

Abstract
The COVID-19 pandemic transformed healthcare delivery, including rapid expansion of telehealth. Telerehabilitation, defined as therapy provided by physical therapy, occupational therapy and speech and language pathology, was rapidly adopted with goals to provide access to care and limit contagion. The purpose of this brief report was to describe feasibility of and satisfaction with telerehabilitation. Two-hundred five participants completed online surveys following a telerehabilitation visit. Most commonly, participants were women (53.7%), 35-64 years old, and completed PT (53.7%) for established visits of 30-44 minutes in duration for primary impairments in sports, lower limb injuries, and pediatric neurology. Overall high ratings (“excellent” or “very good” responses) were observed for all patient-centered outcome metrics (ranging 93.7-99%) and value in future telehealth visit (86.8%) across telerehabilitation visits. Women participated more frequently and provided higher ratings than men participants. Other benefits included eliminating travel time, incorporating other healthcare advocates, and convenience delivering care in familiar environment to pediatric patients. Technology and elements of hands-on aspects of care were observed limitations. Recognizing reduced indirect costs of care that telerehabilitation may provide along with high patient satisfaction are reasons policy makers should adopt these services into future healthcare delivery models.
Keywords: Rehabilitation, Physical Therapy, Occupational Therapy, Speech Therapy, Telemedicine, Telehealth, Pandemics
Introduction
This report describes the rapid conversion from in-person visits to synchronous telerehabilitation visits during the novel coronavirus pandemic (SARS-CoV2 is the virus that causes COVID-19 disease). Following outbreaks in China and Europe beginning in late 2019, COVID-19 quickly spread to the United States (US) and other countries. Ensuing efforts to minimize contagion for patients and healthcare workers and conserve healthcare resources resulted in the dramatic reduction of face-to-face outpatient clinical care. Reduced access to in-person rehabilitation care along with changes in healthcare finance and delivery contributed to an exponential increase in telehealth. Measures of quality and patient satisfaction are unknown in this new model of telerehabilitation. To explore feasibility of telerehabilitation, we initiated a quality improvement project, administering an online survey following adult and pediatric synchronous physical (PT), occupational (OT), and speech therapy visits (SLP). Synchronous visits are those that occur in real time (whereas email exchanges, for example, would be asynchronous).
By May 1, 2020, during the peak surge of initial infections in Massachusetts, there were more than 64,000 confirmed cases of COVID-19 and nearly 4,000 deaths.1 For our academic center, outpatient in-person visits were limited to urgent issues only (e.g., progressive neurological deficit, severe pain or immediate post-operative care). Governor Baker declared a state of emergency for Massachusetts on March 10, 2020 and issued a proclamation that expanded telehealth coverage to all network providers to reimburse for telehealth at same rate as in-person visits.2 Physiatric telemedicine was already in place at our institution, but required rapid expansion and was met with high satisfaction.3 In contrast, telerehabilitation was new to the system.
To date, the literature on telerehabilitation is limited and most commonly describes treatment for an impairment within a specific disease, such as teletherapy to address motor impairment following stroke.4 Telerehabilitation has often been offered in addition to in-person care—complementing usual care rather than replacing it altogether.5,6 Reports often describe asynchronous (versus synchronous) care—providing a different patient experience.4,7–12 Reimbursement expansion during the initial stages of the pandemic created a window of opportunity to study the feasibility of and patient satisfaction with telerehabilitation. This in turn, may help inform future clinical care, reimbursement, and healthcare policy during the pandemic and beyond. The purpose of this report is to evaluate patient and patient care advocate reported experiences using telerehabilitation within a single hospital system during the COVID-19 pandemic.
Methods
This study was approved by our academic center’s quality improvement program and exempt from institutional review board approval (IRB). The quality improvement report followed Standards for Quality Improvement Reporting Excellence (SQUIRE 2.0).13 Therapists performing telerehabilitation within a single hospital system for PT, OT, or SLP were eligible to participate. Patients were informed about the initiative during their visit, and those who verbally agreed to participate were sent a brief online survey. Because this was a virtual visit and participants consented verbally and by filling out the survey, no additional written consent was deemed necessary for this IRB exempt quality initiative.
The online survey contained 16 items, with answer choices selected using radio buttons to improve speed and accuracy of completion. The survey used was designed to measure quality and patient satisfaction in a prior report on physiatry care,3 but modified to collect measures of experience with a therapist, including ability to develop and execute a treatment plan.
Patient demographic data and telerehabilitation visit characteristics were collected. Patient-centered outcome measures were rated using a 5-point Likert scale, and an optional free response question allowed patients to identify elements of the visit that were helpful, report on limitations, and provide general feedback.
We used an online survey tool through REDCap (Research Electronic Data Capture) hosted on our institution’s server.14,15 REDCap is a secure, web-based software platform designed to support data capture for research studies, providing 1) an intuitive interface for validated data capture, 2) audit trails for tracking data manipulation and export procedures, 3) automated export procedures for seamless data downloads to common statistical packages, and 4) procedures for data integration and interoperability with external sources.
Data were analyzed using descriptive statistics performed with IBM SPSS® Statistics software platform. Fisher’s exact test with p-value calculated by Monte Carlo simulation was used to analyze the relationships between patient satisfaction and gender, age category, therapist type, visit type, visit duration, typical travel time for in-person therapy visits, inclusion of patient care advocate during visit, and reason for visit. P-value threshold of 0.05 was considered statistically significant.
Results
A total of 211 patients or patient care advocates completed the online survey after participating in a telerehabilitation visit (Table 1). Six responses were excluded (five incomplete responses, one duplicate entry). Of the 205 participants, 110 (53.7%) identified as girls or women; 92 (44.9%) as boys or men, and 3 as transgender men (1.5%). Approximately one-third of participants were 35-64 years old, and one-quarter were 0-7 years old. All patients reported being insured. Average estimated travel time for in-person visits was 30 minutes or longer in over half of patients. Most visits were with PT (53.7%), followed by SLP (30.7%) and OT (14.1%). The majority were follow-up visits for established issues (80%) of 30-44 minutes in duration (59.5%). Sports injuries, lower limb injuries, and pediatric neurology were the most common primary impairments. Patients were accompanied by family members, friends, or other advocates in nearly half of visits, and usually they were in the same location.
Table 1.
Patient demographics and telerehabilitation visit characteristics, n (%)
| Gender | Type of visit | ||
|---|---|---|---|
| Girl or woman | 110 (53.7) | New | 26 (12.7) |
| Boy or man | 92 (44.9) | Follow-up, established issue | 164 (80.0) |
| Transgender (man) | 3 (1.5) | Follow-up, new issue | 15 (7.3) |
| Age (years) | Duration of visit (minutes) | ||
| 0-7 | 52 (25.4) | 0-14 | 1 (0.5) |
| 8-12 | 13 (6.3) | 15-29 | 22 (10.7) |
| 13-17 | 8 (3.9) | 30-44 | 122 (59.5) |
| 18-34 | 25 (12.2) | 45-59 | 54 (26.3) |
| 35-64 | 67 (32.7) | 60+ | 6 (2.9) |
| 65+ | 40 (19.5) | ||
| Insurance status | Reason for visit | ||
| Insured | 205 (100) | Spine condition | 17 (8.3) |
| Uninsured | 0 | Sports injury | 32 (15.6) |
| Typical travel time (minutes) | Non-sports injury | 19 (9.3) | |
| 5-15 | 47 (22.9) | Upper extremity injury | 9 (4.4) |
| 15-29 | 49 (23.9) | Lower extremity injury | 34 (16.6) |
| 30-59 | 64 (31.2) | Concussion | 2 (1.0) |
| 60-89 | 34 (16.6) | Balance impairment | 11 (5.4) |
| 90-120 | 10 (4.9) | Post-stroke | 11 (5.4) |
| Family or friend involvement | Post-traumatic brain injury | 11 (5.4) | |
| Yes, present | 80 (39.0) | Post-spinal cord injury | 0 |
| Yes, remote | 18 (8.8) | Other neurological injury | 11 (5.4) |
| No | 107 (52.2) | Parkinson's Disease | 2 (1.0) |
| Type of therapist | Multiple Sclerosis | 2 (1.0) | |
| Physical | 110 (53.7) | Pediatric orthopedics | 6 (2.9) |
| Occupational | 29 (14.1) | Pediatric neurology | 36 (17.6) |
| Speech and language | 63 (30.7) | Other | 42 (20.5) |
| Other | 3 (1.5) | ||
Patients and patient care advocates reported high quality healthcare delivery (defined as “excellent” or “very good” responses) for all patient-centered outcome metrics (ranging from 93.7-99%), and high value in future telehealth visits (86.8%) (Figure 1). Overall satisfaction was independent of age, therapist type, visit type, visit duration, typical travel time, inclusion of patient care advocate, or any stated reason for visit (all p>0.05). Women rated their level of overall satisfaction significantly higher than men participants (p=0.02).
Figure 1.
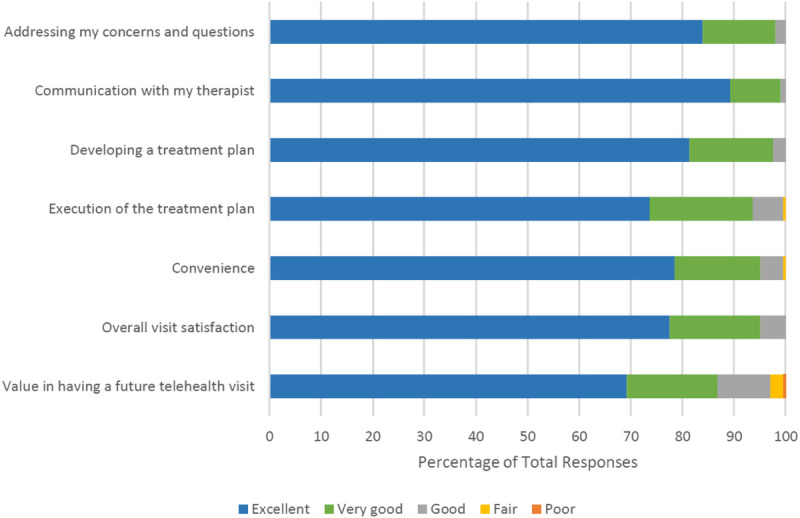
Survey Responses Following Completion of a Telerehabilitation Visit. Figure 1 Legend: Seven measures were obtained on a Likert scale. Responses across the cohort surveyed (n=205) were excellent or very good exceeding 93% across measures during the encounter and 86.8% agreement on value of having a future telerehabilitation visit.
A secondary analysis of patients aged 18 or older (n=132) was conducted as these patients were most likely to have completed the survey independently rather than via patient care advocate proxy in the pediatric population. Among this subset of patients, overall satisfaction was also independent of age, therapist type, visit type, visit duration, typical travel time, and inclusion of patient care advocate. Again, women reported significantly higher levels of satisfaction compared to men participants (p=0.03).
Optional qualitative remarks at the end of the survey revealed many participants expressed appreciation for access to virtual services. Patient care advocates noted that telerehabilitation was useful in establishing a new routine--especially important for providing structure to the population of pediatric patients with behavioral issues. One advocate noted the importance of virtual visits for additional family member training as the pandemic had led to transitions in care responsibilities in the home, and another stated therapy could be tailored to equipment available in the patient’s home, further improving convenience. Many participants wrote that they would prefer to have the option of telerehabilitation visits in the future, but there were certain aspects of care that could not be provided virtually. Limitations include lack of tactile feedback, inability to perform soft tissue work, and absence of the “healing touch.” One advocate expressed challenges with maintaining their child’s engagement and attention using this platform, while others felt that their children were just as attentive as in-person visits. Other technological limitations were noted, including difficulties with camera/device positioning and video quality. No adverse events were reported.
Discussion
The purpose of this quality improvement initiative was to measure patient experience with telerehabilitation. The key findings included high patient satisfaction measures across age, condition, therapist and visit characteristics for both adults and pediatric populations and high reported value for future telerehabilitation visits. Satisfaction with telehealth therapy has been documented for therapy interventions in both neurologic16 and orthopedic populations.17,18 High levels of parent satisfaction with pediatric telehealth therapy have been well described primarily in OT and SLP.19–23 Parents and care advocates also expressed qualitative gains, including increased caregiver training in facilitation strategies tailored to in-home needs and improved parental self-efficacy, consistent with advantages previously reported.19,24 There was no association between age and patient satisfaction with 78% of patients age 18+ and 75% of patients age 65+ operating the telerehabilitation platform without the assistance of a patient care advocate, indicating feasibility of independent technological use in adults of all ages.
Interestingly, in our study population, there was a higher rate of women participating, and they were significantly more likely to report high satisfaction. A prior report25 identified women participants being more motivated to utilize telehealth services due to the perception of shorter wait times.25 It may be the case that women patients and caregivers of pediatric patients face barriers to accessing traditional care, as studies find that they are more likely to manage multiple responsibilities, balancing work, household, childcare, and caretaking roles.26 Another report evaluated utilization of a web-based telehealth model and noted two thirds of patients were women with many visits completed on weekends and holidays when clinics are typically closed.27
Relevance
The pandemic circumstances created an opportunity to study teletherapy, and social distancing requirements created limited access for most patients that expanded beyond typical populations of rural communities previously studied. Prior to the pandemic, third party payor reimbursement was not ubiquitous and therapy visits were typically not covered. For example, in Massachusetts very few private insurers paid eligible practitioners. Nationally, Medicare had a rural telehealth program that was restrictive and challenging to administer. The changes effective March 10, 2020 in Massachusetts required insurers to pay for telehealth at the same rate as a face-to-face visit for duration of state of emergency. In mid-March the Centers for Medicare & Medicaid Services (CMS) expanded telehealth to include therapists, and they were initially able to bill for e-visits (email) or phone consults in a limited manner. At the end of March, CMS added more services to the eligible list which expanded mental health and therapy Current Procedural Terminology (CPT) codes. However, CMS did not allow therapists to have the designation as eligible providers. On April 30, 2020 after intense lobbying efforts, CMS expanded their list of eligible providers to include rehabilitation therapists, and this was retroactive back to March 1, 2020. Legislation was introduced to Congress in 2019, called The Connect Act, which if passed would make the designation for therapists to be eligible providers permanent. The high patient satisfaction across ages, gender, and condition treated suggest these services were valued. Beyond infection control, eliminating travel time, incorporating other healthcare advocates, and convenience delivering care in familiar environments to pediatric patients are all benefits that will be durable outside times of pandemic. Recognizing reduced indirect costs of care that telerehabilitation may provide along with high patient satisfaction are reasons policy makers should adopt these services into future healthcare delivery models.
Limitations
This quality initiative was implemented during a challenging and tumultuous time with pandemic-related COVID-19 infections surging. As such, we were not able to track all of the conversations that therapists had with patients informing them of this initiative. Limitations were noted by participants in lack of hands-on approach. This is consistent with the broader literature showing generally high rates of acceptability of telehealth visits, that may be context dependent and more appropriate for certain types of presentations than others.28 Discipline specific challenges were noted; for example, telerehabilitation requires many modifications to musculoskeletal work.32,33 Thus, for PT and OT, creativity may be required to address myofascial deficits traditionally managed manually. Teaching hands-on facilitation techniques to caregivers can also prove more difficult through teletherapy.35 SLPs further noted barriers to pragmatics practice in the absence of natural, face-to-face social situations and in the assessment of safe oral motor and swallow function during virtual feeding therapy.31 Challenges were also noted in the delivery of virtual pediatric therapy across disciplines for patients with significant behavioral or attention difficulties. A majority of subjective measures can be obtained accurately and incorporate non-verbal communication. However, other aspects of in-person visits build rapport between therapists and patients. Technical challenges were also identified in our study, consistent with prior reports.28–30 Without validated survey tool, we used expert consensus to develop the modified survey.3 More detailed characteristics of patient population and caregivers who completed the survey are difficult to elicit due to goal to provide an anonymous survey tool.
Conclusion
During the novel coronavirus pandemic, we had a unique opportunity to study the feasibility of and patient satisfaction with telerehabilitation. Overall, our findings suggest that this was well accepted across patient populations of varying ages and conditions treated across disciplines. Our study demonstrated a higher proportion of women participating and significantly higher experience ratings compared to men. More research is needed, particularly focusing on functional outcomes, but this study suggests there is value in telerehabilitation. These findings may inform policy and reimbursement for telerehabilitation care.
Acknowledgements
We are grateful to all the therapists and patients who participated in this quality improvement initiative. Specifically, we thank the following for rehabilitation therapists for their contributions to questionnaire development and interpretation of the data: Erin Baumann (PT), Jess Feasby (PT) and Amanda Leonard (SLP).
Footnotes
Disclosures
Author disclosures
Haylee Borgstrom, MD MS – no disclosures
Kester Cotton, PT - no disclosures
Irene S. Davis, PhD PT – no disclosures related to this work
Mary O’Donnell, MS OTR/L – no disclosures
Ginger Polich, MD – no disclosures related to this work
Julie K. Silver, MD – no disclosures related to this work
Hannah Steere, MD – no disclosures
Adam Tenforde, MD – no disclosures related to this work
Funding Information
No funding was received for this work.
Financial Benefits to Author
The authors will not benefit financially from publication of this material.
Previous Presentation
This work has not been presented elsewhere in any form.
References
- 1.Massachusetts Department of Public Health COVID-19 Dashboard; 2020. [Google Scholar]
- 2.Governor Charlie Baker No. 591: Declaration of a State of Emergency to Respond to COVID-19.; 2020.
- 3.Tenforde A Iaccarino M Borgstrom H, et al. :. Telemedicine During COVID-19 for Outpatient Sports and Musculoskeletal Medicine Physicians. Am J Phys Med Rehabil. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Cramer SC Dodakian L Le V, et al. :. Efficacy of Home-Based Telerehabilitation vs In-Clinic Therapy for Adults After Stroke: A Randomized Clinical Trial. JAMA Neurol. June 2019. doi: 10.1001/jamaneurol.2019.1604 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Koppenaal T Arensman RM van Dongen JM, et al. :. Effectiveness and cost-effectiveness of stratified blended physiotherapy in patients with non-specific low back pain: study protocol of a cluster randomized controlled trial. BMC Musculoskelet Disord. 2020. doi: 10.1186/s12891-020-3174-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kloek CJJ, Janssen J, Veenhof C. Development of a Checklist to Assist Physiotherapists in Determination of Patients’ Suitability for a Blended Treatment. Telemed e-Health. 2019. doi: 10.1089/tmj.2019.0143 [DOI] [PubMed] [Google Scholar]
- 7.Tenforde AS, Hefner JE, Kodish-Wachs JE, Iaccarino MA, Paganoni S. Telehealth in Physical Medicine and Rehabilitation: A Narrative Review. PM&R. 2017;9(5S):S51–S58. doi: 10.1016/j.pmrj.2017.02.013 [DOI] [PubMed] [Google Scholar]
- 8.Howard IM, Kaufman MS. Telehealth applications for outpatients with neuromuscular or musculoskeletal disorders. Muscle Nerve. 2018;58:475–485. doi: 10.1002/mus.26115 [DOI] [PubMed] [Google Scholar]
- 9.Ward EC, Wall LR, Burns CL, Cartmill B, Hill AJ. Application of telepractice for head and neck cancer management: a review of speech language pathology service models. Curr Opin Otolaryngol Head Neck Surg. 2017;25:169–174. doi: 10.1097/MOO.0000000000000357 [DOI] [PubMed] [Google Scholar]
- 10.Mani S, Sharma S, Omar B, Paungmali A, Joseph L. Validity and reliability of Internet-based physiotherapy assessment for musculoskeletal disorders: a systematic review. J Telemed Telecare. 2017;23:379–391. [DOI] [PubMed] [Google Scholar]
- 11.Bush ML, Thompson R, Irungu C, Ayugi J. The Role of Telemedicine in Auditory Rehabilitation: A Systematic Review. Otol Neurotol Off Publ Am Otol Soc Am Neurotol Soc [and] Eur Acad Otol Neurotol. 2016;37:1466–1474. doi: 10.1097/MAO.0000000000001236 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Regina Molini-Avejonas D, Rondon-Melo S, de La Higuera Amato CA, Samelli AG. A systematic review of the use of telehealth in speech, language and hearing sciences. J Telemed Telecare. 2015;21:367–376. [DOI] [PubMed] [Google Scholar]
- 13.Ogrinc G, Davies L, Goodman D, Batalden P, Davidoff F, Stevens D. SQUIRE 2.0 (Standards for QUality Improvement Reporting Excellence): revised publication guidelines from a detailed consensus process. BMJ Qual Saf. 2016;25:986–992. doi: 10.1136/bmjqs-2015-004411 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42:377–381. doi: 10.1016/j.jbi.2008.08.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Harris PA Taylor R Minor BL, et al. :. The REDCap consortium: Building an international community of software platform partners. J Biomed Inform. 2019;95:103208. doi: 10.1016/j.jbi.2019.103208 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Knepley KD, Mao JZ, Wieczorek P, Okoye FO, Jain AP, Harel NY. Impact of Telerehabilitation for Stroke-Related Deficits. Telemed e-Health. 2020. doi: 10.1089/tmj.2020.0019 [DOI] [PubMed] [Google Scholar]
- 17.Lovo S, Harrison L, O’connell ME, Trask C, Bath B. Experience of patients and practitioners with a team and technology approach to chronic back disorder management. J Multidiscip Healthc. 2019. doi: 10.2147/JMDH.S208888 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Azma K, RezaSoltani Z, Rezaeimoghaddam F, Dadarkhah A, Mohsenolhosseini S. Efficacy of tele-rehabilitation compared with office-based physical therapy in patients with knee osteoarthritis: A randomized clinical trial. J Telemed Telecare. 2018. doi: 10.1177/1357633X17723368 [DOI] [PubMed] [Google Scholar]
- 19.Wallisch A, Little L, Pope E, Dunn W. Parent Perspectives of an Occupational Therapy Telehealth Intervention. Int J telerehabilitation. 2019;11:15–22. doi: 10.5195/ijt.2019.6274 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Cason J. A pilot telerehabilitation program: delivering early intervention services to rural families. Int J telerehabilitation. 2009;1:29–38. doi: 10.5195/ijt.2009.6007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Cason J. Telehealth: a rapidly developing service delivery model for occupational therapy. Int J telerehabilitation. 2014;6:29–35. doi: 10.5195/ijt.2014.6148 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Clawson B, Selden M, Lacks M, Deaton A V, Hall B, Bach R. Complex pediatric feeding disorders: using teleconferencing technology to improve access to a treatment program. Pediatr Nurs. 2008;34:213–216. [PubMed] [Google Scholar]
- 23.Crutchley S, Campbell M. TeleSpeech Therapy Pilot Project: Stakeholder Satisfaction. Int J telerehabilitation. 2010;2:23–30. doi: 10.5195/ijt.2010.6049 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Little LM, Pope E, Wallisch A, Dunn W. Occupation-Based Coaching by Means of Telehealth for Families of Young Children With Autism Spectrum Disorder. Am J Occup Ther Off Publ Am Occup Ther Assoc. 2018;72:7202205020p1-7202205020p7. doi: 10.5014/ajot.2018.024786 [DOI] [PubMed] [Google Scholar]
- 25.Polinski JM, Barker T, Gagliano N, Sussman A, Brennan TA, Shrank WH. Patients’ Satisfaction with and Preference for Telehealth Visits. J Gen Intern Med. 2016;31:269. doi: 10.1007/S11606-015-3489-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Craig L, Mullan K. Parenthood, Gender and Work-Family Time in the United States, Australia, Italy, France, and Denmark. J Marriage Fam. 2010;72:1344–1361. doi: 10.1111/j.1741-3737.2010.00769.x [DOI] [Google Scholar]
- 27.Uscher-Pines L, Mehrotra A. Analysis Of Teladoc Use Seems To Indicate Expanded Access To Care For Patients Without Prior Connection To A Provider. https://doi.org/101377/hlthaff20130989. August 2017. doi: 10.1377/HLTHAFF.2013.0989 [DOI] [PubMed]
- 28.Thiyagarajan A, Grant C, Griffiths F, Atherton H. Exploring patients’ and clinicians’ experiences of video consultations in primary care: a systematic scoping review. BJGP Open. 2020. doi: 10.3399/bjgpopen20x101020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Hammersley V Donaghy E Parker R, et al. :. Comparing the content and quality of video, telephone, and face-to-face consultations: A non-randomised, quasi-experimental, exploratory study in UK primary care. Br J Gen Pract. 2019. doi: 10.3399/bjgp19X704573 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Donaghy E Atherton H Hammersley V, et al. :. Acceptability, benefits, and challenges of video consulting: A qualitative study in primary care. Br J Gen Pract. 2019. doi: 10.3399/bjgp19X704141 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Tucker JK. Perspectives of speech-language pathologists on the use of telepractice in schools: quantitative survey results. Int J telerehabilitation. 2012;4:61–72. doi: 10.5195/ijt.2012.6100 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Verduzco-Gutierrez M, Bean AC, Tenforde AS, Tapia RN, Silver JK. How to Conduct an Outpatient Telemedicine Rehabilitation or Prehabilitation Visit. PM&R. 2020;n/a(n/a). doi: 10.1002/pmrj.12380 [DOI] [PubMed] [Google Scholar]
- 33.Tanaka MJ, Oh LS, Martin SD, Berkson EM. Telemedicine in the Era of COVID-19: The Virtual Orthopaedic Examination. JBJS. 9000;Latest Articles. https://journals.lww.com/jbjsjournal/Fulltext/9000/Telemedicine_in_the_Era_of_COVID_19__The_Virtual.99743.aspx. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Nelson M, Bourke M, Crossley K, Russell T. Telerehabilitation is non-inferior to usual care following total hip replacement — a randomized controlled non-inferiority trial. Physiotherapy. 2020;107:19–27. doi: 10.1016/j.physio.2019.06.006 [DOI] [PubMed] [Google Scholar]
- 35.Zylstra SE. Evidence for the Use of Telehealth in Pediatric Occupational Therapy. J Occup Ther Sch Early Interv. 2013;6:326–355. doi: 10.1080/19411243.2013.860765 [DOI] [Google Scholar]