

Abstract
Purpose:
To describe the experience of tele-consultations addressed at the centre of excellence of a multi-tier ophthalmology hospital network in India during the ongoing novel coronavirus (COVID-19) lockdown.
Methods:
This cross-sectional hospital-based study included 7,008 tele-consultations presenting between March 23rd and April 19th 2020. A three-level protocol was implemented to triage the calls. The data of patient queries were collected using a Google Form/Sheets and the tele-calls were returned using the patient information retrieved from the electronic medical record system.
Results:
Overall, 7,008 tele-calls were addressed, of which 2,805 (40.02%) patients where a clinical-related query was answered were included for analysis. The most common queries were related to redness/pain/watering/blurring of vision (31.52%), closely followed by usage of medications (31.05%). The majority of the queries were directed to the department of cornea (34.15%), followed by retina (24.74%). Less than one-fifth of the patients were from the lower socio-economic class (16.08%) and one-fourth were new patients (23.96%). The most common advice given to the patient was related to management of medications (54.15%) followed by appointment related (17.79%). Emergency requests requiring further evaluation by an ophthalmologist accounted for a small percentage (16.36%) of patients.
Conclusion:
Tracking of tele-consultations and access to patient information from the electronic medical records enabled a timely response in an ongoing lockdown due to the COVID-19 pandemic. The current experience provided valuable insights to the possibility of managing patient follow-up visits remotely in the future.
Keywords: COVID-19, electronic medical records, India, tele-consultation
The world is at the “eye of the storm” grappling with the challenges posed by the novel coronavirus (COVID-19) which has spread rapidly across different geographies.[1] The pace of the spread of the viral cases prompted nationwide lockdowns promoting “social distancing” in the population with the hope to flatten the curve.[2] India went into a lockdown from March 23rd 2020 with little time to spare posing unique challenges to adapt for institutions providing eye care.[3] Due to the non-emergent nature of ocular disorders in a significant proportion of the presenting cases, clinical care was reduced to the provision of emergency services. Being accessible to the patients who had clinical related queries to provide the right information is of paramount importance. An emergency response involves assessment of local capacity, prioritizing interventions, establishing strategy, identifying resources, collection and tracking of data and regular monitoring.[4] The current emergency created by the ongoing COVID-19 pandemic globally is at an unprecedented level, leaving many around the world trying to find solutions to the evolving challenges. An estimated 2.6 billion people on the planet are in some form of lockdown and it is expected to take its toll on people both physically and psychologically.[5] Lack of information about the status of next visit or the need to clarify a clinical related query can cause undue stress to the patients in this time of crisis in a high volume setting. The establishment of a protocol to be accessible to the patients to offer care is the need of the hour, especially in this unexpected situation of lack of access to the same. In this current context, the authors wish to present the experience of addressing clinical queries of a large cohort of patients through tele-consultations at the centre of excellence of a multi-tier ophthalmology network in India during the unique scenario of the ongoing COVID-19 lockdown.
Methods
Study design, period, location and approval
This cross-sectional observational hospital-based study included tele-consultations of patients addressed between March 23rd and April 19th 2020 to the centre of excellence of a multi-tier ophthalmology network located in India.[6] The patient or the parents or guardians of the patient called the designated landline numbers of the hospital.[7] None of the identifiable parameters of the patient information were used for analysis of the data. The study adhered to the Declaration of Helsinki and was approved by the Institutional Ethics Committee. The clinical data of the patient was retrieved from a browser-based electronic medical records system (eyeSmart EMR) implemented across the network.[8]
Tele-consultation protocol
A total of 7,008 tele-consultations were addressed at the centre of excellence during the study period. The phone calls as per protocol were triaged into three levels as described in Fig. 1. Level 1 involved resolution of the call by the tele-counsellor itself; Level 2 involved escalating the patient query to the tele-consult team comprised of ophthalmologists for further evaluation and follow-up; Level 3 involved connecting the patient directly to the treating physician by the tele-counsellor. The information regarding the patient query was entered into a google form as depicted in Fig. 2 and the details of the calls were accessed by the tele-consult team of ophthalmologists through google sheets and returned the calls accordingly through the landline or mobile phone. A video call was performed to gain further clinical information as required. An informed consent on the call was sought from the patient before the final advice was given and a summary of the conversation was then appended by the consulting ophthalmologist to the electronic medical record of the patient to ensure continuity of information post the lockdown period. The prescription of medicines adhered to the telemedicine practice guidelines of India,[9] and the previous medications advice given during the last visit of the follow-up patients was asked to be continued where relevant. The medical report with the ophthalmologist advice was sent to the patient via email or WhatsApp at the completion of the call in PDF format. All the tele-consultations were provided at no cost to the patient. A standard list of frequently answered questions was provided to the tele-callers which is detailed in Table 1. A total of 3,738 patients were addressed at Level 1 and 3,270 patients were referred to Level 2 or Level 3 using the triage protocol. Of this subset, 2,805 patient calls which were addressed and completed were included for analysis. The subset of 465 patients where the call was unreachable, call not received or repeat calls by the patient were excluded from the analysis. The tele-consult teams were grouped according to the days of the week akin to a sports league to keep interest levels high. The following teams of Monday Maverick, Tuesday Torpedo, Wednesday Warriors, Thursday Thunderbolt, Friday Fantastics, Saturday Soldiers and Sunday Surfers constituted the Eye Tele-consults League (ETL). A leader board was fashioned inspired by the format of the most popular sport of cricket in India to make it engaging and depicted in Fig. 3. The parameters of Highest Score, Strike Rate (average of the calls), Run Rate (percentage of calls returned), Highest individual score and Total calls as per the day of the week were assessed and shared periodically with the tele-consult team. The study duration was divided into a 4-week period starting from Monday to Sunday from March 23rd to April 19th 2020. Periodic feedback was collected in a subset of the patients by the tele-callers to assess the efficiency of the entire process.
Figure 1.
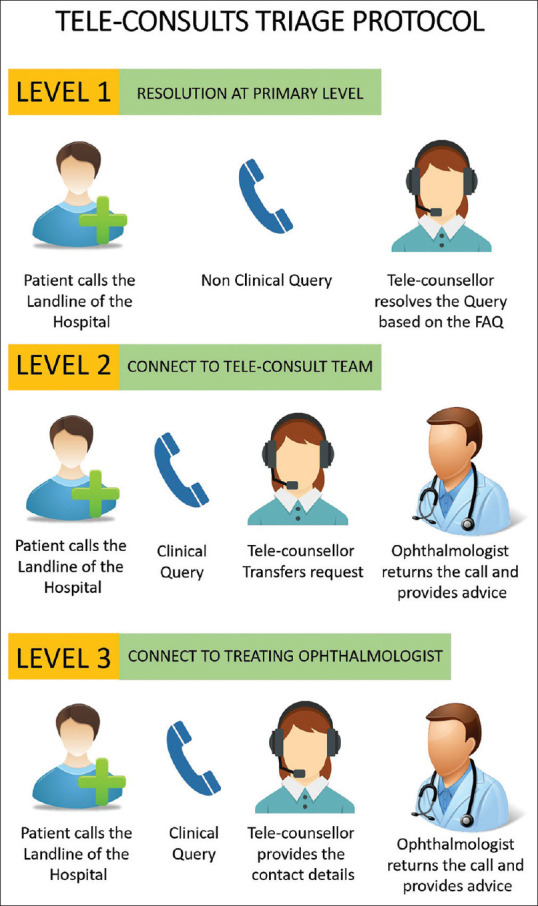
Triage protocol of the tele-consultation calls into 3 levels. Triage performed by the tele-counsellors to the tele-consult team of ophthalmologists
Figure 2.
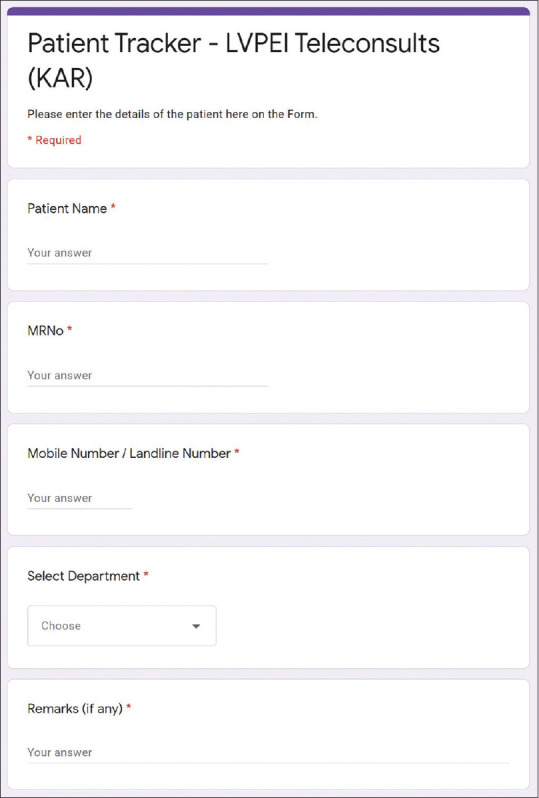
Use of a Google Form to input the information of the tele-calls. The form documented the information of the patient medical record number and contact details with a brief description of the query
Table 1.
Protocol followed by tele-callers to address the queries of the patients
| Patient Query | Tele-counsellor Answer |
|---|---|
| I have an appointment, what shall I do now? | Due to coronavirus situation and based on the government instructions and for your safety, we are dealing with only emergencies. We will call you back and reschedule your appointment when the situation stabilizes. We are noting down your medical record number. |
| When will the situation improve? | We do not know at this point of time. We will call you back when the situation is stabilized, do call the landline numbers in case you have any symptoms or need medical advice. |
| I was scheduled to have surgery? What shall I do? | Due to coronavirus situation and based on the government instructions for your safety, we are dealing with only emergencies. We will call you back and reschedule your surgery when the situation stabilizes. We will note down your medical record number and do reach out in case you have any symptoms or need medical advice. |
| I am having a problem in my eye and I want to talk to my treating doctor | Please indicate the name of your treating ophthalmologist. We are providing you the number of the doctor. You can call or message your doctor between 8 am and 5 pm. |
| I am having a problem in my eye and I want to talk to any available doctor | We are passing on the call to an ophthalmologist in our tele-consultation team. They will reach out to you shortly. |
| I have a problem that might need further evaluation. What should I do? | We are passing on the call to an ophthalmologist in our tele-consultation team. They will guide you whether you need to come to the hospital for a detailed evaluation. |
| When will the Hospital open again? | We do not know at this point in time. We will call you back when the situation stabilizes based on the government guidelines. |
| I have already booked my train/bus/airline ticket. Do I cancel or reschedule the same? | At this point of time, we are not sure of the final date when the lock down will be lifted. It is best to follow the guidelines of the government for the latest information and plan accordingly. You can always reach out to us on the landline numbers for further information on the availability of the clinical services. |
| Can I continue my treatment till my next appointment? | We will transfer your call to speak to an ophthalmologist in our tele-consultation team. They will guide your accordingly after they review your medical records. |
Figure 3.
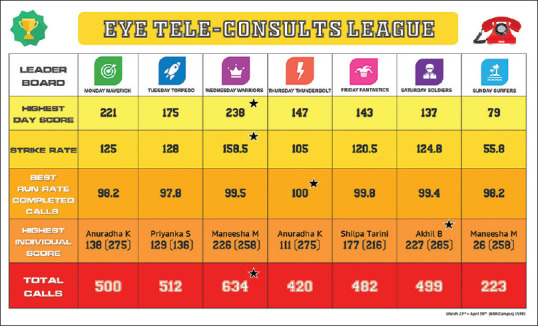
Leader board of the Eye Tele-consults League (ETL). The teams were grouped into 7 teams as per the day of the week and the performance parameters were shared akin to a sports league dashboard
Data retrieval and processing
The electronic medical records data of 2,805 patients included in this study and google sheets information of the tele-consultations were segregated in a single excel sheet. The columns included the data on demographics, clinical presentation, ocular diagnosis, query and advice given which were exported for analysis. The excel sheet with the required data was then used for analysis using the appropriate statistical software. Standardized definitions were used for occupation, socio-economic status and geographic categorization.[10]
Statistical analysis
Descriptive statistics using mean ± standard deviation and median with inter-quartile range (IQR) were used to elucidate the demographic data using Microsoft Excel 2019 (Microsoft Corporation, Redmond, USA).
Results
Demographics
Among the 2,805 patients whose clinical queries were addressed by tele-consultations, 2,133 patients were follow-up patients (76.04%) and 672 patients were new (23.96%). Among the follow-up patients, the mean age of the patients was 40.79 ± 22.86 years, while the median age was 44 (IQR: 24–59) years. There were 1340 (62.82%) male and 793 (37.18%) female patients. There were 813 (38.12%) patients from rural districts, 715 (33.52%) from urban districts, and 605 (28.36%) from metropolitan regions. There were 547 (25.64%) patients from the lower socio-economic class, 1490 (69.85%) from the lower middle class, 57 (2.67%) from the upper middle class and 39 (1.83%) from the upper class. There were 922 (43.23%) patients with a recent (≤2 months) surgical history. The follow-up patients called from 18 states of India and the most common state was Telangana with 1484 (69.57%), followed by Andhra Pradesh with 315 (14.77%) patients.
Patient query
Of the 2,805 patients, 884 (31.52%) were related to symptoms of redness/pain/watering/blurred vision; 871 (31.05%) were medication queries; 432 (15.40%) wanted to speak with the treating ophthalmologist; 317 (11.30%) cited an emergency to visit the hospital for an evaluation; 173 (6.17%) were appointment related; 108 (3.85%) were short follow-up and in a small subset of 20 (0.71%) patients reported sudden loss of vision.
Ocular subspecialty
Of the 2,805 patients, 958 (34.15%) were addressed by the subspecialty of Cornea and anterior segment; 694 (24.74%) were Retina; 414 (14.76%) were Glaucoma; 225 (8.02%) were Paediatric Ophthalmology; 212 (7.56%) were Oculoplasty, 197 (7.02%) were Cataract; 64 (2.28%) were Refractive surgery, and 41 (1.46%) were related to Uvea.
Ophthalmologist advice
Of the 2,805 patients, 1,519 (54.15%) were medication related of which 774 (27.59%) were asked to continue/taper the medications, 525 (18.72%) were prescribed new medications, 131 (4.67%) were asked to stop the medications and 89 (3.17%) were prescribed an alternative medication which was most commonly an unavailable brand of anti-glaucoma medication. 499 (17.79%) were given an appointment at a later date; 459 (16.36%) were asked to come to the emergency for further evaluation and management; 147 (5.24%) were asked to review locally; 91 (3.24%) were directed to the treating ophthalmologist for a final opinion; 73 (2.60%) were related to fixing a surgical appointment. In a small subset of 17 (0.61%) additional reports were shared by the patient for review to assist in providing the advice by the ophthalmologist.
Weekly overview
In the 4 week period, the answered calls steadily increased in number from 573 (20.43%) in week 1, 591 (21.07%) in week 2, 701 (24.99%) in week 3 and 940 (33.51%) in week 4. The busiest day of the week was Wednesday with 634 (19.38%) calls. There was increasing trend seen in calls from new patients (19.02%; week 1 to 27.02%; week 4) and a decreasing trend seen in calls from lower socio-economic strata patients (18.50%; week 1 to 14.47%; week 4). A description of the various patient categories and the trend over the 4 weeks is detailed in Fig. 4.
Figure 4.
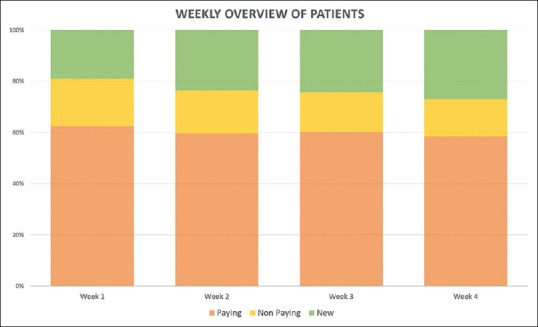
Trend of patient categories among the calls over 4 weeks. There was increasing trend seen in calls from new patients (19.02%; week 1 to 27.02%; week 4) and a decreasing trend seen in calls from lower socio-economic patients (18.50%; week 1 to 14.47%; week 4)
Patient feedback
Of the feedback received in a subset of 280 patients, 184 (65.71%) patients mentioned they could reach us on the first attempt itself and 84 (30%) within 2 attempts. The majority of the calls were returned back within 1 hour of the primary call in 224 patients (80%). A significant proportion of 251 (89.24%) patients indicated that their issue was addressed completely, 258 (92.14%) mentioned they had clarity about their next appointment and a small subset of 18 (6.43%) patients had to call back for further information.
Discussion
This study sought to describe the experience of tele-consultations addressed at the centre of excellence of a multi-tier ophthalmology hospital network in India during the ongoing novel coronavirus (COVID-19) lockdown. The findings of this study suggest that the majority of the patient queries were related to symptoms of redness/pain/watering/blurred vision in the eyes and the most common advice was related to medications being used by the patients. Three fourth of the calls were made by follow-up patients. A small percentage of patients were asked to visit the emergency of the hospital for further evaluation and management. The significant proportion of the patient belonged to the subspecialty of cornea and anterior segment followed by retina. Triage protocols and access to the electronic medical records of the patients enabled the tele-consultation team to handle a large volume of call efficiently during the lockdown period in India.
There has been a steep rise in the shift towards the use of telemedicine platforms because of the social distancing and lockdowns implemented across various countries around the world. However, there is limited literature on the usage of such telemedicine systems and various specialties like radiology[11], psychiatry[12], obstetrics[13], palliative medicine[14] and dermatology[15] have described their experience during the ongoing COVID-19 pandemic. The Ministry of Health and Family Welfare, Government of India had released a set of Telemedicine guidelines during the beginning of the lockdown period.[9] Our study reports the management of the patient eye care remotely with the use of tele-consultations to ensure continuity of care in the absence of a physical visit to the hospital and the rapid implementation of the protocols to ensure information access to the patients during the lockdown. We have also found an increasing trend of new patients calling us as the lockdown progressed and a small decline in calls from lower socio-economic strata patients, which probably can be explained by the decrease in the surgical procedures performed in this group due to the lockdown. Also, only one-fourth of the follow up patients who called were females. We are also understanding the barriers to access in this subset of patients and looking to addressing this gap in the future. Our patients reached out from all parts of the country and the feedback collected in a majority of them was positive.
The use of electronic medical record systems cannot be overemphasized as the access to the right information about the patient records is crucial for the right advice. The lack of EMR in a majority of the institutions leads to dependence on the patient providing the reports to the consulting doctor via an electronic media such as email or WhatsApp. This modality is intensive on the provision of data by the patient and results in an asynchronous advice dependent on the availability of reports. This is in stark contrast to the real time resolution of the patient query with the availability of the electronic medical records. The rapid modifications made to the EMR systems has been described in an academic setting of screening protocols, system level EMR templates, emergency department tracking, reporting and analytics, integrated communication channels and development of patient facing interfaces.[16] This reinforces the benefits of having digital systems to adapt quickly to times, such as the COVID-19 crisis and adapt quickly to continue to deliver patient care services.
Tele-Ophthalmology has great promise in providing care to patients remotely through the use of digital infrastructure using electronic medical records. The authors have already described their experience to use this modality in their multi-tier network for the rural vision centres consults through the development of the eyeSmart App to collect information[17], share clinical pictures for ophthalmologist opinion[18] and transmission of real time slit lamp video from their vision centres.[19] There is potential to explore the same for managing follow up patients coming from distant regions to the tertiary care centres through tele-ophthalmology and integrating this into the patient care services of the organization in near future. The possibility to integrate with elderly follow-up care for the geriatric patients presenting to our network supported by portable diagnostic equipment is being explored as well. The relevance and feasibility of the evaluation of the new patients with the available technology tools such as apps for visual acuity, colour vision and extraocular movements and smart phone pictures needs to be validated. Many of the clinical examination techniques performed in the ophthalmology clinic cannot be substituted with apps for the same unless scientifically proven to give similar results. Hence, these technology tools must be used with caution after prior evaluation and must not be substituted for a thorough clinical ophthalmic examination.
Globally, there is a call to action to critically evaluate the potential of the telemedicine system to be integrated into the delivery of patient care. There do exist challenges like establishment of national guidelines, funding frameworks, clinical guidelines and defining context, training of healthcare providers, increasing uptake among the population, secure data sharing mechanisms and scientific research to evaluate the impact.[20] However, the need to explore the use of digital systems to reach patients in times of crisis has seen an unprecedented rise during the ongoing COVID-19 pandemic and a serious foray into this might prove beneficial for healthcare institutions in the future.
Conclusion
In conclusion, this study aimed to describe the experience of tele-consultations addressed at the center of excellence of a multi-tier ophthalmology hospital network in India. Tracking of tele-consultations and access to patient information from the electronic medical records enabled a timely response in an ongoing lockdown due to the COVID-19 pandemic. The current experience provided valuable insights to the possibility of managing patient follow-up visits remotely in the future through the evolving technology of tele-ophthalmology and its possible applications to reach the population at large to provide eye-care services.
Financial support and sponsorship
Hyderabad Eye Institute, Hyderabad, India.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
The authors wish to acknowledge the amazing support of all the tele-callers, administrators and ophthalmologists who are working tirelessly to address the queries of our patients during the COVID-19 lockdown. The authors also wish to thank the Department of eyeSmart EMR & AEye team specially Mr. Ranganath Vadapalli and Mr. Mohammad Pasha.
References
- 1.Dong E, Du H, Gardner L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect Dis. 2020;20:533–4. doi: 10.1016/S1473-3099(20)30120-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Wilder-Smith A, Freedman DO. Isolation, quarantine, social distancing and community containment: Pivotal role for old-style public health measures in the novel coronavirus (2019-nCoV) outbreak. J Travel Med. 2020;27:taaa020. doi: 10.1093/jtm/taaa020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Prime Minister India [Internet]. c2020. [Last cited on 2020 Apr 19]. Available from: https://wwwpmindiagovin/en/news_updates/pm-calls-for-complete-lockdown-of-entire-nation-for-21-days/
- 4.B Wisner, J Adams., editors. Wisner, Ben, Adams, John & World Health Organization. (2002) Environmental health in emergencies and disasters: A practical guide. World Health Organization; https://apps.who.int/iris/handle/10665/42561 . [Google Scholar]
- 5.World Economic Forum [Internet]. c2020. Available from: https://wwwweforumorg/agenda/2020/04/this-is-the-psychological-side-of-the-covid-19-pandemic-that-were-ignoring/ Last cited on 2020 Apr 19.
- 6.Rao GN, Khanna RC, Athota SM, Rajshekar V, Rani PK. Integrated model of primary and secondary eye care for underserved rural areas: The L V Prasad Eye Institute experience. Indian J Ophthalmol. 2012;60:396–400. doi: 10.4103/0301-4738.100533. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.LV Prasad Eye Institute [Internet]. c2020. Available from: https://wwwlvpeiorg/contact-us/contact-hyderabad . Last cited on 2020 Apr 19.
- 8.Das AV, Kammari P, Vadapalli R, Basu S. Big data and the eyeSmart electronic medical record system-An 8-year experience from a three-tier eye care network in India. Indian J Ophthalmol. 2020;68:427–32. doi: 10.4103/ijo.IJO_710_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ministry of Health and Family Welfare, Government of India [Internet] Telemedicine Practice Guidelines. c2020. [Last cited on 2020 Apr 19]. Available from: https://www.mohfw.gov.in/pdf/Telemedicine.pdf .
- 10.Das AV, Podila S, Prashanthi GS, Basu S. Clinical profile of pterygium in patients seeking eye care in India: Electronic medical records-driven big data analytics report III. Int Ophthalmol. 2020 doi: 10.1007/s10792-020-01326-3. doi: 101007/s10792-020-01326-3. [DOI] [PubMed] [Google Scholar]
- 11.Sanei Taheri M, Falahati F, Radpour A, Karimi V, Sedaghat A, Karimi MA. Role of social media and telemedicine in diagnosis & management of COVID-19; An experience of the Iranian Society of Radiology. Arch Iran Med. 2020;23:285–6. doi: 10.34172/aim.2020.15. [DOI] [PubMed] [Google Scholar]
- 12.Liu S, Yang L, Zhang C, Xiang YT, Liu Z, Hu S, et al. Online mental health services in China during the COVID-19 outbreak. Lancet Psychiatry. 2020;7:e17–8. doi: 10.1016/S2215-0366(20)30077-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Dashraath P, Wong JL, Lim MX, Lim LM, Li S, Biswas A, et al. Coronavirus disease 2019 (COVID-19) pandemic and pregnancy. Am J Obstet Gynecol. 2020 doi: 10.1016/j.ajog.2020.03.021. S0002-9378(20)30343-4. doi: 101016/jajog202003021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Humphreys J, Schoenherr L, Elia G, Saks NT, Brown C, Barbour S, et al. Rapid implementation of inpatient telepalliative medicine consultations during COVID-19 pandemic. J Pain Symptom Manage. 2020 doi: 10.1016/j.jpainsymman.2020.04.001. S0885-3924(20)30195-0. doi: 101016/jjpainsymman 202004001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Jakhar D, Kau S, Kaur I. WhatsApp messenger as a teledermatology tool during coronavirus disease (COVID-19): From bedside to phone-side. Clin Exp Dermatol. 2020 doi: 10.1111/ced.14227. doi: 101111/ced14227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Reeves JJ, Hollandsworth HM, Torriani FJ, Taplitz R, Abeles S, Tai-Seale M, et al. Rapid response to COVID-19: Health informatics support for outbreak management in an academic health system. J Am Med Inform Assoc. doi: 10.1093/jamia/ocaa037. 2020. ocaa037 doi: 101093/jamia/ocaa037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kammari P, Ambadker MC, Loomba A, Deepthi N, M Shravani, Vadapalli R, et al. A novel technology tool to capture the clinical information of patients across rural vision centers in a three-tier eye care network in India using the eyeSmart EMR App. Rural Remote Health. 2019;19:5255. doi: 10.22605/RRH5255. [DOI] [PubMed] [Google Scholar]
- 18.Das AV, Mididoddi S, Kammari P, Deepthi Davara N, Loomba A, Khanna R, et al. App-based tele ophthalmology: A novel method of rural eye care delivery connecting tertiary eye care center and vision centers in India. Int J Telemed Appl. 2019;2019:8107064. doi: 10.1155/2019/8107064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Loomba A, Vempati S, Davara N, Shravani M, Kammari P, Taneja M, et al. Use of a tablet attachment in teleophthalmology for real-time video transmission from rural vision centers in a three-tier eye care network in India: EyeSmart Cyclops? Int J Telemed Appl. 2019;2019:5683085. doi: 10.1155/2019/5683085. doi: 10.1155/2019/5683085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Ohannessian R, Duong TA, Odone A. Global telemedicine implementation and integration within health systems to fight the COVID-19 pandemic: A call to action. JMIR Public Health Surveill. 2020;6:e18810. doi: 10.2196/18810. [DOI] [PMC free article] [PubMed] [Google Scholar]