

Abstract
Purpose of Review
Historically, there have been many advances in the ways in which we treat kidney diseases. In particular, hemodialysis has set the standard for treatment since the early 1960s and continues today as the most common form of treatment for acute, chronic, and end-stage conditions. However, the rising global prevalence of kidney diseases and our limited understanding of their etiologies have placed significant burdens on current clinical management regimens. This has resulted in a desperate need to improve the ways in which we treat the underlying and ensuing causes of kidney diseases for those who are unable to receive transplants.
Recent Findings
One way of possibly addressing these issues is through the use of improved bioartificial kidneys. Bioartificial kidneys provide an extension to conventional artificial kidneys and dialysis systems, by incorporating aspects of living cellular and tissue function, in an attempt to better mimic normal kidneys. Recent advancements in genomic, cellular, and tissue engineering technologies are facilitating the improved design of these systems.
Summary
In this review, we outline various research efforts that have focused on the development of regenerated organs, implantable constructs, and whole bioengineered kidneys, as well as the transitions from conventional dialysis to these novel alternatives. As a result, we envision that these pioneering efforts can one day produce bioartificial renal technologies that can either perform or reintroduce essential function, and thus provide practical options to treat and potentially prevent kidney diseases.
Keywords: Bioratificial kidney, Regenerative medicine, Bioengineering, Dialysis, Cell therapy and gene therapy
Introduction
Kidney disease is a major source of morbidity and mortality worldwide [1]. Approximately 10% of the global population is affected by debilitating kidney diseases [2]. In lesser developed countries, limited access to affordable treatment accounts for staggering annual death tolls [3]. In comparison, around 80% of the individuals that receive clinical treatments reside in developed nations [4]. Ironically, the prognoses for these patients in either situation are similarly daunting [5]. This is because the current standards of clinical care for acute, chronic, and end-stage injuries are limited to methods that merely manage the diseases. These methods are incapable of treating the underlying causes of concern and are primarily focused on correcting fluid and electrolyte imbalances, as well as the avoiding nephrotoxins [6].
Beyond the current forms of management, renal transplantation is the ultimate option [6, 7]. Unfortunately, the supply of viable organs is greatly outweighed by current demand [8]. This issue will only be compounded within the near future, as we estimate significant increases in the number of individuals with acute, chronic, and end-stage injuries. These increases will correlate with growing elderly, diabetic, and metabolic syndrome patient populations [9]. Other facts that will adversely affect the management of kidney diseases are rising and prohibitive costs of healthcare [2], high rates of transplant rejection [10], and enhanced progressions of acute and chronic conditions to renal failure [11].
As of 2015, our annual healthcare spending increased by 5.8%, which resulted in an average cost of $9990 per person [12]. Such costs accounted for a staggering 20% of the US economy and anticipated to increase in the future [12]. However, the regenerative medicine industry has been identified as one possible way to address these rising and prohibitive costs. A recent report by Mason et al. provided a strong financial case for regenerative medicine [13]. In this report, they outlined that the high costs associated with product development and the efforts need to convince government and wealthy private agencies to fund these ventures as significant upfront challenges. They also identified that the potential returns from reduced direct and indirect costs associated with a healthy working adult, coupled with tax-based revenues generated from this industry will make these initial investments worthwhile [14].
By their estimation, this industry would benefit from reduced ongoing expenditure generated from cheaper regenerative procedures and one-time treatments. Specifically, the renal industry would best benefit from great potential savings associated with having cell-based therapies. Based on the complex structure of the kidney, this regenerative strategy would potentially be able to restore health, thereby reducing benefit payouts, insurance premiums, and patient upkeep across the entire population landscape [13]. Moreover, the fact that renal diseases have high interactions with various metabolic disorders could potentially provide additional savings for a spectrum of medical conditions [12, 14]. A clearer view of the potential value of such regenerative treatments was given using the costs per quality-adjusted life year (QALY) metric. This is a measure of the quality of an individual’s remaining years, which provides a useful way to indicate the effectiveness of a given treatment strategy. For instance, high QALY values, associated with treatments like hip replacements, are linked with an individual ability to return to a normal standard of life. This is in turn valued at $50,000 per year in savings [14]. Now, taking existing renal treatments into consideration, hemodialysis has a QALY value that is 60 times higher than that of hip a replacement. Hemodialysis techniques are incapable generating comparable value, yet regenerative strategies like cell therapies are anticipated to match this normal health benchmark, and thus provide future significant returns on initial investments.
Consequently, there is a dire need to improve the existing management of renal care. One way of possibly achieving this goal is through the development of improved bioartificial kidneys. The term bioartificial kidney generally refers to various replacement therapies, excluding human transplantation, which provide essential functions like filtration and volumetric regulation [15]. Traditionally, this definition was synonymous with dialysis, which as previously mentioned, is not focused on treating the underlying causes of the injury. But, recent advancements in genomic, cellular, and tissue engineering technologies have expanded this definition to include regenerated organs, implantable constructs, and whole bioengineered kidneys [16]. It is envisioned that these technologies could perform additional essential functions like erythropoiesis, hormone secretion, and reabsorption of vital nutrients. Such advancements would radically transform the ways in which we treat kidney diseases. In this review, we look at the major advancements in the bioartificial kidney, stemming from the original dialysis system to recently advanced concepts geared towards replacing damaged kidney tissue and whole organs and its potential to impact the future management of renal diseases.
Dialysis Systems
Wearable and Implantable Artificial Kidneys
Since the introduction of the dialysis machine, we have observed many iterations of the artificial kidney, as summarized in Table 1. However, thus far, there has been limited clinical advancement beyond its original design. This stagnation has translated into significant treatment burdens, reduced survival rates, and a debilitated quality of life [19, 20]. To date, the most advanced clinical systems adequately perform renal filtration, but are incapable of performing essential transport, metabolic, and endocrine functions [21]. They also substantially limit patient activity, require an adherence to strict diet and medication regimens, and spawn prohibitive clinical costs. Nevertheless, it has been suggested that more frequent sessions may be required to ultimately improve patient-centered clinical outcomes [22]. For example, dialysis performed 3 days per week may improve metabolic, ventricular hypertrophy, and blood pressure levels linked to cardiovascular disease. More frequent sessions can also limit the accumulation of fluid, metabolic waste, and uremic toxins. Such evidence has prompted support for portable hemodialysis systems to provide continuous solute clearance and ultrafiltration and potentially improve patient-centered outcomes [22].
Table 1.
The leading solutions for kidney disease
| Renal treatment | Latest advancements | Existing challenges and projected introduction into clinical practice |
|---|---|---|
| Dialysis systems |
|
|
| Regenerative technologies |
|
|
| Bioengineering |
|
|
A significant advancement in the development of a more functional artificial kidney came by way of the renal assist device (RAD). The RAD is a bioartificial system that was first introduced in the 1980s by Aebischer et al. in an attempt to meet the need for additional and complex renal functions that could not be provided by traditional dialysis [23]. This system relies on the series combination of a conventional hemofilter and a bioreactor. The hemofilter mimics glomerular filtration, while the tubular cell-based bioreactor is designed to drive reabsorption, secretion, and other essential metabolic, endocrinologic, and immunologic functions. The inclusion of such live epithelial cellular components drastically extended the utility of traditional dialysis by providing benefits unattainable by inanimate technologies [24]. Since then, such extracorporeal systems have been applied to treat renal failure in animal models, as well as humans in clinical trials.
Pioneering efforts led by Humes et al. have also generated a RAD device containing on the order of one billion renal tubular cells that are grown in confluent monolayers [25]. In vitro, ex vivo and clinical studies have confirmed that these cells retain their capacities to facilitate potassium, bicarbonate, glucose transport; ammonia and hormone secretion; and ultra-filtration. Gura et al. also recently conducted an FDA-approved human trial on a wearable artificial kidney for patients with end-stage injuries [17]. This system is composed of a miniaturized, wearable hemodialysis machine based on dialysate-regenerating sorbent technology. All subjects in this study remained hemodynamically stable over the treatment period, and patient fluid removal matched standard ultrafiltration rates over a 24-h period. The results of these trials provide evidence that wearable artificial kidneys can be a viable alternative to standard dialysis.
A further extension of the wearable RAD system is the implantable artificial kidney, which is dubbed as the implantable renal assist device (iRAD) [16]. The iRAD utilizes microelectromechanical systems (MEMS) to scale down the original RAD design into a compact (teacup-sized), implantable, self-monitoring, and self-regulating bioartificial kidney. The iRAD couples a durable, long-life hemofilter with a bioreactor of renal tubule cells. It is able to mimic in vivo conditions and self-regulate extracellular fluid volume and clearance through integrated MEMS sensors, control electronics, and actuators [16]. This device is expected to drastically improve the quality of a patient’s life. The major achievement of this system will be gauged by its ability to minimize the leakage of albumin and other important macromolecules and simultaneously maximizing water permeability. During the past year, the FDA chose this system as one of the three renal device projects to pilot a new regulatory approval program that intends to bring breakthrough medical device technologies to patients faster and more efficiently [26]. The artificial kidney project by Roy et al. is targeted for clinical trials in 2017 [27]. This project was selected for its transformative potential in treating end-stage renal disease (ESRD) and for its potential to benefit from early interactions with the FDA in the approval process and pave the way for future innovations that have the capacity to transform the current management of renal disease. If successful, the system will demonstrate for the first time a miniaturized implantable RAD for the treatment of ESRD. It is thus hoped that in the long-term, wearable and implantable devices can perform dialysis outside of the clinic and provide the desired results at fractions of the in-center dialysis cost. For instance, in 2014, the dialysis costs associated with both male and female patients were $82,762.00 and $88,928.00, respectively. With the introduction of these advanced dialysis systems, it is anticipated that patients will observe at least a 25% cost reduction [28]. One can also foresee that such systems will reduce the existing limits on activity and potentially provide less intrusion on a patient’s lifestyle.
Renal Regenerative Technologies
Bioactive Compounds
With the intention of transitioning from the original artificial kidney, other areas of research have progressed to focus on the treatment and prevention of the underlying causes of the renal disease. Such a shift has led to the identification of various mechanisms through which we can emulate the body’s native regenerative process. Bioactive compounds play an essential role in this process. In the kidney, various bioactive molecules like cytokines and growth factors promote normal tubular cell differentiation in an effort to replace lost and damaged tubular epithelial and function [29, 30]. This phenomenon has been illustrated in models of acute and chronic injury, whereby hepatocyte growth factor (HGF) [31–33], epidermal growth factor (EGF) [34, 35], transforming growth factor-α (TGF-α) [36, 37], and insulin-like growth factor (IGF-1) [38, 39] have expedited renal recovery.
Studies have identified HGF’s ability to mediate tissue regeneration and protect tubular epithelial cells from injury and apoptosis during acute renal failure [31–33]. It has also been used to help preserve the renal structure in chronic injury models by activating matrix degradation to reduce fibrosis. EGF and TGF-α are well-known mitogens that are expressed in the kidney, which compel several types of renal cells to maintain cell cycle activation [37]. This occurs after either nephrotoxic or ischemic injury, through the increased stimulation of extracellular-regulated kinases to increase DNA synthesis [36, 37]. The comparable use of IGF-1 has provided evidence to support its role in enhancing stem cell-mediated renal repair [38, 39].
While the successes of these studies have generated support for the use of such factors to aid renal regeneration, other studies have provided mixed perspectives. For example, data collected by Kopple et al. highlight the limited regenerative capacity of IGF-1 and the high and frequent doses required to impact repair mechanisms [40]. These stringent demands also increase the potential to generate uncontrolled proliferation [37]. Thus, there is a need for further research that can clearly outline the compounds and their optimal doses that are capable of consistently mitigating regulated tissue regeneration. Simultaneous efforts are also required to construct efficient systems that will facilitate the safe and targeted in vivo delivery of these molecules [41••].
Gene Therapy
Our ever-increasing knowledge of the fundamental genetic mechanisms involved in tissue and organ repair is providing us with promising treatment options. With specific regard to the kidney, these therapies have been proposed to improve the prognoses of patients with acute disorders, by enhancing transplantation outcomes [21, 42], and treating and possibly preventing the underlying causes and results of injury [41••, 43]. These strategies could potentially hinder disease progression and facilitate repair. In comparison, other research efforts have focused on the development of strategies to aid patients affected by chronic conditions. This would be a welcomed tactic to reduce the need for dialysis and transplantation. Continued and complimentary research to identify new key structural and functional targets, and better examine existing ones while improving exogenous gene and cell delivery, will further enhance the utility of these therapies.
Gene therapy has historically focused on the treatment of diseases that arise from single genetic disorders like polycystic kidney disease (PKD). PKD remains as one of the most frequently encountered heredity forms of debilitating renal disease [44, 45]. Treatment for this condition has customarily targeted proteins that are thought to play a mechanistic role in the progression of this disease. Such proteins are located in hair-like structures that exist in tissue that line the inside of cysts [46]. These treatments help ease some of the symptoms of PKD, but are unable to cure the condition. Recent work conducted in mouse models used the growth factor vascular endothelial growth factor C (VEGFC) to alter the architecture of microvessels that surround the cysts. Daily intraperitoneal injections of recombinant VEGFC normalized the patterns of these vessels and improved renal function [47]. They also provided modest, yet significant, increases in lifespan of mice afflicted with either the common or rarer forms of the disease [47].
Alternatively, numerous studies have investigated the effects of modifying the activity of genes and proteins known to have essential roles in the progression of other renal conditions. Investigators have used non-viral and viral vectors to elicit their upregulated or downregulated expressions. For example, in vivo studies have confirmed the renotherapeutic potential of upregulating isocitrate dehydrogenase 2 (IDH2) and a member of the sulfotransferase family (SULT1A1) under hydrodynamic conditions [43]. Enhanced expression of either protein facilitated the maintenance of mitochondrial respiration, supporting the fact that adaptive changes in mitochondria can confer protection to ischemic damage.
Likewise, intravenous injections of plasmids encoding HGF provided protective effects similar to those mentioned previously that were generated from recombinant treatment of this bioactive factor [48]. HGF has also been shown to help preserve renal architecture in chronic injury models by activating matrix degradation to reduce fibrosis [48, 49]. Growth hormone-releasing hormone (GHRH) plasmid-based therapy has also shown promise in feline and canine chronic injury models. GHRH-treated animals had improved survival rates, stimulation of erythropoiesis, and blood urea nitrogen and creatinine clearances compared to those of control animals [18].
Cell Therapy
Cell therapy is yet another rapidly developing regenerative technique that has the potential to support the treatment of various diseases. These approaches chiefly rely on the transplantation of primary, stem cells and progenitor cells. Using these approaches, it is hoped that these treatments could become a reality by 2020 [50]. Our group has recently demonstrated that primary renal cells isolated from human kidneys can be used to support renal recovery in rats with CKD [29]. We showed that the intrarenal delivery of an erythropoietin (EPO)-positive-enriched cells provided better protection from inflammation and oxidative stress than that of unsorted cell cultures. In another study, researchers performed 5/6 nephrectomies in rats to generate CKD [37]. These rats were then treated with tubular cell-enriched population and unfractionated heterogeneous renal cells. Again, the enriched cell fraction provided better therapeutic effects by attenuating canonical pathways of pro-fibrotic extracellular matrix (ECM) production [29]. These results support the potential use of such enriched primary cells for the treatment of degenerative kidney disease.
In comparison, several studies have focused on the use of various stem cells to treat kidney diseases. There has much debate over the ethical use and teratoma-derived side effects surrounding the use of embryonic stem cells for human research. However, less controversy surrounds their potential to alleviate suffering. As such, these technologies are being evaluated for its ability to treat acute and chronic kidney conditions in small and large animals, with the hope of successfully translating these findings to patients. Thus far, investigators have delivered these cells to mice with progressive renal fibrosis. The systemic administration of embryonic stem cells hindered the progression of the ischemia-induced fibrosis [51]. Specifically, these cells facilitated the downregulation of hypoxia and inflammation. In the case of addressing acute concerns, adipose-derived stem cell to proximal tubule epithelial cell differentiation has been successfully promoted using condition media [52]. This discovery may prove to be useful for the treatment of acute kidney injury (AKI), by promoting tubular regeneration, at the major site of injury in this disease [53]. Other animal studies using mesenchymal stem cells have also generated exciting results. Exogenously delivered bone marrow-derived stem cells have shown to promote renal tubular cells, mesangial, glomerular endothelial, and podocyte cell transdifferentiation [37]. Other related studies have demonstrated the ability to harness the therapeutic effects generated from growth and trophic factors and cytokines released from these stem cells, as well as their ability to mediate paracrine-based therapeutic activity. In particular, mesenchymal stem cells have been used to regenerate kidneys after AKI [54], and their repeated administration has directly reduced renal fibrosis, aided kidney tissue remodeling, and elevated microvascular density [55].
In an attempt to strike ethical and safety balances, researchers have focused on the development of cell therapies using fetal and adult stem cells. For example, amniotic fluid stem cells (AFSCs) exhibit substantial differentiation and self-renewal capacities minus the teratoma formation. Using these cells, Perin et al. demonstrated that after isolation, human AFSCs that were expanded in culture and reintroduced into murine embryonic kidneys also underwent organ development in vitro [37, 52]. These results outlined their potential to support organ development, as well as renal regeneration. Likewise, adipose-, bone marrow-, mesenchymal-, neuronal-derived adult, or progenitor stem cells have been widely used for tissue repair. These cell types are quite attractive options as they maintain the ability to self-renew and differentiate into multiple lineages, again with a limited risk of teratoma formation [56]. They can also be readily obtained and highly expanded in culture [57].
Similarly, the Nobel Prize-winning research that uncovered the manner in which mature, specialized cells can be reprogrammed to become immature cells called induced pluripotent stem cells (iPSC) capable of developing into all tissues of the body has revolutionized our understanding of cellular and tissue development [58]. Since then, IPSC technology has provided an intriguing system that allows manipulation of signaling to direct the differentiation of stem cell niches towards a variety of renal lineages. In the same way, the controversial existence and identification of rare renal progenitors, which express essential signal-transducing molecules and possess highly clonogenic and self-renewal capabilities, define a potential regenerative pathway. These recent efforts have demonstrated that directed differentiated of stem and progenitor cells into three-dimensional clusters containing whole nephron segments. From these findings, it is possible to envision the use of such immunocompatible tissue segments, which can be derived from a patient’s cells, to develop clinically functional bioartificial kidneys. Overall, these data demonstrate the potential application of primary cells, and embryonic, fetal, adult, and induced pluripotent stem cells for the treatment of kidney diseases, as shown in Fig. 1.
Fig. 1.
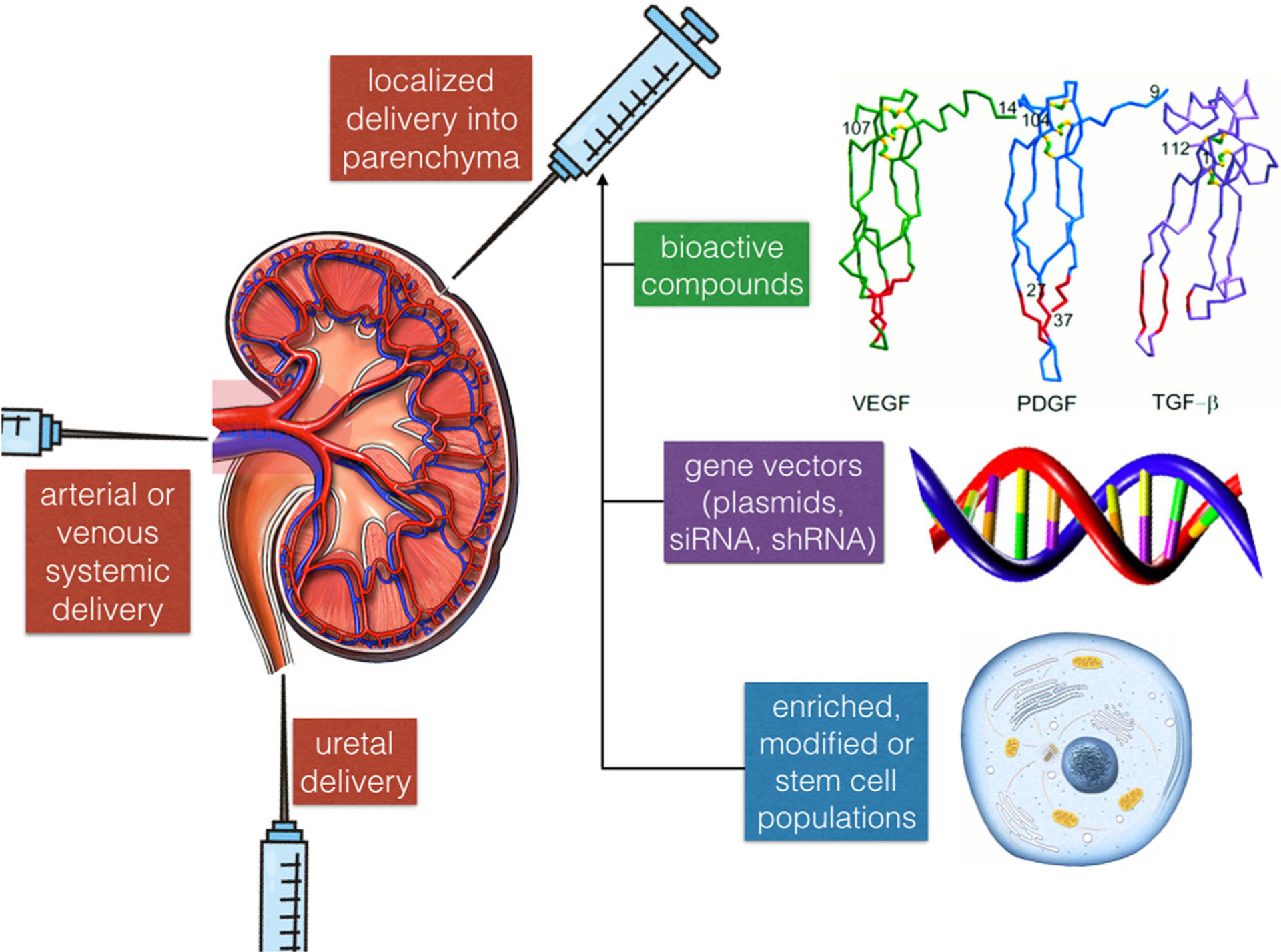
An illustration of bioactive compound, gene therapy, and cell therapy-based renal regeneration technologies. PDGF platelet-derived growth factor, TGF-β transforming growth factor-beta, VEGF vascular endothelial growth factor
Engineering Whole Kidney and Renal Constructs
Other exciting prospects for the development of bioartificial kidneys are scaffolding systems. Scaffolds provide a template, i.e., means to develop tissue constructs and whole organs. Specifically, the principal function of a scaffolding system is to direct cell migration, proliferation, and differentiation and preservation of specific phenotypes. Thus, it is essential that scaffolding systems possess the following three properties. First, the system should contain appropriate biological compounds capable of stimulating and guiding tissue growth [59]. These compounds should be able to also provide specific cues that drive the formation of functional tissues and/or organs. Second, the scaffold should have intact porous three-dimensional structures that can provide sufficient space to properly facilitate the cellular reintroduction [60]. This would ensure an adequate supply of oxygen and nutrients and eliminate the need for cells to compete for survival. Third, the system should also possess the necessary mechanical properties that will maintain tissue formation during in vitro culture and in vivo implantation, as well as support biodegradation necessary for impending tissue growth within the scaffold [61].
Based on the need for these properties, three classes of biomaterials are generally used for scaffolding systems: acellular tissues/organs; natural polymer; and synthetic polymer matrices [60]. Acellular matrices are generated by a process known as decellularization. Decellularization isolates the extracellular matrix of the tissue from its native cells and leaving behind an ECM scaffold of the original organ. Decellularized matrices would offer a microenvironment naturally dense of molecular cues able to drive endogenous organ fabrication [62, 63•]. Human-sized renal scaffolds generated from pig and discarded human kidneys appear to be quite a desirable approach for the development of replacement kidneys. Natural and synthetic polymers provide alternatives to acellular structures. Natural polymers contain a combination of collagen, hyaluronic acid, alginate, agarose, chitosan, fibrin, and gelatin, which serve their ability to adequately support cell adhesion, migration, proliferation, and differentiation [59]. Moreover, the majority of naturally derived polymers have properties that are comparable to innate tissues. In comparison, many of the properties of synthetic polymers vary significantly from those of native tissues and provide less favorable interactions within physiological environments.
These scaffolding systems, as shown in Fig. 2, can be used in combination with previous outlined stem/progenitor and relevant primary cell sources for the recellularization of renal scaffolds [60, 62, 64]. Recellularization is the reintroduction of renal cells into acellular or polymer matrices. After their reintroduction, it is anticipated that these cells can undergo some degree of self-organization to create regions of functional tissues. Initially, renal-specific cells are an integral component of the recellularization process. Therefore, it is feasible to seed scaffolds with stem or progenitor cells, as they have the potential to differentiate into various renal lineages and form functional renal structures. However, an ideal clinical setting would rely on patient-derived cells. Recellularization using patient-specific iPSCs would potentially eliminate immune rejections following implantation. Similarly, primary renal cells would offer a more practical option to obtain optimal sources for recellularization.
Fig. 2.

An outline of the properties of scaffolding systems and the applications for treatment of renal diseases
However, several drawbacks might be encountered when a native matrix is processed and has undergone recellularization. One major concern is the ability to maintain an intact microvasculature within the scaffold. Specifically, researchers have identified angiogenic control as the most significant factor that impacts the clinical success of the tissue engineering field [65]. Decellularized kidneys require a microvascular system capable of supporting endothelial cell linings that can minimize the potential for thrombus formation when transplanted into a living recipient. Moreover, in the absence of an internal vasculature, cell survival within tissue constructs will depend primarily on diffusion [65, 66]. As a result, the innately complex architecture of the kidney and the provisions it makes to maintain its numerous cell populations require special cell-seeding allowances that can permit the proper formation and function of structures like the glomerulus and proximal tubule. Additionally, it is necessary that the derived/primary renal cells maintain their phenotypes prior to implantation.
Conclusions
In conclusion, kidney disease is a major global source of morbidity and mortality. The present clinical standard of care relies primarily on correcting fluid and electrolyte imbalances and the avoidance of nephrotoxins. This standard is incapable of treating the underlying causes of debilitating forms of injury. Thus, there is a clearly defined need to improve the existing management and treatment of renal disease. One way of possibly achieving this goal is through the development of improved bioartificial kidneys. Advancements in the bioartificial kidney, stemming from the traditional dialysis to more recent concepts that rely on hybrid dialysis, regenerative therapies, and whole-organ engineering are exciting options. However, before these novel systems become clinical standards, further research is required to investigate the microelectromechanical and cell and scaffolding systems that can be used to facilitate renal artificial function and drive organ regeneration and recellularization. It is also necessary for us to balance ethical issues and safety that support their respective development and long-term implantation.
Footnotes
Conflict of Interest
Peter R. Corridon has a patent pending on hydrodynamic methods for delivering fluids to kidney tissues and related materials and methods.
In Kap Ko, James J. Yoo, and Anthony Atala declare that they have no conflict of interest.
References
Papers of particular interest, published recently, have been highlighted as:
• Of importance
•• Of major importance
- 1.Stevens LA, Viswanathan G, Weiner DE. CKD and ESRD in the elderly: current prevalence, future projections, and clinical significance. Adv Chronic Kidney Dis. 2010;17(4):293–301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ojo A. Addressing the global burden of chronic kidney disease through clinical and translational research. Trans Am Clin Climatol Assoc. 2014;125:229–46. [PMC free article] [PubMed] [Google Scholar]
- 3.Hunter DJ, Reddy KS. Noncommunicable diseases. N Engl J Med. 2013;369(14):1336–43. [DOI] [PubMed] [Google Scholar]
- 4.Global Facts: About Kidney Disease [Internet]. The National Kidney Foundation. 2015 2016. Available from: https://www.kidney.org/kidneydisease/global-facts-about-kidney-disease.
- 5.Kidney Disease Statistics for the United States [Internet]. 2016. Available from: https://www.niddk.nih.gov/health-information/health-statistics/Pages/kidney-disease-statistics-united-states.aspx.
- 6.Ethiopia KP. Acute kidney injury: an overview [Internet]. 2016. Available from: https://www.uspharmacist.com/article/acute-kidney-injury-an-overview.
- 7.Abecassis M, Bartlett ST, Collins AJ, Davis CL, Delmonico FL, Friedewald JJ, et al. Kidney transplantation as primary therapy for end-stage renal disease: a National Kidney Foundation/Kidney Disease Outcomes Quality Initiative (NKF/KDOQI™) conference. Clin J Am Soc Nephrol CJASN. 2008;3(2):471–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Rosen L, Vining AR, Weimer DL. Addressing the shortage of kidneys for transplantation: purchase and allocation through chain auctions. J Health Polit Policy Law. 2011;36(4):717–55. [DOI] [PubMed] [Google Scholar]
- 9.Mallappallil M, Friedman EA, Delano BG, McFarlane SI, Salifu MO. Chronic kidney disease in the elderly: evaluation and management. Clin Pract Lond Engl. 2014;11(5):525–35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Chapman JR. What are the key challenges we face in kidney transplantation today? Transplant Res. 2013;2(1):1–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Anderson S, Halter JB, Hazzard WR, Himmelfarb J, Horne FM, Kaysen GA, et al. Prediction, progression, and outcomes of chronic kidney disease in older adults. J Am Soc Nephrol. 2009;20(6): 1199–209. [DOI] [PubMed] [Google Scholar]
- 12.Martin AB, Hartman M, Washington B, Catlin A, Team the NHEA. National Health Spending: Faster Growth In 2015 As Coverage Expands And Utilization Increases. Health Aff (Millwood). 2016. December 2; 10.1377/hlthaff.2016.1330. [DOI] [PubMed] [Google Scholar]
- 13.Mason C, Dunnill P. The strong financial case for regenerative medicine and the regen industry. Regen Med. 2008;3(3):351–63. [DOI] [PubMed] [Google Scholar]
- 14.Bubela T, McCabe C, Archibald P, Atkins H, Bradshaw SE, Kefalas P, et al. Bringing regenerative medicines to the clinic: the future for regulation and reimbursement. Regen Med. 2015;10(7):897–911. [DOI] [PubMed] [Google Scholar]
- 15.Tasnim F, Deng R, Hu M, Liour S, Li Y, Ni M, et al. Achievements and challenges in bioartificial kidney development. Fibrogenesis Tissue Repair. 2010;3:14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kim S, Fissell WH, Humes HD, Roy S. Current strategies and challenges in engineering a bioartificial kidney. Front Biosci Elite Ed. 2015;7:215–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Gura V, Rivara MB, Bieber S, Munshi R, Smith NC, Linke L, et al. A wearable artificial kidney for patients with end-stage renal disease. JCI Insight [Internet]. 2016. Fast Track, Breakthrough Therapy, Accelerated. 2016;1(8). Available from: https://insight.jci.org/articles/view/86397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Brown PA, Bodles-Brakhop AM, Pope MA, Draghia-Akli R. Gene therapy by electroporation for the treatment of chronic renal failure in companion animals. BMC Biotechnol. 2009;9:4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Parker T, Hakim R, Nissenson AR, Steinman T, Glassock RJ. Dialysis at a crossroads: 50 years later. Clin J Am Soc Nephrol. 2011;6(2):457–61. [DOI] [PubMed] [Google Scholar]
- 20.Szeto C-C. Peritonitis rates of the past thirty years: from improvement to stagnation. Perit Dial Int J Int Soc Perit Dial. 2014;34(2): 151–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Humes HD. Stem cells: the next therapeutic frontier. Trans Am Clin Climatol Assoc. 2005;116:167–84. [PMC free article] [PubMed] [Google Scholar]
- 22.Fissell WH, Roy S, Davenport A. Achieving more frequent and longer dialysis for the majority: wearable dialysis and implantable artificial kidney devices. Kidney Int. 2013;84(2):256–64. [DOI] [PubMed] [Google Scholar]
- 23.Aebischer P, Ip TK, Panol G, Galletti PM. The bioartificial kidney: progress towards an ultrafiltration device with renal epithelial cells processing. Life Support Syst J Eur Soc Artif Organs. 1987;5(2): 159–68. [PubMed] [Google Scholar]
- 24.Humes HD, Buffington D, Westover AJ, Roy S, Fissell WH. The bioartificial kidney: current status and future promise. Pediatr Nephrol. 2013;29(3):343–51. [DOI] [PubMed] [Google Scholar]
- 25.Song JH, Humes HD. The bioartificial kidney in the treatment of acute kidney injury. Curr Drug Targets. 2009;10(12):1227–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Commissioner O of the. Fast Track, Breakthrough Therapy, Accelerated Approval, Priority Review [Internet]. 2017. Available from: http://www.fda.gov/ForPatients/Approvals/Fast/default.htm.
- 27.McCoy L Artificial kidneys may start saving lives soon MedCareer News [Internet]. MedCareer News. 2015. 2016. Available from: https://www.medcareernews.com/artificial-kidneys-may-start-saving-lives-soon/. [Google Scholar]
- 28.Beltz AD. Wearable, portable, light-weight artificial kidney [Internet]. US5284470 A, 1994 2017. Available from: https://www.google.com/patents/US5284470. [Google Scholar]
- 29.Chung HC, Ko IK, Atala A, Yoo JJ. Cell-based therapy for kidney disease. Korean J Urol. 2015;56(6):412–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Ko IK, Lee SJ, Atala A, Yoo JJ. In situ tissue regeneration through host stem cell recruitment. Exp Mol Med. 2013;45(11):e57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Gong R Anti-inflammatory effect of hepatocyte growth factor in chronic kidney disease: targeting the inflamed vascular endothelium. J Am Soc Nephrol. 2006;17(9):2464–73. [DOI] [PubMed] [Google Scholar]
- 32.Homsi E, Janino P, Biswas SK, Mizuno S, Nakamura T, Lopes de Faria JB. Attenuation of glycerol-induced acute kidney injury by previous partial hepatectomy: role of hepatocyte growth factor/cmet axis in tubular protection. Nephron Exp Nephrol. 2007;107(3): e95–106. [DOI] [PubMed] [Google Scholar]
- 33.Sugimura K, Goto T, Tsuchida K, Takemoto Y, Kim T, Kishimoto T. Production and activation of hepatocyte growth factor in acute renal failure. Ren Fail. 2001;23(3–4):597–603. [DOI] [PubMed] [Google Scholar]
- 34.Tang J, Liu N, Zhuang S. Role of epidermal growth factor receptor in acute and chronic kidney injury. Kidney Int. 2013. May;83(5): 804–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Yen T-H, Alison MR, Goodlad RA, Otto WR, Jeffery R, Cook HT, et al. Epidermal growth factor attenuates tubular necrosis following mercuric chloride damage by regeneration of indigenous, not bone marrow-derived cells. J Cell Mol Med. 2015;19(2):463–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Carley WW, Milici AJ, Madri JA. Extracellular matrix specificity for the differentiation of capillary endothelial cells. Exp Cell Res. 1988;178(2):426–34. [DOI] [PubMed] [Google Scholar]
- 37.Moon KH, Ko IK, Yoo JJ, Atala A. Kidney diseases and tissue engineering. Methods San Diego Calif. 2016;99:112–9. [DOI] [PubMed] [Google Scholar]
- 38.Serum and urinary insulin-like growth factor-1 and tumor necrosis factor in neonates with and without acute renal failure—ProQuest [Internet]. 2016. Available from: http://search.proquest.com/openview/90ca0b91ceba92d1e5ee4b64828a894f/1?pq-origsite=gscholar. [DOI] [PubMed]
- 39.Bach LA, Hale LJ. Insulin-like growth factors and kidney disease. Am J Kidney Dis Off J Natl Kidney Found. 2015. February;65(2):327–36. [DOI] [PubMed] [Google Scholar]
- 40.Kopple JD, Massry SG. Kopple and Massry’s Nutritional Management of Renal Disease. Lippincott Williams & Wilkins; 2004. 712 p. [Google Scholar]
- 41.••.Corridon PR, Rhodes GJ, Leonard EC, Basile DP, Gattone VH, Bacallao RL, et al. A method to facilitate and monitor expression of exogenous genes in the rat kidney using plasmid and viral vectors. Am J Physiol Renal Physiol. 2013;304(9):F1217–29. [DOI] [PMC free article] [PubMed] [Google Scholar]; This method can serve to reduce the barriers to preclinical assessments of clinical interventions related to the kidney.
- 42.Wynn R Stem cell transplantation in inherited metabolic disorders. Hematol Educ Program Am Soc Hematol Am Soc Hematol Educ Program. 2011;2011:285–91. [DOI] [PubMed] [Google Scholar]
- 43.Corridon P, Rhodes G, Zhang S, Bready D, Xu W, Witzmann F, et al. Hydrodynamic delivery of mitochondrial genes in vivo protects against moderate ischemia-reperfusion injury in the rat kidney (690.17). FASEB J. 28(1 Supplement):690.17. [Google Scholar]
- 44.Merta M, Kohoutová M, Rysavá R. Perspectives in gene therapy of polycystic kidney disease. Sb Lek. 1999;100(4):259–68. [PubMed] [Google Scholar]
- 45.Torres VE, Harris PC. Mechanisms of disease: autosomal dominant and recessive polycystic kidney diseases. Nat Clin Pract Nephrol. 2006;2(1):40–55. [DOI] [PubMed] [Google Scholar]
- 46.Freedman BS. Modeling kidney disease with iPS cells. Biomark Insights. 2015;10(Suppl 1):153–69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Huang JL, Woolf AS, Kolatsi-Joannou M, Baluk P, Sandford RN, Peters DJM, et al. Vascular endothelial growth factor C for polycystic kidney diseases. J Am Soc Nephrol. 2015. ;ASN.2014090856. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Systemic administration of naked plasmid encoding hepatocyte growth factor ameliorates chronic renal fibrosis in mice. Publ Online 21 Sept 2001 Doi101038sjgt3301545 [Internet]. 2001. 21 [cited 2016 Oct 10];8(19). Available from: http://www.nature.com/gt/journal/v8/n19/full/3301545a.html. [DOI] [PubMed] [Google Scholar]
- 49.Dai C, Yang J, Liu Y. Single injection of naked plasmid encoding hepatocyte growth factor prevents cell death and ameliorates acute renal failure in mice. J Am Soc Nephrol JASN. 2002;13(2):411–22. [DOI] [PubMed] [Google Scholar]
- 50.Anders H-J, Rovin B, Jayne D, Brunetta P, Coppo R, Davidson A, et al. ISN Nexus 2016 Symposia: translational immunology in kidney disease—the berlin roadmap. Kidney Int Rep. 2016;1(4):327–39. [Google Scholar]
- 51.Maeshima A, Nakasatomi M, Nojima Y. Regenerative medicine for the kidney: renotropic factors, renal stem/progenitor cells, and stem cell therapy. BioMed Res Int [Internet]. 2014. [cited 2016 10];2014 Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4034406/. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Chung HC, Ko IK, Atala A, Yoo JJ. Cell-based therapy for kidney disease. Korean J Urol. 2015;56(6):412–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Chou Y-H, Pan S-Y, Yang C-H, Lin S-L. Stem cells and kidney regeneration. J Formos Med Assoc. 2014;113(4):201–9. [DOI] [PubMed] [Google Scholar]
- 54.Lin F Stem cells in kidney regeneration following acute renal injury. Pediatr Res. 2006;59(S4):74R–8R. [DOI] [PubMed] [Google Scholar]
- 55.Lee S-R, Lee S-H, Moon J-Y, Park J-Y, Lee D, Lim SJ, et al. Repeated administration of bone marrow-derived mesenchymal stem cells improved the protective effects on a remnant kidney model. Ren Fail. 2010;32(7):840–8. [DOI] [PubMed] [Google Scholar]
- 56.Orciani M, Emanuelli M, Martino C, Pugnaloni A, Tranquilli AL, Di Primio R. Potential role of culture mediums for successful isolation and neuronal differentiation of amniotic fluid stem cells. Int J Immunopathol Pharmacol. 2008;21(3):595–602. [DOI] [PubMed] [Google Scholar]
- 57.Gholizadeh-Ghalehaziz S, Farahzadi R, Fathi E, Pashaiasl M. A mini overview of isolation, characterization and application of amniotic fluid stem cells. Int J Stem Cells. 2015;8(2):115–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Nakamura M, Okano H. Cell transplantation therapies for spinal cord injury focusing on induced pluripotent stem cells. Cell Res. 2013;23(1):70–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Arenas-Herrera JE, Ko IK, Atala A, Yoo JJ. Decellularization for whole organ bioengineering. Biomed Mater Bristol Engl. 2013;8(1):14106. [DOI] [PubMed] [Google Scholar]
- 60.Kim I-H, Ko IK, Atala A, Yoo JJ. Whole kidney engineering for clinical translation. Curr Opin Organ Transplant. 2015;20(2):165–70. [DOI] [PubMed] [Google Scholar]
- 61.Scarritt ME, Pashos NC, Bunnell BA. A review of cellularization strategies for tissue engineering of whole organs. Front Bioeng Biotechnol [Internet]. 2015. 30 [cited 2016 Sep 30];3 Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4378188/. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Song JJ, Ott HC. Organ engineering based on decellularized matrix scaffolds. Trends Mol Med. 2011;17(8):424–32. [DOI] [PubMed] [Google Scholar]
- 63.•.Madariaga MLL, Ott HC. Bioengineering kidneys for transplantation. Semin Nephrol. 2014;34(4):384–93. [DOI] [PMC free article] [PubMed] [Google Scholar]; This study provides thorough descriptions of key elements need to support the development of bioengineered kidneys.
- 64.Guyette JP, Charest JM, Mills RW, Jank BJ, Moser PT, Gilpin SE, et al. Bioengineering human myocardium on native extracellular matrixnovelty and significance. Circ Res. 2016;118(1):56–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Cooper TP, Sefton MV. Fibronectin coating of collagen modules increases in vivo HUVEC survival and vessel formation in SCID mice. Acta Biomater. 2011;7(3):1072–83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Corstorphine L, Sefton MV. Effectiveness factor and diffusion limitations in collagen gel modules containing HepG2 cells. J Tissue Eng Regen Med. 2011;5(2):119–29. [DOI] [PMC free article] [PubMed] [Google Scholar]