

Abstract
We present a case of successfully resected periosteal chondroma of the left second rib in view of extremely rare occurrence of such cases and the success achieved in its management. A 12-year-old female child presented to our hospital with a swelling in the upper anterolateral aspect of the left chest wall. On chest X-ray and contrast-enhanced computed tomography (CECT), it was diagnosed to be a case of osteochondroma of the second rib. The tumor was approached through a left posterolateral thoracotomy and parts of the first and second ribs were excised along with the tumor. Patient is now on outpatient follow-up and hemodynamically stable with no recurrence of symptoms. The histopathology revealed periosteal chondroma of the second rib with all margins of the resected mass being free of tumor suggesting complete excision. Patient is now on outpatient follow-up and hemodynamically stable with no recurrence of symptoms. Postoperative results were very satisfactory not only in terms of oncological clearance but also from the functional and cosmetic point of view. We believe our case is going to add to the very limited number of such cases available in literature.
Keywords: Periosteal chondroma, Second rib, Posterolateral approach
Introduction
Periosteal chondroma of the rib is an extremely uncommon tumor with limited number of cases documented in published literature. We present a case of successfully resected periosteal chondroma of the left second rib in view of extremely rare occurrence of such cases and the success achieved in its management.
Case report
In December 2016, a 12-year-old female child presented to our hospital with a swelling in the upper anterolateral aspect of the left chest wall. On clinical examination, it showed as a firm swelling of about 7 × 4 cm over the anterolateral aspect of left chest wall at the level of sternal angle starting from left parasternal level and extending up to left anterior axillary line. The mass was having an irregular surface on palpation. The overlying skin was normal and temperature was also normal on palpation. On deep palpation, it was tender. On chest X-ray and CECT, it was diagnosed to be a case of periosteal chondroma with dimensions of 6.7 cm × 8 cm × 6.4 cm arising from the second rib. Chest X-ray showed a heterogeneously calcified lesion involving the left chest wall, causing cortical scalloping of the left first and second ribs, with multiple foci of ring and arc calcification and associated periosteal reaction. It did not seem to communicate with the medullary cavities of adjacent tubular bones as showed by CT imaging. CT also gave a better idea of scalloped cortex and matrix calcification (Fig. 1).
Fig. 1.

CT image showing heterogeneously calcified lesion with scalloped cortex and matrix calcification
Preoperative fine-needle aspiration cytology (FNAC) revealed it as chondroma. In view of the deformity and the pain, patient was taken up for surgery.
The tumor was approached through a left posterior thoracotomy with mild extension onto lateral aspect and parts of the first and second ribs were excised along with the tumor. The central aspect of the first rib and the second rib was resected almost in its entirety leaving about 1 cm on either side of its vertebral and sternal aspects respectively (Fig. 2). The tumor was seen to arise predominantly from the second rib on gross examination of the resected specimen (Fig. 3). Patient is now on outpatient follow-up and hemodynamically stable with no recurrence of symptoms. Follow-up clinical examinations have also thus far not shown any gross deformity on inspection and the result has been cosmetically satisfactory too. The histopathology revealed periosteal chondroma of the second rib with all margins of the resected mass being free of tumor suggesting complete excision. It showed lobulated hyaline cartilage with variable cellularity. There was mild nuclear atypia with hyperchromasia. The follow-up images until date have also not shown any signs of recurrence and no gross deformity of the chest wall.
Fig. 2.
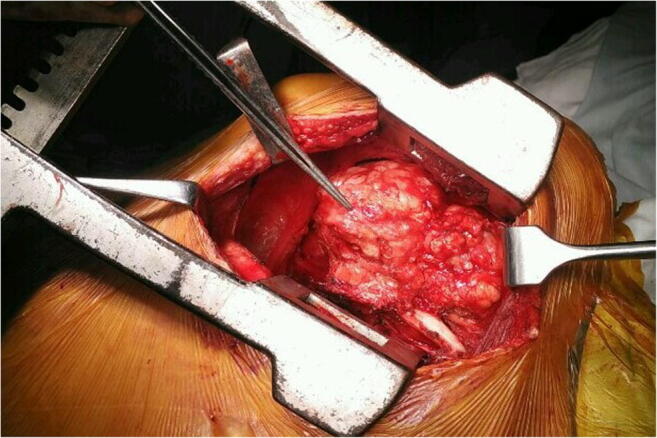
Intraoperative image showing tumor being approached via posterolateral incision
Fig. 3.
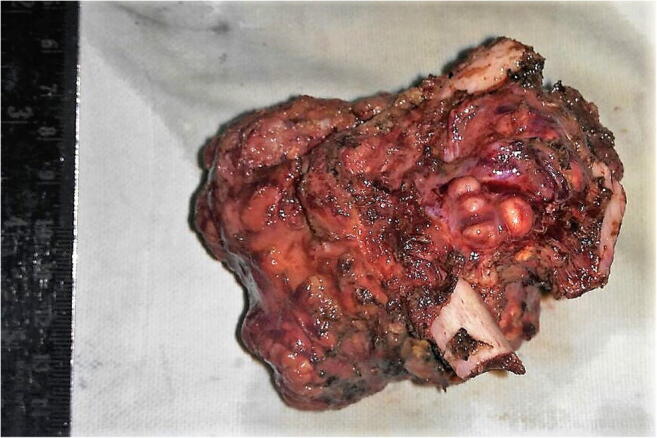
Resected specimen showing tumor arising from the second rib
Discussion
Periosteal (juxtacortical) chondroma is a slow-growing benign cartilaginous tumor, arising within or underneath the periosteum, external to the cortical bone [1]. Although it can occur at any age, this tumor predominantly occurs in children or young adults, with a male predilection [2]. Histologically, periosteal chondroma consists of lobulated hyaline cartilage with variable cellularity. The chondrocytes frequently show mild nuclear atypia with hyperchromasia and binucleation, mimicking chondrosarcoma. Surgical excision is the treatment of choice [3].
Periosteal chondromas appear to be quite rare, with only 46 cases reported in a series of more than 7000 primary bone tumors (0.7%) in a Mayo Clinic study, and representing less than 2% of all primary bone neoplasms in another survey [4]. Besides, periosteal chondroma arising in the rib is an extremely rare event [5]. Our review of the literature revealed only 11 previously documented cases of periosteal chondroma of the rib.
Our patient was a 12-year-old child who had presented with this rare diagnosis. There was visible deformity as well as pain which were causing the child distress as well as emotional setback. In view of the young age of the female child, we not only tried to give her a complete resection of the tumor but also wanted to achieve a good cosmetic outcome. We were prepared for reconstructive measures and had also consulted our plastic surgery team for the same concern. We had four options of approaching the tumor as described in literature for tumors in this region. It could have been either an anterior supraclavicular or infraclavicular approach as described by Dartevelle et al. [6]. The other possibilities were a lateral transaxillary approach, a posterior approach with minimal lateral extension of the incision, and a combination of anterior and posterior approaches as described by Grunenwald et al. [7]. We chose against the anterior and the cervical approaches in view of cosmesis as well as to avoid injuries to the neurovascular structures especially the brachial plexus. We decided against the transaxillary approach as there was chance of extending the incision more anteriorly which could possibly have resulted in poorer cosmetic outcome as well as have affected the development of the breasts for the young girl. Hence, we decided for a posterior approach primarily with minimal lateral extension as successful results have been achieved in most cases by Gandhi et al. by this approach [8]. We had good success in surgical excision of the tumor in spite of difficulty in accessing the tumor site. Post resection, we decided against any form of surgical reconstruction as there was no gross visible deformity and it looked cosmetically acceptable. Besides, in the apical aspect of the chest wall due to good amount of surrounding supportive musculature, the chances of herniation were also minimal. Postoperative results were very satisfactory not only in terms of oncological clearance but also from the functional and cosmetic point of view. Even until date, as the child keeps growing and is on routine follow-up, there has been no affection in either the growth or the cosmetic appearance of the region. The incision line scar too remains posteriorly, which, according to the patient and her parents, can be comfortably hidden beneath her clothing.
Conclusion
We believe our case is going to add to the very limited number of such cases available in literature. Not only from the perspective of rarity of the case but also from the surgical approach deriving satisfactory oncological and cosmetic results, we hope our case will enhance the surgical literature. The take-home message from our side for this case would be in a rare case of periosteal chondroma of the rib with obvious deformity, and surgical resection can be performed through a posterolateral approach which would not only be a cosmetically acceptable approach but also a safe one as well. And finally with this approach, oncologically satisfactory results can be achieved with resection-free margins.
Compliance with ethical standards
Conflict of interest
The authors declare that there are no conflicts of interest.
Informed consent
Informed consent was taken from the parents of the child for the procedures performed as well as prior to publication of the case report.
Ethical approval
All the procedures performed in this case were in accordance to the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declareation and its later amendments or comparable ethical standards.
References
- 1.Zhenjiang L, Wei Y, Lijun Z, Qiwei Li. Periosteal chondroma of the proximal tibia: report of three cases. Int J Clin Exp Med. 2016;9:9908–9916.
- 2.Kirchner SG, Pavlov H, Heller RM, Kaye JJ. Periosteal chondromas of the anterior tibial tubercle: two cases. AJR Am J Roentgenol. 1978;131:1088–1089. [DOI] [PubMed]
- 3.Nojima T, Unni KK, McLeod RA, Pritchard DJ. Periosteal chondroma and periosteal chondrosarcoma. Am J Surg Pathol. 1985;9:666–677. [DOI] [PubMed]
- 4.Miller SF. Imaging features of juxtacortical chondroma in children. Pediatr Radiol. 2014;44:56–63. [DOI] [PubMed]
- 5.Karabakhtsian R, Heller D, Hameed M, Bethel C. Periosteal chondroma of the rib—report of a case and literature review. J Pediatr Surg.2005;40:1505–7. [DOI] [PubMed]
- 6.Dartevelle PG, Chapelier AR, Macchiarini P, et al. Anterior transcervical-thoracic approach for radical resection of lung tumors invading the thoracic inlet. J Thorac Cardiovasc Surg. 1993;105:1025–1034. [PubMed]
- 7.Grunenwald D, Mazel C, Girard P, Berthiot G, Dromer C, Baldeyrou P. Total vertebrectomy for en bloc resection of lung cancer invading the spine. Ann Thorac Surg. 1996;61:723–726. [DOI] [PubMed]
- 8.Gandhi S, Walsh GL, Komaki R, et al. A multidisciplinary surgical approach to superior sulcus tumors with vertebral invasion. Ann Thorac Surg. 1999;68:1778–1784. [DOI] [PubMed]