

Abstract
Background Care-management tools are typically utilized for chronic disease management. Sonoma County government agencies employed advanced health information technologies, artificial intelligence (AI), and interagency process improvements to help transform health and health care for socially disadvantaged groups and other displaced individuals.
Objectives The objective of this case report is to describe how an integrated data hub and care-management solution streamlined care coordination of government services during a time of community-wide crisis.
Methods This innovative application of care-management tools created a bridge between social and clinical determinants of health and used a three-step approach—access, collaboration, and innovation. The program Accessing Coordinated Care to Empower Self Sufficiency Sonoma was established to identify and match the most vulnerable residents with services to improve their well-being. Sonoma County created an Interdepartmental Multidisciplinary Team to deploy coordinated cross-departmental services (e.g., health and human services, housing services, probation) to support individuals experiencing housing insecurity. Implementation of a data integration hub (DIH) and care management and coordination system (CMCS) enabled integration of siloed data and services into a unified view of citizen status, identification of clinical and social determinants of health from structured and unstructured sources, and algorithms to match clients across systems.
Results The integrated toolset helped 77 at-risk individuals in crisis through coordinated care plans and access to services in a time of need. Two case examples illustrate the specific care and services provided individuals with complex needs after the 2017 Sonoma County wildfires.
Conclusion Unique application of a care-management solution transformed health and health care for individuals fleeing from their homes and socially disadvantaged groups displaced by the Sonoma County wildfires. Future directions include expanding the DIH and CMCS to neighboring counties to coordinate care regionally. Such solutions might enable innovative care-management solutions across a variety of public, private, and nonprofit services.
Keywords: artificial intelligence, data integration hub, process improvement, care coordination, emergency care
Background and Significance
Lack of affordable housing, mental illness, substance abuse, and natural disasters have contributed to a growing homelessness crisis in California, estimated at 38 per 10,000 people in 2019, or twice the national average of 17 per 10,000 people. 1 According to the 2019 Point in Time Homeless Count, Sonoma County was among the top three suburban counties with 60 homeless per 10,000 people and has the highest per capita homeless in the United States. 1 Sonoma County is largely a rural region with a diverse population of approximately 500,000, and exhibits significant disparities in health outcomes, living standards, and educational attainment. 2 State and local government agencies that serve the homeless are faced with increasing demand for services as well as budgetary, organizational, and legislative constraints. Typically, agencies are separately funded and staffed, and they operate in “silos of service” with limited interagency integration. 3 Recent disasters have demonstrated the importance of strengthening government organizational systems to help communities respond to naturally occurring threats through the evolving field of emergency management. 4
Recognizing a lack of agency integration as a barrier to support vulnerable citizens, Sonoma County, California implemented a cross-program care coordination tool within their safety net system in early 2017. Sonoma County sought to design and deliver coordinated service for individuals experiencing one or more complex needs, including unemployment, housing insecurity, homelessness, behavioral health issues, substance abuse, and incarceration. The County's siloed departments (e.g., Health Services, Human Services, Housing Services, Child Support Services, Probation, and others relating to criminal justice) collaborated through advanced care-management tools to decrease care fragmentation for shared clients; reduce duplication of services; and create an effective, efficient care management plan. 5 6 Sonoma County's aim was to improve the health, well-being, and self-sufficiency of clients; increase access and referrals to services; grow sustained client engagement; improve communication between care managers; and decrease expenditures per client/family through improved efficiencies.
During implementation, the Sonoma County Complex fires hit, burning more than 36,000 acres, killing 22 people, and destroying 5,636 homes and buildings. 7 Sonoma County is challenged by a high cost-of-living, limited housing, and a homeless crisis exacerbated by the 2017 fires. The need for safety net services intensified during the wildfire response and continued throughout the long recovery process. In the aftermath of the wildfires, many vulnerable citizens were already living in shelters and required ongoing shelter, while others displaced from their homes required shelter and were faced with dwindling supply.
Objectives
This case report describes the system implemented, workflow changes, and impact on vulnerable citizens to inform the field of informatics about lessons learned from this innovative application of care-management tools.
Methods
Sonoma County created the Accessing Coordinated Care to Empower Self Sufficiency (ACCESS) Initiative to achieve their objectives of access, collaboration, and innovation for the most vulnerable residents by matching them with services to help improve their well-being and resilience. The determination of whether an individual is vulnerable is a hybrid approach comprised of agency interviews, a risk assessment, the ascertainment that the person has urgent needs, or an external event, such as a wildfire or tornado, that triggers a dramatic increased need for assistance. The ACCESS Initiative consists of the Interdepartmental Multidisciplinary Team (IMDT) approach to generate and deploy coordinated cross-departmental services for addressing housing insecurity needs and to inform technology strategy and development. Care management by the IMDT had a community-wide perspective and participation by community partners to decrease fragmentation of care across community clinics, regional hospitals, and social service providers. The formation of the IMDT was achieved over several months through a series of meetings to discuss interdepartmental processes. Memorandums between agency department heads were established, which included agreements for data sharing in a manner that was consistent with their department's policies. ACCESS governance was implemented by a Safety Net Collaborative Steering Committee, who regularly reviewed system and data needs, uses, and privacy.
IBM implemented a data integration hub (DIH) and care management and coordination system (CMCS) for Sonoma County in 90 days. The DIH, IBM Connect 360, working with IBM InfoSphere Master Data Management, brought together data from a variety of sources using proprietary and highly accurate probabilistic matching and search algorithms, and created a single, integrated, current master data index resulting in a “golden record” for every individual. In the center of Fig. 1 , the “single view of the individual” is the result of the process of ingesting EMR and social determinants of health data to provide a holistic view of the individual from the multitude of structured and unstructured sources on the right side of the diagram. More than 91,000 resident records were loaded into the DIH from four sources (CalWIN for eligibility operations, SWITS for drug and alcohol dependency, Avatar for mental health, and IJS for proprietary justice data). Depending upon the agency, the frequency that data feeds are refreshed ranges from every 15 minutes to daily. The research team conducted a validation of the “golden records” prior to the system being put into operation. The DIH allowed secure exchange of client data, which could be stored on-premise or on the IBM cloud, across existing systems.
Fig. 1.
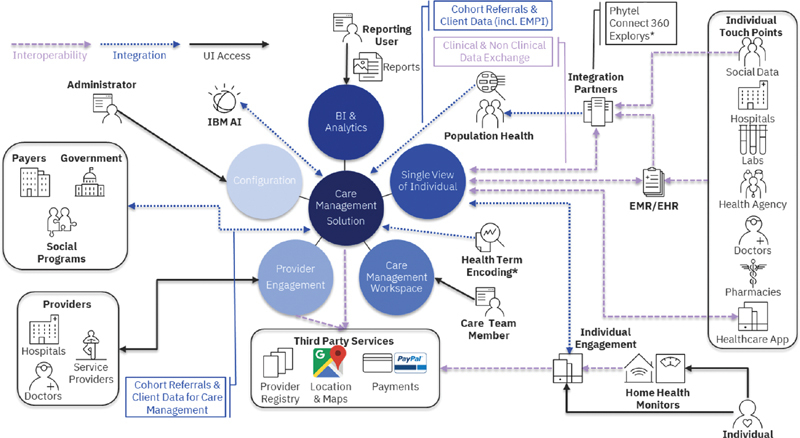
IBM Connect 360 and Watson Care Manager Solution Ecosystem.
The CMCS, IBM Watson Care Manager (WCM), was built on a Health Insurance Portability and Accountability Act (HIPAA)-enabled, cloud-based platform that can aggregate data and connected agencies, payers, and community service providers, to support the design, coordination, and delivery of individualized services. Using multidisciplinary teams, case managers, social workers, and treatment providers optimized workflow for activities such as scheduling, developing individualized care plans, managing budgets, selecting providers, and enabling care for an individual's mental health, physical health, and social service needs. The CMCS applied best practices through structured programs built in alignment with evidence-based medicine, quality standards, and regulatory requirements. The CMCS's artificial intelligence (AI) component can automatically extract and surface social determinants of health and clinical health terms in large volumes of care management notes. 5 8
The integrated IBM Connect 360 and WCM solution is available on tablets, laptops, or mobile devices and offers interoperability with third-party services including PayPal for provider/service payments, provider registry and accreditation, and Google for maps and location, although these third-party services were not deployed in Sonoma County. Analytics and business intelligence are used to identify cohorts and trends and to send and receive alerts and notifications. The CMCS allowed the IMDT to create and manage a new fire-displaced cohort, perform assessments, record case notes, set care plans, and match client needs with community providers.
Results
More than 4,000 fire victims were initially housed in shelters. Two weeks after the disaster, approximately 300 individuals did not have secure housing. Of 127 individuals representing 95 households that remained in shelters, approximately 42% were identified as precariously housed and approximately 26% were homeless prior to the fires. Over the 10-month period from April 2018 to February 2019, the IMDT and care managers identified and managed 77 clients (median age 54.5 years, [29–84], female [58%]) with multidimensional, complex needs (34 cases stable and intermittently monitored, and 43 actively managed). These 77 fire-displaced, homeless individuals required intensive case management and exhibited much higher utilization of MediCal (99 vs. 80%) and rates of mental illness (97 vs. 67%), medical conditions (82 vs. 28%), substance abuse (60 vs. 47%), and emergency room utilization (17 vs. 10%) than the other clients (more than 1,000) served by ACCESS Sonoma. Applications for food stamps, Section 8 housing, and Medi-Cal for these complex individuals were prepared and thoroughly reviewed by IMDT, reducing the burden on multiple staff. The average number of times IMDT formally discussed cases was 2.9.
The IMDT's goal is to help clients progress toward self-sufficiency by providing care coordination to support them in behavioral health treatment, employment and income security, suitable and stable housing, food security, substance use treatment, physical health services, disability management, and reduced recidivism. Client needs are elucidated by the case worker during an encounter, while performing assessments, and via data viewed in the system about assessments and case notes. County residents who are eligible for services must “opt-in”; however, not all of them chose to engage in services. Every client who “opts-in” is monitored. Clients may be monitored less frequently, or cases may be closed due to a client stabilizing, being rehoused, engaging with other collaborative care providers, or an inability to establish or maintain contact.
Two clients, Sandy and Martin (pseudonyms), faced difficulty accessing and navigating multiple service programs. Sandy, a 69-year-old woman with chronic obstructive pulmonary disease and living on a very modest income has a son with substance abuse issues who threatened her, so she sought refuge in Sonoma County. The trauma of being homeless and abused led to behavioral health challenges that went untreated. She often visited the emergency room (ER).
After the 2017 wildfires, Sandy arrived at a homeless shelter to avoid smoke. Two weeks later, the Federal Emergency Management Agency began to close the shelters. Sandy was among approximately 300 individuals and families with unmet needs and no place to go. A mental health caseworker quickly realized Sandy needed a higher level of care and asked permission to share her vital information, thereby allowing the IMDT to coordinate appropriate services (e.g., Medi-Cal, food stamps, Section 8 Housing). Sandy's bank statements revealed she was paying for multiple insurance policies. Eliminating one policy by having Medi-Cal pay for her Medicare insurance provided Sandy with additional income. IMDT workers connected Sandy with a health care provider who addressed her chronic pain, subsequently ending the need for ER visits, and resulting in significant cost savings. Sandy is healthier now than before the fires. Through care coordination, Sandy was able to obtain health insurance, financial assistance, housing, and mental health services and support.
Martin is a 50-year-old man, who has been homeless for more than 10 years, with physical and behavioral health needs. Staying in Guerneville, California and a high utilizer of health services, Martin is out-of-work, has been in and out of jail several times, and started living on the streets after his wife's death. Due to increasing behavioral health and substance-abuse issues, Martin ended up in crisis stabilization services ten times. The IMDT established contact with Martin at a shelter in September 2018. He received rehabilitation services to deal with his addiction and behavioral health issues. In October 2018, Martin became sober for the first time in 10 years. The IMDT helped him find a job, thereby reducing his utilization of economic assistance. In April 2019, Martin moved into permanent housing. Martin is now able to engage in society in a functioning manner since he received the needed services.
These case examples illustrate how Connect360 and Watson Care Manager improved operational efficiency and interdepartmental teamwork, and how successful coordinated care may improve citizen outcomes. Prior to deployment of the CMCS, the IMDT took approximately 4 hours to discuss and provide status updates for approximately 10 homeless people on their housing placements, financial assistance from the state, and health care services. In comparison, after the solution's deployment, the IMDT took approximately 4 hours to discuss and provide updates for approximately 30 to 45 homeless people depending upon the complexity of their cases. Additionally, the CMCS empowered the IMDT to redirect homeless people out of the ER, connect them with suitable insurance, establish care plans, and match them to appropriate health care services more quickly. Benefits realized included reduced duplication of services, increased use of cost-effective treatment, decreased overall expenditures (ER visits), increased awareness of services and programs offered by other departments, and reduced recidivism.
Discussion
Care-management solutions are typically developed for the treatment of chronic illnesses in the ambulatory setting. 9 10 11 This case report describes how an innovative application of a care-management solution helped care management workers transform safety net services, social well-being, and health care for disadvantaged groups displaced by a natural disaster. Key functionalities were integration of siloed data and services, AI to surface social determinants of health and clinical health terms from structured and unstructured sources, matching of clients with services, and a unified view of citizen status that supported coordinated care. The cases of Martin and Sandy illustrate how Sonoma County employed the system to establish stability with respect to behavioral and physical health and associated social circumstances. The case report generated hypotheses for future research studies to examine actual or forecasted expenses, cost avoidance, and health outcomes for cohorts (e.g., fire-displaced, mentally ill) and assess usability. In 2019, the Kincade fire hit more than 75,000 acres in and near Sonoma County with evacuations estimated at 180,000 residents. 12 The potential exists for improving integrated collaborative networks across the region with incorporation of data and services from surrounding counties. 13 Sandy's and Martin's challenges are common to homeless individuals. Using the integrated IBM Connect 360 and WCM solution, governmental services were equipped to serve the most vulnerable residents like Sandy and Martin.
Sonoma County executives, supervisors, and frontline workers from each agency were involved in defining the requirements for the integrated DIH and CMCS system. IMDT members helped to configure the software. These knowledgeable users participated in a half-day training session and found the solution to be very intuitive; thus, they were eager to use the system. New users participated in a full-day training session.
Creative collaborations among public, private, and non-for-profit organizations are likely needed to address adequately the homelessness crisis in the United States. Care management tools that can provide integration and collaboration across diverse service providers may enable the needed solutions.
Conclusion
This innovative application of a data hub and AI-enabled care management solution aggregated near real-time data for caseworkers, clinicians, housing specialists, and other community workers who served Sonoma County citizens. Individual users involved in this study reported improved operational efficiency, information transparency, access to coordinated care, and citizen outcomes. Advanced health information technologies can be instrumental in driving collaboration and governmental service access so that residents at risk and experiencing a crisis can be better served in their greatest times of need.
Clinical Relevance Statement
Care management tools are traditionally applied in chronic disease or primary care settings. This case study describes the implementation and value of a care management solution applied to governmental services.
Multiple Choice Questions
1. The study presented here is:
Randomized controlled trial
Meta-analysis
Case study
Case–control study
Correct Answer: The correct answer is option c, case study.
2. Which response below best describes how AI and advanced health information technologies can be transformative in delivering a rapid response system in the event of a natural disaster?
Improved care coordination.
Better information transparency.
Matching and search algorithms for services.
All of the above.
Correct Answer: The correct answer is option d, all of the above.
Funding Statement
Funding None.
Conflict of Interest G.J., W.K., K.K., M.S.-L, D.B., E.S., J.L.S., and K.W. are employees of the IBM Corporation. T.S. was an employee of IBM Corporation at the time of this study and is now retired.
Protection of Human and Animal Subjects
All reported findings in this case review used aggregated community-level data and deidentified case findings, reporting no unique identifiers. This case report has IRB approval or the equivalent ethics committee approval from Sonoma County.
References
- 1.2019 Annual Homeless Assessment Report (AHAR) to Congress, Part 1—PIT Estimates of Homelessness in the US. U.S. Department of Housing and Urban Development. Washington, DC.; 2020 [Google Scholar]
- 2.Robinson B, Staats C. San Francisco, CA: IBM Think Conference 2019; 2019. Access Sonoma: Enabling Multi-discipline Teams to Deliver Safety Net Services to County Residents with Complex Needs. [Google Scholar]
- 3.Davidson A J. Creating value: unifying silos into public health business intelligence. EGEMS (Wash DC) 2015;2(04):1172. doi: 10.13063/2327-9214.1172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Rose D A, Murthy S, Brooks J, Bryant J.The evolution of public health emergency management as a field of practice Am J Public Health 2017107(S2):S126–S133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lopez V, Mccarthy G, Bettencourt-Silva J. Using semantic technologies to extract highlights from care notes. Stud Health Technol Inform. 2017;245:1331. [PubMed] [Google Scholar]
- 6.Patterson Silver Wolf D A. The new social work. J Evid Inf Soc Work. 2018;15(06):695–706. doi: 10.1080/23761407.2018.1521321. [DOI] [PubMed] [Google Scholar]
- 7.Index-Tribune Staff Report. The timeline of the Sonoma Complex fires. Sonoma-Index Tribune 8 Oct. 2018: n.page. Web. 29 Mar. 2020
- 8.Bettencourt-Silva J, Mulligan N, Cullen C, Kotoulas S. Bridging clinical and social determinants of health using unstructured data. Stud Health Technol Inform. 2018;255:70–74. [PubMed] [Google Scholar]
- 9.Hamine S, Gerth-Guyette E, Faulx D, Green B B, Ginsburg A S. Impact of mHealth chronic disease management on treatment adherence and patient outcomes: a systematic review. J Med Internet Res. 2015;17(02):e52. doi: 10.2196/jmir.3951. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Rudin R S, Fanta C H, Qureshi N. A clinically integrated mhealth app and practice model for collecting patient-reported outcomes between visits for asthma patients: Implementation and feasibility. Appl Clin Inform. 2019;10(05):783–793. doi: 10.1055/s-0039-1697597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Harle C A, DiIulio J, Downs S M. Decision-centered design of patient information visualizations to support chronic pain care. Appl Clin Inform. 2019;10(04):719–728. doi: 10.1055/s-0039-1696668. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Christie J.California fire threatens PG&E’s plan to raise $14 billion. Reuters 30 Oct. 2019. Web. 29 Mar. 2020
- 13.Mattox K L. Hurricanes Katrina and Rita: role of individuals and collaborative networks in mobilizing/coordinating societal and professional resources for major disasters. Crit Care. 2006;10(01):205. doi: 10.1186/cc3942. [DOI] [PMC free article] [PubMed] [Google Scholar]