

Abstract
Objective.
To examine the association between hospital surgical volume and perioperative outcomes for fertility-sparing trachelectomy performed for cervical cancer.
Methods.
This is a population-based retrospective observational study utilizing the Nationwide Inpatient Sample from 2001 to 2011. Women aged ≤45 years with cervical cancer who underwent trachelectomy were included. Annualized hospital surgical volume was defined as the average number of trachelectomies a hospital performed per year in which at least one case was performed. Perioperative outcomes were assessed based on hospital surgical volume in a weighted model, specifically comparing the top-decile centers to the lower volume centers.
Results.
There were a total of 815 trachelectomies performed at 89 centers, and 76.4% of the trachelectomy-performing centers had a minimum surgical volume of one trachelectomy per year. The top-decile group had a higher rate of lymphadenectomy performance compared to the lower volume group (96.4% versus 82.4%, odds ratio [OR] 5.65, 95% confidence interval [CI] 2.81–11.4, P < 0.001). There was a significant inverse linear association between annualized surgical volume and the number of perioperative complications (P = 0.020). The top-decile group also had a lower rate of perioperative complications (9.7% versus 21.0%, P < 0.001) and prolonged hospital stay ≥7 days (2.0% versus 6.5%, P = 0.006) compared to the lower volume group. In a multivariable analysis, the top-decile group had a 65% relative decrease in perioperative complication risk compared to the lower volume group (adjusted-OR 0.35, 95%CI 0.20–0.59, P < 0.001).
Conclusion.
Fertility-sparing trachelectomy for young women with cervical cancer is a rare surgical procedure; <90 centers performed this procedure from 2001 to 2011 and most hospitals perform a small number of cases annually. Higher hospital surgical volume for trachelectomy may be associated with reduced perioperative morbidity.
Keywords: Cervical cancer, Trachelectomy, Surgical volume, Morbidity, Mortality, Outcome
1. Introduction
Cervical cancer has become less frequent in the United States with the incidence rate decreasing by 57% between 1975 and 2016 [1]. Cervical cancer is now ranked as 20th most common malignancy in the United States in 2019 [1,2]. However, cervical cancer is a disease of young women, and is the second most common cause of cancer death in reproductive-aged women after breast cancer [2].
Approximately 45% of women with cervical cancer present with the tumor localized to the cervix in the United States [2]. The standard surgical treatment for such early-stage cervical cancer is hysterectomy with either the simple or radical approach based on the extent of the disease [3]. As a consequence of total hysterectomy, reproductive-aged woman with this disease will lose future fertility. As an alternative, trachelectomy has been proposed as a potential treatment to spare reproductive organs in women who desire future fertility [4-6]. A number of studies have demonstrated the oncologic safety of this surgical procedure in women with small cervical tumors [7,8].
Fertility-sparing trachelectomy is a relatively uncommon surgical procedure. Despite a relative increasing utilization of this surgical approach in the past several years, trachelectomy was utilized in <5% of reproductive-aged women who underwent definitive surgical treatment for early-stage cervical cancer [7-9]. For a number of oncologic surgeries, an association between hospital and surgeon procedural volume and perioperative and oncologic outcomes has been examined (Supplemental Table S1) [10-31]. Yet, this association has not been previously examined for fertility-sparing trachelectomy.
Given the rarity of fertility-sparing trachelectomy, we hypothesized that a larger surgical volume may be associated with improved outcomes. The objective of the study was to examine the association between hospital surgical volume and perioperative outcomes of fertility-sparing trachelectomy performed for early-stage cervical cancer.
2. Materials and methods
2.1. Data source
The Nationwide Inpatient Sample (NIS) is a publically available and deidentified population-based database that is distributed as part of the Healthcare Cost and Utilization Project by the Agency for Healthcare Research and Quality [32]. The NIS database includes hospital discharge data for >36 million hospitalizations per year when weighted, and it provides patient characteristics and resource-use information, such as diagnosis and intervention types, length of stay and hospital charges, as well as hospital-specific data, including location, bed size, and teaching status. Over 90% of the United States population was represented in this database when weighted. The University of Southern California Institutional Review Board deemed the study exempt due to the use of publicly available deidentified data.
2.2. Study eligibility
This is a population-based retrospective observational study utilizing the NIS from 2001 to 2011. Women aged ≤45 years with early-stage cervical cancer who underwent inpatient trachelectomy were included. Age cutoff of <45 years was chosen per our prior study [8]. Absence of metastatic disease and prior chemotherapy/radiotherapy was used as the surrogate indicators for early-stage cervical cancer in this study. The International Classification of Disease 9th revision codes (ICD-9) of 674 was used for the surrogate of trachelectomy. During the study period, the ICD-9 codes for all variables including trachelectomy remained the same.
The study period of year 2001–2011 was chosen because the NIS program randomly captured approximately 20% of the U.S. hospitals and all the consecutive inpatient admissions within the chosen hospitals during the study period. Cases after 2011 were not utilized as the NIS program changed the data capture mechanism for hospital selection thereafter. Exclusion criteria included those who were aged >45 years, did not have trachelectomy, received prior radiotherapy or chemotherapy, and had metastatic disease.
2.3. Clinical information
Among cases eligible for analysis, the following information was abstracted from the NIS database: patient demographics, disease factors, hospital information, surgery types, and surgical outcome. Patient demographics included age (<30, 30–39, and 40–45), calendar year of trachelectomy (2001–2004, 2005–2008, and 2009–2011), race/ethnicity (white, black, Hispanic, and others), medical comorbidities, obesity (yes versus no), primary expected payer (Medicare, Medicaid, private insurance, self-pay, and others), and median household income (<$39,000, $39,000–$47,999, $48,000–$62,999, and ≥$63,000). Obesity was defined as a body mass index of ≥30 kg/m2 according to the ICD-9 coding and based on the CDC classification. Hospital bed size was defined by hospital geographic region, urban-rural designation, and teaching status [32].
For medical comorbidities, the Charlson Comorbidity Index was determined for each patient based on the codes for the specified medical conditions in each category and weighted appropriately to calculate a final score as described previously [33-35]. Surgical information included performance of lymphadenectomy (yes versus no) and use of robotic assisted surgery (yes versus no). Hospital data included hospital bed size (small, medium, and large), teaching status (rural, urban nonteaching, and urban teaching), and hospital region (Northeast, Midwest, South, and West). For surgical outcomes, length of hospital stay, total charge, and perioperative complications were recorded. Total charge covers both surgical and post-surgical costs during the index admission, and was corrected for the medical inflation by the 2015 value as described previously [34].
Perioperative complications were defined as the presence of any of the following as described previously: hemorrhage, shock, wound complications, thromboembolism, cerebrovascular disease or stroke, cardiac failure, myocardial infarction, pneumonia, respiratory failure, systemic inflammatory response syndrome or sepsis, ileus or small bowel obstruction, vascular injury, acute kidney injury, pyelonephritis, abscess, fistula, intestinal perforation, position-dependent complications, and death during the index admission (Supplemental Table S2) [19,34,35]. In the NIS program, perioperative complications included both intraoperative and postoperative complications before hospital discharge.
2.4. Study definition
First, the annualized hospital surgical volume was computed for each trachelectomy-performing center during the study period (Table 1). This was defined as the average number of procedures a hospital performed per year in which at least one case was performed [31]. Then, a scatter plot diagram was constructed to examine the association between the annualized hospital surgical volume and the extent of perioperative complications, and the statistical significance was assessed with a linear regression model. This analytic approach is based on the assumption that a higher surgical volume is associated with improved outcomes [10-19]. Annualized hospital surgical volume was examined as a continuous variable due to the limited number of trachelectomy-performing centers during the study period.
Table 1.
Annualized hospital surgical volume for trachelectomy between 2001 and 2011.
| Annualized SV | Centers | Percent | Grouping definition |
|---|---|---|---|
| 1 | 68 | 76.4% | |
| 1.1–1.5 | 5 | 5.6% | |
| 1.6–2.0 | 10 | 11.2% | Non-top decile centers |
| >2.5 | 6 | 6.7% | Top decile centers |
| Total | 89 | 100% |
The median of annualized SV was 1 trachelectomy per year. Annualized SV of >2 trachelectomies per year represented top decile of annualized SV. Abbreviation: SV, hospital surgical volume for trachelectomy.
The results showed that there is a significant inverse association between the annualized hospital trachelectomy volume and the number of perioperative complications with larger trachelectomy volume being associated with fewer perioperative complications (equation of a line: y = −0.028× + 0.275, P = 0.020; Fig. 1). Based on this linear assumption and the relatively small number of centers performing trachelectomies during the study period (Table 1), the centers were divided into two groups. The cutoff of annualized hospital surgical volume was chosen as >90%ile (top-decile centers) versus ≤90%ile (lower volume centers). This concept of top-decile centers was adopted by a recent study demonstrating improved outcomes in the top-decile surgical volume centers for radical surgery for cervical cancer [16].
Fig. 1.

Correlation between annualized hospital surgical volume and extents of perioperative complication. There is a significant inverse linear association between the annualized surgical volume for trachelectomy and the extent of perioperative complication (equation of a line estimated by a linear regression model: y = −0.028x + 0.275, P = 0.020).
2.5. Statistical consideration
The first-level analysis examined the differences in baseline characteristics based on hospital surgical volume (top-decile centers versus lower volume centers). For continuous variables, outcomes were displayed as means with standard deviation or medians with interquartile range (IQR). The Student t-test or Mann-Whitney U test was used to assess differences among the groups as appropriate. For categorical and ordinal variable, a frequency table for covariates was displayed with the percentage proportion per surgical volume group, and the Fisher exact test or chi-square test was used for univariable analysis as appropriate.
The second-level analysis examined the independent factors associated with perioperative complications. A binary logistic regression model was fitted for the analysis (any perioperative complication, yes versus no). First, all the significant covariates with a P < 0.05 were entered in the initial model. Then, the least significant covariate was removed from the model until all the covariates retained a statistical significance with a P < 0.05 (conditional backward method). The magnitude of statistical significance was expressed with adjusted odds ratio (OR) and 95% confidence interval (CI).
Various sensitivity analyses were undertaken to assess the robustness of the study results. First, the study cohort was restricted to those who underwent lymphadenectomy at trachelectomy. This is based on the rationale that this subgroup likely represents stage IA2-IB cervical cancer for which radical trachelectomy is the standard surgical modality for fertility preservation. Second, cases that underwent robotic-assisted trachelectomy were examined. This approach, generally limited to surgeons with additional training, was infrequently utilized during the study period, so we speculated that surgical volume would also impact outcomes.
Third, outcomes of the top-decile centers were compared to the minimum-volume centers (1 trachelectomy a year). Last, the correlation between annualized hospital trachelectomy and radical hysterectomy volumes was examined, and the number of any mode radical hysterectomy at a minimum trachelectomy annualized surgical volume of 1 case a year was interpreted as the threshold to perform trachelectomy in the institution. This correlation was also examined for pelvic exenteration as an external validation because this procedure represents another rare and complex gynecologic surgery. Dataset from our recent study was utilized for analysis [19].
The surgical volume definition was determined in an unweighted model, and the remaining analyses were performed using a weighted model. A variance inflation factor was used to assess multicollinearity between the covariates, and a value of ≥2.5 was interpreted as multicollinearity in this study. All statistical analyses were based on two-sided hypothesis and a P < 0.05 was considered statistically significant. Statistical Package for Social Sciences (version 25.0, Armonk, NY, USA) was used for all the analyses. The STROBE guidelines were consulted to outline this observational cohort study.
3. Results
A total of 815 women aged ≤45 years who had trachelectomies for early-stage cervical cancer between 2001 and 2011 were identified (Fig. 2). During the study period, there were 89 centers that performed at least one trachelectomy per year. The number of trachelectomy-performing centers increased from 7 in 2001 to 18 in 2011 (2.6-fold increase; Supplemental Fig. S1), but the majority of study sites had an annual trachelectomy volume of 1 case per year (68 [76.4%] out of 89 centers). Six (6.7%) of the 89 centers performed on average >2 trachelectomies per year, and this group composed the top-decile centers (Table 1). Collectively, the top-decile centers performed 247 (30.3%) trachelectomies and the remaining lower volume centers performed 568 (69.7%) trachelectomies.
Fig. 2.
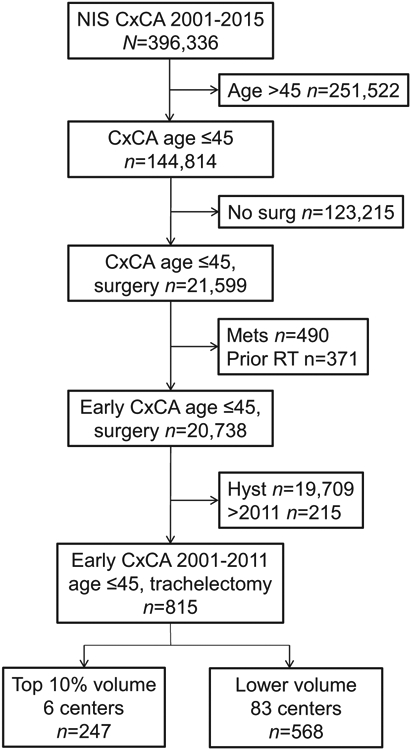
CONSORT diagram for study selection schema. Abbreviations: CxCA, cervical cancer; no surg, no surgery (hysterectomy or trachelectomy); mets, metastatic disease; RT, radiotherapy; and Hyst, hysterectomy.
For the entire cohort, the mean age at surgery was 31.8 (±5.6) years, and the majority of patients were white (n = 476, 58.4%), had no comorbidities (Charlson Index score of 0, n = 713, 87.6%), and underwent lymphadenectomy at the time of trachelectomy (n = 706, 86.6%). Obesity was rare in this population (n = 15, 1.8%), and robotic-assisted surgery was infrequently utilized during the study period (n = 95, 11.7%).
Women in the top-decile group were more likely to be young, white, and non-obese, have a comorbidity, and have private primary payer insurance compared to the lower volume group (all, P < 0.05) (Table 2). Top-decile centers were more likely to be urban teaching centers but less likely to be hospitals with a large number of beds compared to the lower volume group (both, P < 0.05). The top-decile centers had a higher rate of lymphadenectomy compared to lower volume groups (96.4% versus 82.4%, OR 5.65, 95%CI 2.81–11.4, P < 0.001; Fig. 3A).
Table 2.
Patient demographics per hospital surgical volume (whole cohort, N = 815).
| Characteristic | Non-top decile | Top decile | P-value |
|---|---|---|---|
| Number | n = 568 | n = 247 | |
| Age (years) | 32.1 (±5.9) | 31.2 (±4.9) | 0.032 |
| <30 | 207 (36.4%) | 90 (36.6%) | |
| 30–39 | 295 (51.9%) | 141 (57.3%) | |
| 40–45 | 66 (11.6%) | 15 (6.1%) | |
| Year | <0.001 | ||
| 2001–2004 | 107 (18.9%) | 41 (16.6%) | |
| 2005–2008 | 220 (38.8%) | 144 (58.3%) | |
| 2009–2011 | 240 (42.3%) | 62 (25.1%) | |
| Race/ethnicity | <0.001 | ||
| White | 302 (53.2%) | 174 (70.4%) | |
| Black | 31 (5.5%) | 14 (5.7%) | |
| Hispanic | 84 (14.8%) | 25 (10.1%) | |
| Othera | 151 (26.6%) | 34 (13.8%) | |
| Obesity | 0.008 | ||
| No | 553 (97.4%) | 247 (100%) | |
| Yes | 15 (2.6%) | 0 | |
| Charlson Index | 0.025 | ||
| 0 | 505 (88.9%) | 208 (84.2%) | |
| 1 | 47 (8.3%) | 35 (14.2%) | |
| 2 | 16 (2.8%) | b | |
| Median household income | 0.155 | ||
| <$39,000 | 92 (18.3%) | 42 (20.9%) | |
| $39,000–$47,999 | 107 (21.2%) | 28 (13.9%) | |
| $48,000–$62,999 | 154 (30.6%) | 63 (31.3%) | |
| ≥$63,000 | 151 (30.0%) | 68 (33.8%) | |
| Primary expected payer | <0.001 | ||
| Medicare | 27 (4.8%) | 0 | |
| Medicaid | 106 (18.7%) | 28 (11.4%) | |
| Private including HMO | 373 (65.8%) | 200 (81.3%) | |
| Self-pay | 24 (4.2%) | 18 (7.3%) | |
| Other | 37 (6.5%) | 0 | |
| Hospital bed sizec | <0.001 | ||
| Small | 38 (6.7%) | 59 (23.9%) | |
| Medium | 83 (14.6%) | 65 (26.3%) | |
| Large | 446 (78.7%) | 123 (49.8%) | |
| Hospital teaching status | <0.001 | ||
| Rural | b | 0 | |
| Urban Non-teaching | 84 (14.8%) | 0 | |
| Urban teaching | 475 (83.6%) | 247 (100%) | |
| Hospital region | <0.001 | ||
| Northeast | 128 (22.5%) | 58 (23.5%) | |
| Midwest | 102 (18.0%) | 37 (15.0%) | |
| South | 174 (30.6%) | 117 (47.4%) | |
| West | 164 (28.9%) | 35 (14.2%) | |
| Lymphadenectomy | <0.001 | ||
| No | 100 (17.6%) | b | |
| Yes | 468 (82.4%) | 238 (96.4%) | |
| Robotic assisted | 0.342 | ||
| No | 506 (89.1%) | 214 (86.6%) | |
| Yes | 62 (10.9%) | 33 (13.4%) | |
| Length of stay (days) | 3 (IQR 2–4) | 3 (IQR 2–4) | 0.001 |
| Corrected total charge ($) | 42,186 (IQR 26.739–64,176) | 40,431 (IQR 31,913-58,003) | 0.960 |
Mean (±SD), median (IQR), or number (percentage per column) is shown. Total number may not be 815 due to weighted value. Chi-square test, Fisher exact test, Student t-test, or Mann-Whitney U test for P-value.
Including unknown.
Number suppressed due to the HCUP requirement (1–10).
Based upon hospital region, urban-rural designation, and teaching status that was determined per the HCUP.
Fig. 3.

Performance and outcome of trachelectomy per hospital surgical volume. Fisher exact test for P-value. (A) Performance of lymphadenectomy at trachelectomy, (B) prolonged hospitalization, and (C) perioperative complication (any) are shown based on hospital surgical volume. Observed values with 95% confidence intervals are displayed.
For the whole cohort, the median length of stay for the index admission was 3 (IQR 2–4) days, and there were 42 (5.2%) women who had a prolonged hospital stay of ≥7 days. The top-decile centers had a lower risk of prolonged hospital stay following trachelectomy compared to the lower volume centers (2.0% versus 6.5%, OR 0.30, 95%CI 0.12–0.76, P = 0.006; Fig. 3B). The median corrected total charge of the index admission was $40,739 (IQR $29,225–$59,374) that was not associated with surgical volume (P = 0.960).
Overall there were 142 (17.5%) women who had a perioperative complication during the index admission. Among those, the majority had a single complication (n = 119, 83.8%). There were no perioperative deaths in this study population. On univariable analysis, the top-decile centers had a lower risk of perioperative complications following trachelectomy compared to the lower volume centers (9.7% versus 21.0%, 11.3% absolute decrease, P < 0.001; Fig. 3C). On multivariable analysis (Table 3), the top-decile centers had an approximately 65% decreased perioperative complication risk compared to the lower volume centers (adjusted-OR 0.35, 95%CI 0.20–0.59, P < 0.001).
Table 3.
Multivariable analysis for perioperative complication (whole cohort, N = 815).
| Characteristic | Adjusted-OR (95%CI) | P-value |
|---|---|---|
| Age (years) | <0.001* | |
| <30 | 2.43 (1.56–3.78) | <0.001 |
| 30–39 | 1 | |
| 40–45 | 1.37 (0.64–2.97) | 0.420 |
| Year | 0.008* | |
| 2001–2004 | 0.23 (0.08–0.65) | 0.005 |
| 2005–2008 | 1.16 (0.70–1.90) | 0.569 |
| 2009–2011 | 1 | |
| Race/ethnicity | <0.001* | |
| White | 1 | |
| Black | 0.34 (0.10–1.17) | 0.087 |
| Hispanic | 3.94 (2.29–6.79) | <0.001 |
| Other* | 1.65 (0.96–2.83) | 0.071 |
| Charlson Index | <0.001* | |
| 0 | 1 | |
| 1 | 2.06 (1.09–3.87) | 0.026 |
| 2 | 16.9 (5.73–49.5) | <0.001 |
| Median household income | 0.001* | |
| <$39,000 | 1 | |
| $39,000–$47,999 | 2.55 (1.14–5.69) | 0.023 |
| $48,000–$62,999 | 4.00 (1.95–8.19) | <0.001 |
| ≥$63,000 | 2.49 (1.17–5.30) | 0.018 |
| Missing | 6.92 (2.26–21.2) | 0.001 |
| Robotic assisted | ||
| No | 1 | |
| Yes | 2.17 (1.15–4.09) | 0.017 |
| Hospital surgical volume | ||
| Non-top decile | 1 | |
| Top decile | 0.35 (0.20–0.59) | <0.001 |
A binary logistic regression model for multivariable analysis. All the significant covariates with P < 0.05 on univariable were initially entered in the model. Conditional backward method was used to retain only the significant covariates with P < 0.05 in the final model as listed above.
P-value for interaction.
Young age, Hispanic race, a higher comorbidity index, higher median household income, and robotic-assisted surgery were also associated with an increased perioperative complication rate (all, P < 0.05). When the type of perioperative complication was examined based on surgical volume, trachelectomy at the top decile centers was associated with a decreased risk of hemorrhage (0% versus 6.2%), gastrointestinal complications either small bowel obstruction or ileus (0% versus 3.1%), and cardio-pulmonary complications (0% versus 4.2%) compared to trachelectomy at the lower volume centers (all, P < 0.05).
When the study cohort was restricted to those who had lymphadenectomy (n = 706), trachelectomy at the top-decile center was independently associated with decreased perioperative complications compared to the lower volume group (10.1% versus 21.6%, adjusted-OR 0.31, 95%CI 0.16–0.60, P = 0.001; Table 4). Similarly, when robotic-assisted trachelectomies were examined (n = 95), the top-decile centers had lower perioperative complications compared to the lower volume centers (14.7% versus 35.5%, OR 0.31, 95%CI 0.11–0.93, P = 0.035). Finally, when compared to the centers performing a minimum surgical volume of one trachelectomy a year, trachelectomy at the top-decile centers was significantly associated with decreased perioperative complications (9.7% versus 16.9%, adjusted-OR 0.50, 95%CI 0.27–0.90, P = 0.021).
Table 4.
Multivariable analysis for perioperative complication (lymphadenectomy cohort, N = 706).
| Characteristic | Adjusted-OR (95%CI) | P-value |
|---|---|---|
| Year | <0.001* | |
| 2001–2004 | 1 | |
| 2005–2008 | 0.04 (0.01–0.20) | <0.001 |
| 2009–2011 | 0.77 (0.44–1.34) | 0.355 |
| Race/ethnicity | <0.001* | |
| White | 1 | |
| Black | 0.80 (0.22–2.92) | 0.739 |
| Hispanic | 7.81 (4.00–15.3) | <0.001 |
| Other* | 1.38 (0.76–2.51) | 0.298 |
| Charlson Index | <0.001* | |
| 0 | 1 | |
| 1 | 2.27 (1.08–4.77) | 0.031 |
| 2 | 85.6 (12.5–589) | <0.001 |
| Median household income | <0.001* | |
| <$39,000 | 1 | |
| $39,000–$47,999 | 2.78 (1.04–7.46) | 0.042 |
| $48,000–$62,999 | 5.87 (2.47–14.0) | <0.001 |
| ≥$63,000 | 3.88 (1.57–9.59) | 0.003 |
| Missing | 23.7 (4.99–113) | <0.001 |
| Primary expected payer | 0.007* | |
| Medicare | 1 | |
| Medicaid | 0.71 (0.16–3.22) | 0.660 |
| Private including HMO | 0.44 (0.11–1.74) | 0.243 |
| Self-pay | na | 0.998 |
| Other | 0.07 (0.01–0.41) | 0.003 |
| Hospital bed size | 0.002* | |
| Small | 1 | |
| Medium | 5.18 (1.46–18.4) | 0.011 |
| Large | 7.93 (1.40–26.2) | 0.001 |
| Hospital region | 0.005* | |
| Northeast | 1 | |
| Midwest | 2.35 (0.94–5.89) | 0.069 |
| South | 3.16 (1.54–6.46) | 0.002 |
| West | 3.40 (1.66–6.93) | 0.001 |
| Hospital surgical volume | ||
| Non-top decile | 1 | |
| Top decile | 0.31 (0.16–0.60) | 0.001 |
A binary logistic regression model for multivariable analysis. All the significant covariates with P < 0.05 on univariable were initially entered in the model. Conditional backward method was used to retain only the significant covariates with P < 0.05 in the final model as listed above.
P-value for interaction.
There was a significant correlation between any radical hysterectomy and trachelectomy surgical volume with larger radical hysterectomy volume being associated with large trachelectomy volume (P < 0.001, Fig. 4A). The threshold of any radical hysterectomies to have a minimum trachelectomy volume of 1 case a year was 7.8 cases per year. This threshold for trachelectomy was higher compared to that corresponding with performance of one pelvic exenteration (6.0 radical hysterectomies a year; Fig. 4B).
Fig. 4.

Association between radical hysterectomy surgical volume and trachelectomy or exenteration surgical volume. Association of annualized hospital surgical volume between any RH and trachelectomy (panel A) and pelvic exenteration for gynecologic malignancies (panel B) is shown. Total 11 models were assessed for the curve estimation, and the most-fit curve model is shown for each analysis. The threshold of hospital any RH cases to have one trachelectomy case was 7.8 and 6.0 to start one exenteration, respectively. Abbreviation: RH, radical hysterectomy.
4. Discussion
This study found that fertility-sparing trachelectomy for young women with cervical cancer was a rare surgical procedure in the United States between 2001 and 2011. Nationwide, fewer than 90 institutions offered this procedure, and despite the increase in the number of trachelectomy-offering centers most performed few cases annually. A higher hospital surgical volume for fertility-sparing trachelectomy was associated with reduced short-term perioperative morbidity.
The volume-outcome relationships have been extensively studied for many oncologic surgeries, and it appears that the cancer types in which volume-outcome relationships have been demonstrated are relatively uncommon cancer types and have complex surgical procedures as compared to the types in which the volume-outcome relationship is inconsistent across the studies [10-31]. Specific surgeries demonstrating volume-outcome relationship include cranial surgery, pulmonary lobectomy, hepatectomy, pancreatico-duodenectomy, radical hysterectomy, pelvic exenteration, and cytoreductive surgery (Supplemental Table S1). Like the trachelectomy, these are highly complex procedures which are performed less commonly than other similarly complex surgeries which are performed more frequently.
The observed volume-outcome relationship for fertility-sparing trachelectomy suggests a possible target for quality improvement initiatives. A higher hospital surgical volume was associated with a better short-term perioperative outcome. Therefore, a future research direction that merits investigation is an examination of the long-term oncologic outcomes, including disease recurrence and mortality with fertility-sparing trachelectomy. Neither of these outcomes is available in the NIS database, and it remains unknown if a larger hospital surgical volume for fertility-sparing trachelectomy is associated with improved prognosis. Other outcomes of interest include rates of fertility, live birth, and preterm birth.
Given the rarity of fertility-sparing trachelectomy, national and international collaboration is a key to success when conducting these research studies. Annualized surgical volume of more than two trachelectomies per year qualified the top decile centers, clearly implying that surgical volume for trachelectomy is low across the nation in the United States. The sample size of our study is small, making clinically relevant interpretation difficult. Currently, there is a call for an international multicenter retrospective observational study to examine the outcomes of women who have undergone fertility-sparing trachelectomy (IRTA study), and this study may be an opportunity to examine volume-outcome relationship for oncologic and obstetric outcomes [36].
The current national practice patterns clearly point out that the majority of U.S. hospitals and surgeons have relatively limited surgical experience with trachelectomy. Given the decreasing number of radical hysterectomies performed in the United States presumably secondary to the decreasing incidence of cervical cancer [37], it may be that the absolute number of trachelectomies which are performed will also decrease in the future. In the United States, the population incidence rate of localized cervical cancer in women aged <45 years has decreased in recent years (Supplemental Fig. S2). Thus, while the number of trachelectomy-performing center may increase, the hospital surgical volume may decrease in the future. Therefore, if good long-term oncologic outcomes are able to be demonstrated, the improvement in short-term perioperative complications suggests the need for centralizing care of women with early-stage cervical cancer who wish to have a fertility-sparing trachelectomy.
There is an emerging concept for minimum-volume standards in gynecologic surgeries, and the implications of this concept in trachelectomy would be also of interest [38,39]. Our analysis showed that the number of trachelectomy-offering centers is limited (<90 centers over a decade) and there were only 6 centers that met the criteria for top-decile centers in the United States between 2001 and 2011. Moreover, the threshold of radical hysterectomy number to perform one trachelectomy was higher than the threshold to perform one pelvic exenteration (7.8 versus 6). These findings imply that this procedure may have already been regionalized to the centers with high radical hysterectomy volumes in the United States. While centralizing care to higher volume centers can be an intriguing concept, such approach can be indeed challenging for patients (inconvenient access, travel, and cost), especially if the number of offering centers are limited due to rarity.
To our knowledge, this is the first study to examine the volume-outcome relationship in fertility-sparing trachelectomy for early-stage cervical cancer. Utilizing the national database strengthens the interpretation of results and is useful to examine the rare surgical procedure like trachelectomy.
There are several limitations in this study. First, as is inherent to this type of study, there is unmeasured bias in the analysis. Several key confounders that were missing in the analysis due to absence of data or non-distinguishable codes, but likely impact perioperative complications included the patient's performance status, cancer stage, histology subtypes, trachelectomy type (simple versus radical), and hospital quality of care. Moreover, information for sentinel lymph node biopsy was not retrievable in this study during the study period. As this procedure is becoming more common in recentyears [40], lacking this information limits the clinical utility of the study. As the vast majority of women underwent concurrent lymphadenectomy at trachelectomy, it is likely that our study population represented mostly more than microinvasive cervical cancer. However, it is unknown what proportion of patients with more than microinvasive disease did not receive guideline-adherent care in terms of lymph node assessment during trachelectomy in our study [3].
Similarly, though the procedure codes for a robotic approach were available, detailed surgery modes were not distinguishable for the traditional laparoscopy or vaginal approach in the NIS database due to lack of specific codes for trachelectomy. This likely would have impacted the perioperative complication rate. In the recent years, the minimally-invasive robotic approach has been more frequently utilized for trachelectomy in the United States [41]. Information for the history of supracervical hysterectomy is not retrievable in the study, and it is unknown what proportion of the study population underwent trachelectomy for the residual cervix after supracervical hysterectomy. Second, this study only examined outcomes based on hospital surgical volume. It is therefore unknown if individual surgeon's surgical volume, experience, and skills are indeed associated with perioperative complications, however it is expected that these would likely affect the outcomes [42].
Third, the NIS program only captures perioperative complications during the index admission, and not those occurring after discharge. Thus, it is unknown if the inverse association between hospital surgical volume and surgical complication is also sustained in the long-term. Forth, outcome measures were based on the ICD codes but not via review of medical records. Thus, clinical accuracy and relevance of the reported complications are unknown. Fifth, the study period was relatively old and clinical implication to the current practice may be limited. Additionally, the NIS program does not capture same-day surgery, however we suspect that same-day trachelectomy was presumably rare during the study period.
Finally, this study examined only the U.S. population, so the generalizability to different populations is unknown. This is particularly applicable when interpreting what is the definition of a high volume center. In our study, >2 trachelectomies per year qualified as the top 10% of surgical volume, but, it will be paramount to be aware that the populational incidence of cervical cancer varies worldwide; and the defined trachelectomy volume used in our analysis is unlikely to apply in other areas.
In conclusion, fertility-sparing trachelectomy for reproductive-aged women with early-stage cervical cancer was an uncommon surgical procedure in the United States between 2001 and 2011. The number of trachelectomy-offering centers increased nearly 3 times but three quarters of centers had a minimum trachelectomy volume. The hospital surgical volume was an independent predictor for perioperative complications, and performance of trachelectomy at the top 10%ile centers, performing 30% of trachelectomies, was associated with a 65% lower relative risk of short-term composite perioperative complication. Longterm oncologic and obstetrical outcomes, the utility of centralizing care for this procedure, and consensus development of minimum-volume standards merit further investigation.
Supplementary Material
HIGHLIGHTS.
A national study was conducted to examine volume-outcome relationship of fertility-sparing trachelectomy for cervical cancer.
Between 2001 and 2011, fewer than 90 centers performed fertility-sparing trachelectomy.
The majority of trachelectomy-performing centers had minimum surgical volume of one case a year.
Higher hospital surgical volume for trachelectomy may be associated with reduced short-term perioperative morbidity.
Acknowledgments
Funding support
Ensign Endowment for Gynecologic Cancer Research (K.M.)
Footnotes
Declaration of competing interest
Consultant, Clovis Oncology, Tesaro, research funding, Merck (J.D.W.); consultant, Quantgene (L.D.R.); advisory board, Tesaro, GSK (M.K.); research grant, MSD (S.M.); honorarium, Chugai, textbook editorial expense, Springer, and investigator meeting attendance expense, VBL therapeutics (K.M.); none for others.
Appendix A. Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ygyno.2020.01.015.
References
- [1].Cancer stat facts: cervical cancer, National Cancer Institute, Surveillance, Epidemiology, and End Result Program https://seer.cancer.gov/statfacts/html/cervix.html> (9/19/2019). [Google Scholar]
- [2].Siegel RL, Miller KD, Jemal A, Cancer statistics, 2019, CA Cancer J. Clin 69 (2019) 7–34. [DOI] [PubMed] [Google Scholar]
- [3].Cervical cancer, National Comprehensive Cancer Network (US) NCCN Clinical Practice Guideline in Oncology , Version 4.2019. https://www.nccn.org/professionals/physician_gls/pdf/cervical.pdf> (10/14/2019). [Google Scholar]
- [4].Bentivegna E, Gouy S, Maulard A, Chargari C, Leary A, Morice P, Oncological outcomes after fertility-sparing surgery for cervical cancer: a systematic review, Lancet Oncol. 17 (2016)(e240–e53). [DOI] [PubMed] [Google Scholar]
- [5].Zhang Q, Li W, Kanis MJ, Qi G, Li M, Yang X, et al. , Oncologic and obstetrical outcomes with fertility-sparing treatment of cervical cancer: a systematic review and meta-analysis, Oncotarget 8 (2017) 46580–46592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Ramirez PT, Schmeler KM, Soliman PT, Frumovitz M, Fertility preservation in patients with early cervical cancer: radical trachelectomy, Gynecol. Oncol 110 (2008) S25–S28. [DOI] [PubMed] [Google Scholar]
- [7].Cui RR, Chen L, Tergas AI, Hou JY, St Clair CM, Neugut AI et al. , Trends in use and survival associated with fertility-sparing trachelectomy for young women with early-stage cervical cancer, Obstet Gynecol. 131 (2018) 1085–1094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Machida H, Mandelbaum RS, Mikami M, Enomoto T, Sonoda Y, Grubbs BH, et al. , Characteristics and outcomes of reproductive-aged women with early-stage cervical cancer: trachelectomy vs hysterectomy, Am. J. Obstet. Gynecol 219 (461) (2018) e1–e18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Matsuo K, Machida H, Mandelbaum RS, Mikami M, Enomoto T, Roman LD, et al. , Trachelectomy for stage IB1 cervical cancer with tumor size >2 cm: trends and characteristics in the United States, J. Gynecol. Oncol 29 (2018) e85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Shinjo D, Matsumoto K, Terashima K, Takimoto T, Ohnuma T, Noguchi T, et al. , Volume effect in paediatric brain tumour resection surgery: analysis of data from the Japanese national inpatient database, Eur. J. Cancer 109 (2019) 111–119. [DOI] [PubMed] [Google Scholar]
- [11].Moller H, Riaz SP, Holmberg L, Jakobsen E, Lagergren J, Page R, et al. , High lung cancer surgical procedure volume is associated with shorter length of stay and lower risks of re-admission and death: national cohort analysis in England, Eur. J. Cancer 64 (2016) 32–43. [DOI] [PubMed] [Google Scholar]
- [12].Schillemans V, Vrijens F, De Gendt C, Robays J, Silversmit G, Verleye L, et al. , Association between surgical volume and post-operative mortality and survival after surgical resection in lung cancer in Belgium: a population-based study, Eur. J. Surg. Oncol 45 (2019) 2443–2450. [DOI] [PubMed] [Google Scholar]
- [13].Hollenbeck BK, Dunn RL, Miller DC, Daignault S, Taub DA, Wei JT, Volume-based referral for cancer surgery: informing the debate, J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol 25 (2007) 91–96. [DOI] [PubMed] [Google Scholar]
- [14].Chapman BC, Paniccia A, Hosokawa PW, Henderson WG, Overbey DM, Messersmith W, et al. , Impact of facility type and surgical volume on 10-year survival in patients undergoing hepatic resection for hepatocellular carcinoma, J. Am. Coll. Surg 224 (2017) 362–372. [DOI] [PubMed] [Google Scholar]
- [15].Mackay TM, Wellner UF, van Rijssen LB, Stoop TF, Busch OR, Groot Koerkamp B, et al. , Variation in pancreatoduodenectomy as delivered in two national audits, Br.J. Surg 106 (2019) 747–755. [DOI] [PubMed] [Google Scholar]
- [16].Matsuo K, Shimada M, Yamaguchi S, Matoda M, Nakanishi T, Kikkawa F, et al. , Association of radical hysterectomy surgical volume and survival for early-stage cervical Cancer, Obstet. Gynecol. 133 (2019) 1086–1098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Wright JD, Herzog TJ, Siddiq Z, Arend R, Neugut AI, Burke WM, et al. , Failure to rescue as a source of variation in hospital mortality for ovarian cancer, J. Clin. Oncol. Off.J. Am. Soc. Clin. Oncol 30 (2012) 3976–3982. [DOI] [PubMed] [Google Scholar]
- [18].Uppal S, Spencer RJ, Rice LW, Del Carmen MG, Reynolds RK, Griggs JJ, Hospital readmission as a poor measure of quality in ovarian cancer surgery, Obstet. Gynecol. 132 (2018) 126–136. [DOI] [PubMed] [Google Scholar]
- [19].Matsuo K, Matsuzaki S, Mandelbaum RS, Matsushima K, Klar M, Grubbs BH, et al. , Hospital surgical volume and perioperative mortality of pelvic exenteration for gynecologic malignancies, J. Surg. Oncol (2019) 10.1002/jso.25770. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Rouvelas I, Lindblad M, Zeng W, Viklund P, Ye W, Lagergren J, Impact of hospital volume on long-term survival after esophageal cancer surgery, AMA Arch. Surg 142 (2007) 113–117(discussion 8). [DOI] [PubMed] [Google Scholar]
- [21].Kozower BD, Stukenborg GJ, Hospital esophageal cancer resection volume does not predict patient mortality risk, Ann. Thorac. Surg 93 (2012) 1690–1696(discussion 6-8). [DOI] [PubMed] [Google Scholar]
- [22].Chen CS, Liu TC, Lin HC, Lien YC, Does high surgeon and hospital surgical volume raise the five-year survival rate for breast cancer? A population-based study, Breast Cancer Res. Treat 110 (2008) 349–356. [DOI] [PubMed] [Google Scholar]
- [23].Sheckter CC, Rochlin D, Kiwanuka H, Curtin C, Momeni A, The impact of hospital volume on patient safety indicators following post-mastectomy breast reconstruction in the US, Breast Cancer Res. Treat 178 (2019) 177–183. [DOI] [PubMed] [Google Scholar]
- [24].Schrag D, Cramer LD, Bach PB, Cohen AM, Warren JL, Begg CB, Influence of hospital procedure volume on outcomes following surgery for colon cancer, Jama 284 (2000) 3028–3035. [DOI] [PubMed] [Google Scholar]
- [25].Meyerhardt JA Tepper JE, Niedzwiecki D, Hollis DR, Schrag D, Ayanian JZ, et al. , Impact of hospital procedure volume on surgical operation and long-term outcomes in high-risk curatively resected rectal cancer: findings from the intergroup 0114 study, J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol 22 (2004) 166–174. [DOI] [PubMed] [Google Scholar]
- [26].Begg CB, Riedel ER, Bach PB, Kattan MW, Schrag D, Warren JL, et al. , Variations in morbidity after radical prostatectomy, N. Engl.J. Med 346 (2002) 1138–1144. [DOI] [PubMed] [Google Scholar]
- [27].Ellison LM, Trock BJ, Poe NR, Partin AW, The effect of hospital volume on cancer control after radical prostatectomy, J. Urol 173 (2005) 2094–2098. [DOI] [PubMed] [Google Scholar]
- [28].Mayer EK, Bottle A, Darzi AW, Athanasiou T, Vale JA, The volume-mortality relation for radical cystectomy in England: retrospective analysis of hospital episode statistics, BMJ (Clinical research ed) 340 (2010) c1128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [29].Siemens DR, Mackillop WJ, Peng Y, Berman D, Elharram A, Rhee J, et al. , Processes of care and the impact of surgical volumes on cancer-specific survival: a population-based study in bladder cancer, Urology 84 (2014) 1049–1057. [DOI] [PubMed] [Google Scholar]
- [30].Buskwofie A, Huang Y, Tergas AI, Hou JY, Ananth CV, Neugut AI, et al. , Impact of hospital volume on racial disparities and outcomes for endometrial cancer, Gynecol. Oncol 149 (2018) 329–336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Wright JD, Ruiz MP, Chen L, Gabor LR, Tergas AI, St Clair CM, et al. , Changes in surgical volume and outcomes over time for women undergoing hysterectomy for endometrial cancer, Obstet. Gynecol 132 (2018) 59–69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].HCUP National Inpatient Sample (NIS). Healthcare Cost and Utilization Project (HCUP). 2001–2015. Agency for Healthcare Research and Quality, Rockville, MD: <http://www.hcup-us.ahrq.gov/nisoverview.jsp>. (10/14/2019). [Google Scholar]
- [33].Charlson ME, Pompei P, Ales KL, MacKenzie CR, A new method of classifying prognostic comorbidity in longitudinal studies: development and validation, J. Chronic Dis 40 (1987) 373–383. [DOI] [PubMed] [Google Scholar]
- [34].Matsuo K, Mandelbaum RS, Adams CL, Roman LD, Wright JD, Performance and outcome of pelvic exenteration for gynecologic malignancies: a population-based study, Gynecol. Oncol. 153 (2019) 368–375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].Mandelbaum RS, Chen L, Shoupe D, Paulson RJ, Roman LD, Wright JD, et al. , Patterns of utilization and outcome of ovarian conservation for young women with minimal-risk endometrial cancer, Gynecol. Oncol 154 (2019) 45–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [36].Salvo G, Ramirez PT, Leitao M, Cibula D, Fotopoulou C, Kucukmetin A, et al. , International radical trachelectomy assessment: IRTA study, Int. J. Gynecol. Cancer 29 (2019) 635–638. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [37].Uppal S, Rebecca Liu J, Kevin Reynolds R, Rice LW, Spencer RJ, Trends and comparative effectiveness of inpatient radical hysterectomy for cervical cancer in the United States, Gynecol. Oncol 152 (2012-2015) 133–138. [DOI] [PubMed] [Google Scholar]
- [38].Ruiz MP, Chen L, Hou JY, Tergas AI, St Clair CM, Ananth CV, et al. , Effect of minimum-volume standards on patient outcomes and surgical practice patterns for hysterectomy, Obstet. Gynecol 132 (2018) 1229–1237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [39].Wright JD, Huang Y, Melamed A, Tergas AI, St Clair CM, Hou JY, et al. , Potential consequences of minimum-volume standards for hospitals treating women with ovarian cancer, Obstet. Gynecol 133 (2019) 1109–1119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [40].Vercellino GF, Erdemoglu E, Lichtenberg P, Muallem MZ, Richter R, Abu-Rustum NR, et al. , A GCIG international survey: clinical practice patterns of sentinel lymph node biopsies in cervical cancer, Arch. Gynecol. Obstet 300 (2019) 191–199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [41].Matsuo K, Chen L, Mandelbaum RS, Melamed A, Roman LD, Wright JD, Trachelectomy for reproductive-aged women with early-stage cervical cancer: minimally invasive surgery versus laparotomy, Am. J. Obstet. Gynecol 220 (469) (2019) e1–e13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [42].Birkmeyer JD, Finks JF, O'Reilly A, Oerline M, Carlin AM, Nunn AR, et al. , Surgical skill and complication rates after bariatric surgery, N. Engl. J. Med 369 (2013) 1434–1442. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.