

To the Editor: Kasabach-Merritt syndrome (KMS) is a very rare life-threatening aggressive vascular tumor that is related to Kaposiform hemangioendothelioma and tufted angioma. It is characterized by thrombocytopenia and intravascular coagulation that occasionally develops into disseminated intravascular coagulation.[1,2] A rare incidence of diffuse infiltrative pancreatic hemangioma with a high possibility of missed diagnosis of KMS makes it a fatal disease. Here, we described a case diagnosed with diffuse infiltrative hemangioma (DIH) of pancreas accompanied by KMS and provided ultrasonic data for early and accurate diagnosis, and successful treatment experiences with sirolimus.
A 1.5-month-old male infant was admitted because of scleral icterus and jaundice all over his body. The laboratory test showed that the infant had anemia, thrombocytopenia, coagulopathy, and abnormal liver function. Clinical examination showed that his skin color was dark yellow with some apparent petechiae. Abdominal ultrasound scan revealed: (1) the liver was enlarged by 3.3 cm; (2) common bile duct was dilated; and (3) the pancreas showed diffuse swelling with inhomogeneous rough echogenicity, heterogeneous intra-parenchymal texture and abundant vessels [Figure 1A]. These results were further confirmed by enhanced computed tomography (CT), which also revealed the whole pancreas was diffuse swelling with abundant vessels. Therefore, DIH of pancreas accompanied by KMS was diagnosed.
Figure 1.
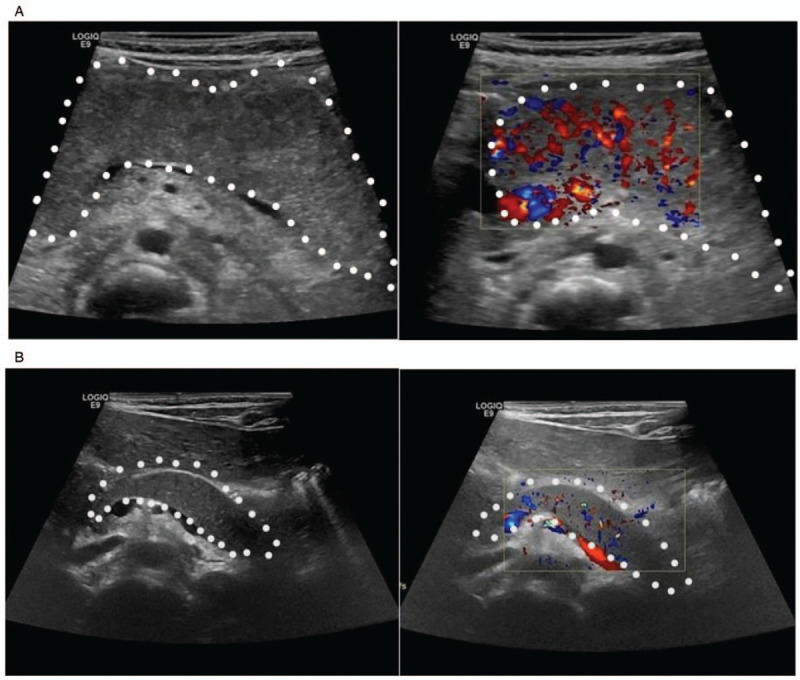
The findings of ultrasound scan in patients with DIH of pancreas accompanied by KMS. (A) Abdominal ultrasounds scan revealed a diffuse swelling and heterogeneous intra-parenchymal texture in the pancreas (left); color Doppler ultrasound scan showed abundant blood flow in the affected pancreas (right). (B) After 1-year treatment with sirolimus, the size of affected pancreas basically returned to normal (left), and the blood flow in the affected pancreas was significantly decreased (right). The affected pancreas is indicated in the dotted line. DIH: Diffuse infiltrative hemangioma; KMS: Kasabach-Merritt syndrome.
The infant was first treated empirically with prednisone (1 mg/kg, intravenously). However, after 1 week of treatment, there was no obvious improvement in the size of his pancreas as well as his coagulation status. Additionally, his platelet count decreased to 3 × 109/L, with no sign of bleeding. Then, his therapeutic regimen was changed to sirolimus therapy. After 1-month of treatment with sirolimus, his jaundice and some petechiae were significantly subsided. Both his indices of blood coagulability and his liver function returned to normal. However, his platelet count was still decreased. After treatment with sirolimus for 4 months, his platelet count returned to normal; whereas abdominal ultrasound scan showed no significant changes in pancreas size, morphology, and blood flow signals within the pancreas. The pancreas internal echo became slightly finer and more homogeneous. After one more year treatment with sirolimus, the laboratory tests of the infant returned to normal and there was no recurrence of thrombocytopenia. A repeat abdominal ultrasound scan showed his affected pancreas basically returned to normal size and blood flow in the pancreas significantly reduced [Figure 1B]. These results were further confirmed by enhanced CT scans. During the 2-year treatment with sirolimus, no side effects were observed. Till now, the infant is still receiving the sirolimus maintenance treatment.
The lesions of KMS are typically cutaneous and solitary hemangioma and rarely occur in visceral organs and bone.[1,3–5] It has been reported that more than 80% of KMS occurred in the first year after birth. Here, the onset age of our reported case was 1.5 months after birth.
Hemangioma that occurs in the pancreas is very rare. Due to its rarity, internal organ location and no special clinical manifestation, it is hard to diagnose. Even if highly suspected, pathologic biopsy cannot be performed considering the serious clinical status of the infant or the specific location of a tumor (eg, the pancreas) that may lead to high tendency of bleeding. Although CT and magnetic resonance imaging are well established to evaluate the pancreatic lesions, there are still some shortcomings. By contrast, ultrasound scan shows its advantages, including its portability, low levels of radiation and its applicability to critically ill patients who could not receive other examinations. Importantly, ultrasound can not only clearly show the size, shape, internal echo of the pancreas but also the changes of blood flow signals inside the pancreas. Thus, ultrasound is considered to be a preferential tool when conducting preliminary screening of the pancreatic hemangioma accompanied by KMS.
There is no standard guideline for treating large hemangiomas accompanied by KMS. Sirolimus has shown excellent prospects for the treatment of hemangioma accompanied by KMS.[2,5] After 1-year treatment with sirolimus, the infant in this study showed stable vital signs, with all laboratory indicators as well as his pancreas size returning to normal. Therefore, sirolimus is effective in the treatment of hemangioma with KMS, but further prospective trials are needed to assess the efficacy of this drug and to determine the scientific therapeutic dose and duration of treatment.
Conclusively, we reported a very rare case of DIH of pancreas accompanied by KMS. In this case, we adopted ultrasound for early diagnosis. This is the first case that was diagnosed with ultrasound. Sirolimus was used for early treatment and good therapeutic efficacy was achieved. Thus, when ultrasound scan reveals diffuse swelling of the pancreas and abundant blood flow signals, with the combination of abnormal hematologic parameters, pancreatic diffuse hemangioma accompanied by KMS should be considered. Additionally, ultrasound is a preferential tool for definite diagnosis of patients with DIH of pancreas accompanied by KMS (especially in infant) as well as a simple tool for prolonged follow-up.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient's guardians have given their consent for the patient's images and other clinical information to be reported in the article. The patient's guardians understand that their names and initials will not be published and due efforts will be made to conceal the identity of the patient, although anonymity cannot be guaranteed.
Funding
This study was supported by a grant from the Medical and Health Science and Technology Development Project of Shandong Province (No. 2018WS261).
Conflicts of interest
None.
Footnotes
How to cite this article: Zhang WH, Luo FQ, Wang H. Diffuse infiltrative hemangioma of pancreas accompanied by Kasabach-Merritt syndrome: a case report. Chin Med J 2020;133:2263–2265. doi: 10.1097/CM9.0000000000001037
References
- 1.Liu FS, Zou MX, Zheng BW, Wang XB, Lyu GH, Li J. A report on kaposiform hemangioendothelioma of the cervical spine. Chin Med J 2019; 132:1378–1380. doi: 10.1097/CM9.0000000000000217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mariani LG, Schmitt IR, Garcia CD, Kiszewski AE. Lowdose sirolimus treatment for refractory tufted angioma and congenital kaposiform hemangioendothelioma, both with Kasabach-Merritt phenomenon. Pediatr Blood Cancer 2019; 66:e27810.doi: 10.1002/pbc.27810. [DOI] [PubMed] [Google Scholar]
- 3.Boccara O, Fraitag S, Lasne D, et al. Kaposiform haemangioendothelioma-spectrum lesions with Kasabach-Merritt phenomenon: retrospective analysis and long-term outcome. Acta Derm Venereol 2016; 96:77–81. doi: 10.2340/00015555-2185. [DOI] [PubMed] [Google Scholar]
- 4.Schulz AS, Urban J, Gessler P, Behnisch W, Kohne E, Heymer B. Anaemia, thrombocytopenia and coagulopathy due to occult diffuse infantile haemangiomatosis of spleen and pancreas. Eur J Pediatr 1999; 158:379–383. doi: 10.1007/s004310051096. [DOI] [PubMed] [Google Scholar]
- 5.Liu Y, Wu X, Ye L, Xu H. Successful treatment of a patient with Kasabach–Merritt syndrome and multiple giant hepatic hemangiomas. J Int Med Res 2020; 48:300060519898358.doi: 10.1177/0300060519898358. [DOI] [PMC free article] [PubMed] [Google Scholar]