

Abstract
Aims
Previous studies found a relationship between elevated phenylalanine levels and poor cardiovascular outcomes. Potential strategies are available to manipulate phenylalanine metabolism. This study investigated whether increased phenylalanine predicted mortality in critical patients with either acute heart failure (HF) or acute on chronic HF, and its correlation with inflammation and immune cytokines.
Methods and results
This study recruited 152 subjects, including 115 patients with HF admitted for critical conditions and 37 normal controls. We measured left ventricular ejection fraction (LVEF), plasma concentrations of phenylalanine, C‐reactive protein, albumin, pre‐albumin, transferrin, and pro‐inflammatory and immune cytokines. Acute Physiology and Chronic Health Evaluation (APACHE II), Sequential Organ Failure Assessment (SOFA), and maximal vasoactive–inotropic scores (VISmax) were calculated. Patients were followed up until death or a maximum of 1 year. The primary endpoint was all‐cause death. Of the 115 patients, 37 (32.2%) were admitted owing to acute HF, and 78 (67.8%) were admitted owing to acute on chronic HF; 64 (55.7%) had ST elevation/non‐ST elevation myocardial infarction. An LVEF measured during the hospitalization of <40%, 40–50%, and ≥50% was noted in 51 (44.3%), 15 (13.1%), and 49 (42.6%) patients, respectively. During 1 year follow‐up, 51 (44.3%) patients died. Death was associated with higher APACHE II, SOFA, and VISmax scores; higher levels of C‐reactive protein and phenylalanine; higher incidence of atrial fibrillation and use of inotropic agents; lower cholesterol, albumin, pre‐albumin, and transferrin levels; and significant changes in pro‐inflammatory and immune cytokines. Phenylalanine levels demonstrated an area under the receiver operating characteristic curve of 0.80 for mortality, with an optimal cut‐off value set at 112 μM. Phenylalanine ≥ 112 μM was associated with a higher mortality rate than was phenylalanine < 112 μM (80.5% vs. 24.3%, P < 0.001) [hazard ratio = 5.07 (2.83–9.05), P < 0.001]. The Kaplan–Meier curves revealed that phenylalanine ≥ 112 μM was associated with a lower accumulative survival rate (log rank = 36.9, P < 0.001). Higher phenylalanine levels were correlated with higher APACHE II and SOFA scores, higher C‐reactive protein levels and incidence of using inotropic agents, and changes in cytokines suggestive of immunosuppression, but lower levels of pre‐albumin and transferrin. Further multivariable analysis showed that phenylalanine ≥ 112 μM predicted death over 1 year independently of age, APACHE II and SOFA scores, atrial fibrillation, C‐reactive protein, cholesterol, pre‐albumin, transferrin, and interleukin‐8 and interleukin‐10.
Conclusions
Elevated phenylalanine levels predicted mortality in critical patients, phenotypically predominantly presenting with HF, independently of traditional prognostic factors and cytokines associated with inflammation and immunity.
Keywords: Phenylalanine, Prognosis, Heart failure, Biomarkers
Introduction
The mortality rate is high among patients in critical condition admitted to the intensive care unit with heart failure (HF). Risk stratification, currently estimated by general risk scores such as the Acute Physiology and Chronic Health Evaluation (APACHE II) and Sequential Organ Failure Assessment (SOFA) scores, 1 , 2 could be better. Multifaceted assessment of critical care patients remains an unmet need.
On the basis of advanced high‐throughput bioinformatics, we and others recently demonstrated that blood phenylalanine concentrations provide both diagnostic and prognostic value in patients with HF. 3 , 4 , 5 , 6 , 7 , 8 Moreover, the SABRE study and the British Women's Health and Heart Study, which have statistically powerful community cohorts, showed that higher phenylalanine levels were associated with increased cardiovascular risk. 9 Furthermore, a study based on the PROSPER and FINRISK cohorts demonstrated that elevated phenylalanine levels predicted HF‐related hospitalization in community cohorts at cardiovascular risk. 10 All evidence suggests a relationship between phenylalanine levels and poor cardiovascular outcomes. In these studies, the definition of HF included HF with reduced and preserved ejection fraction (HFrEF and HFpEF, respectively).
The metabolism of phenylalanine relates to the enzyme phenylalanine hydroxylase, which is functionally attenuated by inflammation. 11 , 12 The association between high phenylalanine levels and increased mortality rates in patients with sepsis also warrants further exploring inflammatory and immune profiles. 13 , 14 Furthermore, potential strategies are currently available to manipulate the function of phenylalanine hydroxylase. 15 Accordingly, this study was designed to investigate (i) whether phenylalanine levels predicted poor outcomes in critical patients with either acute HF or acute on chronic HF, including both HFrEF or HFpEF, because a substantial portion of patients with acute decompensated HF had HFpEF; (ii) the correlation of phenylalanine levels to inflammatory and immune cytokines; and (iii) whether the prognostic value of phenylalanine was independent of traditional risk stratification parameters and inflammation and immune profiles.
Methods
Patient enrolment
From April 2017 to September 2018, patients were consecutively enrolled at the cardiac intensive care unit on the basis of these inclusion criteria: (i) they were transferred to the intensive care unit owing to acute HF or acute on chronic HF; (ii) they had reduced left ventricular ejection fraction (LVEF < 40%, HFrEF), mid‐range (LVEF 40–49%, HFmrEF), or preserved LVEF (LVEF ≥ 50%, HFpEF) on the basis of the 2016 European Society of Cardiology guidelines for the diagnosis and treatment of acute and chronic HF 16 ; (iii) they had N‐terminal‐pro B‐type natriuretic peptide (NT‐proBNP) > 900 pg/mL 17 , 18 ; (iv) they were at critical status with an APACHE II score >15; (v) they needed to stay in the intensive care unit > 48 h; and (vi) they were older than 20 years. The exclusion criteria included the following: (i) patients with co‐morbid disorders other than the main cause for admission that might compromise their survival within 3 months, such as terminal stage cancer; or (ii) patients who died before the baseline blood collection for measuring phenylalanine. Acute on chronic HF presentation was defined by a prior diagnosis of HF on admission, chronic HFrEF, HFmrEF, or HFpEF. Prior diagnosis of HF was determined by reviewing medical records from our institution as well as any referring institution. Acute HF was characterized as a new diagnosis of HF on admission, including a variety of acute HF‐associated aetiologies and acute myocardial infarction with acute pulmonary oedema.
All patients provided informed consent. As normal controls (n = 37), we also enrolled participants who had normal LVEFs and did not have any systemic disease. The study was designed and carried out in accordance with the principles of the Declaration of Helsinki and with the approval from the Ethics Review Board of Chang Gung Memorial Hospital.
Scoring systems
Disease severity was evaluated by calculating SOFA, 1 APACHE II, 2 and maximal vasoactive–inotropic scores (VISmax) 19 on the first day of admission to the intensive care unit.
Blood sampling and examination
Fasting blood samples were collected in ethylenediaminetetraacetic acid‐containing tubes in the early morning, the day after obtaining informed consent. We analysed plasma phenylalanine by ultra‐performance liquid chromatography (UPLC) workflow. NT‐proBNP was measured using Elecsys proBNP sandwich immunoassay on an Elecsys 2010 (Roche Diagnostics, Basel, Switzerland). Measurement of other parameters, including estimated glomerular filtration rate, C‐reactive protein, haemoglobin, and albumin, was performed in the central laboratory.
Echocardiography
Two‐dimensional echocardiographic images (GE Vivid E9) with patients in the left lateral decubitus position were obtained, conducted according to the guidelines suggested by the American Society of Echocardiography. 20 We calculated the LVEF using the Simpson method. Patients with HFpEF or HFmrEF had to fit one of these criteria: (i) left atrial volume index > 34 mL/m2 or a left ventricular mass index ≥ 115 g/m2 for men and ≥95 g/m2 for women; and/or (ii) an E/e′ ≥ 13 and a mean e′ septal and lateral wall < 9 cm/s. 16 For a diagnosis of chronic HF, an echocardiogram performed in the 6 months before enrolment was acceptable. However, all patients had echocardiograms during hospitalization, either before enrolment or within 2 days of enrolment, and these were used for the final analysis.
Phenylalanine measurement
Plasma concentration of phenylalanine was quantified by UPLC. Plasma samples (100 μL) were precipitated with 10% sulfosalicylic acid. After protein precipitation and centrifugation, derivatization was initiated by AQC in acetonitrile. Amino acids were then analysed using the ACQUITY UPLC System, consisting of a binary solvent manager, a sample manager, and a tunable UV detector. We used EmpowerTM 2 Software to control the system and collect data. Separations were performed on a 2.1 × 100 mm ACQUITY BEH C18 column was at a flow rate of 0.70 mL/min. The average intra‐assay coefficient of variation was 2.6% for phenylalanine. The total coefficient of variation was 2.7% for phenylalanine. The detection limit was 3.3 μM. The linear range was 25–500 μM.
Cytokine measurement
Milliplex MAP Human high‐sensitivity T cell Magnetic Bead Panel (MILLIPLEX HSTCMAG‐28SK kit, Millipore Corporation, Billerica, MA, USA) was used to quantify the plasma cytokine levels. Antibody beads, controls, wash buffer, serum matrix, and standards were prepared following the manufacturer's instructions. After all procedures, the plate was analysed using the MAGPIX with xPONENT software. Measured cytokines included granulocyte‐macrophage colony‐stimulating factor (GM‐CSF), interferon (IFN), IFN‐inducible T cell alpha chemoattractant (ITAC), macrophage inflammatory protein (MIP), tumour necrosis factor (TNF), fractalkine, and a variety of interleukins (ILs).
Follow‐up program
Follow‐up data were prospectively obtained from hospital records, personal communication with the patients' physicians, telephone interviews with patients, and patients' regular visits to staff physician outpatient clinics. Patients were followed up until death or a maximum of 1 year. The primary endpoint was death from all causes.
Statistical analyses
Results are expressed as the mean ± SD for variables with normal distribution, as the median [inter‐quartile range (IQR)] for variables with skewed distribution, and as the number (percentage) for categorical variables. We compared data using the Mann–Whitney U test, Kruskal–Wallis H test, and χ 2, when appropriate. We estimated receiver operating characteristic (ROC) curve and used Youden's index to identify the cut‐off value of variables. Area under the curve (AUC) of ROCs was presented. A univariate Cox proportional hazards model was used to determine the variables' predictive value on mortality. By Cox multivariable analysis, we adjusted for covariates to better identify strong independent predictors of mortality using a forward selection model. Variables with a P value < 0.05 in a univariate analysis were included in the multivariable analysis. Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated. To compare time‐dependent outcomes, we performed Kaplan–Meier analyses with a log‐rank test. All statistical analyses were two‐sided and performed using SPSS software (Version 22.0, SPSS, Chicago, IL, USA). A P value of <0.05 was considered significant.
Results
Baseline characteristics and laboratory data
All patients (n = 115) had a high NT‐proBNP level [5922 pg/mL (IQR 1917–11 698 pg/mL)]. The baseline characteristics, laboratory data, and medications are shown in Table 1 and Table S1 . An LVEF measured during the hospitalization of <40%, 40–50%, and ≥50% was noted in 51 (44.3%), 15 (13.1%), and 49 (42.6%) patients, respectively. Of the 115 patients, 64 (55.7%) had ST elevation/non‐ST elevation myocardial infarction; 37 (32.2%) were admitted owing to acute HF, and 78 (67.8%) were admitted owing to acute on chronic HF. Seventeen (14.8%) had infection‐induced acute decompensation of chronic HF. All patients were at functional classification IV. Their average age was 71.7 years, and the average APACHE II and SOFA scores were 25.8 and 8.32, respectively.
Table 1.
Demographic and laboratory data
| All | Survival | Death | P value | |
|---|---|---|---|---|
| n = 115 | n = 64 | n = 51 | ||
| Age (years) | 71.7 ± 13.3 | 69.6 ± 13.7 | 74.3 ± 12.3 | 0.061 |
| Male (%) | 73 (63.4) | 38 (59.3) | 35 (68.6) | 0.335 |
| APACHE II score | 25.8 ± 7.02 | 23.6 ± 5.23 | 28.5 ± 8.01 | <0.001 |
| SOFA score | 8.32 ± 3.76 | 6.91 ± 3.29 | 10.1 ± 3.58 | <0.001 |
| VISmax score | 1.3 (0–16.4) | 1.1 (0–11.9) | 4.8 (0–30.5) | 0.009 |
| LVEF (%) | 46.3 ± 17.9 | 47.2 ± 17.5 | 45.3 ± 18.6 | 0.566 |
| NYHA Fc IV (%) | 115 (100) | 64 (100) | 51 (100) | 1.00 |
| Body mass index (kg/m2) | 25.0 ± 5.18 | 25.2 ± 4.95 | 24.7 ± 5.49 | 0.621 |
| Co‐morbidity | ||||
| Diabetes mellitus (%) | 60 (52.1) | 35 (54.6) | 25 (49.0) | 0.577 |
| Hypertension (%) | 83 (72.1) | 46 (71.8) | 37 (72.5) | 1.00 |
| Coronary artery disease (%) | 77 (67.0) | 40 (62.5) | 37 (72.5) | 0.431 |
| Atrial fibrillation (%) | 23 (20) | 7 (10.9) | 16 (31.3) | 0.009 |
| COPD (%) | 8 (6.9) | 7 (10.9) | 1 (1.9) | 0.075 |
| Chronic kidney disease (%) | 25 (21.7) | 17 (26.5) | 8 (15.6) | 0.179 |
| Ventilator use (%) | 99 (86.1) | 54 (84.3) | 45 (88.2) | 0.599 |
| Inotropic agent use (%) | 53 (46.0) | 19 (29.6) | 34 (66.7) | <0.001 |
| Days in ICU (day) | 13.9 ± 10.6 | 13.2 ± 10.5 | 14.9 ± 10.8 | 0.367 |
| Laboratory data | ||||
| WBC (1000/μL) | 13.5 ± 6.04 | 12.9 ± 5.79 | 14.1 ± 6.34 | 0.308 |
| Haemoglobin (g/dL) | 10.9 ± 2.85 | 11.2 ± 2.78 | 10.5 ± 2.92 | 0.245 |
| CRP (mg/L) | 17.0 (53.6–106) | 33.6 (6.9–58.1) | 83.0 (44.9–157) | <0.001 |
| Cholesterol (mg/dL) | 131 ± 47.8 | 143.4 ± 47.9 | 116 ± 43.5 | 0.002 |
| Triglyceride (mg/dL) | 109 (84–152) | 110 (82–152) | 109 (88–156) | 0.632 |
| Albumin (g/dL) | 3.20 ± 0.55 | 3.30 ± 0.48 | 3.08 ± 0.61 | 0.044 |
| eGFR (mL/min/1.73 m2) | 38.6 ± 32.3 | 43.8 ± 34.3 | 32.0 ± 28.5 | 0.053 |
| ALT (U/L) | 29 (18–57) | 29.5 (21.3–54.5) | 26 (16–72) | 0.630 |
| Serum sodium (mEq/L) | 141 ± 6.78 | 139 ± 5.74 | 142 ± 7.72 | 0.053 |
| Pre‐albumin (mg/dL) | 14.4 ± 6.77 | 16.7 ± 7.33 | 11.5 ± 4.65 | <0.001 |
| Transferrin (mg/dL) | 152 ± 48.6 | 164 ± 51.7 | 136 ± 39.9 | 0.002 |
| NT‐proBNP (ng/mL) | 5920 (1917–11 698) | 5900 (1874–10 680) | 5960 (1917–12 680) | 0.536 |
| Phenylalanine (μM) | 98.5 ± 50.6 | 80.1 ± 26.0 | 122 ± 63.3 | <0.001 |
APACHE II, Acute Physiology and Chronic Health Evaluation; ALT, alanine aminotransferase; COPD, chronic obstructive pulmonary disease; chronic kidney disease, estimated glomerular filtration rate (eGFR) < 60 mL/min/1.73 m2; CRP, C‐reactive protein; ICU, intensive care unit; LVEF, left ventricular ejection fraction; NT‐proBNP, N‐terminal‐pro B‐type natriuretic peptide; NYHA Fc, New York Heart Association functional classification; SOFA, Sequential Organ Failure Assessment; VISmax, maximal vasoactive–inotropic score in 24 h after enrolment; WBC, white blood cell count.
Data are expressed as the mean ± SD for variables with normal distribution, median [inter‐quartile range (IQR)] for variables with skewed distribution, and as number (percentage) for categorical variables.
Factors associated with mortality
During the 1 year follow‐up period, 51 (44.3%) patients died. In 31 (60.8%) patients, death occurred owing to infection, 6 (11.8%) died of HF, and 14 (27.5%) owing to critical cardiovascular conditions. Mortality was associated with higher APACHE II, SOFA, and VISmax scores; higher incidence of atrial fibrillation; and use of inotropic agents (Table 1 ). Death was also associated with higher C‐reactive protein and phenylalanine levels and lower cholesterol, albumin, pre‐albumin and transferrin levels but was not associated with NT‐proBNP levels.
Association of phenylalanine and cytokines to mortality
The association between phenylalanine levels and mortality was analysed. The ROC curve demonstrated an AUC of 0.80, with an optimal cut‐off value for phenylalanine set at 112 μM (Figure 1A ). The mortality rate in patients with phenylalanine ≥ 112 μM was significantly higher than that in patients with phenylalanine < 112 μM (80.5% vs. 24.3%, P < 0.001) (HR = 5.07, 95% CI = 2.83–9.05, P < 0.001) (Figure 1B ). In Figure 1C , the Kaplan–Meier curve revealed that a phenylalanine ≥ 112 μM was associated with a lower accumulative survival rate (log rank = 36.9, P < 0.001). For patients with LVEF < 40% and LVEF ≥ 40%, the AUCs were 0.83 and 0.78, respectively. The analysis was performed again after excluding patients with worsening HF induced by infection; it showed that the AUC was 0.81. As for pro‐inflammatory and immune cytokines, mortality correlated to higher levels of IL‐6, IL‐8, IL‐10, TNFα, MIP1β, MIP3α, and ITAC but lower levels of IL‐23 (Table 2 ).
Figure 1.
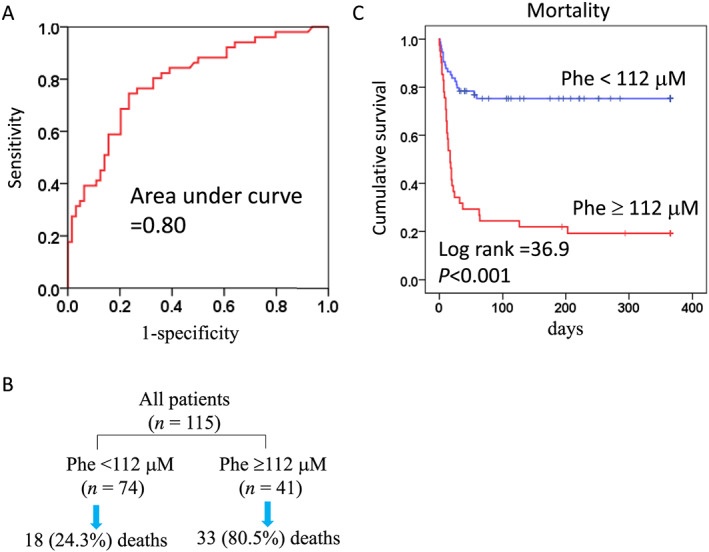
Prognostic value of phenylalanine and leucine. (A) The prognostic value of phenylalanine (Phe) is shown by the receiver operating characteristic curve. (B) The mortality rates in patients with Phe ≥ 112 μM vs. Phe < 112 μM. (C) The Kaplan–Meier curves for patients with Phe ≥ 112 μM vs. Phe < 112 μM.
Table 2.
Cytokines in patients of survival or death
| All | Survival | Death | ||
|---|---|---|---|---|
| pg/mL | n = 115 | n = 64 | n = 51 | P value |
| IL‐1β | 0.31 [0.21–0.68] | 0.37 [0.18–0.73] | 0.26 [0.21–0.63] | 0.800 |
| IL‐2 | 0.53 [0.25–1.04] | 0.54 [0.28–0.99] | 0.50 [0.25–1.08] | 0.848 |
| IL‐4 | 12.2 [6.09–37.3] | 18.0 [5.65–45.3] | 9.45 [6.09–32.8] | 0.190 |
| IL‐5 | 1.97 [1.02–3.57] | 2.07 [1.22–3.69] | 1.81 [0.96–3.49] | 0.181 |
| IL‐6 | 11.1 [3.60–28.9] | 6.99 [3.39–17.8] | 13.9 [5.62–38.2] | 0.005 |
| IL‐7 | 3.41 [1.99–4.91] | 3.58 [2.00–5.49] | 3.17 [1.99–4.83] | 0.642 |
| IL‐8 | 19.3 [9.55–40.9] | 12.6 [7.53–20.9] | 35.0 [20.4–89.9] | <0.001 |
| IL‐10 | 9.93 [5.54–14.5] | 7.73 [4.42–12.6] | 13.0 [7.94–24.8] | <0.001 |
| IL‐12‐p70 | 1.02 [0.55–1.55] | 1.07 [0.55–1.61] | 0.91 [0.51–1.45] | 0.327 |
| IL‐13 | 0.86 [0.33–1.78] | 0.86 [0.40–1.92] | 0.86 [0.33–1.78] | 0.589 |
| IL‐17A | 3.06 [2.04–4.83] | 3.40 [2.16–5.63] | 1.86 [2.95–4.02] | 0.111 |
| IL‐21 | 1.18 [0.54–2.48] | 1.23 [0.65–2.81] | 1.17 [0.54–2.27] | 0.230 |
| IL‐23 | 110 [54.9–233] | 134 [61.7–260] | 72.3 [42.2–163] | 0.011 |
| IFN‐γ | 2.74 [1.58–5.33] | 2.87 [1.76–5.47] | 2.67 [1.35–4.80] | 0.485 |
| TNFα | 7.07 [5.09–11.3] | 6.15 [4.35–8.73] | 9.30 [5.91–15.0] | 0.001 |
| MIP1α | 11.7 [8.93–15.9] | 11.3 [8.00–15.8] | 12.8 [9.02–17.5] | 0.365 |
| MIP1β | 8.79 [5.87–12.6] | 7.78 [5.35–11.3] | 10.4 [6.33–16.2] | 0.011 |
| MIP3α | 18.2 [8.58–47.9] | 11.8 [7.67–33.7] | 27.0 [14.1–86.0] | <0.001 |
| ITAC | 13.5 [8.86–27.1] | 12.3 [8.58–18.9] | 16.5 [9.27–32.3] | 0.028 |
| GM‐CSF | 6.37 [3.82–12.4] | 7.00 [3.95–13.7] | 5.61 [3.82–10.5] | 0.337 |
| Fractalkine | 65.2 [40.2–113] | 75.8 [40.7–115] | 54.4 [37.8–113] | 0.219 |
GM‐CSF, granulocyte‐macrophage colony‐stimulating factor; IL, interleukin; IFN, interferon; ITAC, interferon‐inducible T cell alpha chemoattractant; MIP, macrophage inflammatory protein; TNF, tumour necrosis factor.
Data are expressed as the median [inter‐quartile range (IQR)] because most of the variables are skewed distribution.
Characteristics of patients with high phenylalanine
Compared with patients with phenylalanine < 112 μM, patients with phenylalanine ≥ 112 μM had higher APACHE II and SOFA scores, higher incidence of using inotropic agents, and higher C‐reactive protein but lower pre‐albumin and transferrin levels (Table 3 ). We examined the differences in cytokines between normal controls and patients with different phenylalanine levels. The demographic characteristics of the normal controls are shown in Table S2 . The phenylalanine levels in the normal controls were 67.8 ± 13.1 μM (95% CI = 63.4–72.2 μM). Compared with normal controls, patients admitted to the intensive care unit had significantly higher levels of IL‐6, IL‐8, IL‐10, TNFα, MIP1β, MIP3α, and ITAC but lower levels of IL‐1β, IL‐2, IL‐4, IL‐5, IL‐7, IL‐12‐p70, IL‐17A, IL‐21, IL‐23, IFN‐γ, GM‐CSF, and fractalkine (Table 4 ). Because normal controls were younger than our patients, patients were age and sex matched to the normal controls ( Table S3 ). The comparison in cytokines between normal controls and matched patients reconfirmed these findings (Table S4 ). Furthermore, compared with patients with phenylalanine < 112 μM, patients with phenylalanine ≥ 112 μM had significantly higher levels of IL‐8, IL‐10, TNFα, MIP1β, MIP3α, and ITAC (Table 4 ).
Table 3.
Comparisons of demographic and laboratory data in patients with different levels of phenylalanine
| Phe < 112 μM | Phe ≥ 112 μM | ||
|---|---|---|---|
| n = 74 | n = 41 | P value | |
| Age (years) | 70.6 ± 13.5 | 73.6 ± 12.6 | 0.253 |
| Male (%) | 45 (60.8) | 28 (68.2) | 0.545 |
| APACHE II score | 18.5 ± 6.16 | 21.1 ± 5.32 | 0.029 |
| SOFA score | 7.62 ± 3.66 | 9.59 ± 3.64 | 0.007 |
| VISmax score | 0 (0–12.8) | 1.04 (0–22.5) | 0.561 |
| LVEF (%) | 48.0 ± 18.5 | 43.2 ± 16.4 | 0.161 |
| NYHA Fc IV | 74 (100) | 41 (100) | 1.00 |
| Body mass index (kg/m2) | 25.3 ± 5.33 | 24.3 ± 4.88 | 0.289 |
| Co‐morbidity | |||
| Diabetes mellitus (%) | 41 (55.4) | 19 (46.3) | 0.436 |
| Hypertension (%) | 52 (70.2) | 31 (75.6) | 0.665 |
| Coronary artery disease (%) | 49 (66.2) | 28 (68.3) | 1.00 |
| Atrial fibrillation (%) | 11 (14.8) | 12 (29.2) | 0.088 |
| COPD (%) | 6 (8.1) | 2 (4.8) | 0.710 |
| Chronic kidney disease (%) | 15 (20.2) | 10 (24.3) | 0.642 |
| Ventilator use (%) | 60 (81.0) | 39 (95.1) | 0.048 |
| Inotropic agent use (%) | 30 (40.5) | 23 (56.0) | 0.122 |
| Days in ICU (day) | 13.1 ± 10.7 | 15.4 ± 10.3 | 0.275 |
| Laboratory data | |||
| WBC (1000/μL) | 13.1 ± 5.68 | 14.0 ± 6.65 | 0.419 |
| Haemoglobin (g/dL) | 10.8 ± 2.42 | 10.8 ± 3.51 | 0.937 |
| CRP (mg/L) | 36.5 (9.36–61.3) | 89.3 (51.0–154) | <0.001 |
| Cholesterol (mg/dL) | 137 ± 50.9 | 119 ± 39.6 | 0.040 |
| Triglyceride (mg/dL) | 108 (82.0–149) | 110 (85.0–168) | 0.524 |
| Albumin (g/dL) | 3.20 ± 0.53 | 3.18 ± 0.58 | 0.841 |
| eGFR (mL/min/1.73 m2) | 42.6 ± 35.8 | 31.2 ± 23.1 | 0.041 |
| ALT (U/L) | 18.0 (28.5–53.5) | 18.0 (37.0–139) | 0.308 |
| Serum sodium (mEq/L) | 139 ± 6.10 | 142 ± 7.72 | 0.086 |
| Pre‐albumin (mg/dL) | 15.7 ± 7.19 | 12.0 ± 5.21 | 0.002 |
| Transferrin (mg/dL) | 154 ± 49.5 | 146 ± 47.0 | 0.371 |
| NT‐proBNP (ng/mL) | 5760 (1959–10 591) | 8360 (1819–15 420) | 0.538 |
ALT, alanine aminotransferase; chronic kidney disease, estimated glomerular filtration rate (eGFR) < 60 mL/min/1.73 m2; COPD, chronic obstructive pulmonary disease; CRP, C‐reactive protein; ICU, intensive care unit; LVEF, left ventricular ejection fraction; NT‐proBNP, N‐terminal‐pro B‐type natriuretic peptide; NYHA Fc, New York Heart Association functional classification; VISmax, maximal vasoactive–inotropic score in 24 h after enrolment.
Data are expressed as the mean ± SD for variables with normal distribution, median [inter‐quartile range (IQR)] for variables with skewed distribution, and number (percentage) for categorical variables.
Table 4.
Comparisons of cytokines in normal controls and patients with different levels of phenylalanine (Phe)
| Normal | Phe < 112 μM | Phe ≥ 112 μM | ||
|---|---|---|---|---|
| Variable | (n = 37) | (n = 74) | (n = 41) | P value a |
| IL‐1β | 0.91 [0.57–1.49] | 0.30 [0.20–0.70] ** | 0.36 [0.21–0.66] ** | <0.001 |
| IL‐2 | 0.94 [0.68–1.17] | 0.49 [0.22–0.93] ** | 0.61 [0.35–1.13] * | <0.001 |
| IL‐4 | 42.3 [27.5–67.5] | 13.73 [5.35–41.86] ** | 9.88 [7.03–36.7] ** | <0.001 |
| IL‐5 | 3.83 [2.94–5.08] | 2.01 [1.01–3.55] ** | 1.88 [1.02–3.64] ** | <0.001 |
| IL‐6 | 0.87 [0.60–1.31] | 9.18 [3.47–25.71] ** | 12.6 [5.30–36.5] ** | <0.001 |
| IL‐7 | 5.94 [4.39–8.06] | 3.71 [2.02–5.09] ** | 3.13 [1.99–4.75] ** | <0.001 |
| IL‐8 | 3.06 [2.68–4.02] | 14.08 [7.98–26.63] ** | 36.2 [21.9–58.9] ** , ‡ | <0.001 |
| IL‐10 | 7.47 [5.11–11.05] | 7.84 [4.67–13.50] | 13.1 [9.84–23.9] ** , ‡ | <0.001 |
| IL‐12‐p70 | 1.92 [1.61–2.69] | 1.05 [0.54–1.59] ** | 0.93 [0.54–1.52] ** | <0.001 |
| IL‐13 | 1.13 [0.67–2.23] | 0.68 [0.33–1.70] | 1.00 [0.40–2.31] | <0.062 |
| IL‐17A | 4.94 [4.15–6.78] | 3.11 [2.07–4.56] ** | 3.06 [2.01–4.85] ** | <0.001 |
| IL‐21 | 2.54 [1.74–3.60] | 1.18 [0.54–2.55] ** | 1.29 [0.57–2.42] ** | <0.001 |
| IL‐23 | 259 [166–380] | 118.83 [54.23–224.03] ** | 91.7 [52.1–243] ** | <0.001 |
| IFN‐γ | 5.66 [4.63–7.29] | 2.42 [1.51–5.02] ** | 3.34 [1.82–5.98] ** | <0.001 |
| TNFα | 3.35 [2.75–3.82] | 6.65 [4.62–10.76] ** | 8.12 [5.64–14.10] ** , † | <0.001 |
| MIP1α | 13.4 [10.8–16.0] | 11.05 [7.87–16.078] | 13.1 [10.4–16.7] | 0.092 |
| MIP1β | 4.95 [3.52–6.44] | 7.92 [5.31–11.36] ** | 11.0 [6.39–20.3] ** , ‡ | <0.001 |
| MIP3α | 7.49 [5.23–9.75] | 13.26 [7.91–34.10] ** | 32.6 [14.4–84.1] ** , ‡ | <0.001 |
| ITAC | 7.74 [6.28–9.67] | 12.46 [8.35–18.93] ** | 17.0 [10.61–34.38] ** , † | <0.001 |
| GM‐CSF | 16.9 [12.3–23.8] | 6.54 [3.83–12.84] ** | 5.79 [3.82–12.03] ** | <0.001 |
| Fractalkine | 104 [70.9–126] | 64.38 [39.23–118.50] * | 65.3 [42.0–105] * | 0.01 |
GM‐CSF, granulocyte‐macrophage colony‐stimulating factor; IL, interleukin; IFN, interferon; ITAC, interferon‐inducible T cell alpha chemoattractant; MIP, macrophage inflammatory protein; TNF, tumour necrosis factor.
Data are presented as median [inter‐quartile range].
P < 0.05.
P < 0.01, compared with ‘normal’.
P < 0.05.
P < 0.01, compared with ‘Phe < 112 μM’.
Indicates use of Kruskal–Wallis H test.
Cox univariate and multivariable analyses for mortality
The value of cytokines in predicting mortality was estimated by Cox univariate and multivariable analyses ( Table S5 ). The univariate analysis showed that higher IL‐6, IL‐8, IL‐10, TNFα, MIP1β, MIP3α, and ITAC but lower IL‐23 were associated with a higher mortality rate. Multivariable analysis revealed that only IL‐8 and IL‐10 were independent predictors of mortality. Then we analysed all significant prognostic parameters in the univariate analysis, including clinical and laboratory variables, phenylalanine, and cytokines, together (Table 5 ). The multivariable analysis with a forward selection model demonstrated that only phenylalanine ≥ 112 μM, VISmax, IL‐8, and IL‐10 were independent predictors of mortality over 1 year. Further multivariable analysis revealed that phenylalanine ≥ 112 μM independently predicted mortality after adjusting for age, APACHE II score, SOFA score, atrial fibrillation, CRP, cholesterol, pre‐albumin, and transferrin. After the analysis patients with decompensated HF induced by infection were excluded, phenylalanine ≥ 112 μM remained a significant predictor of mortality after adjusting for the same variables (HR = 2.88, 95% CI = 1.42–5.84, P = 0.003).
Table 5.
Cox univariate and multivariable analyses of factors for predicting mortality
| Univariate | Multivariable a | Multivariable b | ||||
|---|---|---|---|---|---|---|
| HR (95% CI) | P value | HR (95% CI) | P value | HR (95% CI) | P value | |
| Phenylalanine ≥ 112 μM | 5.06 (2.83–9.05) | <0.001 | 3.09 (1.66–5.76) | <0.001 | 2.57 (1.28–5.16) | <0.001 |
| APACHE II score | 1.08 (1.03–1.13) | 0.002 | ||||
| SOFA score | 1.17 (1.09–1.26) | <0.001 | ||||
| VISmax score | 1.04 (1.03–1.06) | <0.001 | 1.03 (1.01–1.05) | 0.006 | 1.04 (1.02–1.07) | 0.001 |
| Atrial fibrillation | 2.47 (1.36–4.47) | 0.003 | ||||
| CRP (log) | 3.20 (1.82–5.63) | <0.001 | ||||
| Cholesterol (mg/dL) | 0.99 (0.98–0.99) | 0.003 | ||||
| Pre‐albumin (mg/dL) | 0.90 (0.85–0.95) | <0.001 | ||||
| Transferrin (mg/dL) | 0.99 (0.98–0.99) | 0.004 | ||||
| IL‐8 (log) × 10−1 | 1.24 (1.17–1.33) | <0.001 | 1.10 (1.01–1.19) | 0.024 | 1.17 (1.08–1.28) | <0.001 |
| IL‐10 (log) × 10−1 | 1.27 (1.16–1.39) | <0.001 | 1.13 (1.02–1.25) | 0.026 | 1.20 (1.08–1.33) | 0.001 |
APACHE II, Acute Physiology and Chronic Health Evaluation; CI, confidence interval; CRP, C‐reactive protein; HR, hazard ratio; IL, interleukin; SOFA, Sequential Organ Failure Assessment; VISmax, maximal vasoactive–inotropic scores in 24 h after enrolment.
Multivariable analysis with forward selection model for all variables with P < 0.05 in the univariate analysis.
Adjusted for age, APACHE II score, SOFA score, atrial fibrillation, CRP, cholesterol, pre‐albumin, and transferrin.
Discussion
Increased plasma concentrations of phenylalanine predicted mortality in critical patients, phenotypically predominantly presenting with HF. Higher phenylalanine levels were correlated with higher APACHE II and SOFA scores, substantial inflammation, changes in cytokines suggestive of immunodepression, and malnutrition. In addition, the prognostic value of phenylalanine was independent of traditional risk scores and factors as well as pro‐inflammatory and immune cytokines.
Traditional risk assessment tools
Recent comprehensive HF surveys reveal that the 1 year mortality rates after discharge from acute HF vary widely, from 10% to 32% in the REPORT‐HF (International Registry to Assess Medical Practice with Longitudinal Observation for Treatment of HF) 21 to 40% in the GWTG‐HF (Get With The Guidelines‐Heart Failure) registry. 22 In the ARIC (Atherosclerosis Risk in Communities) study, the in‐hospital mortality rate for patients with acute decompensated HF was 7%. 23 Our study consistently showed that the 1 year mortality rate was 44.3%, including both in‐hospital and 1 year post discharge deaths. Risk assessment is mandatory for critical care. In this study, patients were admitted to the intensive care unit mainly for cardiovascular causes rather than infection. Natriuretic peptide levels were remarkably elevated in all patients and thus demonstrated no further prognostic value. Unexpectedly, LVEF was not a significant predictor of death within 1 year post discharge, probably because we included both HFrEF and HFpEF and because LVEF measured post coronary intervention or under use of inotropic agents had a confounding effect. A variety of scoring systems and nutritional indexes have been developed for predicting outcomes for patients with critical illness, such as APACHE II, SOFA, and VISmax scores, 1 , 19 , 24 albumin, pre‐albumin, 25 , 26 , 27 and transferrin. 28 The value of these parameters was repeatedly confirmed in our study. However, phenylalanine levels predicted mortality independently of all other parameters. Phenylalanine ≥ 112 μM, as a single variable, was associated with a 1 year mortality rate of 80.5%, remarkably higher than the 24.3% one‐year mortality rate among patients with phenylalanine < 112 μM.
Increased phenylalanine levels and mortality
The association between increased phenylalanine levels and mortality has not been previously explored. Here, we provide a few indirect mechanisms. Higher phenylalanine levels were correlated with higher C‐reactive protein levels and higher pro‐inflammatory, innate, and adaptive T lymphocyte immune cytokines such as IL‐8 and IL‐10. Although the inflammation in our patients was raised, it was different from patients with sepsis, as shown by the low levels of IFN‐γ compared with the normal controls. Generally, our patients, as compared with the normal controls, had a comparatively high level of inflammation (increased IL‐6, IL‐8, TNFα, MIP1β, and MIP3α) but suppressed immunity (increased IL‐10 and decreased IL‐4 and IL‐12). Furthermore, these phenomena were even more remarkable in patients with higher phenylalanine levels. Although suppressed immunity was suggested only by the level of cytokines and needs further confirmation, it may be closely related to the increased mortality rate, because the leading cause of mortality in our study population was infection. The compromised immune system identified by increased phenylalanine may be a pivotal area for further research by immuno‐phenotyping the patients and tackling their poor outcomes. On the other hand, it is worth noting that our previous study revealed that an elevated phenylalanine level was also associated with severe infection and mortality. 14 Therefore, it was necessary to clarify the confounding effect of infection on our findings in this study. After patients with infection‐induced acute decompensation were excluded, our further analysis demonstrated that phenylalanine remained an independent predictor of mortality.
Congenital phenylketonuria involves a deficiency of phenylalanine hydroxylase leading to extremely high phenylalanine concentrations. 29 The moderately increased phenylalanine level in our patients might be associated with insufficient tetrahydrobiopterin (BH4), the co‐factor for phenylalanine hydroxylase. 15 Inflammation‐induced production of reactive oxygen species may consume a significant portion of BH4, which can be assumed to leave phenylalanine unmetabolized. 15 , 30 Moreover, in humans, it has been shown that pro‐inflammatory cytokine‐mediated inflammation paradoxically increases the production of neopterin at the expense of the production of BH4. 12 , 31 Insufficient bioavailability of BH4 also leads to dysfunction in multiple systems, including nitric oxide synthase, tryptophan metabolism, the catecholamine pathway, the neural system, and thyroid hormone production. 15 , 30 , 31 , 32 Moreover, recent reports also demonstrate that insufficient BH4 causes impaired T cell proliferation and function. 33 However, owing to its vulnerability to oxidation, it is difficult to correctly measure BH4 on a routine basis. Elevated phenylalanine is a surrogate for significant BH4 deficiency.
The prognostic value of phenylalanine was independent of inflammation and immune cytokines, suggesting that phenylalanine also predicted poor outcomes via other mechanisms. Previously, we found that patients with elevated phenylalanine levels had substantially more incompletely metabolized waste of fatty acids in the circulation owing to impaired mitochondrial β‐oxidation, indicating dysfunctional energy production machinery. 8 The increase of blood phenylalanine concentration also represents substantial tissue breakdown, which is probably related to insufficient tissue perfusion and increased insulin resistance. 10 In addition, consistent with our previous reports, 8 these patients had low pre‐albumin levels indicating severe malnutrition. All these factors potentially contribute to poor outcomes.
Although the cut‐off value of phenylalanine is pivotal for clinical application, so far, no consensus has been reached. We hereby offer a cut‐off at 112 μM in patients at critical status; however, cut‐offs may differ in various populations and for different outcomes of interest. For example, previously, we identified the cut‐offs for predicting mortality at 84 μM in patients with severe infection 14 and at 88.9 μM among patients with not critically decompensated HF (for predicting composite events of all‐cause death or HF‐related re‐hospitalization). 8 In the study by Delles et al., 10 utilizing different measuring instruments (nuclear magnetic resonance), the phenylalanine concentration values for predicting HF‐related hospitalization were 47.85 (43.30–52.40) vs. 45.10 (40.70–49.80) μM in the high‐risk and low‐risk community cohorts, respectively. The values were generally lower than our measurements done using UPLC. Future studies need to establish cut‐offs on the basis of the same quantification platform.
Study limitations
BH4 deficiency was not directly measured in patients with increased phenylalanine levels. Further efforts need to quantify the amount of BH4 to provide direct evidence. With regard to immunity, although we measured the concentrations of cytokines that regulate or are secreted by T lymphocytes, enumerating innate and adaptive lymphocytes, as measured by flow cytometry, may strengthen the mechanisms associated with increased phenylalanine levels. Finally, the small sample size is definitely a limitation of our study. However, the findings of this study add further support to the notion that phenylalanine provides significant prognostic value, as we previously demonstrated in cohorts of HF and patients at high risk for sepsis. 3 , 7 , 8 , 14
Conclusions
Increased plasma concentration of phenylalanine and disturbed phenylalanine metabolism predict poor outcomes in critical patients phenotypically predominantly presenting with HF, independently of traditional prognostic factors and cytokines associated with inflammation and T lymphocyte immunity. Our study provides additional support to the findings of recent large‐scale cohort studies regarding the value of measuring phenylalanine.
Conflict of Interest
None.
Funding
This study was supported in part by the Ministry of Science and Technology of Taiwan (MOST107‐2314‐B‐182‐071‐MY2) and Chang Gung Memorial Hospital (CMRPG2G0591, 2G0601, 2G0621, 2G0631).
Supporting information
Table S1. Demographic and laboratory data in patients with different left ventricular ejection fractions.
Table S2. Demographic and laboratory data in patients and normal controls.
Table S3. Demographic and laboratory data of patients with sex and age matched to normal controls.
Table S4. Cytokines in patients with sex and age matched to normal controls.
Table S5. COX univariate and multivariable analysis of cytokines for predicting mortality.
Chen, W.‐S. , Wang, C.‐H. , Cheng, C.‐W. , Liu, M.‐H. , Chu, C.‐M. , Wu, H.‐P. , Huang, P.‐C. , Lin, Y.‐T. , Ko, T. , Chen, W.‐H. , Wang, H.‐J. , Lee, S.‐C. , and Liang, C.‐Y. (2020) Elevated plasma phenylalanine predicts mortality in critical patients with heart failure. ESC Heart Failure, 7: 2884–2893. 10.1002/ehf2.12896.
References
- 1. Vincent JL, Moreno R, Takala J, Willatts S, De Mendonca A, Bruining H, Reinhart CK, Suter PM, Thijs LG. The SOFA (Sepsis‐related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis‐Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med 1996; 22: 707–710. [DOI] [PubMed] [Google Scholar]
- 2. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med 1985; 13: 818–829. [PubMed] [Google Scholar]
- 3. Cheng ML, Wang CH, Shiao MS, Liu MH, Huang YY, Huang CY, Mao CT, Lin JF, Ho HY, Yang NI. Metabolic disturbances identified in plasma are associated with outcomes in patients with heart failure: diagnostic and prognostic value of metabolomics. J Am Coll Cardiol 2015; 65: 1509–1520. [DOI] [PubMed] [Google Scholar]
- 4. Hunter WG, Kelly JP, McGarrah RW 3rd, Kraus WE, Shah SH. Metabolic dysfunction in heart failure: diagnostic, prognostic, and pathophysiologic insights from metabolomic profiling. Curr Heart Fail Rep 2016; 13: 119–131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Alexander D, Lombardi R, Rodriguez G, Mitchell MM, Marian AJ. Metabolomic distinction and insights into the pathogenesis of human primary dilated cardiomyopathy. Eur J Clin Invest 2011; 41: 527–538. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Tenori L, Hu X, Pantaleo P, Alterini B, Castelli G, Olivotto I, Bertini I, Luchinat C, Gensini GF. Metabolomic fingerprint of heart failure in humans: a nuclear magnetic resonance spectroscopy analysis. Int J Cardiol 2013; 168: e113–e115. [DOI] [PubMed] [Google Scholar]
- 7. Wang CH, Cheng ML, Liu MH. Amino acid‐based metabolic panel provides robust prognostic value additive to B‐natriuretic peptide and traditional risk factors in heart failure. Dis Markers 2018; 2018: 3784589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Wang CH, Cheng ML, Liu MH. Simplified plasma essential amino acid‐based profiling provides metabolic information and prognostic value additive to traditional risk factors in heart failure. Amino Acids 2018; 50: 1739–1748. [DOI] [PubMed] [Google Scholar]
- 9. Wurtz P, Havulinna AS, Soininen P, Tynkkynen T, Prieto‐Merino D, Tillin T, Ghorbani A, Artati A, Wang Q, Tiainen M, Kangas AJ, Kettunen J, Kaikkonen J, Mikkila V, Jula A, Kahonen M, Lehtimaki T, Lawlor DA, Gaunt TR, Hughes AD, Sattar N, Illig T, Adamski J, Wang TJ, Perola M, Ripatti S, Vasan RS, Raitakari OT, Gerszten RE, Casas JP, Chaturvedi N, Ala‐Korpela M, Salomaa V. Metabolite profiling and cardiovascular event risk: a prospective study of 3 population‐based cohorts. Circulation 2015; 131: 774–785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Delles C, Rankin NJ, Boachie C, McConnachie A, Ford I, Kangas A, Soininen P, Trompet S, Mooijaart SP, Jukema JW, Zannad F, Ala‐Korpela M, Salomaa V, Havulinna AS, Welsh P, Wurtz P, Sattar N. Nuclear magnetic resonance‐based metabolomics identifies phenylalanine as a novel predictor of incident heart failure hospitalisation: results from PROSPER and FINRISK 1997. Eur J Heart Fail 2018; 20: 663–673. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Murr C, Grammer TB, Meinitzer A, Kleber ME, Marz W, Fuchs D. Immune activation and inflammation in patients with cardiovascular disease are associated with higher phenylalanine to tyrosine ratios: the ludwigshafen risk and cardiovascular health study. J Amino Acids 2014; 2014: 783730. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Neurauter G, Schrocksnadel K, Scholl‐Burgi S, Sperner‐Unterweger B, Schubert C, Ledochowski M, Fuchs D. Chronic immune stimulation correlates with reduced phenylalanine turnover. Curr Drug Metab 2008; 9: 622–627. [DOI] [PubMed] [Google Scholar]
- 13. Ploder M, Neurauter G, Spittler A, Schroecksnadel K, Roth E, Fuchs D. Serum phenylalanine in patients post trauma and with sepsis correlate to neopterin concentrations. Amino Acids 2008; 35: 303–307. [DOI] [PubMed] [Google Scholar]
- 14. Huang SS, Lin JY, Chen WS, Liu MH, Cheng CW, Cheng ML, Wang CH. Phenylalanine‐ and leucine‐defined metabolic types identify high mortality risk in patients with severe infection. Int J Infect Dis 2019; 85: 143–149. [DOI] [PubMed] [Google Scholar]
- 15. Bendall JK, Douglas G, McNeill E, Channon KM, Crabtree MJ. Tetrahydrobiopterin in cardiovascular health and disease. Antioxid Redox Signal 2014; 20: 3040–3077. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, Falk V, González‐Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GM, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail 2016; 18: 891–975. [DOI] [PubMed] [Google Scholar]
- 17. Januzzi JL Jr, Chen‐Tournoux AA, Christenson RH, Doros G, Hollander JE, Levy PD, Nagurney JT, Nowak RM, Pang PS, Patel D, Peacock WF, Rivers EJ, Walters EL, Gaggin HK. N‐terminal pro‐B‐type natriuretic peptide in the emergency department: the ICON‐RELOADED study. J Am Coll Cardiol 2018; 71: 1191–1200. [DOI] [PubMed] [Google Scholar]
- 18. Januzzi JL Jr, Camargo CA, Anwaruddin S, Baggish AL, Chen AA, Krauser DG, Tung R, Cameron R, Nagurney JT, Chae CU, Lloyd‐Jones DM, Brown DF, Foran‐Melanson S, Sluss PM, Lee‐Lewandrowski E, Lewandrowski KB. The N‐terminal Pro‐BNP investigation of dyspnea in the emergency department (PRIDE) study. Am J Cardiol 2005; 95: 948–954. [DOI] [PubMed] [Google Scholar]
- 19. Koponen T, Karttunen J, Musialowicz T, Pietiläinen L, Uusaro A, Lahtinen P. Vasoactive–inotropic score and the prediction of morbidity and mortality after cardiac surgery. Br J Anaesth 2019; 122: 428–436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Mitchell C, Rahko PS, Blauwet LA, Canaday B, Finstuen JA, Foster MC, Horton K, Ogunyankin KO, Palma RA, Velazquez EJ. Guidelines for performing a comprehensive transthoracic echocardiographic examination in adults: recommendations from the American Society of Echocardiography. J Am Soc Echocardiogr 2019; 32: 1–64. [DOI] [PubMed] [Google Scholar]
- 21. Tromp J, Bamadhaj S, Cleland JGF, Angermann CE, Dahlstrom U, Ouwerkerk W, Tay WT, Dickstein K, Ertl G, Hassanein M, Perrone SV, Ghadanfar M, Schweizer A, Obergfell A, Lam CSP, Filippatos G, Collins SP. Post‐discharge prognosis of patients admitted to hospital for heart failure by world region, and national level of income and income disparity (REPORT‐HF): a cohort study. Lancet Glob Health 2020; 8: e411–e422. [DOI] [PubMed] [Google Scholar]
- 22. Parikh KS, Sheng S, Hammill BG, Yancy CW, Fonarow GC, Hernandez AF, DeVore AD. Characteristics of acute heart failure hospitalizations based on presenting severity. Circ Heart Fail 2019; 12: e005171. [DOI] [PubMed] [Google Scholar]
- 23. Mounsey LA, Chang PP, Sueta CA, Matsushita K, Russell SD, Caughey MC. In‐hospital and postdischarge mortality among patients with acute decompensated heart failure hospitalizations ending on the weekend versus weekday: the ARIC Study Community Surveillance. J Am Heart Assoc 2019; 8: e011631. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Vasilyev S, Schaap RN, Mortensen JD. Hospital survival rates of patients with acute respiratory failure in modern respiratory intensive care units. An international, multicenter, prospective survey. Chest 1995; 107: 1083–1088. [DOI] [PubMed] [Google Scholar]
- 25. Lee SH, Kim SJ, Choi YH, Lee JH, Chang JH, Ryu YJ. Clinical outcomes and prognostic factors in patients directly transferred to the intensive care unit from long‐term care beds in institutions and hospitals: a retrospective clinical study. BMC Geriatr 2018; 18: 259. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Park JE, Chung KS, Song JH, Kim SY, Kim EY, Jung JY, Kang YA, Park MS, Kim YS, Chang J, Leem AY. The C‐reactive protein/albumin ratio as a predictor of mortality in critically ill patients. J Clin Med 2018; 7: 333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Arabi YM, Aldawood AS, Al‐Dorzi HM, Tamim HM, Haddad SH, Jones G, McIntyre L, Solaiman O, Sakkijha MH, Sadat M, Mundekkadan S, Kumar A, Bagshaw SM, Mehta S. Permissive underfeeding or standard enteral feeding in high‐ and low‐nutritional‐risk critically ill adults. Post hoc analysis of the PermiT Trial. Am J Respir Crit Care Med 2017; 195: 652–662. [DOI] [PubMed] [Google Scholar]
- 28. Lasocki S, Lefebvre T, Mayeur C, Puy H, Mebazaa A, Gayat E. Iron deficiency diagnosed using hepcidin on critical care discharge is an independent risk factor for death and poor quality of life at one year: an observational prospective study on 1161 patients. Crit Care 2018; 22: 314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Blau N, van Spronsen FJ, Levy HL. Phenylketonuria. Lancet 2010; 376: 1417–1427. [DOI] [PubMed] [Google Scholar]
- 30. Nishijima Y, Sridhar A, Bonilla I, Velayutham M, Khan M, Terentyeva R, Li C, Kuppusamy P, Elton TS, Terentyev D, Gyorke S, Zweier JL, Cardounel AJ, Carnes CA. Tetrahydrobiopterin depletion and NOS2 uncoupling contribute to heart failure‐induced alterations in atrial electrophysiology. Cardiovasc Res 2011; 91: 71–79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Fernstrom JD, Fernstrom MH. Tyrosine, phenylalanine, and catecholamine synthesis and function in the brain. J Nutr 2007; 137: 1539S–1547S discussion 1548S. [DOI] [PubMed] [Google Scholar]
- 32. Castillo L, Yu YM, Marchini JS, Chapman TE, Sanchez M, Young VR, Burke JF. Phenylalanine and tyrosine kinetics in critically ill children with sepsis. Pediatr Res 1994; 35: 580–588. [PubMed] [Google Scholar]
- 33. Cronin SJF, Seehus C, Weidinger A, Talbot S, Reissig S, Seifert M, Pierson Y, McNeill E, Longhi MS, Turnes BL, Kreslavsky T, Kogler M, Hoffmann D, Ticevic M, da Luz Scheffer D, Tortola L, Cikes D, Jais A, Rangachari M, Rao S, Paolino M, Novatchkova M, Aichinger M, Barrett L, Latremoliere A, Wirnsberger G, Lametschwandtner G, Busslinger M, Zicha S, Latini A, Robson SC, Waisman A, Andrews N, Costigan M, Channon KM, Weiss G, Kozlov AV, Tebbe M, Johnsson K, Woolf CJ, Penninger JM. The metabolite BH4 controls T cell proliferation in autoimmunity and cancer. Nature 2018; 563: 564–568. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1. Demographic and laboratory data in patients with different left ventricular ejection fractions.
Table S2. Demographic and laboratory data in patients and normal controls.
Table S3. Demographic and laboratory data of patients with sex and age matched to normal controls.
Table S4. Cytokines in patients with sex and age matched to normal controls.
Table S5. COX univariate and multivariable analysis of cytokines for predicting mortality.