

Abstract
Arthroscopic techniques are considered the gold standard for treatment of displaced avulsion fractures of the anterior cruciate ligament. However, most arthroscopic surgical techniques and fixation methods are technically demanding and require removal of hard implant. This report describes a new, easy, safe, and all-arthroscopic method for reduction and fixation of displaced tibial intercondylar eminence fractures by using 1 anchor and 1 Pushlock.
From January 2015 to June 2017, 8 adult patients with type II and III displaced tibial intercondylar eminence fractures were operated using this technique. Clinical assessment included patient demographics, cause of injury, delay before surgery, operation time, time to return to work and sport, International Knee Documentation Committee scores, and Lysholm knee scores.
The average operation time was 48 minutes. The average follow-up period was 12.5 months. At the 6-month follow-up, all patients had acquired fracture union and complete functional recovery and were able to return to work. International Knee Documentation Committee objective scores and Lysholm knee scores were 92.4 (range 88–94) and 93.6 (range 90–96), respectively. At the last follow-up, anterior drawer, Lachman's test, and pivot shift tests were negative, and all patients had returned to their preinjury activity levels.
Arthroscopic fixation by use of 1 anchor and 1 Pushlock is an easy, safe, and minimally invasive technique for treatment of displaced tibial intercondylar eminence fractures and does not require further surgery to remove fixation devices.
Level of Evidence: Level IV, therapeutic case series
Keywords: anterior cruciate ligament, arthroscopic fixation, avulsion fracture, knee joint, tibial eminence fracture
1. Introduction
Avulsion fracture of the anterior cruciate ligament (ACL) from the tibial eminence is a major intra-articular injury that primarily occurs in children and adolescents.[1] At times, these lesions can also occur in adults and are equivalent to an acute rupture of ACL. According to Kendall et al,[2] 40% of such fractures occur in adults. Moreover, recent studies have indicated a much higher incidence of adult morbidity than previously known.[3,4] In adult patients, the primary cause of this avulsion fracture is high-energy trauma, such as motor vehicle accidents, contact sports (soccer, rugby, and football), or fall from a bicycle.[5,6]
The most common classification for these fractures was developed by Meyers and McKeever and it is reliable for decision-making in diagnosis and treatment.[7] Surgical treatment is indicated for Type III and IV fractures and for Type II fractures when attempt at reduction has failed.[1,8]
Different arthroscopic fixation techniques (materials) have been reported such as Kirschner wires, cannulated screws, pull-out sutures, sutures with anchors, metallic sutures, intra-articular buttons, bioabsorbable nails, Herbert screws, and tight-rope fixations.[1,8–10] However, some of these techniques introduce risks of fracture fragment comminution, extension block by a screw head, implant breakage, loosening or migration, infection, and nonunion. In addition, most of them are technically demanding and require removal of hard implant.
The purpose of this article is to present a technical variation that provides an easy, safe, and all-arthroscopic technique for reduction and fixation of displaced tibial intercondylar eminence fractures by using 1 anchor, “figure 8” sutures passing through soft tissues of ACL, and 1 Pushlock anchor working as a tension band, instead of a direct fixation method.
2. Materials and methods
According to the classification by Meyers and McKeever,[7] 8 patients with type II and III displaced tibial intercondylar eminence fractures who received all-arthroscopic fixation by using 1 anchor and 1 Pushlock anchor were enrolled between January 2015 and June 2017. Patients included 3 female and 5 male patients, with ages ranging 19 to 41 (mean, 25.9) years. The left knee was involved in 4 cases and the right in 4. All patients but 1 had meniscal tears. Patient characteristics are outlined in Table 1. The study was approved by the ethics committee of Anhui Second People's Hospital.
Table 1.
Patient characteristics.
The average waiting time before surgery was 4 (range 3–6) days. Radiological examination consisted of anteroposterior and lateral radiographs as well as magnetic resonance imaging scans of the affected knee before surgery.
Both the International Knee Documentation Committee (IKDC) scores and Lysholm knee scores were used to evaluate clinical results, including patient demographics,[13] cause of injury, delay before surgery, time for surgery, time to return to work and sport, postoperative pain, and stability analysis.
2.1. Surgical technique
All patients underwent surgery within 6 days after trauma. The surgical procedure was performed under general or epidural anesthesia, and the patient was placed in the supine position with a thigh tourniquet and with the knee in 90° flexion. The lower limb was exsanguinated, and a pneumatic tourniquet was inflated to minimize blood loss and maximize visualization.
A standard anterolateral visual portal and anteromedial working portal were established, and complete diagnostic arthroscopic examination of the joint was performed, with inspection for chondral damage, loose bodies, and meniscal tears. Joint visualization was enhanced by adequate debridement and shaving of blood clots. The fracture site was exposed with a shaver and carefully examined with an arthroscopic probe to confirm the anatomical condition and integrity of ACL. Inserted tissues such as fat pad, fracture debris, or clots and the posterior part of the transverse ligament were removed using appropriate tools. Subsequently, the bony bed was dug slightly deeper so that the avulsed bone fragment could be easily reduced.
Reduction of the tibial fragment was performed using a probe or a vessel clamp. Thereafter, an additional anterior portal (through the patellar tendon approach) was created, and a 1.5-mm K-wire was drilled into the fragment under direct arthroscopic vision to fix it temporarily (Fig. 1). For eventual fixation, 1 anchor loaded with 2 strands of No. 2 braided polyester suture and 1 Pushlock anchor were used.
Figure 1.
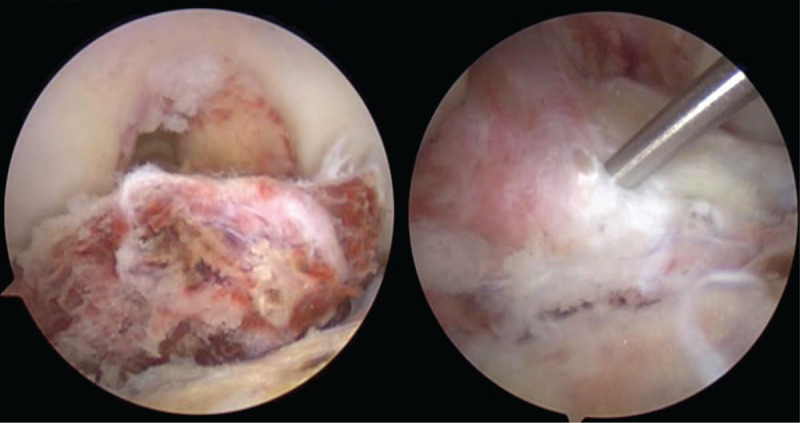
Fracture exposure and a 1.5-mm K-wire transitory fixation.
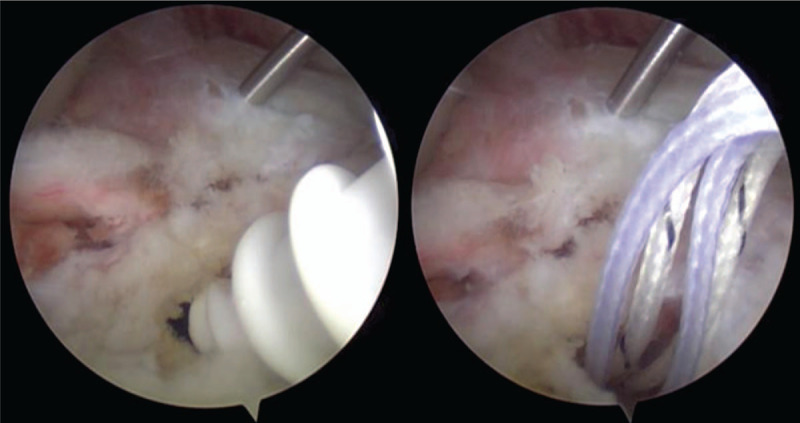
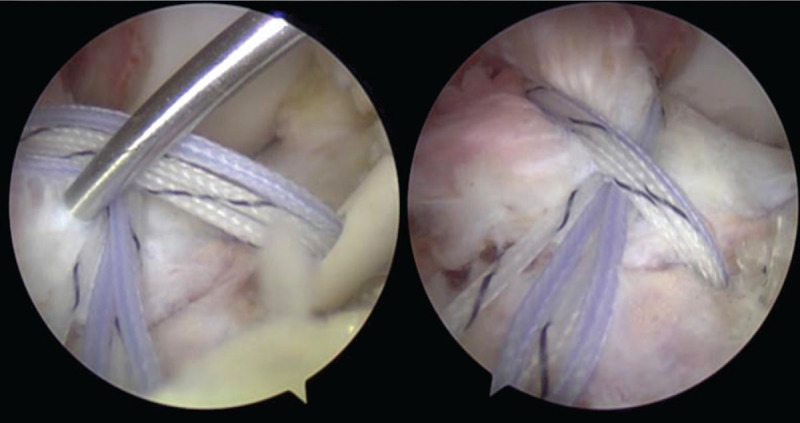
The first anchor was placed 2 to 3 mm anterolateral or anteromedial to the fracture rim, not through the bony fragment (Fig. 2). A 90° curved suture hook was used to pushed through the back of ACL just above its tibial insertion in order to lead and leave 1 guiding thread around the back of ACL. After introduction of a clear cannula through 1 portal, threads of the anchor and the guiding thread were pulled out from the cannula so that the threads could not get intertwined because of tissues around the portal. Subsequently, threads of the anchor were pulled through the back of ACL with the help of the guiding thread. Threads of the anchor were inserted from another side of ACL so that it moved around ACL insertion in the figure “8” (Fig. 3).
Figure 2.
First anchor planted to the fracture rim.
Figure 3.
“Figure of 8” formed around ACL with the help of a suture hook and guiding threads.
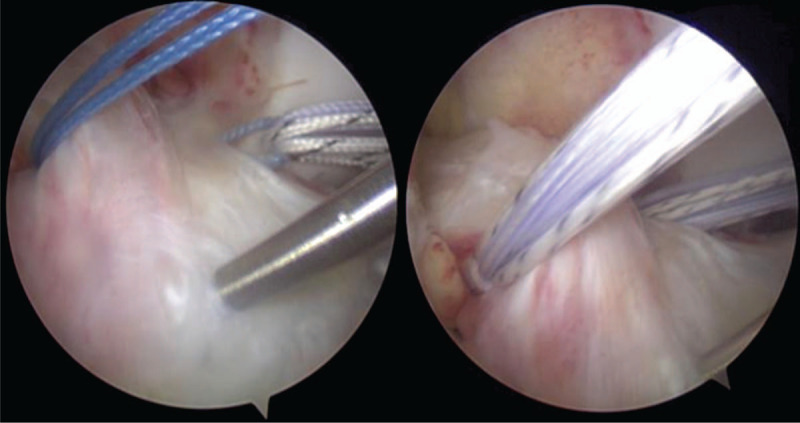
Subsequently, the second anchor(Pushlock) was planted on another side of the anterior rim of the fragment. After exposing the ground bone at the expected point, a hole was drilled using a matched instrument. Threads of the first anchor were inserted into the hole of the Pushlock anchor. Next, the forepart of the Pushlock anchor was inserted into the hole and the wires were pulled and tensed to achieve primary fixation. Thereafter, the K-wire was slowly pulled out using an electric drill, and the Pushlock anchor was finally fixed so that the threads and anchors worked as a tension band (Figs. 4 and 5).
Figure 4.
Second anchor (Pushlock) planted to fix the thread on another side.
Figure 5.
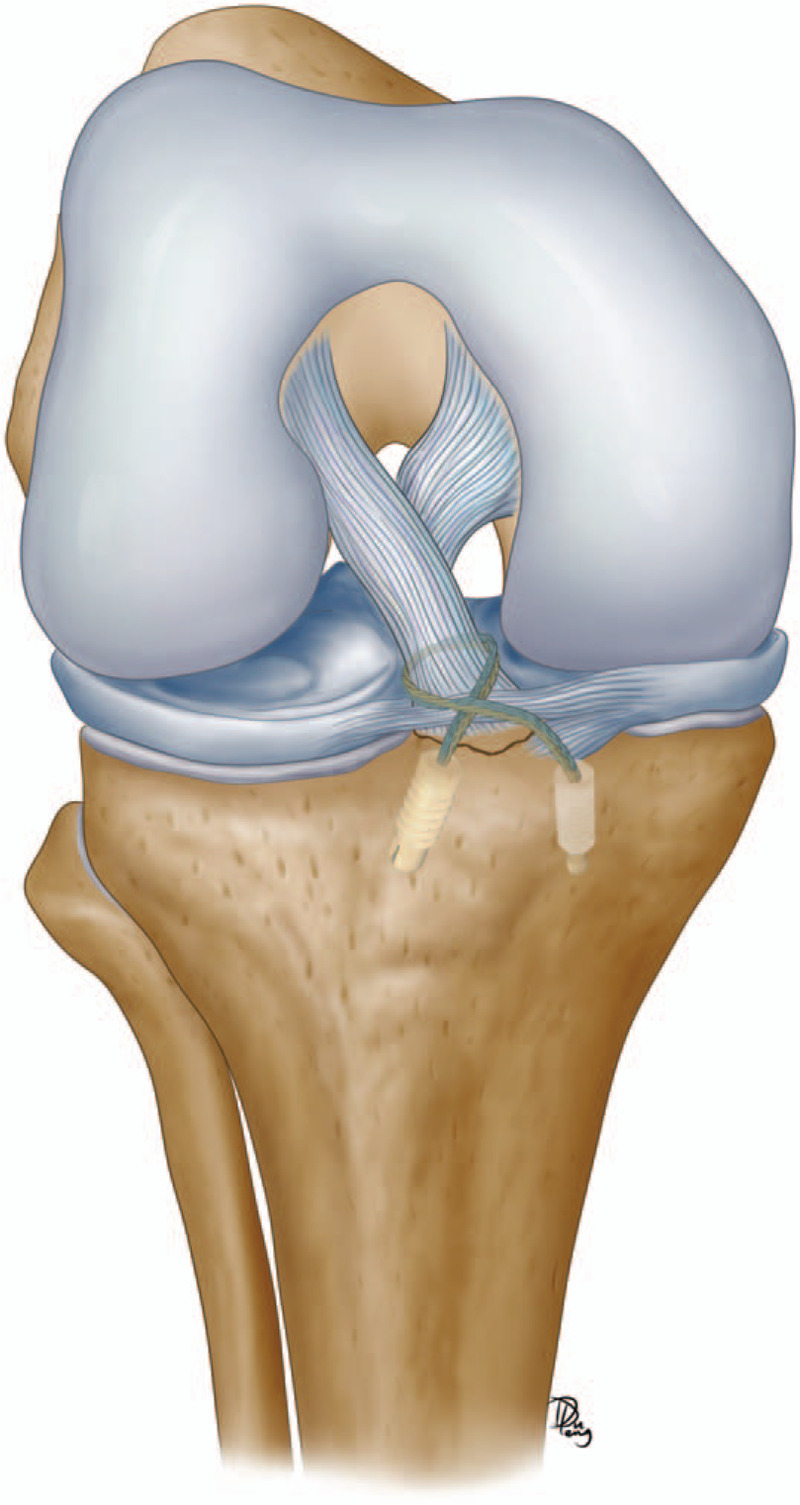
Graphic representation of fixation.
Finally, the knee joint was checked arthroscopically again. Fracture reduction and stability were evaluated by probing during both knee flexion and extension. After surgery, routine anteroposterior and lateral knee radiographs were recorded and evaluated to confirm fracture reduction.
After surgery, a brace was placed with the knee in 20° to 30° flexion for 3 weeks for pain control and further protection. Patients were allowed immediate partial weight bearing with brace protection and crutch support. Patellar mobilization, quadriceps isometric strengthening exercises, and straight leg raise exercises were started 1 day after surgery. After 3 weeks, gradual flexion and full weight bearing were allowed with brace protection to regain complete range of movement (ROM). Walking without brace and crutch was not allowed for 6 weeks after surgery. Nonimpact activities such as cycling and swimming were permitted at 8 weeks. Running and progressive return to athletic activities were allowed at 12 weeks.
Healing status of the fracture was assessed on radiographs at 1, 3, 6, and 12 months after surgery (Fig. 6). Clinical subjective assessment was performed at 6 and 12 months after surgery by using Lysholm knee scores and IKDC subjective questionnaire and objective form.
Figure 6.
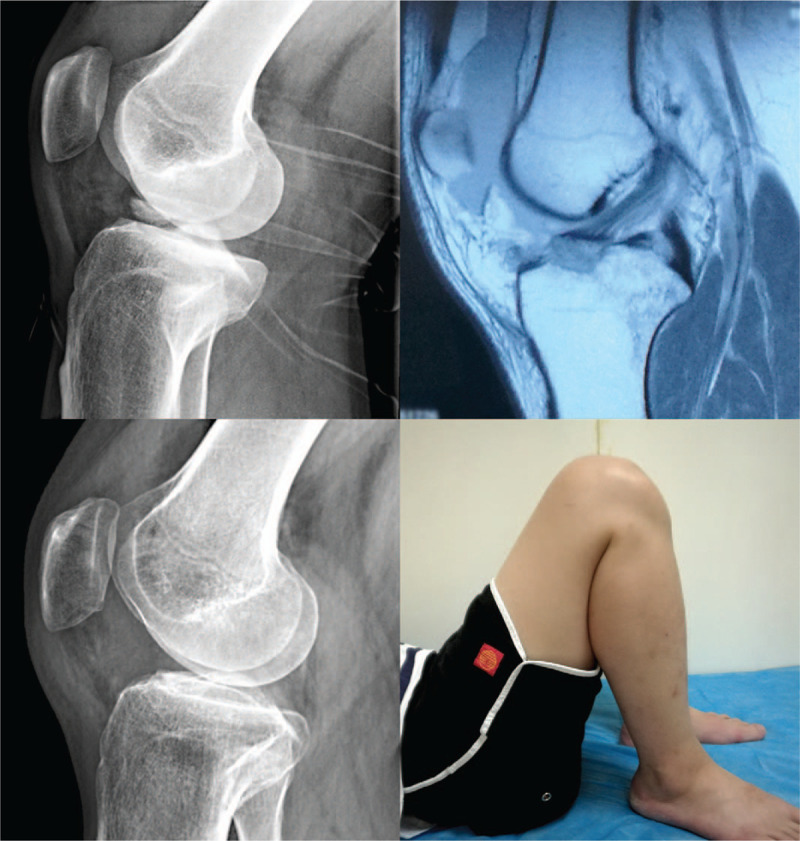
Imaging manifestations and functional restoration in one case.
3. Results
The median patient age was 25.9 years, and the average operation time was 48 minutes. No intraoperative complications occurred, and fractures were satisfactorily reduced in all patients. The average follow-up duration was 12.5 months. At 6 weeks after surgery, ROM was > 90° in all patients. At the 6-month follow-up, all patients showed complete functional recovery and were able to return to work. At the last follow-up, results of anterior drawer, Lachman's test, and pivot shift tests were negative in all patients. The mean side-to-side difference in KT-2000 arthrometer (MEDmetric Corp., San Diego, CA) with the contralateral knee was 1 ± 1.4 mm. The mean global IKDC objective score and Lysholm knee score were 92.4 (range 88–94) and 93.6 (range 90–96), respectively. At the 6-month follow-up, all patients had acquired fracture union without anchor loosening (Fig. 5). At the last follow-up, all patients had returned to their preinjury activity levels.
4. Discussion
Avulsion fractures of ACL are becoming increasingly common in China.[11] Reasons for this increased rate include greater rate of people engaging in physical activity and competitive sports and increased occurrence of road-traffic accidents.
Based on common consensus,[1,2,6,8] Type I undisplaced tibial spine fractures can be managed with a knee cast or splint in extension or mild flexion (20°–30°) for 6 to 12 weeks. Most orthopedic surgeons agree that in Type II tibial eminence fractures with slight displacement, reduction can be achieved with aspiration of hemarthrosis in certain cases, and then, a cast can be applied. However, Type II fractures, particularly wherein attempts at reduction have failed, and Type III and IV fractures require surgical management because displaced fractures can result in nonunion and knee instability.
Open arthrotomy techniques have several disadvantages and more complications such as greater soft-tissue damage, greater postoperative pain, longer hospital stay, and delayed rehabilitation. Recently, arthroscopic techniques have been successfully developed to check intra-articular injuries, accurately reduce fracture fragments, treat associated soft-tissue injuries, and remove loose fragments. Therefore, arthroscopic techniques are considered the gold standard for treatment of such lesions.[3,4,8,12–16]
One of the most commonly used fixation techniques reported in literature is cannulated screws.[4,17,18] The cannulated screw technique includes a simple, firm fixation and allows early mobilization and weight-bearing but has certain disadvantages and contraindications. Use of cannulated screws is challenging if the fracture fragment is small in size or comminuted because its insertion can lead to further displacement. Moreover, the screw head is large and must be placed over the top of the fragment; incorrect positioning of the screw can also cause impingement and cartilage damage. Furthermore, secondary surgery is needed to remove the screw in case of persistent discomfort at the site of fixation after fracture healing. In addition, passage of bone tunnels through growth plates can cause bone growth disorders.
Another common technique used to fix fragments is suture fixation.[19,20] Various suture fixations using metallic wires, or No. 5 Ethibond wires have been extensively described in available literature with extremely favorable outcomes. However, concerns exist regarding difficulties of suture passage and prolonged operation times. In fact, such fixations can be technically demanding and can cause potential intraoperative complications.
Other arthroscopic fixation techniques have also been reported, including bioabsorbable nails, percutaneous K-wires, sutures with 1 anchor, and suspensory button fixation.[1,10–12,21] Overall, clinical results with such procedures have been excellent. However, most of these are time consuming and technically demanding, require removal of hard tissues, and can sometimes lead to complications.
In the present study, we tried to fix fragments by using 2 anchors: one common anchor and 2 knotless anchor (Pushlock). The primary outcome was that our method was easy, safe, reliable, and an all-arthroscopic technique for reduction and fixation of displaced tibial intercondylar eminence fractures. In the study cohort, all fractures were satisfactorily reduced, and no subsequent displacement or fixation loosening occurred during follow-up. No intraoperative or postoperative complications were observed.
One of the advantages of this fixation technique is that it is easy to treat all fractures from the common AM and AL portals, with no need for an additional anterior oblique incision that is used in other suture fixation techniques. Hence, it saves time and reduces damages. Another advantage is that this technique can fix fragments like tension-band behavior, because the second anchor is inserted to reduce and also dynamically pull down the avulsed fragment during knee movement. Furthermore, this method can perhaps be used to fix fractures with small or comminuted fragments as threads of the anchor are twined around the insertion of ACL. In addition, no further interventions are required to remove any device.
Vega et al[22] reported the use of 2 metallic anchor wherein nonabsorbable braided sutures passed through soft tissues of ACL, and the avulsed bone fragment was held in place by tying a locking knot; this method was used to treat 7 patients (aged 7–20 years) with 5 type III fractures and 2 type IV fractures. At the last follow-up, all patients showed favorable outcomes with full ROM and stability, and all patients subsequently returned to their preinjury activity levels. This technique could avoid damage to the open epiphysis and could thus be used safely in pediatric and adult populations. Of note, clinical results of our study group were similar to results of this study, but we used 2 anchors. Thus, our method could probably achieve stronger fixation. In addition, 1 of our anchors was knotless, making it easier to reduce and fix a fragment.
Bley et al[23] reported 1 case, an 8-year-old boy, wherein they used 2 absorbable anchors with adjustable suture-tensioning technology to reduce and fix the fragment. In addition, they used fluoroscopy to check the drill-bit depth to ensure that the tibial growth plate was not damaged during anchor placement. The fixation methods used in the present study are partly similar to the aforementioned ones, but our suture method and type of anchor used were different. Moreover, Bley et al[24] only reported this method, without a series of case observations. Based on results of and comparisons with both aforementioned studies, our methods may be safely used in pediatric patients, even though we did not report any such cases.
5. Limitations
This study had certain limitations, including small sample size, relatively short follow-up duration, and absence of a control group. Moreover, additional biomechanical studies are warranted to confirm this 2-anchor fixation method, and the obtained results should be reviewed in light of the aforementioned limitations.
6. Conclusion
Above all, arthroscopic fixation by use of 1 anchor and 1 Pushlock is an easy, safe, and minimally invasive technique for treatment of displaced tibial intercondylar eminence fractures and does not require further surgery to remove fixation devices.
Author contributions
Defu Yu: developed search strategy and wrote the protocol.
Runze Yu: developed search strategy and supervision.
Jiebin Zhang: formal analysis and data curation.
Tao Chen: revised the manuscript and investigation.
Biao Zhang: revised the manuscript and investigation.
All authors have read and approved the final manuscript
Footnotes
Abbreviations: ACL = anterior cruciate ligament, IKDC = International Knee Documentation Committee, ROM = range of movement.
How to cite this article: Yu D, Yu R, Zhang J, Chen T, Zhang B. Arthroscopic treatment of adult displaced tibial eminence fractures with anchor and pushlock fixation. Medicine. 2020;99:38(e21237).
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
This research received a subsidy from the Health Commission of Anhui Province, China (2018SEYL001).
MeSH Terms: Anterior cruciate ligament, Knee joint, Suture technique, Arthroscopy
The authors have no conflicts of interest to disclose.
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
- [1].Osti L, Buda M, Soldati F, et al. Arthroscopic treatment of tibial eminence fracture: a systematic review of different fixation methods. Br Med Bull 2016;118:77–94.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].Kendall NS, Hsu SC, Chan KM. Facture of the tibial spine in adults and children. J Bone Joint Surg Br 1992;74:848–52.. [DOI] [PubMed] [Google Scholar]
- [3].Rajanish R, Mohammed J, Chandhan M, et al. Arthroscopic tibial spine fracture fixation: novel techniques. J Orthop 2018;15:373–4.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Bachmann KR, Edmonds EW. The pediatric ACL: tibial spine fracture. In: Parikh S, eds The Pediatric Anterior Cruciate Ligament Springer, Cham; 2018;211–22.. [Google Scholar]
- [5].Huang TW, Hsu KY, Cheng CY, et al. Arthroscopic suture fixation of tibial eminence avulsion fractures. Arthroscopy 2008;24:1232–8.. [DOI] [PubMed] [Google Scholar]
- [6].Shelbourne KD, Urch SE, Freeman H. Outcomes after arthroscopic excision of the bony prominence in the treatment of tibial spine avulsion fractures. Arthroscopy 2011;27:784–91.. [DOI] [PubMed] [Google Scholar]
- [7].Meyers MH, McKeever FM. Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am 1959;41-A:209–22.. [PubMed] [Google Scholar]
- [8].Bogunovic L, Tarabichi M, Harris D, et al. Treatment of tibial eminence fractures: a systematic review. J Knee Surg 2015;28:255–62.. [DOI] [PubMed] [Google Scholar]
- [9].Lubowitz JH, Elson WS, Guttmann D. Part II: arthroscopic treatment of tibial plateau fractures: intercondylar eminence avulsion fractures. Arthroscopy 2005;21:86–92.. [DOI] [PubMed] [Google Scholar]
- [10].Mardam-Bey SW, Bernholt DL, Bogunovic L, et al. Treatment of tibial eminence fractures. In: Anterior Cruciate Ligament 2018;555–7.. [Google Scholar]
- [11].Xu X, Liu Z, Wen H, et al. Arthroscopic fixation of pediatric tibial eminence fractures using suture anchors: a mid-term follow-up. Arch Orthop Trauma Surg 2017;137:1409–16.. [DOI] [PubMed] [Google Scholar]
- [12].Zaricznyj B. Avulsion fracture of the tibial eminence: treatment by open reduction and pinning. J Bone Joint Surg Am 1977;59:1111–4.. [PubMed] [Google Scholar]
- [13].Feagin JA, Jr. The office diagnosis and documentation of common knee problems. Clin Sports Med 1989;8:453–9.. [PubMed] [Google Scholar]
- [14].Hunter RE, Willis JA. Arthroscopic fixation of avulsion fractures of the tibial eminence: Technique and outcome. Arthroscopy 2004;20:113–21.. [DOI] [PubMed] [Google Scholar]
- [15].Sang W, Zhu L, Ma J, et al. A comparative study of two methods for treating type III tibial eminence avulsion fracture in adults. Knee Surg Sports Traumatol Arthrosc 2012;20:1560–4.. [DOI] [PubMed] [Google Scholar]
- [16].Hapa O, Barber FA, Süner G, et al. Biomechanical comparison of tibial eminence fracture fixation with high-strength suture, EndoButton, and suture anchor. Arthroscopy 2012;28:681–7.. [DOI] [PubMed] [Google Scholar]
- [17].Reynders P, Reynders K, Broos P. Pediatric and adolescent tibial eminence fractures: arthroscopic cannulated screw fixation. J Trauma 2002;53:49–54.. [DOI] [PubMed] [Google Scholar]
- [18].Sommerfeldt DW. Arthroscopically assisted internal fixation of avulsion fractures of the anterior cruciate ligament during childhood and adolescence. Oper Orthop Traumatol 2008;20:310–20.. [DOI] [PubMed] [Google Scholar]
- [19].Boutsiadis A, Karataglis D, Agathangelidis F, et al. Arthroscopic 4-point suture fixation of anterior cruciate ligament tibial avulsion fractures. Arthrosc Tech 2014;3:e683–7.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Gamboa JT, Durrant BA, Pathare NP, et al. Arthroscopic reduction of tibial spine avulsion: suture lever reduction technique. Arthrosc Tech 2017;6:e121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Loriaut P, Moreau PE, Loriaut P, et al. Arthroscopic treatment of displaced tibial eminence fractures using a suspensory fixation. Indian J Orthop 2017;51:187–91.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Vega JR, Irribarra LA, Baar AK, et al. Arthroscopic fixation of displaced tibial eminence fractures: a new growth plate-sparing method. Arthroscopy 2008;24:1239–43.. [DOI] [PubMed] [Google Scholar]
- [23].Bley JA, Pomajzl RJ, Smith PA. Knotless arthroscopic reduction and internal fixation of a displaced anterior cruciate ligament tibial eminence avulsion fracture. Am J Orthop (Belle Mead NJ) 2017;46:203–8.. [PubMed] [Google Scholar]