

Abstract
Background
The ingestion of grapes or raisins has been reported to cause acute kidney injury (AKI) in dogs, with a clinical picture dominated by early gastrointestinal signs and rapidly developing uremia. Ataxia is mentioned in a few reports, but not further characterized.
Objectives
To evaluate the clinical, laboratory, and pathological features of dogs diagnosed with grape or raisin toxicosis (GRT) with emphasis on renal and neurological manifestations, compared to a control group of dogs with AKI from other causes.
Animals
Fifteen client‐owned dogs with GRT and 74 control dogs.
Methods
Retrospective study over 17 months.
Results
All dogs with GRT were presented with severe AKI (grade 4, n = 5; grade 5, n = 10). Eleven dogs (73%) had marked forebrain, cerebellar, or vestibular signs. These manifestations dominated the clinical picture in some dogs, but were not associated with the severity of azotemia or the presence of systemic hypertension. Eight dogs (53%) survived, and 5 dogs experienced a complete neurological recovery. Causes of death were unrelated to the neurological manifestations. Neuropathological examination of 4 dogs did not identify any structural central nervous system abnormality. Only 2 control dogs (3%) displayed neurological signs with seizures unrelated to the AKI; 42 control dogs (57%) survived.
Conclusions and Clinical Importance
Severe forebrain, cerebellar, or vestibular signs may be an important feature of GRT and dominate the early clinical picture. The described features suggest a reversible functional brain injury specific to GRT and unrelated to uremia.
Keywords: acute kidney injury, ataxia, central nervous system, hemodialysis
Abbreviations
- AKI
acute kidney injury
- BP
systemic blood pressure
- GRT
grape or raisin toxicosis
1. INTRODUCTION
Several reports of dogs developing acute kidney injury (AKI) after ingestion of grapes, raisins, or currants have been published since 1998. 1 , 2 , 3 , 4 , 5 , 6 , 7 , 8 The mechanism of toxicity is still unknown. Hypotheses include contamination of fruits with mycotoxins, heavy metals or pesticides, excess vitamin D, 1 tannin intolerance or excessive ingestion of monosaccharides, 9 hypovolemic shock, and renal ischemia. 4 The exact amount of ingested fruits necessary to cause damage is unknown, and estimations are based on clinical cases. 4 , 5 , 10 The lowest reported dosage to cause AKI is 19.6 g/kg body weight for grapes, and 2.8 g/kg for raisins. 5
Reported clinical signs typically include vomiting within 24 (81% of dogs) to 48 (100% of dogs) hours of ingestion, with vomitus or diarrhea fluid possibly containing grapes or swollen raisins. 5 Other signs were compatible with acute uremia and included anorexia, lethargy, diarrhea, and abdominal pain, as well as oliguria or anuria in 49% of dogs. 1 , 5 Azotemia developed rapidly within 2 days of ingestion. 4 Less frequent signs reported include dehydration, edema, ptyalism, polyuria, polydipsia, hypothermia, hypertension, trembling, seizures, and ataxia in 23% of dogs. Median onset of ataxia was 2 (range, 0.6‐6) days after ingestion of grapes or raisins. It was associated with a negative outcome, and in the only survivor affected, clinical signs of ataxia persisted for 6 days. 5 A case report from Korea describes a Yorkshire Terrier with ataxia that began on the day after grape ingestion. However, the dog died on day 3, and detailed descriptions of neurological signs and associated neuropathology are lacking. 8
In contrast to previous reports, we observed severe neurological signs in the dogs presented to the Small Animal Clinic of the Vetsuisse Faculty Bern, Switzerland, for AKI after grape or raisin toxicosis (GRT), sometimes dominating the clinical picture and confusing the diagnostic evaluation. Our retrospective study had the following aims: First, to evaluate the clinical, laboratory, pathological, and outcome features of dogs diagnosed with GRT compared to dogs diagnosed with AKI of other origin, with emphasis on renal and neurological manifestations; and second, to investigate potential factors for development of neurological signs by comparing dogs with and without central nervous system deficits.
2. MATERIALS AND METHODS
2.1. Dogs and diagnoses
All dogs diagnosed with AKI at the Small Animal Clinic of the Vetsuisse Faculty University of Bern between November 2009 and March 2011 were considered for inclusion. The diagnosis of AKI was based on historical, clinical, laboratory, and imaging results, with ≥2 of the following criteria: (1) presence of renal azotemia with serum creatinine concentration ≥1.7 mg/dL persisting at least 24 hours after correction of prerenal factors; (2) increase in serum creatinine concentration ≥0.3 mg/dL during a 48 hours period in the absence of prerenal factors; (3) persistent pathological oligo‐anuria (<1 mL/kg/h over 6 hours) after volume repletion; and (4) evidence of tubular injury based on renal glucosuria or granular casts on urinalysis. 11 , 12 Acute kidney injury was graded at initial presentation based on the International Renal Interest Society AKI grading system (http://www.iris-kidney.com, last accessed May 10, 2020).
Dogs with AKI were divided into 2 groups, the dogs with AKI associated with GRT (group GRT) and control dogs with AKI associated with other causes (group C). Group GRT included dogs with a history of witnessed ingestion of grapes or raisins and acute onset of vomiting within 48 hours after ingestion. Dogs were excluded if ingestion of grapes or raisins was suspected but not proven. Group C included dogs in which the possibility of an ingestion of grapes or raisins could be definitively ruled out and dogs positively diagnosed with AKI of other causes.
Data of all dogs were collected retrospectively from medical records. Data collected included the expanded history including the time point of grape or raisin ingestion if applicable, physical examination at least once daily, neurological evaluation twice daily during hospitalization in dogs with neurological signs, and measurement of systemic blood pressure (BP) by oscillometric technique (Cardell Veterinary monitor 9403, Midmark Animal Health) according to the American College of Veterinary Internal Medicine (ACVIM) guidelines at least once daily. 13 For the purpose of our study, hypertension was defined as a systolic BP ≥160 mm Hg, which is equivalent to the categories hypertension and severe hypertension with moderate to severe risk of target organ damage based on the most recent ACVIM guidelines. 14 Laboratory results (CBC, serum biochemistry profile, serum ionized calcium concentration, urinalysis from samples obtained by cystocentesis) and diagnostic imaging findings (abdominal ultrasound examination) typically were available from the day of admission and when clinically indicated thereafter. In anuric dogs, urinalysis usually was performed as soon as urine production resumed. Bacteriological culture results of urine were evaluated if available. Serologic testing for leptospirosis was performed by the National Reference Laboratory for Leptospirosis (Institute of Veterinary Bacteriology, National Center for Zoonoses, Bacterial Animal Diseases and Antimicrobial Resistance, Vetsuisse Faculty, University of Bern, Bern, Switzerland) using the microscopic agglutination test (MAT) conducted with a panel of 11 serovars, Leptospira interrogans serovars Australis, Autumnalis, Bataviae, Bratislava, Canicola, Hardjo, Icterohemorrhagiae, Pomona, Sejroe, and Tarassovi, and Leptospira kirschneri serovar Grippotyphosa. The MAT serology was considered diagnostic of leptospirosis in the event of seroconversion with a 4‐fold increase in paired samples taken 2 weeks apart, or with a single MAT titer ≥1:800. 15 In 1 dog, an expanded toxicological screening (Forensic Toxicology, University of Bern, Switzerland) of serum and urine was performed using high pressure liquid chromatography tandem mass spectrometry, gas chromatography screenings and multi‐target screening with liquid chromatography mass spectrometry. 16
2.2. Treatment and outcome
Medical and dialytic treatments were recorded, considering potential association with the progression of neurological signs observed in dogs with GRT. Outcome was defined as discharge from the hospital and 6‐month survival. For nonsurvivors, the main cause of death was defined as renal, neurological, or other. For survivors, the follow‐up of renal and neurological recovery was recorded as available. Necropsy and neuro‐histopathology of dogs with GRT was performed upon owner consent.
2.3. Statistical analyses
Data analyses were performed using commercial software (NCSS 9 Statistical Software, 2013; NCSS, LLC. Kaysville, Utah). A P value of .05 was used as cutoff for statistical significance after Bonferroni correction for multiple comparisons.
Descriptive statistics were performed for signalment, laboratory data, and clinical data. Continuous variables were tested for normality using a Shapiro‐Wilk test. Because multiple variables were not normally distributed, descriptive statistics were reported as median and interquartile range. Categorical variables were reported as absolute numbers and proportions. Clinical and laboratory variables were compared between groups (GRT and C) to evaluate potential characteristics specific for GRT. Clinical and laboratory variables were compared between dogs with and without neurological signs to identify possible associations with the neurological manifestations. Continuous variables were compared using a Mann‐Whitney U test and categorical variables using a Chi‐square or Fisher's exact test.
Because of potential changes associated with dialysis (eg, osmolality, blood pressure), specific details of the dialytic treatments are presented descriptively and separately for the first, second, third, or later treatments. Urea kinetic modeling was performed using Solute Solver Lite online software (http://www.ureakinetics.org) to provide the fractional clearances of urea Kt/V with single‐pool and equilibrated models. 17 The 2 variables reflecting the interdialytic nitrogen and protein metabolism, G (urea generation rate), and nPCR (normalized protein catabolic rate) were calculated using a previously described method for non–steady‐state conditions and irregular schedules. 18
3. RESULTS
3.1. Dogs and diseases
Eighty‐nine dogs with AKI met the inclusion criteria during the study time. Fifteen dogs (17%) were diagnosed with AKI associated with GRT and 74 dogs (83%) with AKI of other origin. The signalment of the dogs is summarized in Table 1.
TABLE 1.
Signalment and diagnosis of the 89 dogs included in the study (15 dogs with grape toxicity, grape or raisin toxicosis [GRT]; 74 control dogs with acute kidney injury [AKI] of other etiology, C)
| Group GRT (n = 15) | Group C (n = 74) | Bonferroni‐corrected P‐value | |
|---|---|---|---|
| Gender | |||
| Male intact | 1 (7%) | 27 (36%) | .03* (male versus female) |
| Male neutered | 3 (20%) | 21 (28%) | |
| Female intact | 2 (13%) | 1 (1%) | .93 (intact versus neutered) |
| Female spayed | 9 (60%) | 25 (34%) | |
| Purebred dogs | 13 (87%) | 65 (88%) | 1.00 |
| # different breeds | 11 | 41 | |
| Age (y) | 3.9 (1.3‐5.6) | 6.6 (2.3‐8.8) | .26 |
| Body weight (kg) | 16.7 (9.9‐27.0) | 20.1 (11.6‐32.1) | 1.00 |
| Diagnosis | |||
| Leptospirosis | 54 (73%) | ||
| Toxic nephrosis a | 2 (3%) | ||
| Polysystemic disease b | 4 (5%) | ||
| Unknown | 14 (19%) |
Toxic nephrosis: gentamicin, NSAID.
Polysystemic disease: acute pancreatitis, snake envenomation, Babesia canis infection, postsurgery.
Statistically significant (P < .05).
All dogs in group GRT had a known history of ingestion of grapes or raisins within 72 hours before presentation. Material ingested included raisins in 2 dogs, grape marc (skins, seeds, and stems of grapes used for wine production) utilized as a natural fertilizer for grassland in 3 dogs, grapes from compost in 1 dog, and fresh grapes in the other 9 dogs. The exact amount of fruit ingested could not be determined. In group C, a diagnosis was made in 60/74 dogs (81%, Table 1). In the remaining 14 dogs (19%), the etiology of AKI was unknown, but exposure to grapes or raisins was considered impossible by the owners.
Physical examination at presentation and during hospitalization of group GRT identified lethargy (15/15), vomiting (15/15), diarrhea (8/15), hematochezia (3/15), oligoanuria (15/15), and hypothermia (15/15). Eleven dogs (73%) in group GRT had marked neurological signs at presentation. Therefore, neurological examination by a board‐certified neurologist was performed in 8 dogs. The remaining dogs were examined by board‐certified internists and results discussed with the neurologists.
3.2. Neurological manifestations
The neurological examination at presentation identified mildly (n = 2) to severely (n = 5) impaired consciousness, kyphotic posture (n = 1), pleurothotonus (n = 1), head tilt (n = 1), generalized tremor (n = 2), generalized ataxia (n = 9, in 1 dog only intermittent), mild ambulatory tetraparesis (n = 1), drifting (n = 3), and hypermetric gait (n = 2). Postural reactions were normal in all but 1 dog. Cranial nerve examination identified bilaterally decreased menace response (n = 2), anisocoria (n = 1), positional ventral strabismus (n = 2), and decreased nasal sensation (n = 1). One dog had mildly decreased segmental spinal reflexes. Additionally, 1 dog had a seizure during hospitalization. None of the dogs had evident pain.
Based on these findings, the neuroanatomical localization of the lesion was considered multifocal intracranial: forebrain (possibly thalamus) with or without cerebellum in 10 dogs, and peripheral vestibular system in 1 dog.
Neurological signs worsened initially in 6/11 dogs, and regressed over 2 to 20 days. For most dogs, neurological improvement was markedly slower than improvement of renal function. Six of 11 dogs (55%) with neurological signs survived and experienced complete neurological recovery. Five dogs (45%) were euthanized for non‐neurological reasons within 1 to 4 days after presentation, at a time where they still were experiencing neurological deficits.
In group C, only 2/74 dogs (3%) had neurological signs, manifested as seizures. One of these 2 dogs previously had been diagnosed with idiopathic epilepsy, and the other was hypoglycemic as a consequence of acute liver failure, associated with leptospirosis. Mildly impaired consciousness attributed to uremia was observed in some of the other 72 control dogs. However, in contrast to the deficits observed in the dogs with GRT, their lethargy resolved rapidly with improvement of azotemia.
3.3. Blood pressure, laboratory, and imaging evaluation
Systemic BP at presentation and the proportion of hypertensive dogs was significantly lower in dogs with GRT than in controls (P = .05 and .04, respectively; Table 2). Five of the 6 hypertensive dogs with GRT had neurological abnormalities, which persisted despite successful BP control after treatment with amlodipine besylate (Amlodipin Mepha, Mepha Pharma AG, Switzerland) 0.25 to 0.75 mg/kg PO q24h in 4 dogs and with correction of fluid overload by dialysis in 1 dog.
TABLE 2.
Relevant clinical and laboratory variables at presentation for the 89 dogs included in the study (15 dogs with grape toxicosis, GRT; 74 control dogs with AKI of other etiology, C)
| N = (GRT/C) | Group GRT (n = 15) | Group C (n = 74) | RR | Bonferroni‐corrected P‐value | |
|---|---|---|---|---|---|
| Systolic blood pressure (mm Hg) | 144 (129‐174) | 170 (150‐192) | 100‐140 | .05* | |
| Normotension | 6/15 (40%) | 10/72 (14%) | |||
| Prehypertension | 3/15 (20%) | 13/72 (18%) | |||
| Hypertension | 4/15 (27%) | 21/72 (29%) | |||
| Severe hypertension | 2/15 (13%) | 28/72 (39%) | |||
| Laboratory | |||||
| Hematocrit (L/L) | 11/72 | 0.40 (0.34‐0.42) | 0.31 (0.27‐0.37) | 0.39‐0.57 | .22 |
| WBC (109/L) | 11/72 | 13.2 (8.7‐14.7) | 15.7 (12.5‐22.6) | 6.0‐12.0 | 1.00 |
| Platelets (109/L) | 10/72 | 196 (119‐236) | 158 (83‐222) | 150‐400 | 1.00 |
| PT (s) | 13/69 | 7.8 (7.2‐8.2) | 7.9 (7.3‐8.7) | 6.3‐8.5 | 1.00 |
| aPTT (s) | 13/69 | 12.3 (11.2‐13.2) | 13.7 (12.1‐16.3) | 9.6‐16.1 | .20 |
| Fibrinogen (mg/L) | 13/68 | 196 (167‐409) | 398 (211‐581) | 150‐300 | .50 |
| Creatinine (mg/dL) | 15/74 | 12 (9.2‐16.1) | 9.1 (5.8‐11.9) | 0.6‐1.4 | .52 |
| Urea (mg/dL) | 15/74 | 172 (112‐184) | 162 (108‐207) | 10‐31 | 1.00 |
| Ca total (mg/dL) | 15/74 | 13.2 (10.7‐14.9) | 10.2 (9.3‐11.2) | 10‐11.8 | .002* |
| Ca ionized (mmol/L) | 11/36 | 1.3 (1.1‐1.3) | 1.1 (1.0‐1.2) | 1.0‐1.4 | 1.00 |
| Phos (mg/dL) | 15/74 | 12.2 (9.3‐18.9) | 13 (8.6‐17.7) | 2.9‐6 | 1.00 |
| Ca × Phos (mmol2/L2) | 15/74 | 12.3 (9.7‐20.1) | 10.3 (7.5‐15.6) | <4.7 | 1.00 |
| Na+ (mEq/L) | 15/74 | 140 (139‐141) | 141 (137‐144) | 144‐155 | 1.00 |
| K+ (mEq/L) | 15/74 | 6.2 (5.6‐8.5) | 4.6 (3.6‐6.3) | 4.1‐5.3 | .01* |
| Glucose (mg/dL) | 11/71 | 110 (90‐119) | 108 (94‐117) | 72‐117 | 1.00 |
| Bilirubin (mg/dL) | 11/70 | 0.31 (0.27‐0.34) | 0.32 (0.2‐0.9) | 0.04‐0.25 | 1.00 |
| pH | 11/36 | 7.25 (7.24‐7.32) | 7.30 (7.25‐7.33) | 7.33‐7.51 | 1.00 |
| HCO3 − (mEq/L) | 9/36 | 16.1 (14.7‐18.6) | 16.5 (14.1‐18.5) | 18.4‐26.3 | 1.00 |
| pCO2 (mm Hg) | 10/36 | 37.3 (34‐39) | 34 (31.1‐38.5) | 25.2‐45.4 | 1.00 |
| AG (mEq/L) | 11/36 | 25.6 (23.1‐33.8) | 28.4 (22.8‐32.2) | 10.8‐19.3 | 1.00 |
| IRIS AKI grading | |||||
| Grade 2 | 0 | 2 (3%) | |||
| Grade 3 | 0 | 13 (18%) | |||
| Grade 4 | 5 (33%) | 30 (41%) | |||
| Grade 5 | 10 (67%) | 29 (39%) | |||
| RRT | 12 (80%) | 46 (62%) | .48 | ||
| Oligoanuria | 15 (100%) | 46/72 (64%) | .05 |
Notes: Blood pressure was classified based on the IRIS recommendations: systolic blood pressure <140 mm Hg, normotension; 140‐159 mm Hg, prehypertension, 160‐179 mm Hg, hypertension; ≥180 mm Hg, severe hypertension. The grade of AKI at presentation was defined based on the IRIS recommendations: serum creatinine <140 μmol/L, grade 1; 140‐219 μmol/L, grade 2; 220‐439 μmol/L, grade 3; 440‐879 μmol/L, grade 4; ≥880 μmol/L, grade 5.
Abbreviations: AG, anion gap; AKI, acute kidney injury; aPTT, activated partial thromboplastin time; GRT, grape or raisin toxicosis; IRIS, International Renal Interest Society; PT, prothrombin time; RR, reference range; RRT, renal replacement treatment; WBC, white blood cell count.
Statistically significant (P < .05).
Relevant laboratory variables and AKI grading for both groups at presentation are presented in Table 2. In summary, serum potassium concentration was higher in the GRT group, likely reflecting somewhat more severe renal impairment, with a higher proportion of dogs with oligoanuria than observed in control dogs. The most distinctive feature of GRT was the markedly higher serum total calcium concentration with similar serum phosphorus and ionized calcium concentrations, compared to C group (Figure 1). No obvious difference was observed in laboratory findings between dogs with or without neurological signs in group GRT (Table 3) and no obvious association was found between the severity of azotemia and the severity of neurological signs.
FIGURE 1.
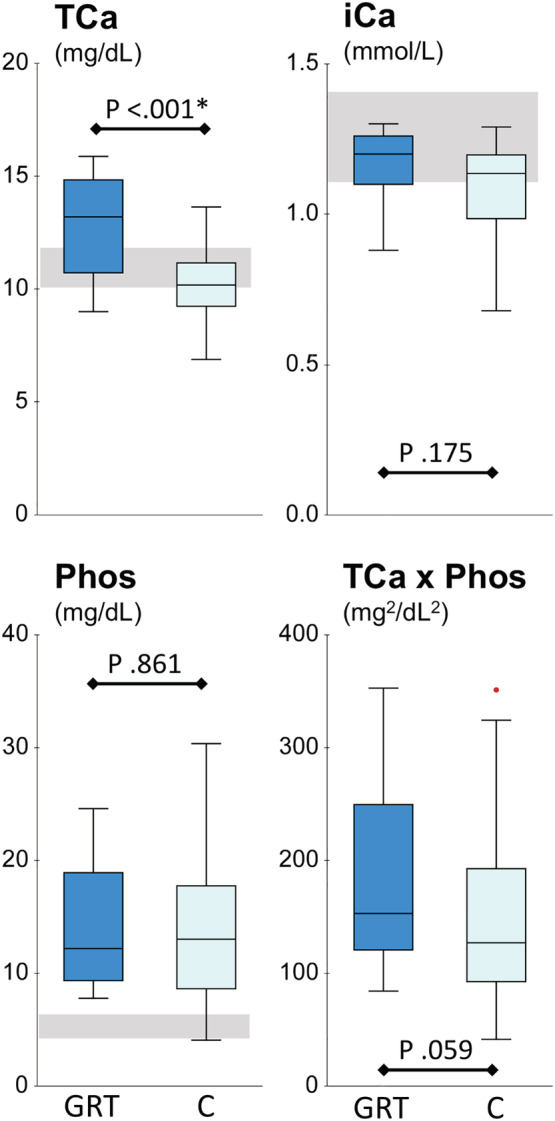
Comparison of the laboratory variables characterizing the calcium phosphorus disturbances among 15 dogs with acute kidney injury (AKI) from grape or raisin toxicosis (GRT) and 74 control dogs with AKI from other causes (C)
TABLE 3.
Relevant clinical and laboratory for the 15 dogs diagnosed with AKI because of grape or raisin toxicosis (GRT), stratified upon the presence of neurological manifestations. Blood pressure was recorded on the day of presentation based on 3 to 5 consecutive measurements
| N = neuro/non‐neuro | GRT with neurological signs (n = 11) | GRT without neurological signs (n = 4) | RR | |
|---|---|---|---|---|
| Systolic blood pressure (mm Hg) | 158 (133‐174) | 130 (122‐174) | 100‐140 | |
| Normotension | 3/11 (27%) | 3/4 (75%) | ||
| Prehypertension | 3/11 (27%) | 0/4 (0%) | ||
| Hypertension | 4/11 (36%) | 0/4 (0%) | ||
| Severe hypertension | 1/11 (9%) | 1/4 (25%) | ||
| Laboratory | ||||
| Hematocrit (L/L) | 9/2 | 0.39 (0.34‐0.43) | 0.41 (0.40‐0.42) | 0.39‐0.57 |
| WBC (109/L) | 9/2 | 11.9 (8.5‐19) | (14.7‐14.7) | 6.0‐12.0 |
| Platelets (109/L) | 8/2 | 205 (134‐257) | 151 (107‐195) | 150‐400 |
| Creatinine (mg/dL) | 11/4 | 12 (7.2‐12.8) | 13.5 (9.3‐19.1) | 0.6‐1.4 |
| Urea (mg/dL) | 11/4 | 172 (112‐186) | 165 (114‐180) | 10‐31 |
| Ca total (mg/dL) | 11/4 | 13.2 (10.7‐15.3) | 12.6 (10.4‐13.8) | 10‐11.7 |
| Ca ionized (mmol/L) | 11/2 | 1.2 (1‐1.3) | (1.3‐1.3) | 1.1‐1.4 |
| Phos (mg/dL) | 11/4 | 11.4 (9.3‐19.8) | 14.2 (9.7‐16.4) | 2.9‐6 |
| Ca × Phos (mmol2/L2) | 11/4 | 12.3 (9.5‐21.2) | 12.7 (9.8‐17.3) | <4.7 |
| Na+ (mEq/L) | 11/4 | 140 (138‐142) | 140 (139‐141) | 144‐155 |
| K+ (mEq/L) | 11/4 | 6.2 (5.8‐8.5) | 5.7 (4.7‐8) | 4.1‐5.3 |
| Glucose (mg/dL) | 9/2 | 110 (90‐119) | 86 (81‐90) | 72‐117 |
| Bilirubin (mg/dL) | 9/2 | 0.3 (0.3‐0.4) | 0.3 (0.3‐0.3) | 0.04‐0.2 |
| pH | 10/1 | 7.28 (7.25‐7.33) | (7.09) | 7.33‐7.51 |
| HCO3 − (mEq/L) | 8/1 | 16.5 (14.6‐18.7) | (15.1) | 18.4‐26.3 |
| pCO2 (mm Hg) | 9/1 | 36.8 (33.7‐37.8) | (50.6) | 25.2‐45.4 |
| AG (mEq/L) | 10/1 | 26.1 (23.1‐34.0) | (25.1) | 10.8‐19.3 |
Abbreviations: AG, anion gap; AKI, acute kidney injury; RR, reference range; WBC, white blood cell count.
Toxicological analysis of blood and urine of 1 dog with GRT and neurological signs identified traces of alcohol, including 0.3 mg/L ethyl glucuronide and 0.2 mg/L ethyl sulfate, but no other toxic substances. This sample was taken at presentation, but 4 days after ingestion of grapes.
Indirect intracranial pressure assessment using transcranial Doppler sonography was performed in 1 dog with progressive neurological signs and normal BP. 19 The resistive index was 0.80 for the basilar artery (normal ≤0.66) and 0.89 for the middle cerebral artery (normal ≤0.58), suggesting increased intracranial pressure.
3.4. Treatment
Treatment strategy was identical in both groups of dogs. Twelve of 15 dogs (80%) in group GRT were treated by hemodialysis, compared to 46/74 dogs (62%) for group C. Relevant specifics of the dialysis treatment for dogs with GRT are summarized in Table 4. Medications administered to dogs of this group included balanced electrolyte solutions, amoxicillin‐clavulanic acid (n = 11), metronidazole (n = 3), enrofloxacin (n = 3), doxycycline (n = 1), ranitidine (n = 11), omeprazole (n = 3), dolasetron (n = 9), maropitant (n = 6), buprenorphine (n = 9), methadone (n = 2), furosemide (n = 4), amlodipine (n = 4), salicylate (n = 1), diazepam (n = 1), phenobarbital (n = 1), dexamethasone (n = 1), 25% glucose (n = 2), darbepoeitin (n = 1), sodium bicarbonate (n = 1), and mannitol (n = 12).
TABLE 4.
Main variables describing the 54 hemodialysis treatments in 12 dogs with AKI because of ingestion of grapes or raisins
| Tx1 n = 12 | Tx2 n = 12 | Tx3 n = 11 | Tx>3 n = 19 | |
|---|---|---|---|---|
| N treatments/dog | 4 (3‐5) | |||
| Dialysis modality | ||||
| HD | 10 (83%) | 7 (58%) | 6 (55%) | 15 (79%) |
| HDF | 2 (17%) | 5 (42%) | 5 (45%) | 4 (21%) |
| Anticoagulation | ||||
| SH | 6 (50%) | 6 (50%) | 5 (45%) | 13 (68%) |
| RCA | 6 (50%) | 6 (50%) | 6 (55%) | 6 (32%) |
| Td (min) | 111 (90‐123) | 160 (148‐191) | 207 (183‐220) | 210 (180‐265) |
| Qp (L/kg) | 372 (309‐414) | 692 (608‐1018) | 1272 (1021‐1391) | 1596 (1374‐1769) |
| Qb (mL/min/kg) | 3.3 (3.1‐4.1) | 4.6 (3.7‐6.4) | 6.1 (5.1‐7.0) | 7.4 (5.8‐8.5) |
| ΔBW (%) | 0.92 (0.00 to 1.64) | 0.85 (−1.30 to 2.70) | 0.38 (−1.23 to 1.11) | 0.41 (−1.40 to 1.39) |
| UF (mL/kg) | 11.6 (1.5‐20.9) | 19.1 (0.3‐35.0) | 30.3 (0.3‐47.5) | 49.3 (12.5‐63.4) |
| CrRR | 0.33 (0.27‐0.38) | 0.51 (0.44‐0.55) | 0.65 (0.64‐0.68) | 0.70 (0.67‐0.77) |
| URR | 0.39 (0.33‐0.44) | 0.57 (0.43‐0.64) | 0.75 (0.71‐0.79) | 0.83 (0.80‐0.87) |
| spKt/V | 0.50 (0.42‐0.61) | 0.93 (0.56‐1.19) | 1.67 (1.53‐1.92) | 1.99 (1.72‐2.26) |
| eKt/V | 0.37 (0.33‐0.50) | 0.76 (0.47‐1.02) | 1.43 (1.29‐1.63) | 1.71 (1.45‐2.00) |
| G (mg/min) | 4.19 (2.20‐5.28) | 2.35 (1.61‐3.73) | 2.70 (1.85‐4.20) | 2.40 (1.55‐3.21) |
| nPCR (g/kg/d) | 1.86 (1.36‐2.82) | 1.35 (1.03‐1.81) | 1.19 (0.98‐1.84) | 1.04 (0.81‐1.25) |
Abbreviations: ΔBW, change in body weight; CrRR, creatinine reduction ration; eKt/V, fractional clearance of the urea distribution volume (equilibrated values); G, urea generation rate; nPCR, normalized protein catabolic rate; Qb, blood flow rate; Qp, volume of blood processed; spKt/V, fractional clearance of the urea distribution volume (single‐pool kinetic model); Td, duration of the dialysis treatment; UF, ultrafiltration volume; URR, urea reduction ratio.
3.5. Outcome
Eight dogs (53%) of group GRT survived and were discharged from the hospital. Of these, 5 had neurological signs during the acute phase of illness and experienced complete neurological recovery. Seven dogs were discharged with partial renal recovery (serum creatinine concentration <3.05 mg/dL) and 1 dog with normal renal function test results. Six of the 7 nonsurvivors had neurological signs, but died or were euthanized for renal‐related reasons (n = 4) or other non‐neurological causes (n = 3), 2 of them while still dialysis‐dependent. Follow‐up by phone was performed for the 8 survivors of group GRT, which all were still alive 9 to 13 months after discharge from the hospital. In 6 dogs, serum creatinine and urea concentrations were within normal limits at the last reevaluations with their referring veterinarians, and in 2 dogs, the owners had declined further blood reevaluations since discharge with mildly increased renal function test results (serum creatinine concentrations 2.99 mg/dL and 1.58 mg/dL, respectively).
In comparison, 42/74 dogs (57%) in group C survived and were discharged. Nonsurvivors died or were euthanized for renal‐related reasons (n = 10) or nonrenal related causes (n = 22). None of the dogs was euthanized because of neurological problems. Seventeen of the 32 nonsurvivors were still dialysis‐dependent at the time of death or euthanasia.
3.6. Pathology
Necropsy was performed in 4 dogs with GRT and neurological signs, and a kidney biopsy sample was obtained from an additional dog with GRT. The findings indicated acute renal tubular necrosis consistent with grape toxicosis. 6 In 1 dog, histopathological examination showed multifocal to confluent degeneration and necrosis of tubular epithelium and concurrent multifocal mild tubular regeneration. Many epithelial cells contained intracytoplasmic golden brown pigment and numerous tubular lumina contained eosinophilic granular casts (Figure 2A). One dog with severely increased calcium × phosphorus product of 28.5 (mmol/L)2 had severe diffuse metastatic calcification of proximal tubules within the renal cortex, whereas medullary tubules were spared. Severe diffuse calcification also was noted in the alveolar walls of the lungs and was associated with hyperemia and multifocal hemorrhages (Figure 2B). Similar findings of severe mineralization of the proximal tubules were observed in a second dog with mild to moderate hypercalcemia.
FIGURE 2.
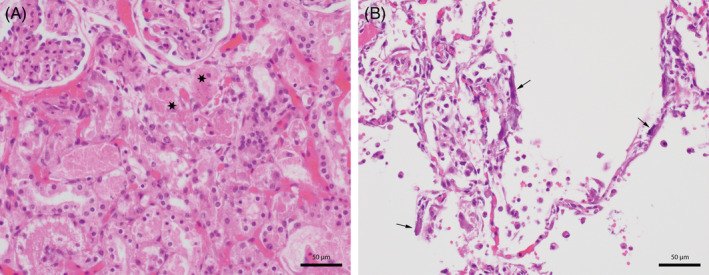
Histopathology of the kidney (3A) and lung (3B) of a dog with acute kidney injury (AKI) from grape or raisin toxicosis. A, Kidney: lumina of tubules contain eosinophilic proteinaceous material admixed with sloughed and necrotic epithelial cells (stars). HE stain, ×400. B, Lung: alveolar walls are mineralized (arrows), free erythrocytes, and many macrophages can be seen in the alveolar space
Neurohistopathological examination of the brain and spinal cord was unremarkable in all 4 dogs examined. None of them had been hypertensive.
4. DISCUSSION
Ingestion of grapes or raisins is known to cause AKI in some dogs. 1 , 2 , 3 , 4 , 5 , 6 , 7 Based on our findings, neurological signs of variable severity, when present, are mainly localized to the forebrain (presumptively thalamus) and cerebellum and seem to be an important feature in >75% of the dogs. These neurological manifestations may even dominate the early clinical picture and confuse the initial diagnostic evaluation.
To date, the toxic agent causing renal damage is still unknown, as is the pathogenesis of the neurological manifestations. Whether the impairment of both organ systems is caused by the same toxin or pathophysiology is therefore unclear. Other potential causes for neurological involvement including severe uremia, systemic hypertension, electrolyte and metabolic derangements, adverse drug effects, and structural damage to the central nervous system with hemorrhage or thromboses were investigated in our study.
Uremic encephalopathy is a well‐described entity in human medicine, resulting in complex mental changes and motor disturbances, 20 whereas similar publications in the veterinary literature are sparse. 21 , 22 The pathophysiology seems to be multifactorial, including accumulation of protein degradation products, such as guanidine and methylguanidine, that possibly act as uremic neurotoxins. Other factors include malfunction of intermediary metabolism, hormonal disturbances, and imbalance between excitatory and inhibitory neurotransmitters. 23 , 24 , 25 In particular, secondary hyperparathyroidism may contribute to the pathogenesis of uremic encephalopathy. In humans with renal failure, calcium concentration in the brain is increased, likely because of altered parathyroid hormone‐sensitive calcium transport within neurons. Increased cellular calcium may cause neuro‐excitation and possibly contribute to clinical signs of encephalopathy. 20
Similar to a previous study, dogs of group GRT showed a statistically significant increase in serum calcium concentration compared to control dogs. 5 This increase was limited to the total serum calcium concentration and did not include the ionized fraction. Because serum albumin concentration was not different from that of the control dogs (data not shown), this finding suggests accumulation of calcium complexed to unidentified anions not reflected in the anion gap. This increase of serum calcium concentration in dogs with GRT may have led to severe calcification of the renal tubules and the alveolar walls observed on histopathology. Apart from these structural changes, hypercalcemia may have contributed to functional hemodynamic disturbances in the kidney by vasoconstriction of the afferent arteriole in the glomeruli, although this effect would rather be expected with ionized hypercalcemia. 26
A potential role for hypercalcemia in the neurological manifestations is difficult to evaluate with the available data. The serum calcium concentrations were not strikingly different between dogs with or without neurological signs, and mineralization was not detectable in the central nervous system of the examined dogs with neurological signs. However, a nonstructural effect of the hypercalcemia leading to brain dysfunction cannot be excluded.
Other electrolyte disturbances including potassium, sodium, chloride, and phosphorus were not significantly different between the groups, and thus unlikely to be a causative factor for the neurological manifestations.
The neurological signs could be directly caused by a component or metabolite of grapes and raisins. The trace amount of alcohol found in 1 dog with GRT caused by grape marc ingestion likely developed during the fermention process but was too low to directly cause the neurological signs observed, especially for the duration of several days.
All dogs with GRT developed oligoanuric AKI with severe azotemia. However, the difference in the severity of renal impairment between the groups was minimal and none of the control dogs showed neurological signs attributable to uremia other than mild transient impaired mentation. Additionally, no structural lesion was observed in the brain compatible with secondary uremic changes such as myelin vacuolization as described in a goat. 21 It is thus unlikely that the neurological manifestations observed in these dogs after GRT are caused by uremic encephalopathy.
Dialysis‐related neurological signs such as dialysis disequilibrium were excluded because all but 1 dog showed neurological signs at the time of presentation before initiation of extracorporeal blood purification treatment. 23 Similarly, aluminum hydroxide toxicosis can be ruled out as a contributing factor, because this phosphorus binder was only administered after the onset of neurological signs and only in a subset of dogs. 27 Other medications administered before referral or during hospitalization for treatment of AKI were not different between the 2 groups or between dogs with and without neurological manifestation, which makes direct drug toxicosis or drug interactions very unlikely.
Systemic hypertension is a well‐known cause of renal failure in human and veterinary medicine and it may lead to infarctions or hemorrhages in the central nervous system. 13 In our study, systemic hypertension with a moderate to severe risk of target organ damage was present in 6/15 dogs (40%) of the group GRT. Five of these 6 dogs had neurological signs, and these persisted in all of them despite successful medical control of their blood pressure. Furthermore, control dogs overall were more hypertensive than dogs with GRT and without showing neurological signs. Systemic hypertension therefore seems unlikely to be a causative factor for the neurological signs of dogs with GRT. In humans with renal failure, hypertensive encephalopathy occurs in approximately 5% of cases, and is thought to be caused by vasogenic edema predominantly in the caudal areas of the brain because of impaired cerebrovascular autoregulation, increased plasma concentrations of natriuretic peptides and endothelial injury. 23 The high resistive index of the cerebral vessels observed in 1 dog possibly indicates increased intracranial pressure in this dog and warrants more systematic assessment in the future.
Summarizing the various individual causes for neurological signs, we cannot exclude that some of them, although not alone responsible for the neurological disturbances, may have aggravated the primary cause. Hemodialysis may have the potential to increase the intracranial pressure, and therefore special caution is mandatory while writing the treatment prescription. Also, analgesics may have a stronger effect in uremic patients compared to normal dogs, and hence worsen the lethargy observed.
Overall, the short‐term survival rate of 53% in dogs with AKI after GRT in our study is comparable to that of previous reports and similar to the survival rate of 57% in the control dogs with other causes of AKI. 5 To our knowledge, ours is the first report of long‐term outcome in dogs with GRT with nearly complete renal recovery in survivors >6 months after discharge. Also, treatment of GRT‐induced AKI has not been reported in a large number of cases so far, including dialysis treatments.
More than 75% of the dogs with GRT showed severe neurological signs, which were reversible in all dogs that survived. The remaining dogs were still neurologically abnormal by the time of euthanasia or death. It therefore is not clear that the neurological manifestations are always reversible, but based on the short survival time of the nonsurviving dogs that were still neurologically abnormal, they likely did not have enough time to regain normal neurological status before death.
The main limitations of our study include a low number of dogs with GRT and the 2 dogs lost to follow‐up for long‐term outcome. However, in our opinion, the severity of neurological signs in the affected dogs and the intensive staging, monitoring, treatment and follow‐up of all patients with renal disease at our facility, strengthen the value of our study. Other limitations include the low number of GRT dogs that underwent neuropathological examination because of owner constraints, as well as the fact that most control dogs were diagnosed with leptospirosis (73%), which is a systemic infection with various organ manifestations in addition to renal function impairment. However, despite the fact that central nervous system involvement is described with leptospirosis, only 2 of the control dogs with leptospirosis had neurological signs. 28 One dog suffered from hypoglycemia because of leptospirosis‐associated liver failure, and the other dog was previously diagnosed with idiopathic epilepsy.
In conclusion, neurological signs seem to be an important feature of GRT in some dogs and they even may dominate the early clinical picture of this toxicosis before signs of uremia emerge. It thus should be an important differential diagnosis along with ethylene glycol poisoning in dogs presenting with severe gastrointestinal and neurological signs. Importantly, neurological signs seem to be reversible and unrelated to the severity of uremia, the presence of systemic hypertension, electrolyte disorders, or other metabolic derangements. The absence of structural changes and the reversibility of the signs suggest functional brain alterations. The pathophysiology of this neurological dysfunction still could include direct neurotoxicity, consequences of disturbances in calcium metabolism, or increased intracranial pressure, which should be addressed in future studies.
CONFLICT OF INTEREST DECLARATION
Authors declare no conflict of interest.
OFF‐LABEL ANTIMICROBIAL DECLARATION
Authors declare no off‐label use of antimicrobials.
INSTITUTIONAL ANIMAL CARE AND USE COMMITTEE (IACUC) OR OTHER APPROVAL DECLARATION
Approved by the ethical committee at the University of Bern.
HUMAN ETHICS APPROVAL DECLARATION
Authors declare human ethics approval was not needed for this study.
ACKNOWLEDGMENTS
The authors thank Dr Mark Neer, Oklahoma State University, for his valuable input in the diagnostic workup and treatment, Prof Wolfgang Weinmann, Forensic Toxicology, University of Bern, Switzerland, for the toxicological analysis, and the Robmar Foundation for the human animal bond, Switzerland, for financial support of the nephrology service and hemodialysis unit at the Vetsuisse Faculty, University of Bern, Small Animal Teaching Hospital.
Schweighauser A, Henke D, Oevermann A, Gurtner C, Francey T. Toxicosis with grapes or raisins causing acute kidney injury and neurological signs in dogs. J Vet Intern Med. 2020;34:1957–1966. 10.1111/jvim.15884
Funding information Robmar Foundation
REFERENCES
- 1. Gwaltney‐Brant S, Holding JK, Donaldson CW, et al. Letters to the editor: renal failure associated with ingestion of grapes or raisins in dogs. J Am Vet Med Assoc. 2001;218:1553‐1554. [PubMed] [Google Scholar]
- 2. Penny D, Henderson SM, Brown PJ. Raisin poisoning in a dog. Vet Rec. 2003;152:308. [PubMed] [Google Scholar]
- 3. Campbell A, Bates N. Raisin poisoning in dogs. Vet Rec. 2003;152:376. [PubMed] [Google Scholar]
- 4. Mazzaferro EM, Eubig PA, Hackett TB, et al. Acute renal failure associated with raisin or grape ingestion in 4 dogs. J Vet Emerg Crit Care. 2004;14:203‐212. [Google Scholar]
- 5. Eubig PA, Brady MS, Gwaltney‐Brant SM, Khan SA, Mazzaferro EM, Morrow CM. Acute renal failure in dogs after the ingestion of grapes or raisins: a retrospective evaluation of 43 dogs (1992–2002). J Vet Intern Med. 2005;19:663‐674. [DOI] [PubMed] [Google Scholar]
- 6. Morrow CMK, Valli VE, Volmer PA, Eubig PA. Canine renal pathology associated with grape or raisin ingestion: 10 cases. J Vet Diagn Invest. 2005;17:223‐231. [DOI] [PubMed] [Google Scholar]
- 7. Stanley SW, Langston CE. Hemodialysis in a dog with acute renal failure from currant toxicity. Can Vet J. 2008;49:63‐66. [PMC free article] [PubMed] [Google Scholar]
- 8. Yoon SS, Byun JW, Kim MJ, et al. Natural occurrence of grape poisoning in two dogs. J Vet Med Sci. 2011;73:275‐277. [DOI] [PubMed] [Google Scholar]
- 9. Singleton VL. More information on grape or raisin toxicosis. J Am Vet Med Assoc. 2001;219:434‐436. [PubMed] [Google Scholar]
- 10. Sutton NM, Bates N, Campbell A. Factors influencing outcome of Vitisvinifera intoxication in dogs (grapes, raisins, currants and sultanas). Vet Rec. 2009;164:430‐431. [DOI] [PubMed] [Google Scholar]
- 11. Cowgill LD, Langston CA. Acute kidney insufficiency In: Bartges J, Polzin DJ, eds. Nephrology and Urology of Small Animals. West Sussex, UK: John Wiley & Sons Ltd; 2011:472‐523. [Google Scholar]
- 12. Holloway A, O'Brien R. Perirenal effusion in dogs and cats with acute renal failure. Vet Radiol Ultrasound. 2007;48:574‐579. [DOI] [PubMed] [Google Scholar]
- 13. Brown S, Atkins C, Bagley R, et al. Guidelines for the identification, evaluation and management of systemic hypertension in dogs and cats. J Vet Intern Med. 2007;21:542‐558. [DOI] [PubMed] [Google Scholar]
- 14. Acierno MJ, Brown S, Coleman AE, et al. ACVIM consensus statement: guidelines for the identification, evaluation, and management of systemic hypertension in dogs and cats. J Vet Intern Med. 2018;32:1803‐1822. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Fraune CK, Schweighauser A, Francey T. Evaluation of the diagnostic value of serologic microagglutination testing and a polymerase chain reaction assay for diagnosis of acute leptospirosis in dogs in a referral center. J Am Vet Med Assoc. 2013;242:1373‐1380. [DOI] [PubMed] [Google Scholar]
- 16. Maurer HH, Pfleger K, Weber AA. Mass Spectral and GC Data of Drugs, Poisons, Pesticides, Pollutants and their Metabolites. Weinheim, Germany: Wiley‐VCH; 2007. [Google Scholar]
- 17. Daugirdas JT, Depner TA, Greene T, Silisteanu P. Solute‐solver: a web‐based tool for modeling urea kinetics for a broad range of hemodialysis schedules in multiple patients. Am J Kidney Dis. 2009;54:798‐809. [DOI] [PubMed] [Google Scholar]
- 18. Casino FG, Marshall MR. Simple and accurate quantification of dialysis in acute renal failure patients during either urea non‐steady state or treatement with irregular or continuous schedules. Nephrol Dial Transplant. 2004;19:1454‐1466. [DOI] [PubMed] [Google Scholar]
- 19. Duque FJ, Dominguez‐Roldan JM, Ruiz P, Zaragoza C, Barrera‐Chacon R. Assessing circle of Willis blood circulation in dogs with transcranial color‐coded duplex sonography. Vet Radiol Ultrasound. 2009;50:530‐535. [DOI] [PubMed] [Google Scholar]
- 20. Seifert JL, Samuels MA. Uremic encephalopathy and other brain disorders associated with renal failure. Semin Neurol. 2011;31:139‐143. [DOI] [PubMed] [Google Scholar]
- 21. Radi ZA, Thomsen BV, Summers BA. Renal (uremic) encephalopathy in a goat. J Vet Med A Physiol Pathol Clin Med. 2005;52:397‐400. [DOI] [PubMed] [Google Scholar]
- 22. Wolf AM. Canine uremic encephalopathy. J Am Anim Hosp Assoc. 1980;16:735‐738. [Google Scholar]
- 23. Brouns R, De Deyn PP. Neurological complications in renal failure: a review. Clin Neurol Neurosurg. 2004;107:1‐16. [DOI] [PubMed] [Google Scholar]
- 24. Vanholder R, De Smet R, Glorieux G, et al. European uremic toxin work group. Review on uremic toxins: classification, concentration, and interindividual variability. Kidney Int. 2003;63:1934‐1943. [DOI] [PubMed] [Google Scholar]
- 25. Depner AT. Uremic toxicity In: Nissenson AR, Fine RE, eds. Handbook of Dialysis Therapy. Philadelphia, PA: Elsevier; 2017:241‐263. [Google Scholar]
- 26. Kövér G, Tost H. Effects of hypercalcemia on kidney function in anesthetized dogs. Acta Physiol Hung. 1993;81:371‐393. [PubMed] [Google Scholar]
- 27. Segev G, Bandt C, Francey T, Cowgill LD. Aluminium toxicity following administration of aluminum‐based phosphate binders in 2 dogs with renal failure. J Vet Intern Med. 2008;22:1432‐1435. [DOI] [PubMed] [Google Scholar]
- 28. Jha S, Ansari MK. Leptospirosis presenting as acute meningoencephalitis. J Infect Dev Ctries. 2010;4:179‐182. [DOI] [PubMed] [Google Scholar]