

Abstract
Introduction
African American/Black adults are severely underrepresented in basic, clinical, and behavioral research studies in Alzheimer's disease and related disorders (ADRD). Innovative, evidence‐based, and culturally salient strategies can maximize the recruitment of African American/Black adults into ADRD research.
Methods
We conducted and analyzed semi‐structured interviews to capture the research participation stories of African American/Black participants and study partners from the University of Pittsburgh's Alzheimer's Disease Research Center. The themes and messaging principles generated through this process informed the development of video‐ and text‐based materials that were evaluated for community member acceptance using focus groups.
Results
Focus group individuals (N = 36) generally favorably rated the video and text materials, characterizing them as “interesting,” “realistic,” and “convincing.”
Discussion
Capturing the narratives of African American/Black research participants is a critical component to developing culturally relevant materials for broader dissemination and is essential to advancing beyond information‐only recruitment approaches, which tend to rely disproportionately on negative messages.
Keywords: African American, Alzheimer's disease, Black, disparities, narrative, recruitment, research, storytelling
1. INTRODUCTION
Despite experiencing Alzheimer's disease–related health problems at a disproportionate rate, African American/Black adults are consistently and severely underrepresented in Alzheimer's disease and related disorders (ADRD) clinical and behavioral research projects. 1 , 2 For example, research shows that the prevalence of cognitive impairment is higher, 3 , 4 diagnoses are assigned later, 5 and Food and Drug Administration–approved treatments are instituted less frequently in this population as compared to non‐Hispanic Whites. 6 , 7 , 8 African American adults spend a greater proportion, over double, of their household income on out‐of‐pocket dementia care 9 when compared to non‐Hispanic Whites. While the need to understand and address these health and economic disparities is receiving unprecedented attention, both basic and clinical research in this area are hampered by a critical, nationwide shortfall of African American/Black research participants. 10
Research involving persons from underrepresented minority groups is crucial to advancing understanding of, and ultimately combating, health disparities in ADRD. Research indicates that African American/Black adults are willing to participate in research when recruited using high‐level engagement through community outreach and other creative strategies (e.g., lay educators). 11 Additionally, developing relationships with research participants and with key stakeholders in their communities is paramount. 12 , 13 However, the field of ADRD research continues to fall drastically short of the goals of recruiting representative samples of African American/Black adults into ADRD clinical trials. For example, African American/Black adults make up less than 5% of clinical trials for ADRD and autopsies in brain banks, and less than 15% of participant assessments for ADRD. 14 , 15 , 16
Given the clear need for innovative approaches to bolster recruitment of African American/Black adults, our overall goal was to design an effective health promotion intervention using a storytelling approach for ADRD research recruitment. Storytelling has been effective in studies designed to increase health access among Latino adults, 17 increase recruitment of rural Americans for type 2 diabetes studies, 18 , 19 , 20 improve blood pressure among African American/Black adults, 21 improve disparities in mental and physical health among Native American elders, 22 provide diabetes education to Somali and Latino adults, 23 and in other health studies. 24 , 25 , 26 , 27 , 28 Regardless of the disease context, what is most critical for success in a storytelling campaign is the cultural relevance of the messaging materials that are deployed. 29
This article describes the development of a set of storytelling materials to be used in a sequential cohort investigation of the impact of a culturally informed narrative campaign on the recruitment of African American/Black adults into ADRD research (also known as the Recruitment Innovations for Diversity Enhancement [RIDE] study).
2. MATERIAL DEVELOPMENT PROTOCOL
We used a multi‐step, iterative approach for the development and evaluation of community members’ acceptance of narrative materials to promote ADRD research recruitment among African American/Black adults (Figure 1).
FIGURE 1.
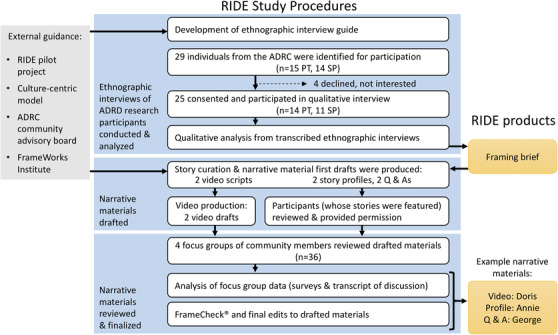
Flowchart of study protocol. Abbreviations: ADRC, Alzheimer's Disease Research Center; PT, patient; RIDE, Recruitment Innovations for Diversity Enhancement study; SP, study partner. Example narrative materials available in supporting information
2.1. Semi‐structured interviews
Semi‐structured (culturally focused) qualitative interviews were conducted with African American/Black adults currently participating in ADRD research at the University of Pittsburgh Alzheimer's Disease Research Center (ADRC; P50AG05133). Our sample size of 14 African American/Black ADRD research participants was determined by the qualitative research principle of data saturation. 30 Data saturation refers to the point at which coding suggests that no additional data collection would change the study findings. Participation in most ADRD research requires that participants be accompanied by a “study partner,” typically a family member or close friend. To ensure the validity of self‐report information on cognition, 31 we also interviewed 11 study partners of current ADRC participants.
Purposive sampling was used to ensure representation from a broad range of African American/Black research participants. 32 To understand a broad range of experiences, we closely monitored recruitment to ensure that we included individuals of varying ages (from mid‐life to late life) with a diverse range of educational levels, living arrangements, and experience with participation in different types of ADRC ancillary studies (brain imaging, genetic testing, clinical trials). As Table 1 shows, we included healthy controls as well as individuals with diagnoses of mild cognitive impairment or early stage dementia. We excluded those with Montreal Cognitive Assessment (MoCA) 33 scores of 18 or lower as more advanced cognitive impairment may have precluded participants from providing accurate accounts of their research participation experiences.
TABLE 1.
Semi‐structured interview sample characteristics
| Participant n = 14 | Study partner n = 11 | |
|---|---|---|
| Age, mean years (range) | 77 (64–100) | 73 (54–85) |
| Education, mean years (range) | 16 (12–19) | 15 (12–20) |
| Mean years at ADRC (range) | 7.67 (1–20) | 6.31 (1–16) |
| Sex | ||
| Female n (%) | 8 (57.1) | 7 (63.6) |
| Male n (%) | 6 (42.9) | 4 (36.4) |
| Race, Black n (%) | 14 (100) | 11 (100) |
| Place of residence* | ||
| Urban, n (%) | 10 (71.4) | 5 (45.5) |
| Suburban, n (%) | 4 (28.6) | 6 (54.5) |
| Relationship, patient/study partner | ||
| Spouse | 6 (43) | 6 (55) |
| Friend | 3 (21) | 2 (18) |
| Sibling | 2 (14) | 1 (9) |
| Other † | 3 (21) | 2 (18) |
| Diagnosis | ||
| No cognitive diagnosis | 8 (57) | n/a |
| MCI | 3 (21) | |
| Alzheimer's disease | 3 (21) | |
| Referral source to ADRC | ||
| Outreach | 4 (29) | 2 (18) |
| Doctor's office | 3 (21) | 4 (36) |
| Family | 2 (14) | 0 (0) |
| Other research studies | 2 (14) | 1 (9) |
| Unknown by participant | 2 (14) | 3 (27) |
| Other | 1 (7) | 1 (9) |
Abbreviations: ADRC, Alzheimer's Disease Research Center; MCI, mild cognitive impairment.
Distance from the ADRC ranged from 4 to 157 miles.
Other relationships include one uncle, one adult child, two cousins, and one grandmother.
Semi‐structured interviews were conducted separately with participants and their study partners. Each lead question began broadly, for example, “Tell me about how you learned about the Alzheimer's Research Center,” “Thinking back, what led you to consider participating in Alzheimer's research?” and “What has it been like to participate in Alzheimer's research?” Such lead questions were followed by probes to ensure the richest possible account of the enrollment process, including cultural considerations. Example probes included, “Who, if anyone, did you discuss your decision with?” “Have there been any drawbacks to volunteering for Alzheimer's research?” and “How has the experience of participating in research differed from what you expected?”
Qualitative interviews were audio‐recorded and transcripts were analyzed using standard line‐by‐line coding and theme generation. 34 Themes characterized participants’ motivations and barriers to research participation, as well as perceptions of the benefits and burdens of participating in ADRD research (Table 2).
TABLE 2.
Focus group sample characteristics
| Group 1 n = 12 | Group 2 n = 10 | Group 3 n = 7 | Group 4 n = 7 | Full sample n = 36 | |
|---|---|---|---|---|---|
| Age, range | 62–74 | 62–74 | 65–83 | 63–76 | 62–83 |
| Age, mean (SD) | 67 (2.98) | 69 (3.99) | 72 (6.08) | 68 (4.07) | 69 (4.45) |
| Sex: female, n (%) | 4 (33) | 8 (80) | 4 (57) | 4 (57) | 20 (56) |
| Ethnicity: African American, n (%) | 12 (100) | 10 (100) | 7 (100) | 7 (100) | 36 (100) |
| Education: ≥4‐year college, n (%) | 6 (50) | 7 (70) | 5 (71) | 5 (71) | 23 (64) |
| Relationship with AD*, n (%) | 4 (33) | 7 (70) | 4 (57) | 3 (43) | 18 (50) |
Abbreviations: AD, Alzheimer's disease; SD, standard deviation.
Endorsed having a friend or family member who has been affected by Alzheimer's disease or another dementia.
Findings from the thematic analysis were integrated with messaging principles by communication scientists at the FrameWorks Institute (www.frameworksinstitute.org), culminating in recommendations for communicating stories of ADRD research participation among African American/Black adults (Table 3).
TABLE 3.
List of FrameWorks’ recommendations from semi‐structured interviews
|
Abbreviation: AD, Alzheimer's disease; ADRC, Alzheimer's Disease Research Center.
Selected participant interviews were then used to derive “personas,” which mostly reflect the narratives and verbatim language of the participant with modifications to adhere to messaging recommendations (as noted above). Names were given to the personas and only when consent was included do the names of the personas match those of actual participants.
2.2. Drafting of narrative‐informed recruitment materials
FrameWorks recommendations (Table 3) guided the development of three types of recruitment materials: (1) videos, (2) profiles, and (3) question and answer (Q&A) sheets on ADRD research participation. Drafts of the video scripts and text for the profile and Q&A sheets (a total of six materials) were reviewed by consultants in the fields of health disparities, community engagement, and by communication scientists from FrameWorks. Materials were then refined before production of the videos and evaluation by community members.
2.3. Evaluating community members’ acceptance of recruitment materials
Four focus groups of 7–12 individuals (N = 36) each were conducted. All groups were comprised of individuals from our target audience of African American/Black adults in mid to late life (mean age of 69 years) with no memory complaints (Table 2).
RESEARCH IN CONTEXT
Systematic Review: A PubMed search yields descriptive studies of facilitators and barriers to African American/Black enrollment in Alzheimer's disease (AD) research, revealing a need to systematically develop and rigorously test new strategies.
Interpretation: The current study provides a rational framework for using culturally relevant narratives to develop a testable and replicable set of tools for African American/Black recruitment into AD research.
Future Directions: The materials developed herein will be deployed in the Recruitment Innovations for Diversity Enhancement (RIDE) study to address the important question, “Are storytelling strategies effective at increasing research participation into Alzheimer's disease and related disorders research amongst African American/Black adults?” a critical step in moving the field toward evidence‐based best practices for recruitment. This approach can be broadly adapted to develop and test recruitment tools in other underrepresented populations and diseases.
The focus group guide consisted of semi‐structured questions with cue prompts that addressed the acceptability and perceived value of each material, as a recruitment tool. A brief survey (ie, eight items for the video and seven items for the profiles and Q&A, respectively) was administered to assess the degree to which the material content conceptually aligned with the Model of Culture Centric Health Promotion. 35 This model asserts that health‐related messages are most effective when they are grounded from within a culture member's view (Figure 2). Survey items (Table 3) were rated on a five‐point scale with higher ratings indicating a more positive impression of the material. Focus groups viewed up to three recruitment materials, provided feedback independently, and then reported out within a facilitated group discussion (that was audio‐recorded) about the materials. Content analysis of the focus groups led to recommendations for further editing the set of materials (Table 4).
FIGURE 2.
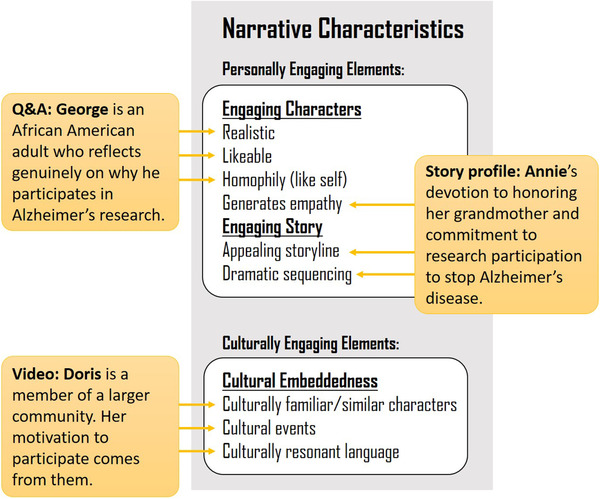
Example story material applications to the Larkey & Hecht 35 culture‐centric model
TABLE 4.
Focus group survey responses by story type and persona
| Annie (n = 19) | Carl (n = 24) | |||
|---|---|---|---|---|
| Profile | M | SD | M | SD |
| The story is interesting | 4.7 | 0.5 | 4.6 | 0.9 |
| The persona seemed realistic | 4.7 | 0.6 | 4.6 | 0.7 |
| The persona was unlikeable* | 1.6 | 1.1 | 1.8 | 1.4 |
| The story said something important to me | 4.6 | 0.5 | 4.5 | 0.7 |
| The story is convincing | 4.8 | 0.5 | 4.6 | 0.6 |
| The story is confusing* | 1.5 | 1.1 | 1.3 | 0.8 |
| I did not like the story* | 2.0 | 1.5 | 2.2 | 1.7 |
| Doris (n = 23) | Paul (n = 25) | |||
|---|---|---|---|---|
| Video | M | SD | M | SD |
| The video is appealing | 4.2 | 1.1 | 4.7 | 0.7 |
| The main persona seemed realistic | 4.4 | 0.9 | 4.9 | 0.3 |
| The main persona was unlikeable* | 1.7 | 1.3 | 1.8 | 1.3 |
| The story was interesting to me | 4.5 | 0.9 | 4.6 | 0.7 |
| The video said something important to me | 4.3 | 1.2 | 4.6 | 0.6 |
| The video is convincing | 4.1 | 1.3 | 4.6 | 0.6 |
| The video is confusing* | 1.7 | 1.1 | 1.6 | 1.2 |
| I did not like the video* | 2.3 | 1.5 | 1.7 | 1.2 |
| Sylvia (n = 17) | George (n = 19) | |||
|---|---|---|---|---|
| Q&A | M | SD | M | SD |
| The Q&A is interesting | 4.4 | 0.7 | 4.5 | 1.0 |
| The answers provided seemed realistic | 4.2 | 0.8 | 4.7 | 0.6 |
| The Q&A said something important to me | 4.2 | 0.8 | 4.6 | 0.8 |
| The Q&A is convincing | 3.8 | 1.3 | 4.6 | 0.6 |
| The Q&A is confusing* | 2.2 | 1.4 | 1.6 | 1.4 |
| I did not like the Q&A* | 2.7 | 1.6 | 1.8 | 1.7 |
Item scales ranged from one (strongly disagree) to five (strongly agree).
Note this item's value is reversed.
3. RESULTS
3.1. Focus group survey results
Survey results (shown in Table 4) from the focus groups demonstrated the participant profile format to be most interesting whereas video and Q&A were perceived as equally interesting or appealing.
3.1.1. Profiles
Profiles represent informational narratives that provide information about the research participant's (i.e., persona) perspective on ADRD research. The focus groups evaluated male and female versions for each profile. Table 4 highlights the main findings from the evaluation of the profile materials for two personas “Annie” and “Carl.” The evaluations for the profiles were very similar for both Annie and Carl and did not appear to display sex‐specific differences. However, Carl did appear slightly more likeable with regard to his persona and his story.
3.1.2. Videos
Focus groups viewed videos for the personas of “Doris” and “Paul” that were approximately 2 minutes in length. The videos in general were well received by the focus groups and had a positive impact. Paul's video was deemed slightly more likeable from the focus group. His persona was also more realistic and less confusing than Doris's. Paul's video also came through as “saying something more important” to the participants and being more convincing than Doris's.
3.1.3. Q&A data
Q&A responses were packaged into an interview of a potential AD researcher with an AD research participant for the personas of “Sylvia” and “George.” The Q&A data (Table 4) were generally deemed “interesting,” “realistic,” and “said something important” for both Sylvia and George. However, George was deemed as saying things of more importance than Sylvia. There was a larger difference between the two personas when it came to how convincing, confusing, and likeable they were. George's Q&A was more convincing and less confusing than Sylvia's. Ultimately, George's Q&A was more likeable than Sylvia's.
3.2. Focus group evaluations
FrameWorks provided an evaluation of focus group discussions and generated messaging recommendations (Table S1 in supporting information), which are discussed below. It should be noted that there were general findings across the various formats (participant profile, video, or Q&A), and then specific feedback given to each persona within each format.
3.2.1. Evaluation of persona profiles and Q&A
Finding 1: Focus groups respond differently to communications featuring men in comparison to those featuring women.
From the discussions and survey results (Table 4) it was clear that focus groups had more positive responses overall to the male personas in comparison to the female personas. For example, focus groups openly commended males for their participation in AD research arguing that it made the research more inclusive and was calming. On the contrary, the materials from the female personas were met with more skepticism and the inclusion of women into AD research was not mentioned.
Finding 2: Focus groups expressed uncertainty about “targeting” African American/Black adults.
The double‐edged sword of inclusion versus targeting also arose in discussions with the focus groups; albeit not with these direct terms. The focus groups felt that while it was clear African American/Black older adults were the focus of this research, it was unclear why they should be targets for this research.
Finding 3: Older adults and caregivers are seen as possible audiences for the promotional materials, and therefore, participants suggested promotional materials be shared on and off of social media.
The focus groups were consistent and clear on the targeted audience for these materials: older adults at risk for AD and their potential caregivers or loved ones. Their suggestions about dissemination of these materials to reach these target audiences included for example, providing materials to Elks clubs and churches highly attended by older adults.
3.2.2. Evaluation of video materials
Focus groups had overall positive feedback and response to the videos for both “Paul” and “Doris.” These videos challenged focus groups to think in new ways about AD and about participation in research. Similar to the profile and Q&A print materials, the focus groups believed the videos to be targeted to the older African American/Black adult population. Focus groups acknowledged two clear goals that arose from watching the videos: (1) increase research participation in AD among African American/Black adults and (2) educate everyone about AD. Because of the focus on African American/Black adults in these videos, there were concerns about patient privacy and lack of trust in medical professionals that are well‐recognized barriers in AD research participation for this population. Thus, the groups discussed the “need for African American communities to have more information" about research and to have a better understanding of “what is expected of research participants.” Throughout and at the conclusion of the focus group, many individuals wanted to know where to find out more specific information about aspects of AD or about participating in AD research.
3.3. Final storytelling materials
Focus group evaluations (Table S1) along with messaging recommendations from FrameWorks Institute were used to generate final example profile materials shared in Figure S1 in supporting information for “Sylvia,” example Q&A materials (Figure S2 in supporting information) for “George,” and research videos for “Doris” (Data S1 and S2 in supporting information) edited for different lengths (i.e., 2 minutes or 45 seconds). Major factors that were helpful in finalizing these materials are discussed below.
4. DISCUSSION
This work details a framework which the ADRD and other research communities can use to capture authentic narratives from ADRD research participants and their study partners and use these stories to generate culturally informed recruitment materials. Overall, a multi‐step iterative approach was used to conduct semi‐structured interviews, theme generation, focus groups, and material development and feedback. This iterative process resulted in the generation of recruitment materials in the form of profiles, videos, and Q&A for male and female personas (representative of the ADRD research participants) that will serve as the basis for a narrative campaign to be evaluated in the RIDE study. Generally, the focus groups felt the personas created were realistic and likeable and that they were convincing in encouraging the target audience of older African American/Black adults to participate in ADRD research. Thus, these stories and this study's goals are in direct alignment with those of the ADRD research community. 10 , 11 Below we highlight important aspects of the study design strategy to serve as best practices and recommendations for others interested in developing storytelling materials for ADRD research.
AD research is unique as most studies require a study partner who serves the role of accompanying the participant to visits, providing information about the participant, and assisting the participant in meeting the research requirements. 36 , 37 Information from study partners was collected so we could capture the study partner perspective and incorporate these findings into the developed stories. Individuals with early AD who are interested in participating in research often do not become research participants because they do not have access to a person who they feel comfortable imposing on in terms of time and effort to serve in the role of a study partner. Thus, an important goal of the recruitment products we produced was in the recruitment of family members (ie, the most common study partners). 36 , 37
Similar to many other focus groups and community‐dwelling African American/Black adults, there is a level of mistrust about research participation. This mistrust has a long history and can contribute to feelings of being targeted without proper justification from African American/Black adults in the community. 10 , 38 The focus groups thus provided important feedback at an early stage of development in our communication materials. This feedback was used to balance authenticity of the exact language in the collected stories to promote understandability of the stories. Initially, we were reticent to diverge from the exact words used by interviewees to capture real stories and provide positive inspiration to others. However, when members of the focus groups had trouble discerning the point of a story, editing of the stories became necessary to ensure understandability by a broad audience. Focus group feedback was also important for creating messaging that was believable to the targeted audiences. This notion became important in the video messaging for “Doris.” Focus group participants believed that “Doris” looked too perfect to be cognitively impaired (see Data S1 or S2). Guidance from communication experts, however, suggested we opt to leave “Doris” as‐is to help with our team's mission to change the perspective that the public has about what early AD looks like. Much of the research we recruit subjects for is aimed at enrolling patients with early AD so presenting early AD patients who look “normal” should help with recruitment. Focus groups also provided very positive feedback about showcasing men to encourage more male enrollment in research. This could be impacted by unconscious gender bias, which has been previously reported across disciplines and research participants. 39 , 40 Finally, focus groups had uniform dislike of products that had a lot of uninterrupted text and thus our final materials use a mix of images, text, bullet points, and graphics to convey our message about research participation.
An important component of our design strategy for producing new storytelling materials to increase recruitment of African American/Black participants into ADRD research was to partner with experts in developing and testing communication strategies aimed at creating social change. Our partnership with FrameWorks Institute was key with regard to providing expertise on how to frame our stories to move our target audiences to take action and get involved (www.frameworksinstitute.org). The cognitive and social scientists at FrameWorks have a 20‐year history of communication expertise aimed at creating social change and this was not an area of expertise of the clinicians, neuroscientists, and social workers within the ADRC. For example, we wanted to use the power of storytelling to engage the public in the topic of ADRD research. FrameWorks helped us to tell a “thematic” story in which an individual becomes part of a community of people working together to accomplish social change 41 , 42 as opposed to just an individual story. This approach was used in creating the video of “Doris” by telling her story but also having her connect to the larger community who will benefit from AD research.
“My family and I are planning ahead for the future and participating in the study has provided me with access to important information and expertise. I feel good about that because it's given my husband and daughter some peace of mind. But I also feel good about my participation because what I'm doing will someday help other people—will someday lead to a prevention, or a cure. It may help my loved ones. It may help yours.”
Another important lesson learned through our collaboration with FrameWorks was making sure that the communications materials we were developing did not make African American/Black adults feel “targeted” but rather made them feel “included.” This strategy is evident in how Doris ends her story.
“Here's something I've learned: Alzheimer's and other memory conditions affect every community, every race. For research to benefit everyone, it has to reflect each of us. That means every color, every gender, every ZIP code.”
These broader issues are important for promoting individuals to take action to become a part of social change but are built on more basic communication skills. These skills are critical for effectively conveying a message to a general audience, such as avoiding medical and scientific jargon, using strong explanatory chains to build understanding of the research process, and making data meaningful to non‐experts through the use of social math (see Methods section and www.frameworksinstitute.org). The six narratives developed herein have aimed to counteract the negative perceptions and stereotypes of older adults that are pervasive, 43 , 44 portraying them as vulnerable, impaired, and dependent. 45 Instead we have reframed the older adults in our stories as partners in the fight against AD, by telling stories that emphasize both the collective benefits of research and the personal benefits to the individual. These stories also show the contribution of the protagonists in our stories to society as recently recommended 46 on how to reframe aging.
The recruitment materials (see Figures S1 and S2 and Data S1 and S2) produced are being used in a culturally informed narrative campaign. This includes videos of different lengths being released online and through social media, and use of profile and Q&A materials at recruitment events and at general community events.
The strengths of this study include the diversity of the research team and personnel and focus groups. Additionally, it was a strength to capture multiple narrative stories across male and female older adults, although even more stories would ensure there is a message to speak to everyone in our targeted audience. This approach uses a positive messaging strategy that highlights perceived benefits of participating in research by actual research participants and avoids focusing negative messaging related to known barriers to participation. Negative messages, for example, might focus on a potential participant avoiding a research study due to historical mistrust of medical professionals. While negative messages are authentic and likely common, they generally come from individuals who did not decide to participate in a research study. Future studies could include interviews from community‐dwelling individuals who have explicitly declined to participate in research studies to better understand barriers to research participation and to identify the type of positive messaging needed to engage these individuals. The semi‐structured interviews conducted herein allowed for participants to share negative perceptions or experiences about research and/or AD; however, a positive messaging strategy provides better opportunity to engage future potential research participants. A notable limitation of this study is that captured stories reflect some cultural and regional specificity from Western Pennsylvania that may not be directly translatable to other African American/Black adults from other geographic regions. Additionally, because our participants self‐identified as African American or Black this limits our ability to generalize these particular stories to all subpopulations of Black individuals such as those from Afro‐Caribbean or other immigrant backgrounds. Other subpopulations based on sexual preference, education, and income status could be beneficial to capture additional narratives in future semi‐structured interviews. Similar subpopulation diversity adequately powered in larger focus group sizes would also allow survey results and discussion to be evaluated on the basis of variables such as sex, socioeconomic status, and education as well as other social or environmental factors. Finally, this study focused exclusively on African American/Black adults and thus other focus groups and semi‐structured interviews would need to be conducted on other subpopulations to be culturally relevant to others.
5. CONCLUSIONS
This is among the first of studies designed to create a rational framework for using culturally relevant narratives to develop a testable and replicable set of tools for recruitment of African American/Black adults into ADRD research. This is a unique approach compared to conventional ones that leverage community engagement through interviews and focus groups and include an iterative feedback process to generate mixed media products. We created a mechanism by which other ADRCs can easily incorporate narratives into existing materials and can develop new materials tailored for their specific communities. Capturing the narratives of African American/Black research participants is critical to developing culturally relevant materials for broader dissemination and is essential to advancing beyond information‐only recruitment approaches, which tend to rely disproportionately on negative messages.
CONFLICTS OF INTERESTS
The authors have no conflicts to report.
Supporting information
Supporting Figure S1
Supporting Figure S2
Supporting Figure S3
Supporting Information
Supporting Information 1
Supporting Video S1
Supporting Video S1
ACKNOWLEDGMENTS
This work was supported by the National Institutes of Health, National Institute on Aging R01AG054518 and P50AG005133. The authors would like to acknowledge the staff of the FrameWorks Institute for their assistance and contribution to video coding and recommendations for video development.
Robinson RAS, Williams IC, Cameron JL, et al. Framework for creating storytelling materials to promote African American/Black adult enrollment in research on Alzheimer's disease and related disorders. Alzheimer's Dement. 2020;6:e12076 10.1002/trc2.12076
REFERENCES
- 1. Petersen RC, Aisen PS, Beckett LA, Donohue MC, Gamst AC, Harvey DJ, et al. Alzheimer's Disease Neuroimaging Initiative (ADNI): clinical characterization. Neurology. 2010;74:201‐209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Tsuang D, Simpson KL, Li G, Barnhart RL, Edland SD, Bowen J, et al. Evaluation of selection bias in an incident‐based dementia autopsy case series. Alzheimer Dis Assoc Disord. 2005;19:67‐73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Demirovic J, Prineas R, Loewenstein D, Bean J, Duara R, Sevush S, et al. Prevalence of dementia in three ethnic groups: the South Florida program on aging and health. Ann Epidemiol. 2003;13:472‐478. [DOI] [PubMed] [Google Scholar]
- 4. Potter GG, Plassman BL, Burke JR, Kabeto MU, Langa KM, Llewellyn DJ, et al. Cognitive performance and informant reports in the diagnosis of cognitive impairment and dementia in African Americans and whites. Alzheimers Dement. 2009;5:445‐453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Griffith PA LO. Disparities in the diagnosis and treatment of Alzheimer's disease in African American and Hispanic patients: a call to action. Generations. 2009;33:37‐46. [Google Scholar]
- 6. Hernandez S, McClendon MJ, Zhou XH, Sachs M, Lerner AJ. Pharmacological treatment of Alzheimer's disease: effect of race and demographic variables. J Alzheimers Dis. 2010;19:665‐672. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Lerner AJ, McClendon MJ, Sami SA, Ogrocki PK, Adams KB, Smyth KA. Factors affecting usage patterns of memantine in Alzheimer disease. Alzheimer Dis Assoc Disord. 2008;22:137‐143. [DOI] [PubMed] [Google Scholar]
- 8. Mehta KM, Yin M, Resendez C, Yaffe K. Ethnic differences in acetylcholinesterase inhibitor use for Alzheimer disease. Neurology. 2005;65:159‐162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Kelley AS, McGarry K, Gorges R, Skinner JS. The burden of health care costs for patients with dementia in the last 5 years of life. Ann Intern Med. 2015;163:729‐736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Barnes LL, Bennett DA. Alzheimer's disease in African Americans: risk factors and challenges for the future. Health Aff (Millwood). 2014;33:580‐586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Gilmore‐Bykovskyi AL, Jin Y, Gleason C, et al. Recruitment and retention of underrepresented populations in Alzheimer's disease research: a systematic review. Alzheimers Dement (N Y). 2019;5:751‐770. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Burns D, Soward AC, Skelly AH, Leeman J, Carlson J. Effective recruitment and retention strategies for older members of rural minorities. Diabetes Educ. 2008;34:1045‐1052. [DOI] [PubMed] [Google Scholar]
- 13. Bushy A. Conducting culturally competent rural nursing research. Annu Rev Nurs Res. 2008;26:221‐236. [PubMed] [Google Scholar]
- 14. Besser L, Kukull W, Knopman DS, et al. Version 3 of the national Alzheimer's coordinating center's uniform data set. Alzheimer Dis Assoc Disord. 2018;32:351‐358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Besser LM, Kukull WA, Teylan MA, et al. The revised national Alzheimer's coordinating center's neuropathology form‐available data and new analyses. J Neuropathol Exp Neurol. 2018;77:717‐726. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Doody RS, Thomas RG, Farlow M, et al. Phase 3 trials of solanezumab for mild‐to‐moderate Alzheimer's disease. N Engl J Med. 2014;370:311‐321. [DOI] [PubMed] [Google Scholar]
- 17. Kim YC, Moran MB, Wilkin HA, Ball‐Rokeach SJ. Integrated connection to neighborhood storytelling network, education, and chronic disease knowledge among African Americans and Latinos in Los Angeles. J Health Commun. 2011;16:393‐415. [DOI] [PubMed] [Google Scholar]
- 18. Utz SW, Williams IC, Jones R, et al. Culturally tailored intervention for rural African Americans with type 2 diabetes. Diabetes Educ. 2008;34:854‐865. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Williams IC, Utz SW, Hinton I, Yan G, Jones R, Reid K. Enhancing diabetes self‐care among rural African Americans with diabetes: results of a two‐year culturally tailored intervention. Diabetes Educ. 2014;40:231‐239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Williams IC, Utz SW, Jones R, Hinton I, Steeves R, Alexander G. Recruitment of rural African Americans for research projects: lessons learned. South Online J Nurs Res. 2011;11:8. [PMC free article] [PubMed] [Google Scholar]
- 21. Houston TK, Allison JJ, Sussman M, et al. Culturally appropriate storytelling to improve blood pressure: a randomized trial. Ann Intern Med. 2011;154:77‐84. [DOI] [PubMed] [Google Scholar]
- 22. Grandbois DM, Sanders GF. Resilience and stereotyping: the experiences of native American elders. J Transcult Nurs. 2012;23:389‐396. [DOI] [PubMed] [Google Scholar]
- 23. Njeru JW, Patten CA, Hanza MM, et al. Stories for change: development of a diabetes digital storytelling intervention for refugees and immigrants to minnesota using qualitative methods. BMC Public Health. 2015;15:1311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Affonso DD, Shibuya JY, Frueh BC. Talk‐story: perspectives of children, parents, and community leaders on community violence in rural Hawaii. Public Health Nurs. 2007;24:400‐408. [DOI] [PubMed] [Google Scholar]
- 25. Banks J. Storytelling to access social context and advance health equity research. Prev Med. 2012;55:394‐397. [DOI] [PubMed] [Google Scholar]
- 26. Grassley JS, Nelms TP. Tales of resistance and other emancipatory functions of storytelling. J Adv Nurs. 2009;65:2447‐2453. [DOI] [PubMed] [Google Scholar]
- 27. McDonald DD, Goncalves PH, Almario VE, et al. Assisting women to learn myocardial infarction symptoms. Public Health Nurs. 2006;23:216‐223. [DOI] [PubMed] [Google Scholar]
- 28. Yang LL. The life stories of motherhood among divorced women in Taiwan. J Nurs Res. 2008;16:220‐230. [DOI] [PubMed] [Google Scholar]
- 29. Schulz AJ, Kannan S, Dvonch JT, et al. Social and physical environments and disparities in risk for cardiovascular disease: the healthy environments partnership conceptual model. Environ Health Perspect. 2005;113:1817‐1825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Guest G, Bunce A, Johnson L. How many interviews are enough? An experiment with data saturation and variability. Field Methods. 2006;18:59‐82. [Google Scholar]
- 31. Lingler JH, Parker LS, DeKosky ST, Schulz R. Caregivers as subjects of clinical drug trials: a review of human subjects protection practices in published studies of Alzheimer's disease pharmacotherapies. IRB: Ethics & Human Research. 2006;28:11‐18. [PubMed] [Google Scholar]
- 32. Sandelowski M. Sample size in qualitative research. Res Nurs Health. 1995;18:179‐183. [DOI] [PubMed] [Google Scholar]
- 33. Nasreddine ZS, Phillips NA, Bedirian V, et al. The Montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53:695‐699. [DOI] [PubMed] [Google Scholar]
- 34. Krueger RA, Designing and conducting focus group interviews. Contract. 2002; No.: 2.
- 35. Larkey LK, Hecht M. A model of effects of narrative as culture‐centric health promotion. J Health Commun. 2010;15:114‐135. [DOI] [PubMed] [Google Scholar]
- 36. Black BS, Taylor HA, Rabins PV, Karlawish J. Study partners perform essential tasks in dementia research and can experience burdens and benefits in this role. Dementia. 2018;17:494‐514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Grill JD, Raman R, Ernstrom K, Aisen P, Karlawish J. Effect of study partner on the conduct of Alzheimer disease clinical trials. Neurology. 2013;80:282‐288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Williams MM, Scharff DP, Mathews KJ, et al. Barriers and facilitators of African American participation in Alzheimer disease biomarker research. Alzheimer Dis Assoc Disord. 2010;24(Suppl):S24‐S29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Holdcroft A. Gender bias in research: how does it affect evidence based medicine?. J R Soc Med. 2007;100:2‐3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Mazure CM, Jones DP. Twenty years and still counting: including women as participants and studying sex and gender in biomedical research. BMC Womens Health. 2015;15:94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Bales SN, Gilliam FD, Jr . Communications for Social Good, Practice Matters: The Improving Philanthropy Project The Foundation Center; 2004. [Google Scholar]
- 42. Iyengar S, Kinder DR. News that Matters: Television and American Opinion. Chicago: University of Chicago Press; 1987. [Google Scholar]
- 43. McConatha JT, Schnell F, McKenna A. Description of older adults as depicted in magazine advertisements. Psychol Rep. 1999;85:1051‐1056. [DOI] [PubMed] [Google Scholar]
- 44. Palmore E. Three decades of research on ageism. Generations. 2005;3:87‐90. [Google Scholar]
- 45. Adams‐Price CE, Morse LW. Dependency stereotypes and aging: the implications for getting and giving help in later life. J. Appl. Soc. Psychol.. 2009;39:2967‐2984. [Google Scholar]
- 46. Busso DS, Volmert A, Kendall‐Taylor N. Reframing aging: effect of a short‐term framing intervention on implicit measures of age bias. J Gerontol B Psychol Sci Soc Sci. 2019;74:559‐564. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting Figure S1
Supporting Figure S2
Supporting Figure S3
Supporting Information
Supporting Information 1
Supporting Video S1
Supporting Video S1