

Abstract
Background:
Female physicians are significantly less likely than male physicians to be full professors, even after accounting for age, experience, specialty, and measures of research and clinical productivity.
Objective:
To evaluate sex differences in academic rank in the Allergy and Immunology workforce.
Methods:
We used a cross-sectional physician dataset containing allergist sex, age, years since residency, faculty appointment, authored publications, National Institutes of Health (NIH) funding, clinical trial investigation, and Medicare reimbursement to investigate sex differences in the academic Allergy and Immunology workforce using multilevel logistic regression models.
Results:
Among 507 academic allergists (9.3% of practicing U.S. allergists in 2014), 323 (63.7%) were men and 184 (36.3%) were women. Female allergists were younger (47.9 vs 56.9 years, p<0.001), had fewer total (12.5 vs 28.7, p<0.001) and first/last author (8.0 vs. 21.5, p<0.001) average publications, were less likely to have NIH funding (13.0% vs 23.5%, p=0.004), were less frequently a clinical trial investigator (10.3% vs 16.1%, p=0.07), and generated less average annual Medicare revenue ($44,000 vs $23,000, p=0.10). Of 152 (30.0%) full professors, 126 (82.9%) were male and 26 (17.0%) were female. After multivariable adjustment, rates of full professorship among female and male allergists were not significantly different (absolute adjusted difference for female vs male allergists, 6.0%; 95% confidence interval: −8.3%, 20.2%).
Conclusions:
Among allergists with U.S. medical school faculty appointments, men and women were similarly likely to be full professor after accounting for factors influencing promotion. Underlying differences in research productivity and NIH funding not explained by age differences alone warrant additional investigation.
Keywords: allergy, promotion, professor, disparity, gender, women, advancement
Capsule Summary:
Among U.S. academic allergists in 2014 (n=507; 36.3% female), 126 (83%) of full professors were male. After accounting for factors that influence promotion, men and women were similarly likely to be full professor (absolute adjusted difference for female vs male allergists, 6.0%; 95% confidence interval: −8.3%, 20.2%).
INTRODUCTION
Women comprise half of medical school classes and residency programs and 39% of full-time medical school faculty.1 However, obstacles exist for female physicians in academic medicine: women physicians are paid less than men performing similar work, complete more unpaid household-related work, and are less frequently full professors, deans, department chairs, and speakers at national meetings.2-5
Despite federal protections ensuring equal pay for equal work,6 women physicians receive less salary even when in the same specialty7-9 and academic rank10 as their male colleagues. While the salary gender gap has decreased in nonhealthcare industries, the salary gap for female physicians grew from $34,620 between 1996-2000 to $56,019 between 2006-2010.11 In a survey of 20,329 practicing United States (U.S.) physicians, full-time male physicians reported higher mean salaries than full-time female physicians.12 Academic female physicians were found to earn almost $20,000 less per year than academic male physicians after adjusting for age, experience, specialty, faculty rank, and measures of research and clinical productivity.3 Early career female researchers earned $30,000 less per year than the early career male researchers on identical mentored career development awards from the National Institutes of Health (NIH).8
In addition to the identified salary disparities, disparities in rank exist for academic female physicians and this difference has been shown to persist after adjustment for factors known to impact promotion in academic medicine.5 To date, sex differences in the rate of full professorship have been identified in most medical specialties examined, including surgery, emergency medicine, cardiology, and infectious diseases.5,13-15
Allergy and Immunology has a relatively small footprint in academic medicine, occasionally combined with Pulmonary or Rheumatology, and may be housed within the Department of Medicine and/or Pediatrics.16 Prior adjusted analyses of sex and academic rank did not consider allergists, although over 1,000 members (15%) of the American Academy of Allergy, Asthma and Immunology (AAAAI) reported being medical school faculty (Personal communication, AAAAI). The last Allergy and Immunology workforce report showed that women were increasingly represented in Allergy and Immunology; while women comprised just 10% of Allergy and Immunology physicians in 1989, they comprised 20% in 1999 and 25% in 2004.16
In this study, our objective was to evaluate sex differences in rank in the academic Allergy and Immunology workforce using a comprehensive cross-sectional physician dataset with information on physician sex, age, years since residency, faculty appointment, authored publications, NIH funding, clinical trial investigation, and Medicare reimbursement.
METHODS
Dataset Description
Physician-level data were provided by Doximity (doximity.com), an online networking service for physicians in the U.S., on November 10, 2014. The data included all 1,005,419 U.S. physicians in all specialties as of the date data were provided, regardless of Doximity registration status. Physicians can personally register with Doximity and use its services free of charge. As of November 10, 2014, 24% of US physicians (n=239,136) were registered members. Doximity physicians included all those with a National Plan and Provider Enumeration System National Provider Identifier (NPI); physicians without an NPI were also included if they self-registered or worked at an institution that collaborates with Doximity. Thus, Doximity physicians included physicians who graduated from medical school but did not enter residency and physician researchers or administrators who do not have an NPI.
Doximity-provided data included physician sex, age, residency completion year, U.S. medical school faculty appointment and rank (assistant, associate, or full professor), specialty, number of publications indexed in PubMed (total publications, first or last author publications), active or prior grants from the NIH (from NIH RePORT database including principal investigator title only), and clinical trials for which the physician was a principal investigator or sub-investigator (from ClinicalTrials.gov). The methods by which Doximity assembled their dataset have also been described in detail in prior physician workforce analyses that included assessments of data validity.5,13-15,17
The research team added Medicare reimbursements for providers to the Doximity dataset in 2013, using the NPI for dataset linkage. Medicare reimbursement data were publicly available data from the Centers for Medicare and Medicaid Services Medicare Provider Utilization and Payment Database.18 The research team also used the 2013 US News and World Report rankings for research to determine whether or not the physician was faculty at an institution ranked in the “top 20.”
Study Population
We used physician specialty and faculty appointment data to identify all academic Allergy and Immunology physicians in 2014 with titles of Assistant, Associate, or Full Professor at a U.S. Medical School.
Statistical Analysis
We performed descriptive analyses, presenting numbers with frequencies for variables such as age groups, faculty at a US News and World Report “top 20” medical school, NIH grants, and clinical trials investigation. We used means with standard deviations or medians with interquartile ranges, as indicated, to describe the continuous variables age, years since residency, number of NIH grants, number of clinical trials, and Medicare reimbursements. We compared these measures between male and female Allergy and Immunology faculty members, and used chi-squared tests and t-tests, as indicated.
We considered the primary outcome of academic rank for allergy faculty members. We determined the frequency with which male and female allergists were full, associate, and assistant professors in a univariate analysis with chi-squared tests. We then determined the rate of full professorship (compared to associate and assistant professors) and the rate of full or associate professorship (compared to assistant professors) first considering a partially adjusted logistic regression model of academic rank as a function of the allergist’s sex and age only. Then, because sex differences in research and clinical productivity might also confound sex differences in academic rank we used a hierarchical multivariable logistic model of the probability of full professorship (or full or associate professorship as a combined outcome), assessed as a function of the allergist’s sex, age, years since residency completion, faculty appointment at US News and World Report “top 20” medical school, number of publications (total and first/last author), NIH grants, clinical trial investigation, and Medicare reimbursements. Medicare reimbursements were considered important to control for as they might be differential by allergist sex because of populations treated (adult vs pediatric patients), effort (full-time status vs part-time status), and clinical volume among full-time allergists (primarily research track vs primarily clinical track). The model also contained medical school-level random effect parameters because outcomes might be correlated among allergy faculty within each institution. While the final model included all variables considered potential confounders a priori, we performed sensitivity analyses considering alternative models of sex and academic rank.
We considered authored publications as a secondary outcome given its importance to faculty rank. We determined mean total number of publications, as well as first/last authored publications, comparing male and female allergy faculty in unadjusted analyses with chi-squared tests. We then considered a partially adjusted linear regression model of publications (total and first/last author) as a function of the allergist’s sex and age only. We finally used a hierarchical multivariable linear regression model of publications (total and first/last author) as a function of the allergist’s sex, age, years since residency, faculty appointment at US News and World Report “top 20” medical school, NIH funding, and total Medicare payments.
The models are presented with 95% confidence intervals (CIs) around adjusted estimates that reflect 0.025 in each tail or a p-value of less than 0.05. All statistical analyses were performed using STATA version 15.0 (STAT Inc, College Station, TX).
RESULTS
Faculty Characteristics
The Doximity dataset included 5,454 practicing U.S. allergists as of 2014, including 3,677 (67.4%) male allergists and 1,777 (32.6%) female allergists. We identified 507 Allergy and Immunology medical school assistant, associate and full professors (9.3% of all U.S. allergists), of whom 323 (63.7%) were men and 184 (36.3%) were women (Table 1).
Table 1.
Characteristics of academic Allergy and Immunology faculty by sex
| All (n = 507) | Male (n = 323) | Female (n = 184) | P-value* | |
|---|---|---|---|---|
| Age (years), μ (SD) | 53.7 (12.7) | 56.9 (12.5) | 47.9 (10.8) | <0.001 |
| Age groups (years), n (%) | <0.001 | |||
| Age <40 | 87 (17.8) | 37 (11.7) | 50 (28.7) | |
| Age 40-44 | 53 (10.8) | 26 (8.2) | 27 (15.5) | |
| Age 45-49 | 53 (10.8) | 28 (8.9) | 25 (14.4) | |
| Age 50-54 | 68 (13.9) | 40 (12.7) | 28 (16.1) | |
| Age 55-59 | 67 (13.7) | 51 (16.1) | 16 (9.2) | |
| Age 60-64 | 61 (12.5) | 45 (14.2) | 16 (9.2) | |
| Age 65+ | 101 (20.6) | 89 (28.2) | 12 (6.9) | |
| Years since residency,† μ (SD) | 22.8 (13.2) | 26.4 (13.2) | 16.6 (10.7) | <0.001 |
| Faculty at US News “top 20” medical school,¶ n (%) | 152 (30.0) | 97 (30.0) | 55 (29.9) | 0.97 |
| National Institutes of Health grants | ||||
| μ (SD) | 1.66 | 2.07 | 0.95 | 0.02 |
| At least one, n (%) | 100 (19.7) | 76 (23.5) | 24 (13.0) | 0.004 |
| At least one, Median (IQR) | 5 (2.0-11.0) | 4 (2.0-11.5) | 5 (2.5-9.0) | 0.71 |
| Clinical trials investigation | ||||
| At least one, n (%) | 71 (14.0) | 52 (16.1) | 19 (10.3) | 0.07 |
| At least one, Median (IQR) | 2 (1.0-2.0) | 2 (1.0-3.0) | 2 (1.0-2.0) | 0.84 |
| Medicare payments | ||||
| n (%) | 252 (49.7) | 177 (54.8) | 75 (40.8) | 0.002 |
| μ (SD), 2013 U.S. dollars | 38,000 (0.9) | 44,000 (1.1) | 23,000 (0.4) | 0.10 |
P-values reflect 2-sided t tests and chi-squared comparisons, as indicated.
Excluded the 156 allergists for whom years since residency was missing.
Physician on faculty at a medical school ranked among the “top 20” medical schools for research by US News and World Report in 2013.
Female allergists were younger than male allergists (47.9 vs 56.9 years; p <0 .001). Allergists <40 years old included 50 (28.7%) females and 37 (11.7%) males whereas allergists over 65 years old included 12 (6.9%) females, but 89 (28.2%) males. Female allergists had fewer mean years since residency completion (16.6 years vs 26.4 years, p<0.001). There were 152 allergists (30.0%) who were faculty at a US News and World Report “top 20” medical school with women equally likely as men to be faculty members at a US News and World Report “top 20” medical school (29.9% vs 30.0%, p= 0.97). Female allergists had fewer mean NIH grants (0.95 vs 2.07, p=0.02) and were less likely to have had at least one grant from the NIH (13.0% vs 23.5%, p=0.004). Women less frequently had one or more clinical trials compared to men (10.3% vs 16.1%, p = 0.07). Fewer female allergists had Medicare payments than male allergists (40.8% vs 54.8%, p=0.002). On average, female allergists had lower mean Medicare billing revenue than men ($23,000 vs $44,000, p = 0.10).
Outcomes: Univariable Analysis
Female allergists were less likely than male allergists to be full professors (14.1% vs 39.0% p < 0.001). Female allergists were similarly likely to male allergists to be associate professors (22.3% vs 19.8%, p=0.51), and more likely than male allergists to be an assistant professor (63.6% vs 41.2%, p<0.001, Table 2). Female allergists had fewer total (12.5 vs 28.7, p< 0.001) and first or last author (8.0 vs 21.5, p<0 .001) mean publications (Table 2).
Table 2.
Univariable analysis of allergist academic rank and publications by sex
| All (n = 507) | Male (n = 323) | Female (n = 184) | P-value* | |
|---|---|---|---|---|
| Academic rank, n (%) | ||||
| Assistant professor | 250 (49.3) | 133 (41.2) | 117 (63.6) | <0.001 |
| Associate professor | 105 (20.7) | 64 (19.8) | 41 (22.3) | 0.51 |
| Full professor | 152 (30.0) | 126 (39.0) | 26 (14.1) | <0.001 |
| Publications, μ (SD) | ||||
| Total | 22.8 (37.7) | 28.7 (43.6) | 12.5 (20.3) | <0.001 |
| First/last Author | 16.6 (31.2) | 21.5 (36.9) | 8.0 (13.8) | <0.001 |
P-values reflect 2-sided t tests and chi-squared comparisons, as indicated.
Outcomes: Multivariable Analyses
Academic Rank
In the model adjusting for age only, there was a significant sex difference in full professorship among academic allergists (adjusted difference, −9.0%; 95% CI: −18.0%, −.03%). The adjusted rate of full professorship was 26.6% among men and 17.3% among women (p = 0.049). Considering the combined outcome of associate or full professorship compared with assistant professorship there was no significant difference between male and female allergists when adjusted for age alone (adjusted difference, −3.3%; 95% CI: −11.5%, 5.0%). The adjusted rate of full or associate professorship (compared with assistant professorship) adjusted for age only was 45.1% among men and 40.3% among women (p=0.44).
After multivariate analysis adjusted for age, years since residency completion, faculty appointment at US News and World Report “top 20” medical school, number of publications (first or last author and total, first/last author), NIH grants, clinical trial investigation, and total Medicare payments, there was no statistically significant sex difference in full professorship among academic allergists (adjusted difference, 6.0%; 95% CI: −8.3%, 20.2%) (Table 3). The adjusted rate of full professorship was 29.1% among men and 35.1% among women (p = 0.42, Figure 1). We also found no significant sex difference in the combined outcome of associate or full professorship compared with assistant professorship (adjusted difference, −0.2%; 95% CI: −15.2%, 14.8%) (Table 3). The adjusted rate of full or associate professorship (compared with assistant professorship) was 45.8% among men and 45.6% among women (p=0.97) (Figure 1). Assessing different multivariable analyses in sensitivity analysis led to different adjusted differences, but there was still no statistically significant sex difference in full professorship (or associate or full professorship) among academic allergists (Supplemental Table 1).
Table 3.
Multivariable analyses of sex difference in U.S. academic allergists
| Full Professor vs. Assistant Professor and Associate Professor | Full Professor and Associate Professor vs. Assistant Professor | |||
|---|---|---|---|---|
| n/total N academic allergists (%) | Adjusted difference (95%CI)* | n/total N academic allergists (%) | Adjusted difference (95%CI)* |
|
| Sex | ||||
| Men | 126 / 323 (39.0) | [Reference] | 190 / 323 (58.8) | [Reference] |
| Women | 26 / 184 (14.1) | 6.0 (−8.3, 20.2)† | 67 / 184 (36.4) | −0.2 (−15.2, 14.8)¶ |
| Age groups, years | ||||
| Age <50 | 9 / 193 (4.7) | [Reference] | 36 / 193 (18.7) | [Reference] |
| Age 50-54 | 16 / 68 (23.5) | 5.2 (−25.0, 35.4) | 40 / 68 (58.8) | 5.0 (−23.5, 33.4) |
| Age 55-59 | 24 / 67 (35.8) | 4.3 (−22.0, 30.6) | 48 / 67 (71.6) | 5.1 (−23.7, 33.8) |
| Age 60-64 | 31 / 61 (50.8) | 6.0 (−33.1, 45.0) | 47 / 61 (77.0) | −8.9 (−42.7, 25.0) |
| Age 65+ | 69 / 101 (68.3) | 5.6 (−39.9, 51.0) | 79 / 101 (78.2) | −12.9 (−52.1, 26.3) |
| Years since residency (per one year) | 1.5 (0.1, 3.0) | 2.0 (0.4, 3.6) | ||
| Publication (per one publication) | ||||
| Total | 0.7 (0.2, 1.1) | 0.3 (−1.5, 2.0) | ||
| First/last Author | −0.3 (−0.5, 0.0) | 1.5 (−0.9, 3.9) | ||
| National Institutes of Health grants | ||||
| None | 85 / 407 (20.9) | [Reference] | 170 / 407 (41.8) | [Reference] |
| At least one | 67 / 100 (67.0) | −8.4 (−25.6, 8.8) | 87 / 100 (87.0) | −7.5 (−59.5, 44.5) |
| Clinical trial investigation | ||||
| None | 109 / 436 (25.0) | [Reference] | 201 / 436 (46.1) | [Reference] |
| At least one | 43 / 71 (60.6) | 39.8 (10.6, 69.1) | 56 / 71 (78.9) | 30.3 (4.8, 55.7) |
| Faculty at US News “top 20” Medical School | ||||
| No | 103 / 333 (30.9) | [Reference] | 164 / 333 (49.2) | [Reference] |
| Yes | 42 / 152 (27.6) | 0.3 (−5.3, 5.8) | 80 / 152 (52.6) | .19 (−0.4, 0.8) |
| Medicare payments, 2013 US dollars (per $100,000) | −12.8 (−30.9, 5.3) | −2.91 (−19.9, 14.1) | ||
CI, confidence interval
Regression model adjusted for faculty appointment at US News and World Report “top 20” medical school, age, years since residency completion, number of publications (first or last author and total), NIH grants, clinical trial investigation, total Medicare payments, and medical-school level fixed effects.
Adjusted difference in sensitivity analyses ranged of from −5.8% to +6.0% and all 95% Confidence Intervals included 0.0% (see Supplemental Table 1).
Adjusted difference in sensitivity analyses ranged of from −8.5% to +10.3% and all 95% Confidence Intervals included 0.0% (see Supplemental Table 1).
Figure 1. Sex differences in academic allergy faculty rank.
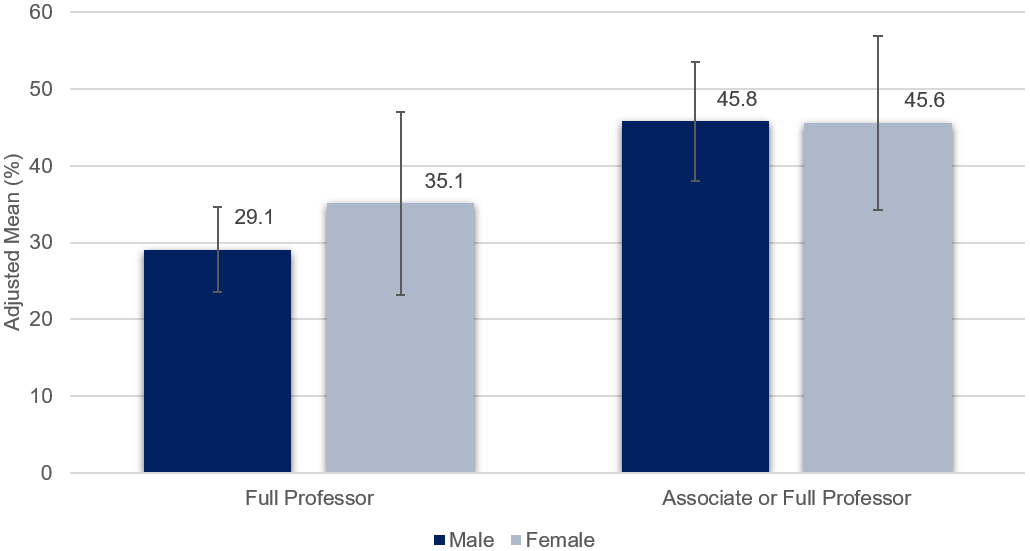
This figure displays the adjusted mean difference in academic rank for male and female U.S. academic allergists considering full professorship (vs. associate and assistant professor) and associate or full professorship (vs. assistant professor). The means are adjusted for age, years since residency completion, faculty appointment at US News and World Report “top 20” medical school, number of publications (first or last author and total), NIH grants, clinical trial investigation, and total Medicare payments.
Full professorship was positively associated with years since residency (adjusted difference 1.5%, 95% CI 0.1% to 3.0%), and being a clinical trials investigator (adjusted difference 39.8%, 95% CI 10.6% to 69.1%, Table 3). Associate or full professorship was also positively associated with years since residency (adjusted difference 2.0%, 95%CI 0.4% to 3.6%) and clinical trials investigation (adjusted difference 30.3%, 95% CI 4.8% to 55.7%, Table 3).
Publications
Female allergists had fewer mean total publications than male allergists after adjusting for age only (adjusted mean 17.8 for women and 25.8 for men, p=0.03). First or last author publications were also significantly fewer for female allergists compared to male allergists adjusted for age only (adjusted mean 12.2 for women and 19.4 for men, p=0.022).
We found no significant difference in mean publications between female and male allergists after adjusting for age, years since residency, faculty appointment at US News and World Report “top 20” medical school, NIH funding, and total Medicare payments (adjusted mean 13.9 for women and 19.2 for men, p=0.16, Figure 2). First or last author publications were also nonsignificant fewer for female allergists compared to male allergists (adjusted mean 9.3 for women and 17.2 for men, p=0.08).
Figure 2. Sex differences in academic allergy faculty publications.
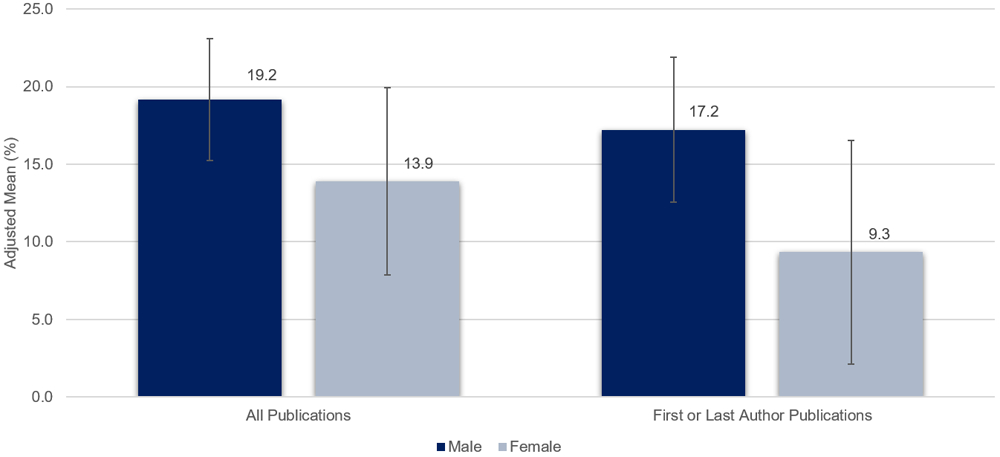
This figure demonstrates sex differences in the adjusted mean difference in all publications and first or last author publications, adjusted for age, years since residency, faculty appointment at US News and World Report “top 20” medical school, NIH funding, and total Medicare payments.
DISCUSSION
We used a comprehensive physician dataset that included all U.S. allergists to study sex differences in the academic Allergy and Immunology workforce. We found that the proportion of female allergists in the Allergy and Immunology workforce is increasing over time, with female allergists comprising 32.6% of all allergists, and 36.3% of academic allergists in 2014. Although female academic allergists were 25% less likely than male academic allergists to be a full professor, we found no difference in faculty rank between academic male and female allergists after multivariable adjustment for age, years since residency completion, faculty appointment at US News “top 20” medical school, research productivity, NIH grants, clinical trial involvement, and total Medicare payments. Although we found that female allergy faculty had fewer total and first/last author publications, there was no difference in mean publications between academic male and female allergists after similar multivariable adjustment.
There were only 26 full professor female allergists among the 152 full professors in academic Allergy and Immunology. However, the primary multivariable adjusted analysis showed that women were equally likely as men to be a full professor (or full or associate professor as a combined outcome). This finding was stable across sensitivity analyses performed and has not been typical in other medical specialties studied. In-depth analyses of surgery, psychiatry, emergency medicine, cardiology, and infectious diseases identified sex differences in academic rank that persisted despite multivariable adjustments.5,13-15, Although Allergy and Immunology represents a small discipline of academic medicine, it seems to be appropriately advancing female faculty. While there are no corroborative studies in Allergy and Immunology to date, females are well-represented in Allergy and Immunology leadership roles in the U.S. Indeed, based on a survey of AAAAI membership in 2017, 37.1% of Allergy and Immunology’s clinical and division leaders in academic medicine were women (unpublished data, Aidan A. Long, MD). Additionally, females represent over one-third of AAAAI board members and American Board of Allergy and Immunology (ABAI) board of directors.
We found significant unadjusted differences in academic rank and publications between male and female academic allergists, and differences were not explained by age alone. Specifically, the rate of full professorship was 8% lower for female academic allergist adjusted for age only. This suggests that female allergists may lack comparable research opportunities, or alternatively, may be choosing different tracks than male allergists. We found that women comprised 32.6% of allergists and 36.3% of academic allergists. A prior study found that women were generally more likely than men to pursue an academic medical career, but once in academic medicine, women were significantly less likely than men to achieve the next level of professorship.19 Although Allergy and Immunology appears to be doing comparably well attracting and promoting female academicians, similar analyses must be repeated as the proportion of female allergists grows and female academic allergists age.
Factors that may contribute to the observed differences in academic rank and publications between male and female allergists not explained by age include part-time work status, time taken for maternity leave, child-rearing or household duties, and/or type of faculty track. Indeed, a survey suggested that 30% of female allergists worked part-time, while only 15% of male allergists worked part-time.12 Differences in household responsibilities20,21 or work–life balance preferences22 may also contribute to lower publication rates among women, which subsequently leads to reduced likelihood of promotion on research tracks. Prior studies showed that women spend about twice as much time as men on domestic tasks (44% vs 25%), even when their family structure (married with kids, married without kids, single, etc.) is the same.21 Another study found that female physicians with children spent 100.2 minutes (95% CI, 67.0-133.3 minutes) more per day on household activities and childcare than did male physicians.23 Further, it is still unclear if female allergists in academic medicine choose research tracks, and if they have the same opportunities are the same as their male colleagues. For example, a recent study demonstrated that gender gaps in grant funding were attributable to less favorable assessments of women as principal investigators, not of the quality of their proposed research.24 An analysis of funding packages for physician scientists found that men received substantially higher research start-up packages than women, even after adjustment for research productivity.25 Another study found significant perceived differences in access to secretarial support, grant administrators, and statistical support for early career female investigators compared to their male colleagues.26 Recognizing these challenges, some institutions offer grant programs that target female investigators with young children.27-29
The Doximity dataset lacked information on faculty track and part-time status, and may have included voluntary faculty holding assistant, associate, or full professor titles. While we used Medicare reimbursement as a proxy for clinical volume and effort when adjusting for differences in faculty rank and publications, Medicare reimbursements vary and depend on institutional case mix. However, adult academic practices accept Medicare. Although we adjusted for measures of research productivity, important details such as total NIH dollars awarded and the impact factors of journals where allergists published manuscripts included in this analysis were not available. While a recent study found no significant difference in NIH dollars awarded for comparable first-time male and female principal investigators,30 there may be a negative correlation between a journal impact factor and the frequency of female first or last authorship.31 Further, we were unable to consider first authorship separately from last authorship with the available data, and could not meaningfully assess for effect modification by allergist sex. While data from Doximity were previously validated in a large study of faculty rank,5 data inaccuracies are possible. However, any errors would be expected to be nondifferential with respect to allergist sex. Finally, we assessed sex differences in faculty rank at a specific point in time (i.e., 2014), rather than analyzing rates of promotion rates over time, because the Doximity data are cross-sectional. Even so, these data represent the most comprehensive academic Allergy and Immunology workforce analysis to date, and the only available data since the last formal analysis published in 2007.16
In summary, we found no sex difference in academic rank among Allergy and Immunology faculty after multivariable adjustments accounting for physician age, years since residency, faculty appointment at a highly ranked research institution, publications, NIH grants, clinical trial involvement, and total Medicare payments. However, comparisons between female and male academic allergists reveal significant differences in academic rank, publications, and NIH funding that were not attributed simply to allergist age and may reflect a disparity in opportunity, or alternatively, a different choice. Future Allergy and Immunology workforce analyses are warranted to assess sex differences as the sex composition of the Allergy and Immunology workforce changes. Further, subsequent Allergy and Immunology workforce analyses must investigate salary differences in sex, since salary gaps have been previously identified in rigorous studies and this analysis did not consider salary.3 Although policies designed to reduce gender inequality are broadly warranted in academic medicine, Allergy and Immunology is one of the few specialties in which the likelihood of being a full professor appears equal for men and women of similar experience and research productivity.
Supplementary Material
Clinical Implications:
Although disparities in rank exist for women physicians in general, this study found no disparity in academic rank for male and female academic allergists after multivariable adjustment for factors known to influence promotion.
Acknowledgments
Conflict of Interest: Dr. Kimberly G. Blumenthal discloses grant funding from the NIH K01AI125631, the American Academy of Allergy Asthma and Immunology Foundation, and the MGH Claflin Distinguished Scholars Award. Dr. Gross is co-founder of Doximity and reports Doximity employment, stock and stock options. Dr. Neena Kapoor disclosed grant funding from an AUR GE Radiology Research Academic Fellowship Award. Ms. Huebner, Dr. Banerji, Dr. Long, and Dr. Daniel M. Blumenthal have nothing to disclose.
Funding: None
Abbreviations:
- US
United States
- NIH
National Institutes of Health
- AAAAI
American Academy of Allergy, Asthma and Immunology
- NPI
National Provider Identifier
- CI
Confidence Intervals
- ABAI
American Board of Allergy and Immunology
Referesnces
- 1.The State of Women in Academic Medicine: The Pipeline and Pathways to Leadership, 2015-2016. Washington DC, Association of American Medical Colleges; 2019. [cited 2019 January 25]. Available from https://www.aamc.org/members/gwims/statistics/489870/stats16.html. [Google Scholar]
- 2.Reed DA, Enders F, Lindor R, McClees M, Lindor KD. Gender differences in academic productivity and leadership appointments of physicians throughout academic careers. Acad. Med 2011;86(1):43–47. [DOI] [PubMed] [Google Scholar]
- 3.Jena AB, Olenski AR, Blumenthal DM. Sex Differences in Physician Salary in US Public Medical Schools. JAMA Intern Med. 2016;176(9):1294–1304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Shishkova E, Kwiecien NW, Hebert AS, Westphall MS, Prenni JE, Coon JJ. Gender Diversity in a STEM Subfield - Analysis of a Large Scientific Society and Its Annual Conferences. J Am Soc Mass Spectrom. 2017;28(12):2523–2531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Jena AB, Khullar D, Ho O, Olenski AR, Blumenthal DM. Sex Differences in Academic Rank in US Medical Schools in 2014. JAMA. 2015;314(11):1149–1158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Equal Pay/Compensation Discrimination. Washington DC, U.S. Equal Employment Opportunities Commission; 2018. [cited 2018 December 14]. Available from https://www.eeoc.gov/laws/types/equalcompensation.cfm. [Google Scholar]
- 7.Jagsi R, Griffith KA, Stewart A, Sambuco D, DeCastro R, Ubel PA. Gender differences in the salaries of physician researchers. JAMA. 2012;307(22):2410–2417. [DOI] [PubMed] [Google Scholar]
- 8.Jagsi R, Griffith KA, Stewart A, Sambuco D, DeCastro R, Ubel PA. Gender differences in salary in a recent cohort of early-career physician-researchers. Acad. Med. 2013;88(11):1689–1699. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Carr PL, Friedman RH, Moskowitz MA, Kazis LE. Comparing the status of women and men in academic medicine. Ann Internal Med. 1993;119(9):908–913. [DOI] [PubMed] [Google Scholar]
- 10.Kaplan SH, Sullivan LM, Dukes KA, Phillips CF, Kelch RP, Schaller JG. Sex differences in academic advancement. Results of a national study of pediatricians. NEJM. 1996;335(17):1282–1289. [DOI] [PubMed] [Google Scholar]
- 11.Seabury SA, Chandra A, Jena AB. Trends in the earnings of male and female health care professionals in the United States, 1987 to 2010. JAMA Intern Med. 2013;173(18):1748–1750. [DOI] [PubMed] [Google Scholar]
- 12.Medscape Allergist Compensation Report 2018. New York, NY, Medscape; 2018. [cited 2019 January 28]. Available from https://www.medscape.com/slideshow/2018-compensation-allergist-6009649. [Google Scholar]
- 13.Bennett CL, Raja AS, Kapoor N, Kass D, Blumenthal D, Gross N, et al. Gender Differences in Faculty Rank Among Academic Emergency Physicians in the United States. Acad Emerg Med. 2019; 26(3):281–285. [DOI] [PubMed] [Google Scholar]
- 14.Blumenthal DM, Bergmark RW, Raol N, Bohnen JD, Eloy JA, Gray ST. Sex Differences in Faculty Rank Among Academic Surgeons in the United States in 2014. Ann Surg. 2018;268(2):193–200. [DOI] [PubMed] [Google Scholar]
- 15.Blumenthal DM, Olenski AR, Yeh RW, DeFaria Yeh D, Sarma A, Stefanescu Schmidt AC, et al. Sex Differences in Faculty Rank Among Academic Cardiologists in the United States. Circulation. 2017;135(6):506–517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Marshall GD, AAAAI Workforce Committee. The status of US allergy/immunology physicians in the 21st century: a report from the American Academy of Allergy, Asthma & Immunology Workforce Committee. J Allergy Clin Immunol. 2007;119(4):802–807. [DOI] [PubMed] [Google Scholar]
- 17.Kapoor N, Blumenthal DM, Smith SE, Ip IK, Khorasani R. Gender Differences in Academic Rank of Radiologists in U.S. Medical Schools. Radiology. 2017;283(1):140–147. [DOI] [PubMed] [Google Scholar]
- 18.Medicare Provider Utilization and Payment Data: Physician and Other Supplier Data CY 2013. Baltimore, MD, Centers for Medicare & Medicaid Services; 2018. [cited 2018 December 17] Available from https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Medicare-Provider-Charge-Data/Physician-and-Other-Supplier2013.html. [Google Scholar]
- 19.Nonnemaker L. Women physicians in academic medicine: new insights from cohort studies. NEJM. 2000;342(6):399–405. [DOI] [PubMed] [Google Scholar]
- 20.Carr PL, Ash AS, Friedman RH, Scaramucci A, Barnett RC, Szalacha L, et al. Relation of family responsibilities and gender to the productivity and career satisfaction of medical faculty. Ann Internal Med. 1998;129(7):532–538. [DOI] [PubMed] [Google Scholar]
- 21.Jolly S, Griffith KA, DeCastro R, Stewart A, Ubel P, Jagsi R. Gender differences in time spent on parenting and domestic responsibilities by high-achieving young physician-researchers. Ann Internal Med. 2014;160(5):344–353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Dorsey ER. Jarjoura D, Rutecki GW. Influence of Controllable Lifestyle on Recent Trends in Specialty Choice by US Medical Students. JAMA. 2003;290(9):1173–1178. [DOI] [PubMed] [Google Scholar]
- 23.Ly DP, Jena AB. Sex Differences in Time Spent on Household Activities and Care of Children Among US Physicians, 2003–2016. Mayo Clin Proc. 2018;93(10):1484–1487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Witteman HO, Hendricks M, Straus S, Tannenbaum C. Are gender gaps due to evaluations of the applicant or the science? A natural experiment at a national funding agency. Lancet. 2019;393(10171):531–40.30. [DOI] [PubMed] [Google Scholar]
- 25.Sege R, Nykiel-Bub L, Selk S. Sex Differences in Institutional Support for Junior Biomedical Researchers. JAMA. 2015;314(11). [DOI] [PubMed] [Google Scholar]
- 26.Holliday E, Griffith KA, De Castro R, Stewart A, Ubel P, Jagsi R. Gender differences in resources and negotiation among highly motivated physician-scientists. J Gen Intern Med. 2015;30(4):401–407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Claflin Distinguished Scholar Awards. Boston, MA, Massachusetts General Hospital Center for Faculty Development, Office for Women’s Careers; 2019. [cited 2019 January 28] Accessed from https://facultydevelopment.massgeneral.org/owc/claflin.html. [Google Scholar]
- 28.Eleanor and Miles Shore 50th Anniversary Fellowship Program for Scholars in Medicine. Boston, MA, Harvard Medical School Office of Faculty Affairs; 2019. [cited 2019 January 28]. Accessed from https://fa.hms.harvard.edu/shore. [Google Scholar]
- 29.UCSOM Fund to Retain Clinical Scientists (CU-FRCS). Aurora, CO, University of Colorado School of Medicine; 2019. [cited 2019 January 28]. Accessed from http://www.ucdenver.edu/academics/colleges/medicalschool/departments/medicine/GIM/Pages/Now%20Recruiting%20Scholars%20for%20UCSOM%20Fund%20to%20Retain%20Clinical%20Scientists.aspx. [Google Scholar]
- 30.Oliveira DFM, Ma Y, Woodruff TK, Uzzi B. Comparison of National Institutes of Health Grant Amounts to First-Time Male and Female Principal Investigators. JAMA. 2019;321(9):898–900. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Shen YA, Webster JM, Shoda Y, Fine I. Persistent Underrepresentation of Women’s Science in High Profile Journals. bioRxiv; doi: 10.1101/275362 [DOI]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.