

ABSTRACT
Paediatric orbital trauma is uncommon, but it can be associated with significant morbidity. Traumatic pseudomeningocele is an infrequent complication of orbital trauma; it occurs due to an extradural collection of cerebrospinal fluid (CSF) that develops after a dural tear. Herein, we report a case of a seven-month-old male child who presented with eye swelling and suspicion of orbital cellulitis, along with a history of a road traffic accident. He was later diagnosed with traumatic orbital pseudomeningocele and underwent a left frontal craniotomy and duroplasty along with repair of medial orbital pseudomeningocele. Postoperatively, the child remained stable and resolution of proptosis was observed.
KEYWORDS: Orbital pseudomeningocele, orbital trauma, medial orbital wall
Introduction
Paediatric orbital trauma, though rare, can be caused in multiple situations; ranging from relatively minor falls to “high-energy multi-vector trauma” such as road traffic accidents.1,2 Orbital fractures can lead to various complications such as entrapment syndromes, nerve injuries, impingement syndromes, and less commonly, traumatic pseudomeningoceles. Whereas the majority of published articles describe pseudomeningoceles in relation to the spine and posterior fossa surgery,3,4 there are comparatively fewer reports on intradiploic and orbital pseudomeningoceles. In a review of the literature over the last 66 years, very few cases of traumatic orbital pseudomeningoceles in children have been reported. Only four cases pseudomeningoceles in the paediatric age group were located in or near the orbit.5–8 Furthermore, only one of the cases occurred within one month of the traumatic event, as is the case with our patient.7
Case report
A seven-month-old male child presented to the ophthalmology outpatient clinic in the Aga Khan University Hospital (AKUH), a tertiary care hospital in Karachi, with a one-month complaint of left eye swelling following a road traffic accident. He had been previously hospitalised in a government tertiary care hospital in Karachi for 12 days, for the same complaint. During his stay there, he was discharged after incision and drainage of the lesion but was subsequently readmitted with persistent eye swelling. He had undergone daily dressings of the wound along with aspirations, which showed clear yellow fluid. The child had now been brought to AKUH and was admitted under paediatric care with a query of orbital cellulitis. His review of systems and family history was unremarkable. There was no history of seizures.
On clinical examination, the child was alert and oriented, with a Glasgow Coma Scale (GCS) score of 15. On inspection, there was severe left lid swelling, proptosis and chemosis (Figure 1). The child had difficulty opening the eye, and a serous white discharge could be seen from the eye. The orbit was tense on palpation and a bruit could not be heard. No gross neurological focal deficits were seen. The rest of the systemic examination was unremarkable. However, visual acuity could not be assessed.
Figure 1.

Pre-operative view of the orbital encephalocele.
Detailed imaging studies were performed. A CT scan of the head showed a hypodense collection along the superolateral aspect of the left globe, measuring approximately 31 × 27 mm and displacing the globe inferiorly (Figure 2a). Focal encephalomalacia in the left frontal lobe and displaced fragments of lamina papyracea on the left side were also seen (Figure 2b and c). Magnetic resonance imaging (MRI) of the brain showed a T2 hyperintense and T1 hypointense collection along the superolateral aspect of the left globe, measuring approximately 34 × 24 mm and displacing the globe inferiorly. It also showed bilateral subdural collections and focal cystic encephalomalacia in left frontal lobe (Figure 3).
Figure 2.

(a) Coronal section showing a hypodense collection along the superolateral aspect of the left globe and bilateral subdural collections; (b) Fracture of the left medial orbital wall, showing displaced fragments of the lamina papyracea; (c) Fracture of the left medial orbital wall, with displacement of bony fragments medially.
Figure 3.
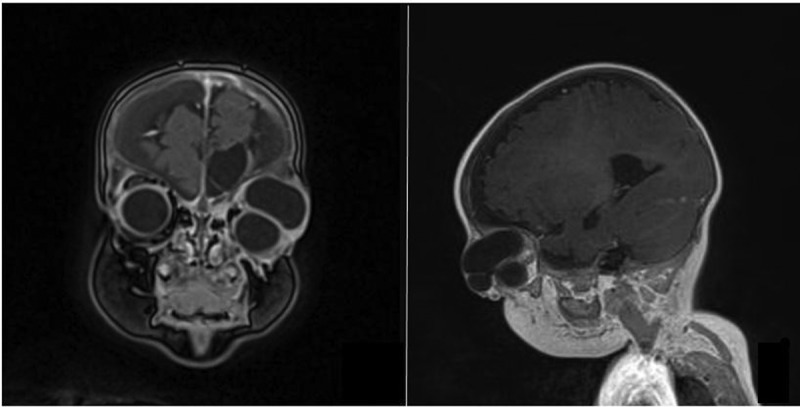
(a) Coronal section showing a hypointense collection along the superolateral aspect of the left globe; (b) Sagittal section showing a hypointense collection along the superolateral aspect of the left globe.
The patient was taken to the operating room, where he underwent a left frontal craniotomy with repair of medial orbital pseudomeningocele. A burr hole was made in the left frontal bone and a craniotomy was done, without detaching the orbital roof and medial and lateral orbital walls. Two dural defects, one along the medial orbital wall (Figure 4) and another in the skull base, were identified. The defects were plugged with a pericranial vascularised graft and Surgicel, with subsequent application of a fibrin sealant (Beriplast). The bone flap was secured back into its original position and the wound was closed.
Figure 4.
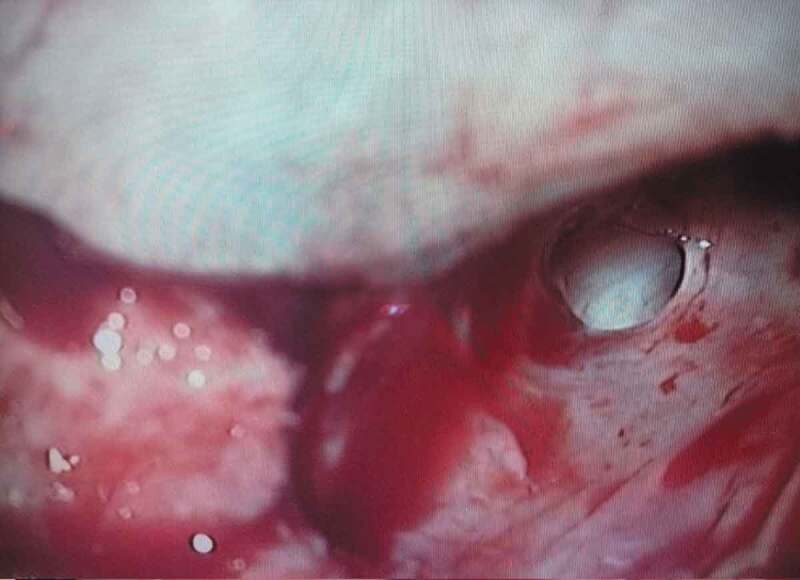
Defect seen intra-operatively in the medial wall of the orbit.
Postoperatively; the child remained stable, albeit irritable. The eye swelling seemed to be resolving (Figure 5) and the child remained active without any evidence of neurological deficits. The patient was closely monitored for a few days and then discharged home on IV antibiotics. The child was doing well one week later in his clinic follow up. The position of the left eye appeared to be slightly lower than the right one and there was mild left lid swelling. The incision looked well healed.
Figure 5.

Post-operative view.
Discussion
Orbital trauma is of crucial significance as it can result in loss of vision. The orbital cavity is a bony structure that contains and protects the eye and its associated structures. Injury to the orbit can result from both blunt and penetrating trauma. Trauma to the orbital walls causes swelling of the soft tissues and retroocular oedema, which results in vascular congestion. This leads to an increase in intra-orbital pressure, which propels the eyeball forward, causing proptosis and stretching the extra-ocular muscles and nerves and compressing the draining veins. The presence of a depressed orbital fracture worsens the process by further compromising the orbital space. This increased intra-orbital pressure can be associated with significant morbidity, as it can cause the occlusion of retinal veins and artery along with damage to the optic nerve. All of this can ultimately result in visual failure.9,10
Isolated orbital fractures can either be “blow-out” fractures or “blow-in” fractures. Blowout fractures commonly damage the inferior or medial orbital wall and can result in entrapment syndromes.9–11 Blow-in fractures can lead to a rise in intra-orbital pressure and impingement syndromes. Patients usually present with proptosis and limited extra-ocular movement with all cases requiring surgical intervention.1,9
As mentioned earlier, one of the consequences of orbital trauma can be the formation of a pseudomeningocele. A pseudomeningocele is sometimes also used interchangeably with the terms leptomeningeal cyst and growing skull fracture. A precise definition is not available because different mechanisms have been used to explain the pathogenesis of pseudomeningoceles. Most authors consider a pseudomeningocele as an extravasated collection of extradural CSF that results from a dural tear. As the extradural fluid may be contained in an arachnoid-lined membrane or in a fibrous capsule, multiple terms to describe this entity exist. It may arise due to iatrogenic injury, traumatic dural tears or a congenital anomaly.3,12 Pseudomeningoceles and growing skull fractures are caused by similar mechanisms and can therefore, be considered on a continuum. However, growing skull fractures occur gradually and should be suspected if ocular symptoms occur in a child who sustained a head injury several months or years prior.13,14 Pseudomeningoceles also lack the characteristic bony lytic defect of growing skull fractures.
There have been a few reports of more unusual complications such as complete herniation of the entire eyeball inside the anterior cranial fossa beneath the right frontal lobe following a right orbital roof fracture.15 Trauma causing objects to enter through the eyeball can cause penetrating damage to the brain, as the orbital roof is relatively thinner compared to other bones in the cranial vault and more susceptible to penetrating injury.16 The formation of a blepharocele (i.e. CSF leak and brain herniation into the eyelid) following orbital roof and rim fracture has also been reported.17
In 1953, Taveras and Ransohoff18 suggested a frequently cited mechanism for the formation of a leptomeningeal cyst. A dural tear underlying a skull fracture, due to trauma, is believed to be the single most important factor in the pathogenesis of leptomeningoceles. And it is likely that without a dural tear, the fractures would heal as expected. Subsequently, arachnoid tissue herniates through the dural tear and CSF collects inside the trapped leptomeninges, forming a cyst.
However, we believe a similar mechanism to what Bhandari et al.5 proposed (that is specific to traumatic orbital pseudomeningoceles in children) is what formed the pseudomeningocele in our case. CSF, that leaked through into the orbit via the torn dura and fracture, became trapped above the orbit and arachnoidal adhesions around the fracture site caused it to become encysted within a pseudomembrane. The entrapped pseudomeningocele led to proptosis and a tense orbit and was only relieved after surgical intervention.
Patients with post-traumatic pseudomeningoceles present in a variety of ways; the most common presentation being proptosis, either pulsatile7,8 or non-pulsatile.5 They may also present with bruit heard over the swelling, headache,5 seizures,19 post-traumatic epilepsy, progressively increasing swelling over the fracture, depression of the eyeball, diminution of vision,6 diplopia, displaced globe and restricted eye movements.
When possible, a complete neuro-ophthalmological examination and thorough palpation of orbital rims should be performed in all patients presenting with exophthalmos and ecchymosis, especially with a history of preceding trauma.10 Furthermore, early diagnosis is of vital importance in cases of orbital trauma. X-ray, CT, and MRI are modalities used in the diagnosis of pseudomeningoceles. Plain film X-rays can accurately show bony injury if present but there is a lack of soft tissue detail. CT scans are especially useful in detecting the bone fractures.19–21 MRI is useful for distinguishing pseudomeningoceles from other pathologies and is more sensitive in showing their intra-orbital extension.13,19 Associated pathologies, like encephalomalacia, subdural fluid collection, haematomas, and ventricular dilatation, can also be seen on CT and MRI.19 Such radiological scans of the orbits and skull can help in accurate diagnosis and selection of the appropriate surgical technique.
The recommendations for emergency orbital surgery following orbital trauma include progressive loss of vision, progressive proptosis and radiological demonstration of optic nerve compression by bony spicules.2 Our patient had presented with persistent proptosis as well as orbital cellulitis, hence the need for surgery. According to the literature, the standard treatment for such traumatic orbital injuries involves watertight repair of the dural defect and cranioplasty.19,21 Some authors have also used ventriculoperitoneal shunting to drain the CSF collection and improve symptoms.7,22,23 We opted to perform a left frontal craniotomy to repair the pseudomeningocele and closed the dural defects with a pericranial graft. Postoperatively, the child remained stable and resolution of proptosis was seen. While most cases of this nature have described using a frontal craniotomy to access the orbit, Sahoo et al. performed a fronto-orbital craniotomy using the fracture line of the orbital roof and frontal bone as edges of the craniotomy.24 They claim that this approach minimises bone loss and prevents complications like enophthalmos and transmitted pulsations in the obit. Furthermore, the bony defect above the dura can be repaired using a mesh or bone graft. While meshes may be used in adults, the physiological growth of the cranium in children may lead to subsequent orbital deformities if meshes are used.25 Instead, one may resort to using bone grafts such as a calvarial split graft used by Vankipuram et al., who reported a good cosmetic outcome with this technique.26
The threat of irreversible visual loss makes the early diagnosis and management of such cases vitally important. However, as these cases are rare, they can easily get overlooked and under-diagnosed. Even in the case of our patient, he was admitted for several days in another hospital in Karachi, where the medial wall fracture and resultant orbital pseudomeningocele could not be diagnosed. There is a need for a thorough examination and complete radiological work up of these patients, so they can be managed in a proper and timely manner.
Conclusion
This case highlights the importance of doing a complete neuro-ophthalmological examination and thorough palpation of orbital rims along with complete radiological workup of all patients presenting with exophthalmos and ecchymosis, especially with a history of preceding trauma. Traumatic orbital pseudomeningocele is a rare complication; however, if left untreated it can have serious consequences.
Declaration of interest statement
The authors declare that they have no conflict of interest.
References
- 1.Coon D, Yuan N, Jones D, Howell LK, Grant MP, Redett RJ.. Defining pediatric orbital roof fractures. Plast Reconstr Surg. 2014;134(3):442e–448e. doi: 10.1097/PRS.0000000000000421. [DOI] [PubMed] [Google Scholar]
- 2.Oppenheimer AJ, Monson LA, Buchman SR. Pediatric orbital fractures. Craniomaxillofac Trauma Reconstr. 2013;6(1):9–20. doi: 10.1055/s-0032-1332213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hawk MW, Kim KD. Review of spinal pseudomeningoceles and cerebrospinal fluid fistulas. Neurosurg Focus. 2000;9(1):1–8. doi: 10.3171/foc.2000.9.1.5. [DOI] [PubMed] [Google Scholar]
- 4.Smith GA, Strohl MP, Manjila S, Miller JP. Incidence, management, and outcome of symptomatic postoperative posterior fossa pseudomeningocele: a retrospective single-institution experience. Operative Neurosurg. 2016;12(3):298–304. doi: 10.1227/NEU.0000000000001329 [DOI] [PubMed] [Google Scholar]
- 5.Bhandari YS. Traumatic orbital pseudo-meningocele. J Neurosurg. 1969;30(5):612–614. doi: 10.3171/jns.1969.30.5.0612. [DOI] [PubMed] [Google Scholar]
- 6.Mahapatra AK, Tandon PN. Post-traumatic intradiploic pseudomeningocele in children. Acta Neurochir (Wien). 1989;100:120–126. [DOI] [PubMed] [Google Scholar]
- 7.Ranjan M, Arivazhagan A, Chandrajit P, Chandramouli BA. Unusual manifestation of an orbital roof fracture in a child: acute orbital leptomeningeal porencephalic cyst. Neurol India. 2010;58(6):974–975. doi: 10.4103/0028-3886.73773. [DOI] [PubMed] [Google Scholar]
- 8.Kumar R, Verma A, Sharma K, Rathi B, Malik V. Post-traumatic pseudomeningocele of the orbit in a young child. J Pediatr Ophthalmol Strabismus. 2003;40:110–112. [DOI] [PubMed] [Google Scholar]
- 9.Rothman M Orbital trauma. Semin Ultrasound, CT and MRI. 1997;18(6):437–447. doi: 10.1016/S0887-2171(97)90005-6 [DOI] [PubMed] [Google Scholar]
- 10.Jaiswal M, Sundar IV, Gandhi A, Purohit D, Mittal RS. Acute traumatic orbital encephalocele: a case report with review of literature. J Neurosci Rural Pract. 2013;4(4):467–470. doi: 10.4103/0976-3147.120209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Smith B, Regan WF. Blow-out fracture of the orbit; mechanism and correction of internal orbital fracture. Am J Ophthalmol. 1957;44:733–739. [DOI] [PubMed] [Google Scholar]
- 12.Richardson D, Duncan C, Sinha A, Hennedige AA. Pseudomeningocele with orbital extension as a complication of fronto-orbital advancement and remodeling in craniosynostosis. J Craniofac Surg. 2015;26:7. doi: 10.1097/SCS.0000000000001732. [DOI] [PubMed] [Google Scholar]
- 13.Suri A, Mahapatra AK. Growing fractures of the orbital roof. A report of two cases and a review. Pediatr Neurosurg. 2002;36(2):96–100. doi: 10.1159/000048360. [DOI] [PubMed] [Google Scholar]
- 14.Jamjoom ZAB . Growing fracture of the orbital roof. Surg Neurol. 1997;48(2): 184–188. [DOI] [PubMed] [Google Scholar]
- 15.Tripathi M, Varshney N, Batish A, Mohindra S. Eye in the brain. Neurol India. 2018;66(3):883–884. doi: 10.4103/0028-3886.232284. [DOI] [PubMed] [Google Scholar]
- 16.Satyarthee G, Borkar S, Tripathi A, Sharma B. Transorbital penetrating cerebral injury with a ceramic stone: report of an interesting case. Neurol India. 2009;57(3):331–333. doi: 10.4103/0028-3886.53285. [DOI] [PubMed] [Google Scholar]
- 17.Mishra A, Gupta D, Gamangatti S, Sharma B. Post-traumatic blepharocele: a rare manifestation of head injury. Neurol India. 2014;62(5):568–570. doi: 10.4103/0028-3886.144502. [DOI] [PubMed] [Google Scholar]
- 18.Taveras JM, Ransohoff J. Leptomeningeal cysts of the brain following trauma with erosion of the skull. J Neurosurg. 1953;10(3):233–241. doi: 10.3171/jns.1953.10.3.0233. [DOI] [PubMed] [Google Scholar]
- 19.Guler I, Buyukterzi M, Oner O, Tolu I. Post-traumatic leptomeningeal cyst in a child: computed tomography and magnetic resonance imaging findings. J Emerg Med. 2015;48(5):e121–e122. doi: 10.1016/j.jemermed.2014.12.042. [DOI] [PubMed] [Google Scholar]
- 20.Koç RK, Kurtsoy A, Öktem İS, Akdemir H. Growing skull fracture of the orbital roof. Pediatr Neurosurg. 1999;30(1):35–38. doi: 10.1159/000028758. [DOI] [PubMed] [Google Scholar]
- 21.Meier JD, Dublin AB, Strong EB. Leptomeningeal cyst of the orbital roof in an adult: case report and literature review. Skull Base. 2009;19(3):231–235. doi: 10.1055/s-0028-1096206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Smith DK, El-Sayed I, Pafundi E, Dolan RW. Presentation and treatment of a posttraumatic pseudomeningocele of the superior orbit. Am J Otolaryngol. 2000;21:219–221. [DOI] [PubMed] [Google Scholar]
- 23.Agrawal D, Mishra S. Post-traumatic intradiploic pseudomeningocele. Indian Pediatr. 2010;47:271–273. [DOI] [PubMed] [Google Scholar]
- 24.Sahoo SK, Salunke PS, Ghuman MS. Traumatic orbital encephalocele in an infant: using the fracture line to our advantage. Acta Neurochir (Wien). 2014;156(7):1357–1359. doi: 10.1007/s00701-014-2002-3. [DOI] [PubMed] [Google Scholar]
- 25.Arslan E, Arslan S, Kalkısım S, Arslan A, Kuzeyli K. Long-term results of orbital roof repair with titanium mesh in a case of traumatic intraorbital encephalocele: a case report and review of literature. Craniomaxillofac Trauma Reconstr. 2016;9(3):255–259. doi: 10.1055/s-0036-1581064. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Vankipuram S, Srivastava C, Ojha BK, Sahoo S. Penetrating orbital trauma leading to trans-orbital brain herniation. Childs Nerv Syst. 2018;34(2):373–375. doi: 10.1007/s00381-017-3600-1. [DOI] [PubMed] [Google Scholar]