

Abstract
Although experiencing bullying and other forms of assault is associated with adverse physical, emotional, and psychological consequences, the long-term consequences, especially in the aftermath of a severe trauma in adulthood, is not known. This study examined the relationship between history of being bullied and/or assaulted and posttraumatic stress disorder (PTSD) symptoms among responders to the World Trade Center (WTC) disaster. During 2015–16, a modified life events checklist was administered to responders at Stony Brook WTC Health Program. WTC-related PTSD symptoms were assessed by PTSD checklist (PCL). Longitudinal mixed models examined associations between bullying, other forms of assault, and severity and chronicity of PTSD symptoms. Approximately 13% of 920 responders had probable WTC-PTSD (PCL≥44). Being bullied in childhood was associated with increased odds of WTC-PTSD (adjusted odds ratio [aOR] =7.34; 95% confidence interval [CI] = 2.12–25.34), adjusted for demographics, other stressors, and WTC exposures. PTSD odds decreased over time among those not bullied (aOR 0.82; 95% CI: 0.73–0.92), but not among victims. Experiencing physical, sexual, or verbal assaults during adulthood, also had a significant association with WTC-PTSD (aOR 4.64; 95% CI: 1.98–10.92). Findings suggest being bullied in childhood and/or assaulted in adulthood can increase PTSD risk and progression after mass trauma.
Keywords: Bullying, Assault, PTSD, WTC responders, Childhood, Adulthood, Progressi
Posttraumatic stress disorder (PTSD) is a psychiatric condition that is more common in women, people with prior mental health conditions, and those exposed to traumas involving violence, such as childhood abuse, disasters, and rape (Sareen, 2014). While it is clear that severe childhood maltreatment can cause PTSD, the research is equivocal about the extent to which experiences of bullying victimization and/or experiences of assault affect individuals’ risk of experiencing PTSD symptoms after a severe trauma. Although being the victim of bullying has been linked to a variety of adult-onset physical and mental health conditions, the extent to which bullying modifies the risk of developing PTSD or experiencing more severe PTSD symptoms after a trauma has rarely been studied. Bullying refers to the repeated, systematic, and intentional abuse of power perpetrated by one person against another (Olweus, 1994). Bullying is a repeated and intentional harm caused by one or more persons that involves an actual or perceived power imbalance between victims and their bullies (Shetgiri, 2013) and often includes physical, verbal, and other forms of interpersonal aggression. Bullying is common in the United States, with 15–20% of community samples reporting bullying in school premises or, increasingly, electronically (Limber, Olweus, & Luxemborg, 2013; Kann et al., 2016). In adulthood, bullying appears to be common, though less well understood, with as many as 25% of U.S. workers reporting having been bullied at work (Workplace Bullying Institute, 2014).
Although sometimes underplayed as a “rite of passage,” victims of bullying have an elevated risk of adverse physical, emotional, and psychological problems (Reijntjes, Kamphuis, Prinzie, & Telch, 2010) including depression, anxiety, sleep disturbances, and poor adjustment in school. Results from a prospective cohort study in North Carolina suggest that involvement with bullying in childhood, either as a victim, a perpetrator, or both, was associated with adverse health, financial, behavioral, and social outcomes in young adults (Wolke, Copeland, Angold, & Costello, 2013). In particular, the victims of bullying in school had higher likelihood of becoming a regular smoker, being diagnosed with a serious physical or psychiatric illness, and experiencing slower recovery from illness in adulthood (Wolke et al., 2013). Other studies have found that children who were bullied during childhood were at a higher risk for having anxiety (Stapinski et al., 2014) and depressive disorders that extend into adulthood (Copeland, Wolke, Angold, & Costello, 2013; Takizawa, Maughan, & Arseneault, 2014). Little is known about the long-term effects of childhood bullying after taking into account experiences of getting bullied in adulthood and other traumatic events in childhood and/or adulthood.
Research suggests that some of the mental health symptoms emerging from bullied individuals are similar to those experienced after other traumatic events (Mikkelsen & Einarsen, 2002). Because symptoms of PTSD are believed to accumulate across independent traumatic events, childhood bullying could be a risk factor for developing more severe or chronic PTSD after subsequent traumatic exposures. Additionally, those who were bullied could be sensitized to stress such that they become more vulnerable to trauma experienced later in life (Zvolensky et al., 2015). Therefore, it is crucial for research examining bullying victimization and mental health in adulthood to account for whether individuals were bullied in childhood and also whether they encountered traumatic situations in adulthood. Moreover, research inquiring about experiences of bullying victimization that took place a long time ago, suffers from the possibility of other forms of abuse being characterized as bullying (Smolinski, 2011). In order to minimize the misclassification of other forms of abuse or assault as bullying, our study included questions of physical, sexual, and emotional abuse, so as to disentangle bullying and its implications from other forms of trauma. Moreover, experiencing abuse or assault in childhood—whether physical, emotional, or sexual—has been noted for its lingering effect well into adulthood and can result in PTSD after subsequent traumas (US Department of Health and Human Services, 2008). Although bullying was our primary exposure variable of interest, it was necessary to consider other forms of assault which can easily coexist with bullying.
Individuals who participated in search, rescue, and cleanup efforts after the World Trade Center (WTC) attacks on 9/11/2001, hereafter referred to as “responders,” were exposed to hazardous conditions including unsafe physical and chemical conditions, as well as traumatic psychological situations. Many responders witnessed death and injury of others, handled human remains, searched through dirt and debris, and lost their friends, colleagues, or family members in the aftermath of the WTC disaster. In the intervening years many responders continue to suffer from physical and mental health consequences, including PTSD (Bromet et al., 2016; Dasaro et al., 2015; Galea, Nandi, & Vlahov, 2005; Luft et al., 2012; Neria, DiGrande, & Adams, 2011; Neria, Nandi, & Galea, 2008). It is possible that those responders who were bullied and/or assaulted in the past are more vulnerable to PTSD after a massive trauma later in life. Moreover, the very nature and environment of work of the responders, especially those that had traditional jobs, can make them more vulnerable to experience assault, making it imperative to examine the relationship of these past experiences with WTC-related PTSD.
This manuscript examines whether being bullied and/or assaulted increased the risk of WTC-related PTSD in a responder cohort. We hypothesized that responders who reported childhood bullying would be more likely to experience severe and chronic PTSD after the WTC disaster, even after accounting for experiences of getting bullied in adulthood prior to the WTC attack, as well as experiences of other forms of assault in childhood or adulthood.
Methods
Participants
The Centers for Disease Control and Prevention (CDC) initiated a monitoring and treatment program for WTC responders, spanning five clinical centers, in 2002. The second largest clinical center is located at Stony Brook University (SBU) and monitors more than 8,000 responders residing on Long Island, NY. SBU’s population was similar to the entire population of WTC enrollees across the 5 centers (Dasaro et al., 2015). However, the SBU population includes a higher number of law enforcement personnel and men, and fewer individuals without a high-school degree.
The current study interviewed all responders (n=920) who attended monitoring visits at SBU clinics between November 2015 and June 2016. All responders who were seen during monitoring visits and were consented to research were eligible for inclusion in this study. Data were linked to existing data on PTSD collected prospectively during monitoring visits starting as early as 2002. All responders were monitored at intervals of 12 to 18 months. However, the number of monitoring visits varied because of continuous enrollment. The number of visits ranged from 1 to 12, with 4.8 visits (SD: 2.7) on an average. The study was approved by the Institutional Review Board. Responders provided informed written consent.
Assessment of PTSD Symptoms
PTSD symptoms were assessed at each monitoring visit using the PTSD checklist, specific trauma version tailored to the WTC disaster (PCL-S trauma specific version) (Blanchard, Jones-Alexander, Buckley, & Forneris, 1996). It was a 17-item self-report measure to assess PTSD symptoms over the past month. Each respondent rated the extent to which they were bothered by 17 DSM-IV WTC-related PTSD symptoms in the past month on a scale from 1 (not at all) to 5 (extremely). The PCL has good internal consistency and convergent validity (Wilkins, Lang, & Norman, 2011). The total PCL score was used to categorize respondents into those who had or did not have probable WTC-related PTSD, using a cut-off of 44 (Blanchard et al., 1996).
Experiences of Being Bullied in Childhood and Adulthood
Between November 2015 and June 2016 participants were asked to complete a life events questionnaire which asked whether the respondent experienced (or witnessed) traumatic life events, and if yes, whether she/he experienced (or witnessed) it during childhood, during adulthood before 9/11, during adulthood at the time of 9/11, or during adulthood after 9/11. For this study, experience of getting bullied during childhood was the main variable of interest. Responders were asked, “When did the following event happen to you: bullying (for example being teased incessantly or excluded by peers)?” There were multiple-choice response options specifying different time-points during their lives as well as the option to respond if they did not experience the said event ever. If a responder reported experiencing bullying during childhood (age 0–17), s/he was considered to have been bullied in childhood. If a responder reported to have been bullied in adulthood before the 9/11 attack—she/he was considered to have experienced bullying as adults.
Other Assaults/Threats Experienced
If a respondent reported having experienced one or more of the following during childhood—”a physical assault (for example, being attacked, hit, or slapped),” “an assault with a weapon (for example being shot, stabbed, threatened),” “sexual assault (rape, attempted rape, made to perform any unwanted sexual acts),” “regular verbal assault (for example, being yelled at, insulted),” and “physically threatened by the actions of a friend or family member”—she/he was considered to have experienced an assault/threat during childhood. Similarly, if they had any of these experiences at any time during their adulthood prior to 9/11, they were considered to have experienced assault/threat as adults.
Covariates
Predisposing characteristics were included. Education was categorized into those with some college, those with a university degree, and those with less education. Occupation was dichotomized into law enforcement (the majority at SBU) versus nontraditional responders (e.g., construction or utility workers). Age at the time of 9/11 was categorized as being 40 years or older, or less than 40 years old. The number of years since 9/11 attack was used in the longitudinal models. To take the severity of the responders’ exposure to the WTC disaster into account, four exposure groups were created following the work of Wisnivesky et al. (2011): very high, high, intermediate, and low (Wisnivesky et al., 2011). The very high exposure group comprised of those who worked more than 90 days, were exposed to the dust cloud due to the collapse of WTC buildings, and worked at least some time on the pile of debris. Rescue workers who were exposed to the dust cloud but either worked less than 90 days or did not work on the debris pile, were categorized as high exposure. The intermediate group of workers were exposed to the dust cloud and either worked between 40 days and 90 days or did not work on the pile. Workers in the lowest exposure group worked less than 40 days, were not exposed to dust from the collapse, and did not work on the debris pile.
Race was categorized as Caucasian or other, due to very few responders of non-Caucasian racial/ethnic groups. Respondents were also categorized as whether they experienced at least one stressful event since their previous visit to the WTC clinic, or experienced none of those events. This variable was used to account for the possible impact, if any, of responders’ recent stressful life experiences on their pre-existing PTSD symptoms (Schock, Böttche, Rosner, Wenk-Ansohn, & Knaevelsrud, 2016) and any change in symptomatology since last visit. Prior work by Zvolensky et al. (2015) has shown that post-9/11 stressful life events can affect WTC-related PTSD of responders. The stressful events assessed in our study included job loss or substantial loss of income, change of address, break up with spouse/partner, break up with best friend, major car trouble, robbery or house break in, bad debt problems, serious illness, injury, arrests, legal problems, illness or injury of a household member, death of a household member, death among relatives or close friends, pressure to provide shelter to someone against the respondent’s wish, getting mugged or beaten up, threatened or verbally assaulted by a household member, physically threatened or confronted by a household member, or any other event.
Data Analyses
Descriptive statistics were calculated to examine the distribution of respondents who were bullied and/or assaulted or threatened with socio-demographic factors including age at the time of 9/11, race, gender, occupation, and education.
Bivariate analyses were performed to examine unadjusted associations of childhood bullying and covariates with probable PTSD assessed during the visit when their life events were assessed. The prevalence of each of the PTSD symptoms was compared between those bullied and not bullied as children. False discovery rate (FDR) control method, developed by Benjamini & Hochberg (1995) and recommended for use in health studies (Glickman, Rao, & Schultz, 2014), was used to adjust for multiple comparisons. A maximum FDR of 0.05 was used as the level of significance. In order to understand sampling bias, we examined differences in the risk of PTSD, WTC-related exposures, age, sex, and occupation among those who were included as compared to those who were not.
Multivariate analyses were conducted using PTSD data from multiple visits. Generalized linear mixed models (GLMMs) with the logit link functions (multilevel logistic regression) were used to account for clustering of observations within the same individual. Random intercepts were utilized to account for unobserved temporally invariant differences in propensity for WTC-PTSD. Random slopes, using time since 9/11, were introduced to account for heteroskedasticity common in growth curve modeling and an unstructured intercept-slope covariance matrix was used to adjust for possible associations between baseline PTSD severity and PTSD chronicity. Interaction terms were introduced between childhood bullying and years since 9/11 to examine whether childhood bullying had a moderating effect on any change in WTC-PTSD with time.
Due to the fact that PTSD and depressive disorder often coexist (Flory & Yehuda, 2015) and because cutoffs commonly reduce power to detect differences, sensitivity analyses replicated the aforementioned analyses employing linear mixed models using a Gaussian distribution with raw PCL scores as the outcome and with the same set of predictors after adjusting for responders’ depression scores, measured by Patient Health Questionnaire-9 (PHQ-9), to account for potential confounding between getting bullied or assaulted and PTSD.
Results
Table 1 shows the distribution of WTC responders according to their experiences of being bullied and/or being assaulted/threatened in childhood and adult life. Among the 920 respondents with valid life event data, 7% reported having experienced bullying during childhood and 1.5% during adulthood prior to the WTC attacks. Because of the low frequency of responders who reported having been bullied during adulthood prior to the WTC attacks, we decided to not consider this variable in any further analysis. Other forms of assault/threat were far more common with 12.3% experiencing at least one form of assault/threat during their childhood and 29.4% in adulthood. The distribution of each type of assault and the prevalence of WTC-PTSD according to those assault experiences is illustrated in the Supplementary Table 1. The proportion of responders experiencing pre-9/11 assault/threat during their adulthood was higher (p<0.05) among those working in the law enforcement (30.6%) at the time of 9/11, compared with non-traditional responders (22.3%).
Table 1.
Distribution of WTC Responders According to their Experiences of Being Bullied and Other Assaults/Threats (n=920)
| Variable | Categories | Got bullied in childhood (%)b | Childhood assault(s)/threat(s)a (%)b | Assault(s)/threat(s) in adulthood pre-9/11a (%)b |
|---|---|---|---|---|
| Genderc | Female (n=63) | 5 (7.9) | 6 (9.5) | 12 (19.1) |
| Male (n=797) | 54 (6.8) | 95 (11.9) | 230 (28.9) | |
| Age at 9/11 (yrs.) | Less than 40 (n=557) | 45 (8.1) | 71 (12.8) | 169 (30.3) |
| ≥40 years (n=363) | 19 (5.2) | 42 (11.6) | 101 (27.8) | |
| Educationc | Less than college (n=212) | 17 (8.0) | 25 (11.8) | 50 (23.6) |
| Some college (n=358) | 25 (7.0) | 49 (13.7) | 107 (29.9) | |
| University degree (n=199) | 15 (7.5) | 22 (11.1) | 64 (32.2) | |
| Racec | Other (n=140) | 15 (10.7) | 20 (14.3) | 31 (22.1) |
| Caucasian (n=659) | 42 (6.4) | 78 (11.8) | 193 (29.3) | |
| Responder | Non-traditional (n=215) | 17 (7.9) | 34 (15.8) | 48 (22.3)* |
| typec | Police (n=569) | 39 (6.9) | 61 (10.7) | 174 (30.6) |
| Total (n=920) | 64 (7.0) | 113 (12.3) | 270 (29.3) |
at least one of physical assault, assault by a weapon, sexual assault, regular verbal assault, or being physically threatened by the actions of a friend or family member
Row percentage
Missing values
p for Chi-square test: <0.05
Thirteen percent of the responders had WTC-PTSD at the wave in which they completed the life events checklist (Table 2). In bivariate analyses (Table 2), the prevalence of WTC-related probable PTSD was significantly higher among non-traditional responders (odds ratio [OR]: 2.41; 95% confidence interval [CI]: 1.53, 3.78), those who reported that they had experienced bullying during childhood (OR: 3.27; 95% CI: 1.73, 6.17). Experiencing any other kind of assault or threat during childhood and/or during adulthood was also significantly associated with WTC-PTSD.
Table 2.
Characteristics of Responders and Associations with Probable WTC-PTSD (PCL≥44) Concurrent to their Life Events Assessment (n=920)
| WTC-PTSD [n=122 (13.3%)] n(%)a | No WTC-PTSD [n=798 (86.7%)] n(%)a | OR (95% CI) | |
|---|---|---|---|
| Genderb | |||
| Female | 6 (9.5) | 57 (90.5) | 0.78 (0.30, 2.02) |
| Male | 109 (13.7) | 688 (86.3) | 1 |
| Age at 9/11 (yrs) | |||
| Less than 40 | 65 (11.7) | 492 (88.3) | 1 |
| ≥40 years | 57 (15.7) | 306 (84.3) | 1.27 (0.82, 1.97) |
| Educationb | |||
| Less than college | 30 (14.2) | 182 (85.9) | 1.21 (0.65, 2.26) |
| Some college or associate degree | 52 (14.5) | 306 (85.5) | 1.26 (0.72, 2.21) |
| University degree | 22 (11.1) | 177 (88.9) | 1 |
| WTC exposure severityb | |||
| Very high | 3 (16.7.7) | 15 (83.3) | 1.49 (0.39, 5.70) |
| High | 17 (13.1) | 113 (86.9) | 1.17 (0.57, 2.39) |
| Intermediate | 57 (14.0) | 351 (86.0) | 1.19 (0.67, 2.14) |
| Low | 17 (11.6) | 129 (88.4) | 1 |
| Raceb | |||
| Other | 13 (9.3) | 127 (90.7) | 0.53 (0.27, 1.06) |
| Caucasian | 94 (14.3) | 565 (85.7) | 1 |
| Type of responderb | |||
| Non-traditional | 49 (22.8) | 166 (77.2) | 2.41 (1.53, 3.78) |
| Police | 57 (10.0) | 512 (90.0) | 1 |
| Experienced bullying during childhood | |||
| Yes | 18 (28.1) | 46 (71.9) | 3.27 (1.73, 6.17) |
| No | 104 (12.2) | 752 (87.9) | 1 |
| Experienced assault/threatb,c during childhood | |||
| Yes | 20 (17.7) | 93 (82.3) | 1.80 (1.01, 3.18) |
| No | 102 (12.6) | 705 (87.4) | 1 |
| Experienced assault/threatb,c during adulthood before the WTC attack | |||
| Yes | 49 (18.2) | 221 (81.9) | 2.15 (1.37, 3.37) |
| No | 73 (11.2) | 577 (88.8) | 1 |
Row percentage
Missing values
at least one of physical assault, assault by a weapon, sexual assault, regular verbal assault, or being physically threatened by the actions of a friend or family member
The distribution of responders according to the prevalence of specific PTSD symptoms with childhood bullying experiences is depicted in Figure 1. After adjusting for FDR, the prevalence of most of the symptoms were significantly higher among those bullied as children, compared with those who were not bullied as children.
Figure 1.
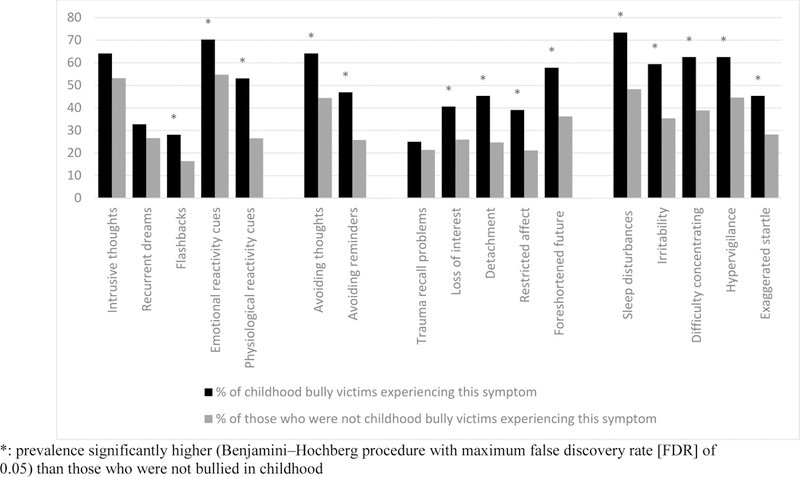
Distribution of Respondents (n=920) According to Their Experiences of Being Bullied in Childhood and Specific PCL Symptoms
Multivariate analyses utilizing longitudinal data revealed that the adjusted odds of having probable PTSD was higher (Table 3, model 1) among those who were bullied during childhood (aOR 7.34; 95% CI: 2.12–25.34) as well as among those assaulted/threatened as adults (aOR 4.64; 95% CI: 1.98–10.92). Having lower education, experiencing high WTC exposure, being a non-traditional responder, experiencing one or more stressful life events were also significantly associated with probable WTC-PTSD. With increasing years since 9/11, there was a slight, yet significant (aOR 0.88; 95% CI: 0.79–0.98), decrease in the odds of WTC-PTSD (table 3, model 1). Although the interaction term between childhood bullying and years since 9/11 was not statistically significant (p=0.07) (table 3, model 2), stratified analysis (Supplementary Table 2) revealed that those that were not bullied in childhood experienced a significant decrease in the odds (aOR 0.82; 95% CI: 0.73– 0.92) of WTC-PTSD with increasing years since 9/11. The longitudinal change in the odds of PTSD was not statistically significant for those that were bullied during childhood.
Table 3.
Multilevel Multivariate Analyses Results for Probable PTSD Among WTC Responders (n=920) Taking Multiple Visits into Consideration (n=920)
| aOR (95% CI) for WTC-related probable PTSD | ||
|---|---|---|
| Model 1 (without childhood bullying and time interaction) |
Model 2 (with the interaction variable) |
|
| Fixed effects | ||
| Years since 9/11 | 0.88 (0.79, 0.98) | 0.84 (0.74, 0.94) |
| Gender female (ref: male) | 2.71 (0.68, 10.88) | 2.88 (0.73,11.37) |
| Age at 9/11: 40 or more (ref: < 40) | 0.77 (0.35, 1.67) | 0.77 (0.36, 1.66) |
| Severity of WTC exposure (ref: low) | ||
| Very high | 1.32 (0.15, 11.60) | 1.30 (0.15, 11.20) |
| High | 4.58 (1.37, 15.31) | 4.70 (1.42, 15.55) |
| Intermediate | 1.67 (0.60, 4.63) | 1.71 (0.62, 4.71) |
| Education (ref: university degree) | ||
| Less than college | 3.36 (1.17, 9.69) | 3.31 (1.17, 9.42) |
| Some college or associate degree | 2.40 (0.95, 6.05) | 2.36 (0.94, 5.88) |
| Race: non-Caucasian (ref: Caucasian) | 0.48 (0.17, 1.37) | 0.49 (0.17, 1.39) |
| Type of responder: non-traditional (ref: traditional responder) | 9.05 (3.65, 22.42) | 9.00 (3.67, 22.07) |
| No. of monitoring visits: 1–2 (ref: >2) | 1.16 (0.19, 6.99) | 1.08 (0.17, 6.78) |
| Experienced at least one stressful event since last visit (ref: none) | 2.57 (1.84, 3.57) | 2.49 (1.79, 3.47) |
| Experienced bullying during childhood (ref: not bullied in childhood) | 7.34 (2.12, 25.34) | 8.04 (2.34, 27.62) |
| Experienced assault/threatb during childhood (ref: not assaulted or threatened during childhood) | 0.63 (0.21, 1.89) | 0.65 (0.22, 1.91) |
| Experienced assault/threatb during adulthood prior to WTC attack (ref: not assaulted or threatened during adulthood prior to WTC attack) | 4.64 (1.98, 10.92) | 4.56 (1.96, 10.60) |
| Experienced childhood bullying*years since 9/11 | − | 0.97 (0.83, 1.14) |
| Random effects | ||
| Intercept variance | 16.87, 5.00, 3.37, 0.0004 | 14.20, 4.47, 3.18, 0.0007 |
| Slope variance | 0.10, 0.03, 3.86, <0.0001 | 0.10, 0.03, 3.88, <0.0001 |
| Intercept-slope covariance | -0.44, 0.27, −1.63, 0.10 | -0.32, 0.24, −1.30, 0.19 |
Each aOR is adjusted for all the other covariates in the model
at least one of physical assault, assault by a weapon, sexual assault, regular verbal assault, or being physically threatened by the actions of a friend or family member
Childhood bullying and assault/threat during adulthood remained significantly associated with WTC-PTSD when sensitivity analyses were performed using the actual PCL scores instead of the cut-offs as the outcome, both before and after adjusting for PHQ-9 scores (Supplementary Table 3). Given the higher prevalence of childhood bully victimization reported by women than men in our sample, the analyses were repeated after stratifying by gender (Supplementary Table 4). For men, most of the results were similar to that of the entire sample, with significantly higher adjusted odds for WTC-PTSD among those who were bullied during childhood (aOR: 8.85; 95% CI: 2.32–33.77) and those who were assaulted or threatened during adulthood (aOR: 5.55; 95% CI: 2.25–13.69). Women showed similar trend for childhood bullying, but the results were not statistically significant.
Discussion
This study examined the role of bullying in increasing the risk of PTSD in a cohort of individuals who were all exposed to the tragic WTC events. This study found that 7% of WTC responders were bullied as children, whereas 12% were assaulted/threatened during childhood and 29% were assaulted/threatened during adulthood. Exposure to both childhood bullying and adult assaults was related to 4- to 7-fold increased odds of WTC-related PTSD, after controlling for all covariates. The prevalence of WTC-PTSD decreased with time following 9/11 among those who were not bullied during childhood, while there was no significant longitudinal improvement among childhood bully victims.
Prevalence of Being Bullied in Childhood
The prevalence (Table 1) of childhood bullying experiences (7%) was lower in our sample than estimated in a recent nationally-representative study of 12 to 18-year-old students (U.S. Department of Education, 2015), and lower than the 15–20% reported by CDC (Centers for Disease Control and Prevention [CDC], 2017). This could be because the experiences of being bullied as children were being recalled by the WTC responders after many years, resulting in lower recall rates. However, the proportion of responders who reported childhood bullying was not significantly different between age groups (Table 1), potentially suggesting a lower likelihood of recall bias. At the same time, individuals with current WTC-related PTSD symptoms are more likely to remember or report bullying experiences, a possibility that has been discussed in the limitations section. It is worth noting that our study sample was overrepresented by men, who reported a lower prevalence of getting bullied in childhood, compared with women (Table 1). Although the difference was not statistically significant, the lower prevalence among men was similar to findings based on the School Crime Supplement (SCS) to the National Crime Victimization Survey for the years 2005 through 2013 (National Center for Education Statistics, 2014). However, victimization with certain specific types of bullying, such as the more physically aggressive forms, have been found to be more common in males (National Center for Education Statistics, 2014). The majority of WTC responders belonged to law enforcement and had high educational attainment, so it is likely that the study sample comprised of relatively healthy individuals who had a lower prevalence of childhood abuse and were less likely to be bullied than the general population. The nature of bullying has changed since many of these participants were children, with the advent of cyber and media-related bullying for instance.
Bully Victimization in Childhood and Probable WTC-PTSD
We found a significantly higher prevalence of probable PTSD among victims of childhood bullying even after controlling for covariates (Table 3). Although there are a limited number of studies focusing on childhood bully victimization and adult PTSD symptoms in the U.S., a latent class analysis of data drawn from the Adult Psychiatry Morbidity Survey (APMS) in the UK found that those in the bullying and domestic violence class had higher PTSD scores (Dhingra, Boduszek, & Sharratt, 2016). A recent study based on the World Mental Health (WMH) Surveys have found that childhood family adversities in the form of maladaptive family functioning is a risk factor of disaster-related PTSD among adults (Bromet et al., 2016). Our study adds that bully victimization in childhood is a long-term risk factor for PTSD in the wake of a disaster. It is interesting that experiencing other forms of assault or threat during childhood was not significantly associated with probable PTSD, in multivariable analyses (Table 3) in our study.
Those who have experienced events of an interpersonal nature exhibit higher levels of PTSD symptoms than others (Lancaster, Melka, & Rodriguez, 2009). Bullying is an interpersonal event that often takes place at the vital phase of development of a variety of cognitive, emotional, and behavioral brain systems and functions, including self-regulation and processing of emotions, executive functions, social connectivity, and the ability to respond appropriately to the perceptions of threat (Bremner, 2006; Cicchetti, 2006; Derryberry & Tucker, 2006; Johnson & de Haan, 2006). Being bullied has also been hypothesized to alter the physiological responses to stress by affecting the hypothalamus-pituitary-adrenal (HPA)-axis activity and cortisol responses (Harkness, Stewart, & Wynne-Edwards, 2011; Ouellet-Morin et al., 2011), with these physiological alterations posing risk for the development of subsequent PTSD (Delahanty, Raimonde, & Spoonster, 2000). In general, exposure to early life adversity has been associated with hypercortisolism, marked by low cortisol levels and blunted morning-to-evening cortisol rhythms (Bernard, Butzin-Dozier, Rittenhouse, & Dozier, 2010; Bruce, Fisher, Pears, & Levine, 2009), which can then compromise healthy physiological responses to adult trauma.
Longitudinal Decline in PTSD Odds After Stratifying by Childhood Bullying
An interesting observation from our study was that those who did not report childhood bullying had a significant longitudinal decline in PTSD odds (Supplementary Table 2), which is similar to what would generally be expected with the highest risk of PTSD right after a highly stressful event and then decreasing somewhat. However, those bullied in childhood did not exhibit any change with time (Supplementary Table 2). Thus, it is a matter of concern that childhood bully victims were more likely to experience PTSD years after their traumatic experience, in the aftermath of a massive disaster such as the WTC attack. It is possible that early-life traumatic experiences such as childhood bullying leave a life-long impact and bolster the adverse consequences of a subsequent disaster, thereby making those WTC responders who were bullied as children a highly vulnerable group showing resistance to decline in PTSD risk over time. It has been suggested that exposure to traumatic events during childhood can result in exacerbated emotional reactions to potential threat cues, thereby increasing the susceptibility to future PTSD (Kessler et al., 2014; McLaughlin et al., 2017).
Our study adds to the expanding research on adverse childhood experiences by specifically focusing on childhood bullying, which is seldom examined as a PTSD risk factor. It is worth noting though, that the sample size of childhood bully victims in our study was small (n=64) compared with the total number of responders (n=920) (Table 1). Therefore, the multivariate analysis (Supplementary Table 2) among bully victims may have been inadequately powered to detect any longitudinal decline in WTC-PTSD risk. Replication of our findings on larger representative datasets are imperative to rule out findings owing to inadequate sample size.
Implications for Practice
In light of these results concerning the associations between bullying and PTSD, treating the sequelae of early trauma exposure among first responders is important. Although scientific research on treatment—especially pharmacotherapy-- of PTSD among first responders is limited compared with treatment research conducted in other trauma populations (Haugen, Evces, & Weiss, 2012), treatment targets can include understanding the psychological coping mechanisms, including the maladaptive ones such as dissociation, post-incident mental health needs, and reprocessing significant emotional reactions and physiological responses (Adler-Tapia, 2013). Cognitive Processing Therapy (CPT) and Prolonged Exposure (PE) are two of the most effective treatments for PTSD including PTSD symptoms among first responders (Lowell et al., 2018). In particular, PE, in conjunction with pharmacotherapy using certain selective serotonin reuptake inhibitors, has shown promise in alleviating WTC-related PTSD symptoms (Schneier et al., 2012). PE and CPT need further exploration in the context of addressing WTC responders’ traumatic experiences and their consequences. Therapists should also consider the ways cumulative trauma and bullying impact the health of WTC first responders and their families. The types of available treatments that incorporate protocols specific to first responders, include individual and family psychotherapy, Cognitive-Behavioral Therapy (CBT) that can also address depression secondary to the effects of bullying and behavioral dysregulation, and Eye-Movement Desensitization and Reprocessing (EMDR) (Luber, 2015).
Limitations
This study has a number of limitations. First, although this is one of the first studies to examine childhood bullying experiences as a risk factor for PTSD in adulthood, the study has limited specificity regarding the bullying experience. The study asked about childhood bullying but did not distinguish between school bullying and being bullied outside of school. The study did not include an external control of individuals who were non-responders, in part because such a control was not necessary to answer the question posed here. Second, this study population is unique, and findings may not be generalizable to other populations. All responders lived on Long Island, NY, and were responders to a severe traumatic event. As such, they were predominantly highly educated White males, and nearly all were employed (many as police officers) at the time of the disaster. Third, although longitudinal data was a key strength of this study, results could have been affected by the fact that the number of waves as well as the intervals between consecutive visits were unequal. However, multilevel models such as the one used in this study can address the issue of irregularly spaced observations. Fourth, this study relied on questions regarding past experiences of getting bullied that were asked after the traumatic experience of responding to the WTC attacks, which makes it subject to errors in recall and recall bias. This could be one of the explanations behind the low prevalence of childhood bullying victimization reported in this study compared with national surveys. Notably, results will be biased if individuals with current WTC-related PTSD symptoms are more likely to remember or report bullying experiences. The reverse is also plausible, whereby those with PTSD symptoms are inclined to avoid reporting painful memories from the past, resulting in lower recall rates for childhood experiences (Van der Kolk, 1998).
Another limitation is that we did not know whether any of the responders had PTSD symptoms prior to the 9/11 attacks, as an aftermath of other trauma and/or assault that they might have experienced throughout their lives. It is possible that some responders had difficulty disentangling symptoms of 9/11-induced PTSD from PTSD symptoms they already had. Moreover, we were unable to measure responders’ resilience levels, which can differ substantially between individuals and play a vital role in PTSD development or progression. Lastly, perceived stigma towards mental health issues as well as against reporting of victimization to traumatic experiences, could have had an impact on responders’ retrospective reports, especially because a majority of them were engaged in law enforcement. Indeed, childhood bullying victimization reported by those not in the law enforcement (7.9%) was slightly higher than those in law enforcement (6.9%) in our sample. Although this difference was not statistically significant, future research on this topic needs to address experiences and perceptions of stigma.
Conclusion
Despite the limitations, this study examined the relationship between being bullied in childhood and adult PTSD in a large sample of WTC responders. Our findings suggest that even in the context of PTSD in the aftermath of a massive disaster such as the 9/11 attacks, bullying victimization in childhood plays an important role and this relationship persists even after controlling for adult bullying. Adult bullying experiences and/or depressive symptoms cannot entirely explain the relationship between childhood bullying and WTC-PTSD. This adds to the evidence regarding the importance of screening for childhood adversities among adults who have gone through a traumatic event. The link between being bullied and WTC-PTSD is troublesome, especially when observed in a sample comprised mostly of law enforcement officers and only reinforces the need to combat the menace of bullying in all settings.
Supplementary Material
Acknowledgments
Funding for this study was provided by the National Institutes of Health (R01 AG049953; PI: Dr. Clouston), and by the Centers for Disease Control and Prevention’s National Institute of Occupational Safety and Health to administer the monitoring survey (CDC-200–2011-39361). The funders played no role in data collection, analysis, interpretation, reporting, or the decision to submit for publication.
Footnotes
Disclosure of Interest All the authors declare that they have no conflicts of interest to report.
Ethical Standards and Informed Consent All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation [institutional and national] and with the Helsinki Declaration of 1975, as revised in 2000. Informed consent was obtained from all responders for being included in the study.
Contributor Information
Soumyadeep Mukherjee, Rhode Island College and Stony Brook University.
Sean Clouston, Stony Brook University.
Evelyn Bromet, Stony Brook University.
George S. Leibowitz, Stony Brook University
Stacey B. Scott, Stony Brook University
Kristin Bernard, Stony Brook University.
Roman Kotov, Stony Brook University.
Benjamin Luft, Stony Brook University.
References
- Adler-Tapia R (2013). Early Mental Health Intervention for First Responders/Protective [Google Scholar]
- Service Workers Including Firefighters and Emergency Medical Services (EMS) Professionals. In Luber M (Ed.), Implementing EMDR early mental health interventions for man-made and natural disasters: Models, scripted protocols and summary sheets New York: Springer Publishing Company. [Google Scholar]
- Benjamini Y, & Hochberg Y (1995). Controlling the false discovery rate: a practical and powerful approach to multiple testing. Journal of the Royal Statistical Ssociety. Series B (Methodological), 289–300. [Google Scholar]
- Bernard K, Butzin-Dozier Z, Rittenhouse J, & Dozier M (2010). Cortisol production patterns in young children living with birth parents vs children placed in foster care following involvement of Child Protective Services. Archives of Pediatrics & Adolescent Medicine, 164(5), 438–443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blanchard EB, Jones-Alexander J, Buckley TC, & Forneris CA (1996). Psychometric properties of the PTSD Checklist (PCL). Behaviour Research and Therapy, 34(8), 669–673. [DOI] [PubMed] [Google Scholar]
- Bremner J (2006). Traumatic stress from a multiple-levels-of-analysis perspective. In Cicchetti D & Cohen DJ (Eds.), Developmental Psychopathology (Vol. 2): Developmental Neuroscience (2nd ed., pp. 656–676). Hoboken: John Wiley & Sons, Inc. [Google Scholar]
- Bromet E, Hobbs M, Clouston S, Gonzalez A, Kotov R, & Luft B (2016). DSM-IV post-traumatic stress disorder among World Trade Center responders 11–13 years after the disaster of 11 September 2001 (9/11). Psychological Medicine, 46(04), 771–783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bruce J, Fisher PA, Pears KC, & Levine S (2009). Morning cortisol Levels in preschool‐aged foster children: Differential effects of maltreatment type. Developmental Psychobiology, 51(1), 14–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Centers for Disease Control & Prevention (2017). Preventing Bullying worksheet Retrieved from https://www.cdc.gov/violenceprevention/pdf/bullying-factsheet.pdf
- Cicchetti DC(2006). The developing brain and neural plasticity: Implications for normality, psychopathology, and resilience. In Cicchetti D & Cohen DJ (Eds.), Developmental Psychopathology (Vol. 2): Developmental Neuroscience (2nd ed., pp. 1–64). Hoboken, NJ: Wiley. [Google Scholar]
- Copeland WE, Wolke D, Angold A, & Costello EJ (2013). Adult psychiatric outcomes of bullying and being bullied by peers in childhood and adolescence. JAMA Psychiatry, 70(4), 419–426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dasaro CR, Holden WL, Berman KD, Crane MA, Kaplan JR, Lucchini RG, Tirunagari US (2015). Cohort profile: World trade center health program general responder cohort. International Journal of Epidemiology, 46 (2), e9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Delahanty DL, Raimonde AJ, & Spoonster E (2000). Initial posttraumatic urinary cortisol levels predict subsequent PTSD symptoms in motor vehicle accident victims. Biological Psychiatry, 48(9), 940–947. [DOI] [PubMed] [Google Scholar]
- Derryberry D, & Tucker DM (2006). Motivation, Self‐Regulation, and Self‐Organization. In Cicchetti D & Cohen DJ (Eds.) Developmental Psychopathology (Vol. 2): Developmental Neuroscience (2nd ed., pp502–532. Hoboken, NJ: Wiley. [Google Scholar]
- Dhingra K, Boduszek D, & Sharratt K (2016). Victimization profiles, non-suicidal self-injury, suicide attempt, and post-traumatic stress disorder symptomology: application of latent class analysis. Journal of Interpersonal Violence, 31(14), 2412–2429. [DOI] [PubMed] [Google Scholar]
- Flory JD, & Yehuda R (2015). Comorbidity between post-traumatic stress disorder and major depressive disorder: alternative explanations and treatment considerations. Dialogues in Clinical Neuroscience, 17(2), 141–150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Galea S, Nandi A, & Vlahov D (2005). The epidemiology of post-traumatic stress disorder after disasters. Epidemiologic Reviews, 27(1), 78–91. [DOI] [PubMed] [Google Scholar]
- Glickman ME, Rao SR, & Schultz MR (2014). False discovery rate control is a recommended alternative to Bonferroni-type adjustments in health studies. Journal of Clinical Epidemiology, 67(8), 850–857. [DOI] [PubMed] [Google Scholar]
- Harkness KL, Stewart JG, & Wynne-Edwards KE (2011). Cortisol reactivity to social stress in adolescents: role of depression severity and child maltreatment. Psychoneuroendocrinology, 36(2), 173–181. [DOI] [PubMed] [Google Scholar]
- Haugen PT, Evces M, & Weiss DS (2012). Treating posttraumatic stress disorder in first responders: A systematic review. Clinical Psychology Review, 32 (5), 370–380. [DOI] [PubMed] [Google Scholar]
- Johnson MH, & de Haan M (2006). Typical and atypical human functional brain development. In Cicchetti D & Cohen DJ (Eds.) Developmental Psychopathology (Vol 2): Developmental Neuroscience (2nd ed., pp.197–215). Hoboken, NJ: Wiley. [Google Scholar]
- Kann L, McManus T, Harris WA, Shanklin SL, Flint KH, Hawkins J,…..Zara S (2016). Youth Risk Behavior Surveillance—United States, 2015. Morbidity and Mortality Weekly Report (MMWR) Surveillance Summaries 65(6) (SS10), 46–50. [DOI] [PubMed] [Google Scholar]
- Kessler RC, Rose S, Koenen KC, Karam EG, Stang PE, Stein DJ, … McLaughlin KA (2014). How well can post‐traumatic stress disorder be predicted from pre‐trauma risk factors? An exploratory study in the WHO World Mental Health Surveys. World Psychiatry, 13(3), 265–274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lancaster SL, Melka SE, & Rodriguez BF (2009). An examination of the differential effects of the experience of DSM-IV defined traumatic events and life stressors. Journal of Anxiety Disorders, 23(5), 711–717. [DOI] [PubMed] [Google Scholar]
- Limber SP, Olweus D, & Luxenberg H, (2013). Bullying in US schools: 2012 status report Hazelden Foundation; Retrieved from https://www.pdastats.com/PublicFiles/OBPP_Bullying_in_US_Schools_2012Report.pdf. [Google Scholar]
- Lowell A, Suarez-Jimenez B, Helpman L, Zhu X, Durosky A, Hilburn A, … & Neria Y (2018). 9/11-related PTSD among highly exposed populations: a systematic review 15 years after the attack. Psychological Medicine, 48(4), 537–553. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luber M (2015). EMDR with First Responders Models, Scripted Protocols, and Summary Sheets for Mental Health Interventions New York: Springer Publishing Company. [Google Scholar]
- Luft B, Schechter C, Kotov R, Broihier J, Reissman D, Guerrera K, … Friedman-Jimenez G (2012). Exposure, probable PTSD and lower respiratory illness among World Trade Center rescue, recovery and clean-up workers. Psychological Medicine, 42(05), 1069–1079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLaughlin KA, Koenen KC, Bromet EJ, Karam EG, Liu H, Petukhova M, …..Ronald C (2017). Childhood Adversities and Post-traumatic Stress Disorder: Evidence for Stress Sensitization in the World Mental Health Surveys. British Journal of Psychiatry, 211(5), 280–288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mikkelsen EG, & Einarsen S (2002). Basic assumptions and symptoms of post-traumatic stress among victims of bullying at work. European Journal of Work and Organizational Psychology, 11(1), 87–111. [Google Scholar]
- Neria Y, DiGrande L, & Adams BG (2011). Posttraumatic stress disorder following the September 11, 2001, terrorist attacks: a review of the literature among highly exposed populations. American Psychologist, 66(6), 429. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Neria Y, Nandi A, & Galea S (2008). Post-traumatic stress disorder following disasters: asystematic review. Psychological Medicine, 38(04), 467–480. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Olweus D (1994). Bullying at school: basic facts and effects of a school-based intervention program. Journal of Child Psychology and Psychiatry, 35(7), 1171–1190. [DOI] [PubMed] [Google Scholar]
- Ouellet-Morin I, Danese A, Bowes L, Shakoor S, Ambler A, Pariante CM, … Arseneault L (2011). A discordant monozygotic twin design shows blunted cortisol reactivity among bullied children. Journal of the American Academy of Child & Adolescent Psychiatry, 50(6), 574–582. e3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reijntjes A, Kamphuis JH, Prinzie P, & Telch MJ (2010). Peer victimization and internalizing problems in children: A meta-analysis of longitudinal studies. Child Abuse & Neglect, 34(4), 244–252. [DOI] [PubMed] [Google Scholar]
- Sareen J (2014). Posttraumatic stress disorder in adults: impact, comorbidity, risk factors, and treatment. The Canadian Journal of Psychiatry, 59(9), 460–467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schneier FR, Neria Y, Pavlicova M, Hembree E, Suh EJ, Amsel L, & Marshall RD (2012). Combined prolonged exposure therapy and paroxetine for PTSD related to the World Trade Center attack: a randomized controlled trial. American Journal of Psychiatry, 169(1), 80–88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schock K, Böttche M, Rosner R, Wenk-Ansohn M, & Knaevelsrud C (2016). Impact of new traumatic or stressful life events on pre-existing PTSD in traumatized refugees: results of a longitudinal study. European Journal of Psychotraumatology, 7: 10.3402/ejpt.v7.32106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shetgiri R (2013). Bullying and victimization among children. Advances in Pediatrics, 60(1), 33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smolinski J (2011, September 29). Sexual harassment versus bullying [Blog post] Retrieved from https://www.aauw.org/2011/09/29/sexual-harassment-versus-bullying/. [Google Scholar]
- Stapinski LA, Bowes L, Wolke D, Pearson RM, Mahedy L, Button KS, … Araya R (2014). Peer victimization during adolescence and risk for anxiety disorders in adulthood: a prospective cohort study. Depression and Anxiety, 31(7), 574–582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Takizawa R, Maughan B, & Arseneault L (2014). Adult health outcomes of childhood bullying victimization: evidence from a five-decade longitudinal British birth cohort. American Journal of Psychiatry, 171(7), 777–784. [DOI] [PubMed] [Google Scholar]
- U.S. Department of Education. (April 2015). Student Reports of Bullying and Cyber-Bullying: Results from the 2013 School Crime Supplement to the National Crime Victimization Survey Washington DC: Retrieved from http://nces.ed.gov/pubs2015/2015056.pdf. [Google Scholar]
- U.S. Department of Health and Human Services, Administration on Children, Youth and Families. Child Maltreatment 2006 (Washington, DC: U.S. Government Printing Office, 2008). Retrieved from http://www.acf.hhs.gov/programs/cb/stats_research/. [Google Scholar]
- Van der Kolk BA (1998). Trauma and memory. Psychiatry and Clinical Neurosciences, 52(S1), S52–S64. [Google Scholar]
- Wilkins KC, Lang AJ, & Norman SB (2011). Synthesis of the psychometric properties of the PTSD checklist (PCL) military, civilian, and specific versions. Depression and anxiety, 28(7), 596–606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wisnivesky JP, Teitelbaum SL, Todd AC, Boffetta P, Crane M, Crowley L, … Herbert R (2011). Persistence of multiple illnesses in World Trade Center rescue and recovery workers: a cohort study. The Lancet, 378(9794), 888–897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wolke D, Copeland WE, Angold A, & Costello EJ (2013). Impact of bullying in childhood on adult health, wealth, crime, and social outcomes. Psychological Science, 24(10), 1958–1970. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Workplace Bullying Institute (WBI) (2014) 2014 WBI U.S. Workplace Bullying Survey Retrieved from http://workplacebullying.org/multi/pdf/WBI-2014-US-Survey.pdf.
- Zvolensky MJ, Farris SG, Kotov R, Schechter CB, Bromet E, Gonzalez A, … Kaplan J (2015). World Trade Center disaster and sensitization to subsequent life stress: a longitudinal study of disaster responders. Preventive Medicine, 75, 70–74. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.