinical Trials Group. Intensive care management of coronavirus disease 2019 (COVID-19): challenges and recommendations. Lancet Respir Med. 2020;8:506-17. [PMID: 32272080] doi:10.1016/S2213-2600(20)30161-2 [DOI] [PMC free article] [PubMed]
- 4. Ipsos. What worries the world. April 2020. Accessed at www.ipsos.com/sites/default/files/ct/news/documents/2020-04/what-worries-the-world-april-2020-ipsos.pdf on 7 May 2020.
- 5. Ipsos. Topline & methodology. 2020. Accessed at www.ipsos.com/sites/default/files/ipsos-coronavirus-us-aggregate-topline-050120.pdf on 9 May 2020
- 6. Hajj Hussein I, Chams N, Chams S, et al. Vaccines through centuries: major cornerstones of global health. Front Public Health. 2015;3:269. [PMID: 26636066] doi:10.3389/fpubh.2015.00269 [DOI] [PMC free article] [PubMed]
- 7. Fine P, Eames K, Heymann DL. “Herd immunity”: a rough guide. Clin Infect Dis. 2011;52:911-6. [PMID: 21427399] doi:10.1093/cid/cir007 [DOI] [PubMed]
- 8. Zhang J, Xie B, Hashimoto K. Current status of potential therapeutic candidates for the COVID-19 crisis. Brain Behav Immun. 2020;87:59-73. [PMID: 32334062] doi:10.1016/j.bbi.2020.04.046 [DOI] [PMC free article] [PubMed]
- 9. Kim E, Erdos G, Huang S, et al. Microneedle array delivered recombinant coronavirus vaccines: immunogenicity and rapid translational development. EBioMedicine. 2020;55:102743. [PMID: 32249203] doi:10.1016/j.ebiom.2020.102743 [DOI] [PMC free article] [PubMed]
- 10. Corum J, Grady D, Wee SL, et al. Coronavirus vaccine tracker. The New York Times. 2020. Accessed at www.nytimes.com/interactive/2020/science/coronavirus-vaccine-tracker.html on 26 August 2020.
- 11. Salmon DA, Dudley MZ, Glanz JM, et al. Vaccine hesitancy: causes, consequences, and a call to action. Am J Prev Med. 2015;49:S391-8. [PMID: 26337116] doi:10.1016/j.amepre.2015.06.009 [DOI] [PubMed]
- 12. Patel M, Lee AD, Clemmons NS, et al. National update on measles cases and outbreaks—United States, January 1-October 1, 2019. MMWR Morb Mortal Wkly Rep. 2019;68:893-6. [PMID: 31600181] doi:10.15585/mmwr.mm6840e2 [DOI] [PMC free article] [PubMed]
- 13. Hotez PJ. Texas and its measles epidemics. PLoS Med. 2016;13:e1002153. [PMID: 27780206] doi:10.1371/journal.pmed.1002153 [DOI] [PMC free article] [PubMed]
- 14.WHO releases list of 10 threats to global health. NEJM Journal Watch. 18 January 2019. Accessed at www.jwatch.org/fw114986/2019/01/18/who-releases-list-10-threats-global-health on 26 August 2020.
- 15. Braun V, Clarke V. Thematic analysis. In: Cooper H, Camic PM, Long DL, et al, eds. APA Handbook of Research Methods in Psychology. Vol. 2. American Psychological Assoc; 2012:57-71.
- 16. Institute for Health Metrics and Evaluation. COVID-19 projections. 2020. Accessed at https://covid19.healthdata.org/united-states-of-america on 6 May 2020.
- 17. Centers for Disease Control and Prevention. Flu vaccination coverage, United States, 2018-19 influenza season. 26 September 2019. Accessed at www.cdc.gov/flu/fluvaxview/coverage-1819estimates.htm on 6 May 2020.
- 18. Hughes MM, Reed C, Flannery B, et al. Projected population benefit of increased effectiveness and coverage of influenza vaccination on influenza burden in the United States. Clin Infect Dis. 2020;70:2496-502. [PMID: 31344229] doi:10.1093/cid/ciz676 [DOI] [PMC free article] [PubMed]
- 19. Alimohamadi Y, Taghdir M, Sepandi M. Estimate of the basic reproduction number for COVID-19: a systematic review and meta-analysis. J Prev Med Public Health. 2020;53:151-7. [PMID: 32498136] doi:10.3961/jpmph.20.076 [DOI] [PMC free article] [PubMed]
- 20. Kelly B, Bann C, Squiers L, et al. Predicting willingness to vaccinate for COVID-19 in the US. JHC Impact. 12 May 2020. Accessed at https://jhcimpact.com/posts/f/predicting-willingness-to-vaccinate-for-covid-19-in-the-us on 10 July 2019.
- 21. Paasche-Orlow MK, Parker RM, Gazmararian JA, et al. The prevalence of limited health literacy. J Gen Intern Med. 2005;20:175-84. [PMID: 15836552] [DOI] [PMC free article] [PubMed]
- 22. Scott TL, Gazmararian JA, Williams MV, et al. Health literacy and preventive health care use among Medicare enrollees in a managed care organization. Med Care. 2002;40:395-404. [PMID: 11961474] [DOI] [PubMed]
- 23. Yancy CW. COVID-19 and African Americans. JAMA. 2020. [PMID: 32293639] doi:10.1001/jama.2020.6548 [DOI] [PubMed]
- 24. Garg S, Kim L, Whitaker M, et al. Hospitalization rates and characteristics of patients hospitalized with laboratory-confirmed coronavirus disease 2019—COVID-NET, 14 states, March 1-30, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:458-64. [PMID: 32298251] doi:10.15585/mmwr.mm6915e3 [DOI] [PMC free article] [PubMed]
- 25. Gold JAW, Wong KK, Szablewski CM, et al. Characteristics and clinical outcomes of adult patients hospitalized with COVID-19—Georgia, March 2020. MMWR Morb Mortal Wkly Rep. 2020;69:545-50. [PMID: 32379729] doi:10.15585/mmwr.mm6918e1 [DOI] [PMC free article] [PubMed]
- 26. Vahidy FS, Nicolas JC, Meeks JR, et al. Racial and ethnic disparities in SARS-CoV-2 pandemic: analysis of a COVID-19 observational registry for a diverse U.S. metropolitan population. medRxiv. Preprint posted online 12 May 2020. doi:10.1101/2020.04.24.20073148 [DOI] [PMC free article] [PubMed]
- 27. Bibbins-Domingo K. This time must be different: disparities during the COVID-19 pandemic [Editorial]. Ann Intern Med. 2020;173:233-4. [PMID: 32343767] doi:10.7326/M20-2247 [DOI] [PMC free article] [PubMed]
- 28. Quinn SC, Hilyard KM, Jamison AM, et al. The influence of social norms on flu vaccination among African American and White adults. Health Educ Res. 2017;32:473-86. [PMID: 29220514] doi:10.1093/her/cyx070 [DOI] [PMC free article] [PubMed]
- 29. Freimuth VS, Jamison AM, An J, et al. Determinants of trust in the flu vaccine for African Americans and Whites. Soc Sci Med. 2017;193:70-9. [PMID: 29028558] doi:10.1016/j.socscimed.2017.10.001 [DOI] [PMC free article] [PubMed]
- 30. Karafillakis E, Larson HJ; ADVANCE consortium. The benefit of the doubt or doubts over benefits? A systematic literature review of perceived risks of vaccines in European populations. Vaccine. 2017;35:4840-50. [PMID: 28760616] doi:10.1016/j.vaccine.2017.07.061 [DOI] [PubMed]
- 31. Bernstein S. Most Americans would take coronavirus vaccine if deemed safe: Reuters/Ipsos poll. Reuters Health News. 6 May 2020. Accessed at www.reuters.com/article/us-health-coronavirus-usa-poll/most-americans-would-take-coronavirus-vaccine-if-deemed-safe-reuters-ipsos-poll-idUSKBN22I019 on 6 May 2020.
- 32. McQueen A, Kreuter MW, Kalesan B, et al. Understanding narrative effects: the impact of breast cancer survivor stories on message processing, attitudes, and beliefs among African American women. Health Psychol. 2011;30:674-82. [PMID: 21895370] doi:10.1037/a0025395 [DOI] [PMC free article] [PubMed]
- 33. Larson HJ, Clarke RM, Jarrett C, et al. Measuring trust in vaccination: a systematic review. Hum Vaccin Immunother. 2018;14:1599-609. [PMID: 29617183] doi:10.1080/21645515.2018.1459252 [DOI] [PMC free article] [PubMed]
- 34. Trethewey SP. Strategies to combat medical misinformation on social media [Editorial]. Postgrad Med J. 2020;96:4-6. [PMID: 31732511] doi:10.1136/postgradmedj-2019-137201 [DOI] [PubMed]
- 35. Lu PJ, Srivastav A, Amaya A, et al. Association of provider recommendation and offer and influenza vaccination among adults aged > =18 years—United States. Vaccine. 2018;36:890-8. [PMID: 29329685] doi:10.1016/j.vaccine.2017.12.016 [DOI] [PubMed]
- 36. Wray RJ, Jupka K, Ross W, et al. How can you improve vaccination rates among older African Americans? J Fam Pract. 2007;56:925-9. [PMID: 17976341] [PubMed]
- 37. Lemaitre T, Carrier N, Farrands A, et al. Impact of a vaccination promotion intervention using motivational interview techniques on long-term vaccine coverage: the PromoVac strategy. Hum Vaccin Immunother. 2019;15:732-9. [PMID: 30457421] doi:10.1080/21645515.2018.1549451 [DOI] [PMC free article] [PubMed]
- 38. Dempsey AF, Pyrznawoski J, Lockhart S, et al. Effect of a health care professional communication training intervention on adolescent human papillomavirus vaccination: a cluster randomized clinical trial. JAMA Pediatr. 2018;172:e180016. [PMID: 29507952] doi:10.1001/jamapediatrics.2018.0016 [DOI] [PMC free article] [PubMed]
- 39. Jarrett C, Wilson R, O'Leary M, et al; SAGE Working Group on Vaccine Hesitancy. Strategies for addressing vaccine hesitancy—a systematic review. Vaccine. 2015;33:4180-90. [PMID: 25896377] doi:10.1016/j.vaccine.2015.04.040 [DOI] [PubMed]