

Abstract
Aim
To assess whether an enhanced category combining suicides with nonsuicide drug self-intoxication fatalities more effectively captures the burden of self-injury mortality (SIM) in the USA among US non-Hispanic black and Hispanic populations and women irrespective of race/ethnicity.
Methods
This observational study used deidentified national mortality data for 2008–2017 from the CDC’s Web-based Injury Statistics Query and Reporting System. SIM comprised suicides by any method and age at death plus estimated nonsuicide drug self-intoxication deaths at age ≥15 years. Measures were crude SIM and suicide rates; SIM-to-suicide rate ratios; and indices of premature mortality.
Results
While the suicide rate increased by 29% for blacks, 36% for Hispanics and 25% for non-Hispanic whites between 2008 and 2017, corresponding SIM rate increases were larger at 109%, 69% and 55% (p<0.0001). SIM:suicide rate ratio gaps were widest among blacks but similar for the other two groups. Gaps were wider for females than males, especially black females whose ratios measured ≥3.71 across the observation period versus <3.00 for white and Hispanic counterparts. Total lost years of life for Hispanic, white and black SIM decedents in 2017 were projected to be 42.6, 37.1 and 32.4, respectively.
Conclusion
Application of SIM exposed substantial excess burdens from substance poisoning relative to suicide for minorities, particularly non-Hispanic blacks and for women generally. Results underscored the need to define, develop, implement and evaluate comprehensive strategies to address common antecedents of self-injurious behaviours.
Keywords: Suicide/Self?Harm, Poisoning, Mental Health, Drugs, Mortality, Cross Sectional Study
Introduction
Actively killing oneself—that is, self-injury mortality (SIM)—involves more than suicide. Suicide—as codified by medical examiners and coroners (ME/Cs) and the US CDC—is an ‘intentional’ manner of death (MOD) as is homicide. It often is viewed as a sentinel event indicative of distressed individuals and distressed communities.1 However, suicide alone as a MOD fails to capture adequately the toll of lives where persons’ actions lead directly to their death. For example, a national, multivariable study found that official suicide rates for non-Hispanic blacks and Hispanics during 2003–2005 were approximately two-fifths of the rates for the majority non-Hispanic white population.2 However, when suicides were pooled with deaths of undetermined intent—the MOD category most susceptible to suicide misclassification3—blacks and Hispanics, respectively, had 2.38 and 1.17 higher odds than whites of being assigned an undetermined classification, despite evidence reflecting immediate (proximal) actions causing their demise.2 A subsequent multilevel (individual and county), multivariable study, which used the enriched restricted access database of the National Violent Death Reporting System (NVDRS), attested to the importance of an authenticated suicide note and psychiatric/psychological history in distinguishing ME/C cases as suicides versus undetermined deaths.4 That study further demonstrated the paucity of such corroborative evidence, a data deficit appearing most consequential for the (mis-)classification of drug and other poisoning suicides, as compared with suicides by gunshot or hanging. However, its authors noted that non-drug poisoning suicides, for example, such as those implicating gases, pesticides and household cleaners, were much rarer than drug poisoning suicides and also that non-drug poisoning tends to be less ambiguous than drug poisoning as a suicide method for ME/Cs. This category also included alcohol poisoning suicides, which could justifiably have been placed in the drug poisoning category.
While suicides have been conventionally used as the sole representative of fatal self-injury, there has been a growing argument that a broader, behaviourally based, working category of SIM would facilitate injury research, prevention and treatment.5 6 SIM has been operationalised as a combination of:
Registered suicides by all methods at all ages.
Estimated drug-associated self-intoxication deaths, where instrumental behaviours of the decedents had proved lethal on the day of death (eg, dying from a fentanyl overdose in the course of using injectable opioids) among persons aged ≥15 years.
SIM arose to address health data disparities in recognition that: (1) suicides are undercounted non-randomly by demographic characteristics, such as sex and race/ethnicity, and method or injury mechanism2 4; (2) psychological autopsies or in-depth investigations of decedent histories of psychiatric disorders or distress are rarely used to inform MOD determination in cases of equivocal intent7–9; (3) regional medicolegal and epidemiological paradigms possess different functions and priorities, with differing implications for suicide and other injury mortality surveillance, aetiological understanding, prevention and treatment10; (4) standards for ME/Cs assigning suicide as the MOD are much more stringent than those governing homicide11 and would require unaffordable investigative resources (as outlined in (2) above); (5) burdens placed on overstressed and under-resourced emergency healthcare12 13 and medicolegal death investigation systems14 15 in affirming drug intoxication suicides, in particular,16 have likely been exacerbated by the Great Recession of 200817 and the opioid and suicide epidemics18–20; (6) ME/Cs use ‘accident’ as a default MOD assignment in the absence of affirmative criteria; (7) governmental coding of the great majority of drug-intoxication deaths as ‘accidents’ mischaracterises what is known regarding the association between recurring drug misuse and drug use disorders with increased rates of suicidal ideation, planning and attempts21–23; and (8) mandated by nationwide statutes, ‘accident’, as a formal MOD category, is unlikely to be modified in the foreseeable future to account for evidentiary, behaviourally based ‘non-suicide’ self-injury deaths.
Prior reports on SIM rate trends and patterns in the US highlighted comparisons with other leading causes of death.5 6 24 Suicide remains the 10th ranked cause of death. However, the SIM rate in 2016 surpassed the mortality rate for diabetes, the seventh leading cause, reflecting the continuing rise in suicide since 2000 and the rapid acceleration of drug-related fatalities.6 In 2014, SIM accounted for an estimated 32 and 37 years of life lost by the male and female decedents, respectively, compared with 16 and 17 years from diabetes.5 Suicide is likely relatively more undercounted for women than men because women tend disproportionately to employ less violent, less forensically obvious methods (eg, drugs vs gunshot or hanging),25 which provides important justification for investigating sex differentials in SIM rates relative to suicide rates.
Buttressing the need for racial/ethnic research on SIM, psychiatric and psychological evidence for suicide corroboration is plausibly rarer for blacks and Hispanics than for whites.26 Consistent with differential healthcare access and suicide accounting, an NVDRS analysis conducted by CDC found that black and Hispanic suicide decedents had fewer reported mental health conditions than white counterparts.27 Their suicides also were accompanied by a lower prevalence of evidentiary suicide notes.4 28 An unanticipated consequence, disparities in access to healthcare and pain management may have decreased overall exposure among black and Hispanic populations to high potency prescription opioids during the early years of the opioid epidemic,29 30 thus attenuating their risk for fatal drug intoxication with prescription opioids. However, as individuals using highly purified heroin and fentanyl analogues have emerged as the primary overdose fatalities, black and Hispanic men and women have experienced increasing related mortality.31
We evaluated two research questions in this national study of racial/ethnic trends and patterns in SIM during the decade 2008–2017. While non-Hispanic white men have been identified as the highest profile risk group for ‘deaths of despair’,32 33 including mortality from suicide, drug intoxication and alcohol-related diseases, does SIM capture relatively more ‘accidental’ and undetermined drug intoxication deaths among non-Hispanic blacks and Hispanics than non-Hispanic whites of both sexes? Is the impact of SIM more pronounced among females than males across all three of the major racial/ethnic groups?
Methods
This cross-sectional, observational study used deidentified manner and underlying cause-of-death data and associated population data from CDC’s Web-based Injury Statistics Query and Reporting System (WISQARS).34 Distinguishing the sexes, and also age for comparing SIM patterns, the study population was confined to non-Hispanic blacks, Hispanics and non-Hispanic whites, who constituted 93% of the US population in 2017. Persons of Asian and Pacific Islander heritage and American Indians and Native Alaskans were excluded from this study due to heterogeneity and instability with small numbers. Following previous practice, SIM was operationalised as a composite of all suicides (International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10) UO3, X60-84, Y 87.0), by any method at any age at death, and 80% of ‘accidental’ (‘unintentional’ under CDC nomenclature) drug deaths (X40-44) and 90% of undetermined drug deaths (Y10-14) among persons aged >15 years.5 6 The ‘accidental’ drug death component was at least sevenfold higher than the undetermined component throughout the observation period, 2008–2017, in each of the racial/ethnic groups under scrutiny. Our SIM formula estimated and removed the small proportion of drug poisoning deaths not attributable to repetitive self-harm behaviours most commonly associated with drug use disorders. The age cutoff ≥15 years for the nonsuicide drug component assumed that purposive self-harm behaviours were rare among preteen and younger teens.
We examined SIM-to-suicide rate ratios to compare the changing relative contributions of suicides and drug intoxication deaths to the overall burden of self-injury fatalities. We also tested and described linear trends in crude SIM and suicide rates by race/ethnicity and sex over the observation period, modelling time as a continuous variable. In order to compare patterns as well as changes in SIM across groups, we then computed age-specific and sex-specific rates for the years 2008 and 2017. Two measures were employed to assess the premature mortality burdens attributable to SIM: cumulative percentage of SIM under age 55 years, and projected years of life lost by SIM decedents (derived from a double decrement life table procedure) based on our predetermined age groups.35 36
This study did not meet the criteria for human research established by the West Virginia University Office of Research Integrity and Compliance, as the mortality and population data were deidentified and obtained from a publicly accessible, secondary database. Thus, no protocol approval was necessary.
Results
A linear test for trend (p<0.0001) showed rising crude SIM and suicide rates across all three racial/ethnic groups between 2008 and 2017, independent of sex (table 1). Due to the large number of deaths annually, the SEs of the rate estimates were small (0.1–0.2 deaths per 100 000 population). SIM rates for whites were almost triple those of Hispanics and more than double those of Blacks throughout most of the observation period, with rate increases accelerating towards the end. Comparing 2017 with 2008, the SIM rate increased 109% for blacks, 69% for Hispanics and 55% for whites. These rate changes generally were similar for both sexes across the three groups. Suicide rates also rose universally, though less for men than women—29% for blacks, 36% for Hispanics and 25% for whites. These increases were markedly smaller than the growth of SIM rates overall, indicating greater contributions from drug fatalities.
Table 1.
Self-Injury mortality (SIM)* and suicide rates per 100 000 population and SIM-to-suicide rate ratios for three racial/ethnic groups by sex, USA, 2008–2017
| Race/ethnicity | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | % change 2008/2017 |
| Both sexes | SIM rate | ||||||||||
| White (non-Hispanic) | 27.9 | 28 3 | 29.5 | 31.0 | 31.2 | 32.4 | 34.1 | 36.6 | 40.5 | 43.3 | 55.1 |
| Black (non-Hispanic) | 12.9 | 12.7 | 12.6 | 13.3 | 13.7 | 14.6 | 15.5 | 17.3 | 22.8 | 26.9 | 109.1 |
| Hispanic | 9.7 | 9.9 | 9.8 | 10.4 | 10.5 | 10.9 | 11.6 | 12.6 | 14.8 | 16.3 | 68.8 |
| Male | |||||||||||
| White (non-Hispanic) | 40.6 | 41.0 | 42.4 | 44.5 | 44.7 | 46.1 | 48.5 | 52.1 | 58.3 | 62.7 | 54.5 |
| Black (non-Hispanic) | 19.6 | 18.9 | 18.6 | 19.7 | 20.2 | 21.8 | 22.8 | 26.0 | 34.3 | 41.2 | 109.6 |
| Hispanic | 15.1 | 15.3 | 14.8 | 15.7 | 15.8 | 16.4 | 17.5 | 19.0 | 22.8 | 25.4 | 68.1 |
| Female | |||||||||||
| White (non-Hispanic) | 15.7 | 16.1 | 16.9 | 18.0 | 18.1 | 19.1 | 20.1 | 21.4 | 23.2 | 24.4 | 55.8 |
| Black (non-Hispanic) | 6.7 | 7.0 | 7.2 | 7.5 | 7.7 | 8.0 | 8.8 | 9.3 | 12.3 | 13.9 | 106.2 |
| Hispanic | 4.0 | 4.4 | 4.7 | 5.0 | 5.1 | 5.3 | 5.6 | 6.0 | 6.6 | 7.0 | 75.1 |
| Both sexes | Suicide rate | ||||||||||
| White (non-Hispanic) | 15.2 | 15.4 | 16.0 | 16.5 | 16.8 | 17.1 | 17.6 | 18.1 | 18.2 | 18.9 | 24.9 |
| Black (non-Hispanic) | 5.3 | 5.2 | 5.3 | 5.5 | 5.7 | 5.6 | 5.6 | 5.8 | 6.3 | 6.9 | 29.2 |
| Hispanic | 4.9 | 5.2 | 5.3 | 5.2 | 5.3 | 5.3 | 5.9 | 5.8 | 6.3 | 6.7 | 36.0 |
| Male | |||||||||||
| White (non-Hispanic) | 24.3 | 24.7 | 25.6 | 26.2 | 26.7 | 26.9 | 27.7 | 28.3 | 28.3 | 29.9 | 23.3 |
| Black (non-Hispanic) | 9.3 | 8.8 | 9.1 | 9.4 | 9.6 | 9.5 | 9.5 | 9.8 | 10.6 | 11.4 | 21.9 |
| Hispanic | 8.0 | 8.5 | 8.5 | 8.5 | 8.5 | 8.3 | 9.2 | 9.1 | 10.1 | 10.7 | 32.6 |
| Female | |||||||||||
| White (non-Hispanic) | 6.3 | 6.5 | 6.7 | 7.0 | 7.2 | 7.5 | 7.9 | 8.3 | 8.3 | 8.2 | 29.8 |
| Black (non-Hispanic) | 1.7 | 1.9 | 1.8 | 1.9 | 2.1 | 2.1 | 2.1 | 2.1 | 2.4 | 2.8 | 64.0 |
| Hispanic | 1.7 | 1.8 | 2.0 | 1.9 | 2.1 | 2.2 | 2.4 | 2.6 | 2.5 | 2.6 | 56.4 |
| Both sexes | SIM: suicide rate ratio | ||||||||||
| White (non-Hispanic) | 1.84 | 1.84 | 1.84 | 1.88 | 1.86 | 1.90 | 1.93 | 2.02 | 2.23 | 2.28 | 23.9 |
| Black (non-Hispanic) | 2.41 | 2.44 | 2.39 | 2.43 | 2.41 | 2.61 | 2.75 | 2.99 | 3.60 | 3.91 | 62.2 |
| Hispanic | 1.97 | 1.90 | 1.86 | 1.99 | 1.96 | 2.06 | 1.98 | 2.15 | 2.33 | 2.44 | 23.9 |
| Male | |||||||||||
| White (non-Hispanic) | 1.67 | 1.66 | 1.65 | 1.70 | 1.68 | 1.71 | 1.75 | 1.84 | 2.06 | 2.09 | 25.1 |
| Black (non-Hispanic) | 2.10 | 2.14 | 2.04 | 2.11 | 2.10 | 2.30 | 2.40 | 2.66 | 3.24 | 3.62 | 72.4 |
| Hispanic | 1.88 | 1.80 | 1.75 | 1.85 | 1.85 | 1.97 | 1.90 | 2.09 | 2.26 | 2.39 | 27.1 |
| Female | |||||||||||
| White (non-Hispanic) | 2.47 | 2.49 | 2.55 | 2.56 | 2.50 | 2.55 | 2.56 | 2.60 | 2.81 | 2.96 | 19.8 |
| Black (non-Hispanic) | 3.98 | 3.72 | 3.94 | 3.88 | 3.71 | 3.88 | 4.18 | 4.38 | 5.01 | 5.00 | 25.6 |
| Hispanic | 2.40 | 2.41 | 2.35 | 2.60 | 2.44 | 2.41 | 2.33 | 2.35 | 2.60 | 2.68 | 11.7 |
*Self-injury mortality (SIM) is a composite of all registered suicides, and estimated nonsuicide deaths from drug self-intoxication at ages 15 years and older.
Reflecting the drug-related deaths whose manner was assigned by ME/Cs as ‘accident’ or undetermined, examination of SIM-to-suicide rate ratios revealed widening gaps between the respective magnitude of the SIM rate and the suicide rate for all three racial/ethnic groups, as a whole and by sex. This widening was especially pronounced for Blacks. The ratios for black females measured 3.71 or higher across the observation period, while those for white and Hispanic females remained under 3.00. The ratios for black males invariably surpassed those of their white and Hispanic counterparts and exceeded 3.00 during 2016 and 2017.
Figure 1 relates respective SIM-to-suicide rate ratios for blacks and Hispanics to the white ratios for the total groups and by sex. Black-to-white ratios steadily increased from 1.29 in 2011 to a high of 1.70 by 2017. By contrast, Hispanic-to-white ratios generally approached parity, ranging from a low of 1.01 in 2010 to a high of 1.09 in 2013. Although patterns of Black-to-white SIM-to-suicide rate ratios for men and women both mirrored the pattern for the combined sexes, ratios were more concentrated and typically higher for women. Hispanic-to-white ratios remained marginally above parity for men throughout the observation period, and marginally below for women 2011 aside. Figure 2 provides direct comparisons between the sexes in the respective magnitude of their SIM-to-suicide rate ratios across race/ethnicity. Black female-to-male SIM-to-suicide rate ratios exceeded those for whites and Hispanics, except in 2017 when approximating the ratio for whites. Ratios trended downwards across all three racial/ethnic groups.
Figure 1.
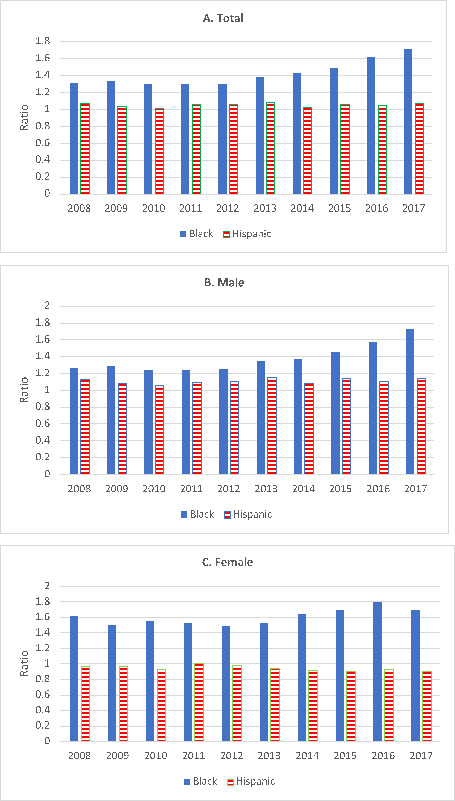
Ratio of minority racial/ethnic group-to-white self-injury mortality-to-suicide rates by sex, USA, 2008–2017.
Figure 2.
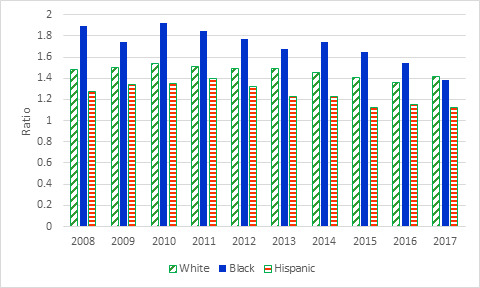
Female-to-male ratio of self-injury mortality-to-suicide rates by race/ethnicity, USA, 2008–2017.
Table 2 presents comparative age-specific and sex-specific SIM rates for 2008 and 2017. Rates were higher in the middle of the age spectrum than at the extremes. They also were substantially higher in 2017. While whites continued to manifest the highest SIM rates, blacks exhibited the largest cross-period changes overall, with increases approaching or exceeding twofold. Age-specific SIM-to-suicide rate ratios were typically larger in 2017 than in 2008 for all racial/ethnic groups. In 2017, SIM rates for blacks were sevenfold, ninefold and fourfold higher than corresponding suicide rates at ages 45–54 years, 55–64 years and 35–44 years, respectively. They were threefold higher for blacks at ages 25–34 years, Hispanics at ages 35–64 years and whites at ages 25–44 years. Reference to the cumulative percentages of SIM deaths showed appreciable transfer of the burden to older middle-age among blacks between 2008 and 2017. In 2008 and 2017, respectively, 85% and 86% of Hispanic SIM deaths occurred within the population 54 years and younger, our first indicator of the premature mortality burden. Corresponding percentages for blacks and whites were lower and showed marked declines.
Table 2.
Patterns and change in self-injury mortality (SIM) by race/ethnicity and age, USA, 2008 versus 2017
| White (non-Hispanic) | Black (non-Hispanic) | Hispanic | ||||||||||||||||
| No. of deaths | Cumulative deaths, % | Rate* | Period change, % | SIM: SRR† | YLL‡ | No. of deaths | Cumulative deaths, % | Rate* | Period change, % | SIM: SRR† |
YLL‡ | No. of deaths | Cumulative deaths, % | Rate* | Period change, % | SIM: SRR† |
YLL‡ | |
| Age, years | 2008 | |||||||||||||||||
| 0–14 | 148 | 0.3 | 0.4 | NA | 1.00 | 35.7 | 30 | 0.6 | 0.3 | NA | 1.00 | 32.2 | 22 | 0.5 | 0.2 | NA | 1.00 | 37.0 |
| 15–24 | 5803 | 10.7 | 22.5 | NA | 1.92 | 35.6 | 610 | 12.8 | 9.3 | NA | 1.22 | 32.1 | 772 | 17.2 | 9.2 | NA | 1.51 | 36.9 |
| 25–34 | 9079 | 27.0 | 38.2 | NA | 2.28 | 32.7 | 826 | 29.4 | 15.6 | NA | 1.68 | 29.7 | 1096 | 40.9 | 13.4 | NA | 1.99 | 34.8 |
| 35–44 | 11 801 | 48.1 | 43.8 | NA | 2.12 | 28.3 | 1112 | 51.8 | 20.6 | NA | 2.84 | 26.3 | 1126 | 65.3 | 16.1 | NA | 2.26 | 32.3 |
| 45–54 | 15 090 | 75.2 | 47.7 | NA | 2.06 | 23.4 | 1423 | 80.3 | 26.6 | NA | 4.38 | 22.4 | 962 | 86.2 | 19.2 | NA | 2.50 | 29.2 |
| 55–64 | 7705 | 89.1 | 29.6 | NA | 1.54 | 17.6 | 694 | 94.3 | 19.6 | NA | 4.31 | 17.4 | 372 | 94.3 | 12.9 | NA | 2.14 | 24.3 |
| 65–74 | 2987 | 94.4 | 18.5 | NA | 1.19 | 13.7 | 191 | 98.1 | 10.0 | NA | 1.95 | 13.5 | 148 | 97.5 | 9.8 | NA | 1.41 | 20.0 |
| 75+ | 3112 | 100 | 18.3 | NA | 1.02 | 13.2 | 94 | 100 | 6.9 | NA | 1.45 | 14.1 | 117 | 100 | 11.3 | NA | 1.19 | 19.5 |
| All | 55 725 | NA | 27.9 | NA | 1.84 | 4980 | NA | 12.9 | NA | 2.41 | 4615 | NA | 9.7 | NA | 1.97 | |||
| 2017 | ||||||||||||||||||
| 0–14 | 328 | 0.4 | 1.0 | 137.1 | 1.00 | 37.2 | 66 | 0.6 | 0.7 | 119.4 | 1.00 | 32.4 | 91 | 0.9 | 0.6 | 265.2 | 1.00 | 42.6 |
| 15–24 | 8011 | 9.6 | 33.6 | 49.3 | 1.97 | 37.0 | 1125 | 10.4 | 17.0 | 83.3 | 1.58 | 32.2 | 1582 | 17.4 | 16.2 | 76.9 | 1.61 | 42.4 |
| 25–34 | 19 001 | 31.4 | 74.1 | 93.7 | 3.34 | 34.4 | 2274 | 30.2 | 35.0 | 123.9 | 2.87 | 30.1 | 2505 | 43.5 | 26.9 | 100.6 | 2.60 | 39.1 |
| 35–44 | 17 324 | 51.3 | 73.6 | 68.1 | 3.01 | 29.2 | 2180 | 49.1 | 40.7 | 97.4 | 4.23 | 26.3 | 2168 | 66.1 | 25.6 | 58.6 | 3.08 | 34.1 |
| 45–54 | 18 030 | 72.0 | 66.6 | 39.6 | 2.48 | 23.8 | 2670 | 72.4 | 49.9 | 87.7 | 6.71 | 22.5 | 1847 | 85.3 | 26.8 | 39.7 | 3.17 | 29.3 |
| 55–64 | 14 692 | 88.9 | 49.2 | 66.0 | 2.05 | 18.3 | 2392 | 93.2 | 48.8 | 149.4 | 9.34 | 18.1 | 966 | 95.3 | 20.5 | 58.9 | 2.94 | 24.1 |
| 65–74 | 5614 | 95.3 | 24.8 | 34.4 | 1.34 | 13.8 | 652 | 98.9 | 22.6 | 125.6 | 4.94 | 13.4 | 296 | 98.4 | 11.6 | 18.2 | 1.85 | 20.0 |
| 75+ | 4065 | 100 | 24.3 | 19.4 | 1.11 | 13.2 | 126 | 100 | 7.1 | 3.8 | 1.80 | 14.1 | 151 | 100 | 9.1 | −19.0 | 1.23 | 19.5 |
| All | 87 067 | NA | 43.3 | 55.1 | 2.28 | 11 485 | NA | 26.9 | 109.1 | 3.91 | 9606 | NA | 16.3 | 68.8 | 2.44 | |||
*Rate per 100 000 population.
†SIM-to-suicide rate ratio.
‡Projected ‘years of life lost’ at exact age at the beginning of the age interval.
SRR, suicide rate ratio; YLL, years of life lost.
Separation of the sexes revealed much higher age-specific SIM rates for men than women irrespective of race/ethnicity (table 3). Rate increases between 2008 and 2017 were much greater across most of the age spectrum for blacks than for Hispanics and whites. They also tended to be greater for Hispanic men and women than for white counterparts, especially at the younger ages. Sex-specific and age-specific SIM-to-suicide rate ratios commonly expanded across the observation period, with female ratios generally exceeding male ratios in 2008 and 2017. Blacks were a high outlier regardless of sex. The second indicator of premature mortality was estimated years of life lost by the individuals who died from self-injury. Greater in 2017 than in 2008, total respective lost years of life (based on exact age zero) for Hispanics, whites and blacks in 2008 and 2017 were projected to be 37.0 and 42.6, 35.7 and 37.1 and 32.2 and 32.4.
Table 3.
Patterns and change for self-injury mortality (SIM) by race/ethnicity, age and sex, USA, 2008 versus 2017
| White (non-Hispanic) | Black (non-Hispanic) | Hispanic | ||||||||||||||||
| No. Deaths | Cumulative Deaths, % | Rate* | Period Change, % | SIM: SRR† | YLL‡ | No. Deaths | Cumulative Deaths, % | Rate* | Period Change, % | SIM: SRR† |
YLL‡ | No. Deaths | Cumulative Deaths, % | Rate* | Period Change, % | SIM: SRR† |
YLL‡ | |
| Age, years | Male, 2008 | |||||||||||||||||
| 0–14 | 108 | 0.3 | 0.6 | NA | 1.0 | 33.6 | 22 | 0.6 | 0.5 | NA | 1.00 | 29.0 | 13 | 0.3 | 0.2 | NA | 1.00 | 35.5 |
| 15–24 | 4692 | 12.1 | 35.7 | NA | 1.85 | 33.5 | 489 | 14.1 | 14.8 | NA | 1.17 | 28.9 | 632 | 17.5 | 14.2 | NA | 1.49 | 35.4 |
| 25–34 | 6891 | 29.4 | 57.7 | NA | 2.15 | 30.3 | 641 | 31.8 | 25.6 | NA | 1.55 | 26.5 | 907 | 42.2 | 21.0 | NA | 1.94 | 32.7 |
| 35–44 | 8029 | 49.5 | 59.4 | NA | 1.90 | 25.7 | 769 | 53.1 | 30.3 | NA | 2.38 | 22.9 | 905 | 66.7 | 25.3 | NA | 2.16 | 29.1 |
| 45–54 | 9974 | 74.6 | 63.5 | NA | 1.81 | 21.0 | 959 | 79.6 | 38.2 | NA | 3.56 | 19.2 | 724 | 86.4 | 28.8 | NA | 2.37 | 25.1 |
| 55–64 | 5343 | 88.0 | 42.0 | NA | 1.38 | 15.9 | 520 | 93.9 | 32.4 | NA | 3.77 | 15.0 | 289 | 94.3 | 21.1 | NA | 1.99 | 20.6 |
| 65–74 | 2286 | 93.8 | 30.1 | NA | 1.11 | 12.7 | 147 | 98 | 18.2 | NA | 1.77 | 11.5 | 117 | 97.4 | 17.5 | NA | 1.24 | 18.0 |
| 75+ | 2486 | 100 | 41.7 | NA | 1.06 | 12.5 | 73 | 100 | 15.5 | NA | 1.30 | 12.7 | 94 | 100 | 23.1 | NA | 1.09 | 17.9 |
| All | 39 809 | NA | 40.6 | NA | 1.67 | 3620 | NA | 19.6 | NA | 2.10 | 3681 | NA | 15.1 | NA | 1.88 | |||
| Male, 2017 | ||||||||||||||||||
| 0–14 | 227 | 0.4 | 1.4 | 125.4 | 1.00 | 35.4 | 46 | 0.6 | 1.0 | 108.6 | 1.00 | 28.9 | 61 | 0.8 | 0.8 | 314.9 | 1.00 | 39.3 |
| 15–24 | 6126 | 10.2 | 50.1 | 40.4 | 1.84 | 35.2 | 830 | 10.4 | 24.7 | 66.9 | 1.47 | 28.7 | 1232 | 17.1 | 24.6 | 73.1 | 1.58 | 39.1 |
| 25–34 | 14 090 | 32.9 | 108.3 | 87.7 | 3.11 | 32.5 | 1700 | 30.6 | 53.2 | 107.6 | 2.61 | 26.7 | 1995 | 43.4 | 40.8 | 93.8 | 2.51 | 35.9 |
| 35–44 | 12 164 | 52.4 | 102.7 | 73 | 2.77 | 27.1 | 1566 | 49.3 | 61.8 | 104.1 | 4.00 | 23.1 | 1729 | 66.2 | 39.8 | 57.3 | 3.04 | 31.1 |
| 45–54 | 12 058 | 71.8 | 89.4 | 40.7 | 2.26 | 21.7 | 1869 | 71.5 | 74.5 | 94.9 | 5.90 | 19.4 | 1449 | 85.4 | 41.7 | 44.5 | 3.18 | 26.4 |
| 55–64 | 9992 | 87.9 | 68.5 | 63.0 | 1.85 | 16.7 | 1766 | 92.5 | 78.8 | 143.7 | 9.44 | 15.5 | 749 | 95.3 | 32.8 | 55.5 | 2.77 | 21.6 |
| 65–74 | 4143 | 94.6 | 38.5 | 28.2 | 1.26 | 12.8 | 532 | 98.9 | 42.9 | 136.4 | 4.93 | 11.4 | 236 | 98.4 | 20.3 | 16.4 | 1.77 | 18.0 |
| 75+ | 3373 | 100 | 48.6 | 16.5 | 1.05 | 12.5 | 96 | 100 | 15.0 | −3.5 | 1.65 | 12.7 | 123 | 100 | 18.5 | −19.6 | 1.13 | 17.8 |
| All | 62 174 | NA | 62.7 | 54.5 | 2.09 | 8405 | NA | 41.2 | 109.6 | 3.62 | 7575 | NA | 25.4 | 68.1 | 2.39 | |||
| Female, 2008 | ||||||||||||||||||
| 0–14 | 40 | 0.2 | 0.2 | NA | 1.00 | 36.9 | 8 | 0.6 | 0.2 | NA | 1.00 | 34.8 | 9 | 1.0 | 0.1 | NA | 1.00 | 41.4 |
| 15–24 | 1111 | 7.2 | 8.8 | NA | 2.24 | 36.7 | 121 | 9.5 | 3.7 | NA | 1.44 | 34.6 | 140 | 15.9 | 3.5 | NA | 1.61 | 41.2 |
| 25–34 | 2188 | 21.0 | 18.5 | NA | 2.82 | 34.7 | 185 | 23.1 | 6.7 | NA | 2.37 | 32.7 | 189 | 36.2 | 4.9 | NA | 2.28 | 38.4 |
| 35–44 | 3772 | 44.7 | 28.1 | NA | 2.78 | 31.2 | 343 | 48.3 | 12.0 | NA | 4.97 | 30.0 | 221 | 59.8 | 6.5 | NA | 2.76 | 35.0 |
| 45–54 | 5116 | 76.8 | 32.1 | NA | 2.80 | 26.3 | 464 | 82.4 | 16.3 | NA | 8.29 | 25.8 | 238 | 85.3 | 9.5 | NA | 3.01 | 31.0 |
| 55–64 | 2362 | 91.7 | 17.8 | NA | 2.08 | 19.6 | 174 | 95.2 | 9.0 | NA | 7.56 | 19.7 | 83 | 94.2 | 5.5 | NA | 2.86 | 25.0 |
| 65–74 | 701 | 96.1 | 8.2 | NA | 1.61 | 14.6 | 44 | 98.5 | 4.0 | NA | 2.93 | 15.0 | 31 | 97.5 | 3.7 | NA | 2.82 | 21.5 |
| 75+ | 626 | 100 | 6.7 | NA | 1.64 | 13.7 | 21 | 100 | 2.3 | NA | 2.33 | 15.1 | 23 | 100 | 3.6 | NA | 1.92 | 20.9 |
| All | 15 916 | NA | 15.7 | NA | 2.47 | 1360 | NA | 6.7 | NA | 3.98 | 934 | NA | 4.0 | NA | 2.4 | |||
| Female, 2017 | ||||||||||||||||||
| 0–14 | 101 | 0.4 | 0.6 | 170.3 | 1.00 | 38.7 | 20 | 0.6 | 0.4 | 149.1 | 1.00 | 35.8 | 30 | 1.5 | 0.4 | 193.8 | 1.00 | 46.0 |
| 15–24 | 1885 | 8.0 | 16.3 | 84.6 | 2.53 | 38.5 | 295 | 10.2 | 9.1 | 145.0 | 2.03 | 35.6 | 350 | 18.7 | 7.4 | 109.2 | 1.75 | 45.6 |
| 25–34 | 4911 | 27.3 | 38.8 | 109.4 | 4.24 | 36.3 | 574 | 28.9 | 17.4 | 161.5 | 4.07 | 33.4 | 510 | 43.8 | 11.5 | 136.0 | 3.04 | 42.1 |
| 35–44 | 5160 | 48.4 | 44.1 | 57.1 | 3.74 | 31.7 | 614 | 48.8 | 21.7 | 81.0 | 4.95 | 29.8 | 439 | 65.4 | 10.6 | 63.8 | 3.25 | 36.9 |
| 45–54 | 5972 | 72.4 | 44 | 37.0 | 3.09 | 26.4 | 801 | 74.8 | 28.1 | 72.7 | 9.89 | 25.8 | 398 | 85.0 | 11.6 | 22.6 | 3.16 | 32.1 |
| 55–64 | 4700 | 91.3 | 30.7 | 73.0 | 2.67 | 20.4 | 626 | 95.1 | 23.5 | 162.2 | 9.07 | 20.7 | 217 | 95.7 | 9.0 | 62.9 | 3.74 | 26.5 |
| 65–74 | 1471 | 97.2 | 12.4 | 51.6 | 1.67 | 14.8 | 120 | 99.0 | 7.3 | 81.8 | 5.00 | 15.1 | 60 | 98.6 | 4.3 | 16.6 | 2.22 | 21.7 |
| 75+ | 692 | 100 | 7.1 | 5.3.0 | 1.56 | 13.7 | 30 | 100 | 2.6 | 13.9 | 2.50 | 15.1 | 28 | 100 | 2.8 | −22.5 | 2.00 | 20.9 |
| All | 24 893 | NA | 24.4 | 55.8 | 2.96 | 3080 | NA | 13.9 | 106.2 | 5.00 | 2032 | NA | 7.0 | 75.1 | 2.68 | |||
*Rate per 100 000 population. The CDC cautions that rates based on cases fewer than 20 may be unstable.
†Self-injury mortality-to-suicide rate ratio.
‡Projected ‘years of life lost’ at exact age at the beginning of the age interval.
Discussion
SIM rates escalated rapidly in all three of the major racial/ethnic groups in the USA over the observation period. Non-Hispanic blacks recorded greater relative increases than non-Hispanic whites, the group with by far the highest rates. Examination of SIM-to-suicide rate ratios exposed health data disparities, which profoundly affected blacks, and women more than men independent of race/ethnicity. Beyond the issue of disparities emanating from differential suicide undercounting, the current approach of recording most drug-related fatalities as an ‘accident’ or ‘unintentional’ dampens the urgent public health need to develop effective upstream preventive interventions for recurring self-injurious behaviours—interventions with the potential to address common risks for the full range of self-injury fatalities.1 This need speaks to the inadequacy of many clinical care systems and state regulations that separate the treatment of persons with substance-related disorders from those with mental health problems in the face of substantial comorbidity and common social determinants of antecedent life turmoil and subsequent negative outcomes.
Inclusion of the great preponderance of ‘accidental’ and undetermined drug intoxication deaths into our estimation of SIM revealed evidence of convergence in trends between black and white rates for both sexes that in suicide trends manifested in women but not men. Some convergence was also apparent between Hispanics and whites, but the SIM rate trajectory for Hispanics was appreciably lower than those for the other two groups. Black and Hispanic suicide rates were similar throughout the observation period, while black SIM rates rose much more sharply than Hispanic as well as white rates. However, the group with the lowest SIM rates, Hispanics, incurred the largest relative burden of SIM-attributable premature mortality for either sex. Application of SIM showed relatively greater capture of the nonsuicide drug component among women, irrespective of race/ethnicity—consistent with the observation that their suicides may be under-reported relatively more often than those of males because drug ingestion is their leading method of suicide25 and suicide attempts.37
The surging tide of opioid deaths is now in the vanguard of public health concerns and commands pervasive media attention. However, despite their rising rate trend since 2000,5 societal sensitivity to the overlapping38 39 but generally less visible suicides40 waxes and wanes with intermittent media stories on teenage clusters or celebrity deaths and important but intermittent reports on suicides among the active military and military veterans. Emphasising premorbid decedent behaviour rather than postmortem inference of decedent intent, SIM accommodates self-injurious drug deaths and misclassified drug suicides as importantly related ‘elephants in the room’ in current US MOD accounting and classification. Moreover, a comprehensive examination of SIM rates relative to rates of specific subsets—suicide and substance poisoning, in particular—likely would reveal substantial variations in regional mortality trends requiring local investigation of aetiology and locally tailored prevention planning, resource allocation and treatment.
Limitations
Our operationalisation of SIM currently augments registered suicides by all methods and any age at death with 80% of selected ‘accidental’ or unintentional drug poisoning deaths and 90% of selected undetermined drug poisoning deaths among persons aged >15 years. Although we believe they are conservative, these fractional estimates are nonetheless arbitrary. Confirmation or refutation of their accuracy as minima may be accomplished through in-depth analysis of selected samples of ME/C cases involving: (1) an assessment of sources of medications, including diversion/theft of medications, procurement of illicitly manufactured pills and documentation of associated doctor and pharmacy shopping in prescription drug monitoring databases; (2) such autopsy-confirmed evidence as a large amount of pills and fragments in the stomachs or small intestines of decedents and stigmata of injection drug use; (3) illicit drug concentrations in toxicological samples; and (4) verification of decedent drug paraphernalia at the death scene from medicolegal death investigators. Even if fortifying medicolegal death investigations of equivocal intent cases with formal psychological autopsy inquiries of key informants, it may often be impossible to establish whether a person dying from drug intoxication was intentional and therefore a suicide. However, we have confidence it would be possible to define that this person died from self-injurious behaviours rather than an ‘accident’.
Other than in the suicide (ICD-10X65) component, deaths from alcohol poisoning were omitted in our operationalisation of SIM. Acute alcohol consumption is common among suicides as part of lethal drug cocktails or associated with more violent methods,41 especially among men,42 but is rarely the sole or primary agent in suicides. Alcohol poisoning deaths assigned as suicide, ‘accident’ or undetermined by medical examiners or coroners were subsumed under the non-drug category in the WISQARS database. They could not be differentiated within their assigned MOD. However, differentiation was enabled through accessing the federal, restricted access Wide-ranging Online Data for Epidemiologic Research database. Suicides by alcohol poisoning were few across the observation period, 2008–2017, with an annual average of 42.43 ‘Accident’ (ICD-10X45) and undetermined alcohol poisoning deaths (ICD-10 Y15) in the US population aged 15 years and older averaged 2188 and 70, respectively. The combined rate of alcohol poisoning deaths assigned as ‘accident’ or undetermined for this age group remained stable at 0.9 per 100 000 population. By contrast, the rate for the corresponding opioid and drug death component, which we represented in SIM, rose and ranged from 7.0 per 100 000 in 2008 to 24.5 in 2017. Besides ‘accident’ and undetermined alcohol poisoning deaths, not factored into SIM were the inaccessible numbers of relevant injury deaths that were potentially obscured within the mortality categories of assault (ICD-10X85), mental and behavioural disorders due to psychoactive substance use (ICD-10 F10-19) and ill-defined and unknown causes (ICD-10 R99). Other limitations of this observational study included our lack of detailed data on social determinants to explain plausible mechanisms for demographic variation in SIM trends and patterns, and inability to discern their potential relationships to state and local variation in autopsy and toxicological testing rates, or the type, quality and accreditation status of medicolegal death investigation systems.
Conclusion
Application of SIM exposed substantial excess burdens in the USA from substance poisoning relative to suicide for minorities, particularly non-Hispanic blacks, and for women generally. The continuing segregation of mortality statistics—and in turn, of public health prevention efforts that separate persons and populations based on the coding of events on the day of death rather than the nature of their daily lives and vulnerabilities—impedes broadly applied efforts targeting common risks. Using SIM, SIM-to-suicide rate ratios and SIM-attributable premature mortality to examine the burden of self-destructive, lethal behaviours draws attention to the rapidly growing challenges for clinical medicine and public health, while mitigating the confounding effects of differential undercounting of suicides as singular sentinel events often used by clinicians, regulatory agencies and policymakers to define distressed individuals and programmatic inadequacies, in addition to our distressed society.
In order to facilitate surveillance and aetiologic research on SIM, and hence the design and targeting of effective prevention and treatment, we suggest the inclusion of a check box on death certificates and in reports from ME/Cs, police and other first responders that signify ‘self-injury’ (or ‘self-harm’ regardless of intentionality) whenever appropriate. Without this tool, we are forced to estimate the changing patterns of SIM rates. SIM serves to counter the ingrained forensic notion that overdose deaths are ‘accidents’, and even CDC’s substitution of the term ‘unintentional’ for ‘accidental’ fails to confront directly the consciously self-injurious nature of repetitive ingestion of toxic drugs. A societal imperative is the development and implementation of comprehensive strategies to address and prevent the common antecedents of self-injurious behaviours for women, racial/ethnic minorities and all groups.
What is already known on the subject.
Suicides are undercounted in the USA, in part reflecting discrepancies based on race/ethnicity and sex.
Self-injury mortality (SIM), as a composite of registered suicides and estimated ‘accidental’/undetermined substance-related fatalities, is increasing rapidly.
What this study adds.
Racial/ethnic and sex differences are obscured by separately presenting suicide rates and ‘accidental’ substance overdose mortality rates.
Examination of SIM to suicide rate gaps exposed substantial excess burdens from substance poisoning for minorities, especially non-Hispanic blacks, and for women generally.
Arbitrary distinctions based on determining the proximate manner of death fail to provide the necessary foundation for planning effective upstream prevention and clinical intervention strategies.
Footnotes
Contributors: IRHR conceived and designed the study and acquired the data. IRHR, EDC, HSC, HJ and KBN prepared the first draft of the manuscript. IRHR and HJ conducted the analysis. All authors were involved in the interpretation of the data, revision of the manuscript and provided final approval of the submission.
Funding: This study was partially funded by the National Center for Injury Prevention and Control (grant no: R49CE002093).
Disclaimer: The views expressed are those of the authors and do not necessarily represent the position or policy of the Centers for Disease Control and Prevention or the United States' Government.
Competing interests: None declared.
Patient consent for publication: Not required.
Provenance and peer review: Not commissioned; externally peer reviewed.
Data availability statement: Data are available in a public, open-access repository. All data relevant to the study are included in the article or uploaded as supplementary information.
References
- 1. Caine ED. Forging an agenda for suicide prevention in the United States. Am J Pub Health 2013;103:822–9. 10.2105/AJPH.2012.301078 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Rockett IRH, Wang S, Stack S, et al. . Race/ethnicity and potential suicide misclassification: window on a minority suicide paradox? BMC Psychiatry 2010;10:35 10.1186/1471-244X-10-35 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Goldsmith SK, Pellmar TC, Kleinman AM, et al. . Reducing suicide: a national imperative. Washington, DC: National Academies Press, 2002. [PubMed] [Google Scholar]
- 4. Rockett IRH, Caine ED, Connery HS, et al. . Discerning suicide in drug intoxication deaths: paucity and Primacy of suicide notes and psychiatric history. PLoS One 2018;13:e0190200 10.1371/journal.pone.0190200 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Rockett IRH, Lilly CL, Jia H, et al. . Self-Injury mortality in the United States in the early 21st century: a comparison with proximally ranked diseases. JAMA Psychiatry 2016;73:1072–81. 10.1001/jamapsychiatry.2016.1870 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Rockett IRH, Caine ED, Connery HS, et al. . Mortality in the United States from self-injury surpasses diabetes: a prevention imperative. Inj Prev 2019;25 10.1136/injuryprev-2018-042889 [DOI] [PubMed] [Google Scholar]
- 7. US Public Health Service National Strategy for Suicide Prevention: Goals and Objectives for Action. Washington, DC: Department of Health and Human Services, 2001. [PubMed] [Google Scholar]
- 8. Botello T, Noguchi T, Sathyavagiswaran L, et al. . Evolution of the psychological autopsy: fifty years of experience at the Los Angeles County chief medical examiner-coroner's office. J Forensic Sci 2013;58:924–6. 10.1111/1556-4029.12138 [DOI] [PubMed] [Google Scholar]
- 9. Gray D, Coon H, McGlade E, et al. . Comparative analysis of suicide, accidental, and undetermined cause of death classification. Suicide Life Threat Behav 2014;44:304–16. 10.1111/sltb.12079 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Rockett IRH, Smith GS, Caine ED, et al. . Confronting death from drug self-intoxication (DDSI): prevention through a better definition. Am J Public Health 2014;104:e49–55. 10.2105/AJPH.2014.302244 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Litman RE. Psychological-psychiatric aspects in certifying modes of death. J Forensic Sci 1968;13:46–54. 10.2466/PR0.105.3.685-686 [DOI] [PubMed] [Google Scholar]
- 12. Institute of Medicine Emergency medical services at the crossroads. Washington, DC: National Academies Press, 2006. [Google Scholar]
- 13. Institute of Medicine Hospital-based emergency care: at the breaking point. Washington, DC: National Academies Press, 2006. [Google Scholar]
- 14. Committee on Identifying the Needs of the Forensic Sciences Community, National Research Council Strengthening forensic science in the united states: a path forward. Washington, DC: National Academies Press, 2009. [Google Scholar]
- 15. Hanzlick RL. A perspective on medicolegal death investigation in the United States: 2013. Acad Forens Pathol 2014;4:2–9. 10.23907/2014.001 [DOI] [Google Scholar]
- 16. Stone DM, Holland KM, Bartholow B, et al. . Deciphering suicide and other manners of death associated with drug intoxication: a centers for disease control and prevention consultation meeting summary. Am J Public Health 2017;107:1233–9. 10.2105/AJPH.2017.303863 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Glei DA, Goldman N, Weinstein M. A growing socioeconomic divide: effects of the great recession on perceived economic distress in the United States. PLoS One 2018;14:e0214947 10.1371/journal.pone.0214947 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Ciccarone D. The triple wave epidemic: supply and demand drivers of the US opioid overdose crisis. Int J Drug Policy 2019. 10.1016/j.drugpo.2019.01.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Scholl L, Seth P, Kariisa M. Drug and opioid-involved overdose deaths- United States, 2013–2017. MMWR: Morbidity and Mortality Weekly Report 2019;67:1419–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Vestal C. Opioid overdoses swamp medical examiners. Stateline: The Pew Charitable Trusts, 2017. https://www.pewtrusts.org/en/research-and-analysis/blogs/stateline/2017/07/06/opioid-overdose-deaths-swamp-medical-examiners [Google Scholar]
- 21. Darke S, Ross J, Marel C, et al. . Patterns and correlates of attempted suicide amongst heroin users: 11-year follow-up of the Australian treatment outcome study cohort. Psychiatry Res 2015;227:166–70. 10.1016/j.psychres.2015.04.010 [DOI] [PubMed] [Google Scholar]
- 22. Olfson M, Crystal S, Wall M, et al. . Causes of death after nonfatal opioid overdose. JAMA Psychiatry 2018;75:820–7. 10.1001/jamapsychiatry.2018.1471 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Bohnert ASB, Ilgen MA. Understanding links among opioid use, overdose, and suicide. N Engl J Med 2019;380:71–9. 10.1056/NEJMra1802148 [DOI] [PubMed] [Google Scholar]
- 24. Rockett IRH, Caine ED. Self-Injury is the eighth leading cause of death in the United States. It is time to pay attention. JAMA Psychiatry 2015;72:1069–70. [DOI] [PubMed] [Google Scholar]
- 25. Rockett IRH, Caine ED, Stack S, et al. . Method overtness, forensic autopsy, and the evidentiary suicide note: a multilevel national violent death reporting system analysis. PLoS One 2018;13:e0197805 10.1371/journal.pone.0197805 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Rockett IRH, Lian Y, Stack S, et al. . Discrepant comorbidity between minority and white suicides: a national multiple cause-of-death analysis. BMC Psychiatry 2009;9:10 10.1186/1471-244X-9-10 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Stone DM, Simon TR, Fowler KA, et al. . Vital Signs: Trends in State Suicide Rates - United States, 1999-2016 and Circumstances Contributing to Suicide - 27 States, 2015. MMWR Morb Mortal Wkly Rep 2018;67:617–24. 10.15585/mmwr.mm6722a1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Stack S, Rockett IRH. Are suicide note writers representative of all suicides? Analysis of the National violent death reporting system. Suicide Life Threat Behav 2018;48:12–20. 10.1111/sltb.12320 [DOI] [PubMed] [Google Scholar]
- 29. Morrison RS, Wallenstein S, Natale DK, et al. . “We Don't Carry That” — Failure of Pharmacies in Predominantly Nonwhite Neighborhoods to Stock Opioid Analgesics. N Engl J Med 2000;342:1023–6. 10.1056/NEJM200004063421406 [DOI] [PubMed] [Google Scholar]
- 30. Green CR, Ndao-Brumblay SK, West B, et al. . Differences in prescription opioid analgesic availability: comparing minority and white pharmacies across Michigan. J Pain 2005;6:689–99. 10.1016/j.jpain.2005.06.002 [DOI] [PubMed] [Google Scholar]
- 31. Shiels MS, Freedman ND, Thomas D, et al. . Trends in U.S. drug overdose deaths in non-Hispanic black, Hispanic, and non-Hispanic white persons, 2000–2015. Ann Intern Med 2018;168:453–5. 10.7326/M17-1812 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Case A, Deaton A. Rising morbidity and mortality in midlife among white non-Hispanic Americans in the 21st century. Proc Natl Acad Sci U S A 2015;112:15078–83. 10.1073/pnas.1518393112 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Case A, Deaton A. Mortality and morbidity in the 21st century. Brookings Pap Econ Act 2017;2017:397–476. 10.1353/eca.2017.0005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. US Department of Health and Human Services Web-Based Injury Statistics Query and Reporting System (WISQARS). Available: http://www.cdc.gov/injury/wisqars/index.html [Accessed 23 Apr 2019].
- 35. Manton KG, Patrick CH, Stallard E. Population impact of mortality reduction: the effects of elimination of major causes of death on the 'saved' population. Int J Epidemiol 1980;9:111–20. 10.1093/ije/9.2.111 [DOI] [PubMed] [Google Scholar]
- 36. Rockett IRH. Injury elimination and survival a cross-national study. Public Health 1998;112:27–30. 10.1016/S0033-3506(98)00202-9 [DOI] [PubMed] [Google Scholar]
- 37. Ting SA, Sullivan AF, Boudreaux ED, et al. . Trends in US emergency department visits for attempted suicide and self-inflicted injury, 1993-2008. Gen Hosp Psychiatry 2012;34:557–65. 10.1016/j.genhosppsych.2012.03.020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Wilcox HC, Conner KR, Caine ED. Association of alcohol and drug use disorders and completed suicide: an empirical review of cohort studies. Drug Alcohol Depend 2004;76:S11–S19. 10.1016/j.drugalcdep.2004.08.003 [DOI] [PubMed] [Google Scholar]
- 39. Rockett IRH, Hobbs G, De Leo D, et al. . Suicide and unintentional poisoning mortality trends in the United States, 1987-2006: two unrelated phenomena? BMC Public Health 2010;10:705 10.1186/1471-2458-10-705 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Oquendo MA, Volkow ND. Suicide: a silent contributor to opioid-overdose deaths. N Engl J Med 2018;378:1567–9. 10.1056/NEJMp1801417 [DOI] [PubMed] [Google Scholar]
- 41. Kaplan MS, McFarland BH, Huguet N, et al. . Acute alcohol intoxication and suicide: a gender-stratified analysis of the National violent death reporting system. Inj Prev 2013;19:38–43. 10.1136/injuryprev-2012-040317 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Kaplan MS, Huguet N, Caetano R, et al. . Heavy alcohol use among suicide decedents relative to a nonsuicide comparison group: gender-specific effects of economic contraction. Alcohol Clin Exp Res 2016;40:1501–6. 10.1111/acer.13100 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. US Department of Health and Human Services Wide-ranging Online Data for Epidemiologic Research (WONDER). Available: https://wonder.cdc.gov/ucd-icd10.html [Accessed 15 Aug 2019].