

Abstract
Objective:
To assess the validity and clinical utility of the Brief Illness Perception Questionnaire (BIPQ) to measure illness perceptions in multiple forms of vasculitis.
Methods:
Patients with giant cell arteritis (GCA), Takayasu’s arteritis (TAK), ANCA-associated vasculitis (AAV) and relapsing polychondritis (RP) were recruited into a prospective, observational cohort. Patients independently completed the BIPQ, Multidimensional Fatigue Inventory (MFI), SF-36 Health Survey (SF-36) and a Patient Global Assessment (PtGA) at successive study visits. Physicians concurrently completed a Physician Global Assessment (PhGA) form. Illness perceptions, as assessed by the BIPQ, were compared to responses from the full-length Revised Illness Perception Questionnaire (IPQ-R) and to other clinical outcome measures.
Results:
196 patients (GCA=47, TAK=47, RP=56, AAV=46) were evaluated over 454 visits. Illness perception scores in each domain were comparable between the BIPQ and IPQ-R (3.28 vs 3.47, p=0.22). Illness perceptions differed by type of vasculitis, with the highest perceived psychological burden of disease in RP. The BIPQ was significantly associated with all other patient-reported outcome measures (ρ=0.50–0.70, p<0.0001) but did not correlate with PhGA (ρ=0.13, p=0.13). A change in the BIPQ composite score of ≥7 over successive visits was associated with concomitant change in the PtGA. Change in the MFI and BIPQ scores significantly correlated over time (ρ= 0.38, p=0.0008).
Conclusions:
The BIPQ is an accurate and valid assessment tool to measure and monitor illness perceptions in patients with vasculitis. Use of the BIPQ as an outcome measure in clinical trials may provide complimentary information to physician-based assessments.
Keywords: giant cell arteritis, Takayasu’s arteritis, vasculitis, cohort studies
Introduction
Vasculitis encompasses a rare set of systemic autoimmune diseases characterized primarily by inflammation of blood vessels. These diseases can result in organ damage leading to life-threatening complications. Different types of vasculitis are often classified by the size of affected arteries into three main categories: small vessel vasculitis (e.g. granulomatosis with polyangiitis, GPA); medium vessel vasculitis (e.g. polyarteritis nodosa, PAN); and large vessel vasculitis (e.g. giant cell arteritis, GCA)(1). Beyond these categories, patients with other systemic autoimmune conditions can develop vasculitis as an associated disease feature. For example, relapsing polychondritis (RP) is a rare disease characterized by inflammation of cartilaginous structures, with associated vasculitis reported in 10–20% of these patients(2, 3). The various forms of vasculitis are generally chronic, unpredictable, relapsing illnesses that pose significant physical and psychological burdens on patients(2, 4).
Illness perceptions are the formulated beliefs that patients have about their illness. According to Leventhal’s Self-Regulatory Model, illness perceptions can be confined to specific domains(5). Common illness perception domains include beliefs about the symptoms attributed to the disease, what caused the illness, the length of time the illness will last, how much the illness affects the patient’s life, and how much the treatment can control the illness. Patient perception of disease may not always align with physician-based assessments in vasculitis(6). Physicians may prioritize different aspects of illness compared to patients in the assessment of vasculitis(6). Therefore, it may be important to consider patient-reported outcome measures in addition to physician-based measures of disease activity.
The revised Illness Perception Questionnaire (IPQ-R) is an extensive survey that was developed to assess illness perceptions. The IPQ-R has been used in a wide range of diseases and can be customized to a specific disease(7, 8). A previous study demonstrated the utility of the IPQ-R in vasculitis and confirmed that patients with different forms of vasculitis commonly perceive a high burden of illness(4). While the IPQ-R is useful to understand patient-held beliefs about disease, the survey is lengthy and can be burdensome to complete. The Brief Illness Perception Questionnaire (BIPQ) was developed to provide a rapid assessment of illness perception(9). While the BIPQ has been used to assess illness perception in a range of diseases, it has not been validated for use in patients with vasculitis(10).
Therefore, the objectives of the current study were to 1) assess the validity of the BIPQ to measure illness perceptions in several forms of systemic vasculitis and to 2) determine the relationship of the BIPQ to other patient- and physician-reported outcome measures in vasculitis.
Methods
Study population
Patients with different forms of systemic vasculitis were recruited into a prospective, observational cohort at the National Institutes of Health in Bethesda, MD, USA. The diseases included in this study were chosen to represent different forms of vasculitis, including giant cell arteritis (GCA), Takayasu’s arteritis (TAK), ANCA-associated vasculitis (AAV) and relapsing polychondritis (RP). Patients with AAV had either eosinophilic granulomatosis with polyangiitis (EGPA), granulomatosis with polyangiitis (GPA) or microscopic polyangiitis (MPA). Each patient’s diagnosis was confirmed by the evaluating study team, and every patient met established classification or diagnostic criteria for their disease(11–15). All patients provided written informed consent and the study protocol was approved by local ethics review (NIAMS IRB: 14-AR-0200).
Data elements and assessment intervals
Patient demographics were recorded, including age, sex, race and ethnicity. Patients were assessed at 3–6 month intervals. At each study visit, patients completed the Brief Illness Perception Questionnaire (BIPQ); the Multidimensional Fatigue Inventory (MFI); the SF-36 Health Survey; and a Patient Global Assessment (PtGA). Similarly, at each visit, the study team physicians completed a Physician Global Assessment (PhGA) blinded to all patient-reported data.
Patient-reported outcome measures and physician-reported outcome measures
The Brief Illness Perception Questionnaire (BIPQ)
The BIPQ is a 9-item questionnaire that measures illness perceptions across nine domains. The illness perception domains assessed by the BIPQ are: identity–symptoms experienced (1 item), timeline-acute/chronic–perception on length of disease (1 item), consequences–effect of disease on one’s life (1 item), personal control–control over disease (1 item), treatment control–perception of treatment impact (1 item), emotional representations–emotional effect of disease (1 item), illness coherence–understanding of disease (1 item), illness concern–concern about disease (1 item), and cause–perceived cause of disease. The cause item is an open-ended question which asks patients to rank the top three factors they believe caused their disease. The other eight questions are scored on a 0 to 10 scale. The personal control, treatment control and coherence items are reverse scored, as higher scores in these elements represent positive illness perceptions(9, 10). To calculate a composite BIPQ score, the individual 8 domain scores are summed together. A higher BIPQ score indicates a greater perceived psychological burden of illness (range: 0–80).
The Multidimensional Fatigue Inventory (MFI-20)
The MFI-20 has been widely used to measure fatigue in a variety of diseases(4). The MFI-20 has 20 questions that measure five different domains of fatigue. The general fatigue domain has previously been shown to differentiate between vasculitis patients and healthy controls(4). In this study, only the general domain items were used. The general domain consists of 4 questions; (1) I feel fit, (2) I feel tired, (3) I am rested, and (4) I tire easily. Each item is scored on a 5-point Likert scale (1-strongly disagree to 5-strongly agree), with questions 1 and 3 reverse-scored. The 4 items are summed to generate a composite score. Scores range from 4–20, and higher scores represent a higher level of fatigue(4, 16).
Short-Form-36 Health Survey (SF-36)
The SF-36 is a 36-item questionnaire that measures health related quality of life (HRQOL) across eight domains. The SF-36 domains include: physical functioning (10 items), role limitations due to physical health (4 items), role limitations due to emotional problems (3 items), energy/fatigue (4 items), emotional well-being (5 items), social functioning (2 items), pain (2 items) and general health (5 items). There is an additional unscaled question that measures change in health. Version 2.0 of the SF-36 was used in the current study. The domain scores are scaled to a 0–100 scale (0 – poor health, 100 – best possible health). The SF-36 responses can be condensed into a Physical Composite Score (PCS) and a Mental Composite Score (MCS)(17–19).
Patient Global Assessment (PtGA)
At each visit, patients rated the severity of their vasculitis disease on the day of the study visit. PtGA was assessed on a scale of 0 (no disease) to 10 (very severe disease). This measure has previously been validated in different forms of vasculitis (19, 20).
Physician Global Assessment (PhGA)
The PhGA is widely used to measure physician-observed assessment of disease activity (20). The PhGA has been used as a clinical assessment measure in different forms of vasculitis (19). PhGA was measured on a scale from 0 (clinical remission) to 10 (very active disease). PhGA > 0 was assigned to patients experiencing any clinical feature that could be directly attributed to active vasculitis. Fatigue or elevated acute phase reactants alone were not considered clinically active disease. PhGA was performed blinded to all patient-reported outcome measures.
Illness Perception Questionnaire-Revised (IPQ-R)
To compare the BIPQ to the more extensive full-length IPQ-R, patient-level data was extracted from a previous online study where 692 patients with self-reported vasculitis completed the IPQ-R (3). The IPQ-R assesses illness perception across nine domains and has 80 items. The nine domains include: identity (22 items), timeline-acute/chronic (6 items), timeline-cyclical (4 items), consequences (6 items), personal control (6 items), treatment control (5 items), emotional representations (6 items), illness coherence (5 items) and cause (3 items). The vasculitis identity domain is measured on a 0–22 point scale. All other domains use a 5 point Likert scale (1- strongly disagree, 2- disagree, 3-neither agree or disagree, 4-agree, 5-strongly agree)(4).
Analytic methods
Validity of the Brief Illness Perception Questionnaire
Scores on the BIPQ from this study were compared to scores on the IPQ-R from previously published data (3). Responses from patients with GCA, TAK, or AAV were studied, as patients with RP were not included in the previous IPQ-R study. To determine if the BIPQ could be used as a surrogate for the IPQ-R, disease-specific scores for each illness perception domain were compared between the BIPQ and IPQ-R using a two-tailed student’s t-test. As the BIPQ scale is different from the IPQ-R scale, BIPQ domain scores were first transformed from a 0–10 point scale to a 1–5 point scale using the Linear Stretch method(21). The IPQ-R vasculitis identity scale was not included in these analyses as it uses a 0-to-22-point scale and is very different from the other domains(4). Further, domains unique to either the BIPQ or IPQ-R were not included in analyses, including the IPQ-R timeline-cyclical and the BIPQ illness concern.
Validity of creating a composite summary score of the BIPQ domains
If appropriate, domain elements of the BIPQ may be combined into a single summary score that could be used to monitor illness perceptions (9). There is no clear consensus on the appropriate methodology to justify use of a BIPQ composite score, and investigators have combined between 2 and eight domain items (22). Pearson correlation was used to study whether pairwise domain items were strongly correlated (e.g. r>0.70). Factor analysis (maximum likelihood factoring method with varimax rotation) was used to explore whether data reduction was appropriate. Optimal number of factors was selected based on Scree plot and chi square testing. A factor loading of >0.60 was considered a strong association (23).
Validity of the BIPQ for assessing disease-specific differences in illness perceptions
To determine whether the BIPQ is useful to identify disease-specific differences in illness perception, BIPQ scores were compared between patients with different forms of vasculitis using one-way ANOVA with Tukey’s multiple comparisons test.
Clinical utility of the Brief Illness Perception Questionnaire
To understand the clinical relevance of the BIPQ, Spearman’s correlation between patient-reported outcome measures (BIPQ, MFI, SF-36 MCS and PCS, PtGA) and PhGA was calculated. Multivariable linear regression was used to study the relationships of specific illness perception domains of the BIPQ to patient and physician-reported measures of fatigue, mental health, physical health and disease activity.
Longitudinal analyses
To facilitate the interpretation of BIPQ scores in future longitudinal studies, the minimum clinically defined important difference was determined. To determine the smallest change in BIPQ composite score that was important to patients, the PtGA was used as the anchor measure (24). Change in the composite BIPQ score was compared to change in the PtGA scores within-patients over successive study visit. Different threshold scores were tested iteratively to determine the optimal BIPQ threshold score most strongly associated with change in corresponding PtGA scores. The average change in the composite BIPQ score was calculated between interval visits and used as a starting point to inform a threshold score. Patients with an absolute change in the BIPQ composite score less than the threshold were categorized as unchanged. Patients whose composite score was reduced by greater than the threshold score were categorized as improved and whose score increased by greater than threshold were categorized as worse. Mean differences in PtGA were compared between the BIPQ composite score-defined categories.
Fatigue is a common complaint among patients with vasculitis that is often poorly understood and does not necessarily align with physician assessment of disease activity (4). Illness perceptions have been associated with fatigue in cross sectional analyses (4). To determine if changes in illness perceptions over time are associated with patient reported degree of fatigue, correlation between change in MFI and BIPQ scores over successive interval visits was assessed.
Results
Study population
A summary of patient characteristics is listed in Table 1. 196 patients with four forms of vasculitis were recruited into the study [giant cell arteritis (GCA) n=47; Takayasu’s arteritis (TAK) n=47; relapsing polychondritis (RP) n=56; and ANCA-associated vasculitis (AAV) n=46]. Patients with AAV consisted of a combination of eosinophilic granulomatosis with polyangiitis (EGPA) n=5, granulomatosis with polyangiitis (GPA) n=34 and microscopic polyangiitis (MPA) n=7. Patients were evaluated over a total of 454 visits. Most patients were Caucasian (75.5%), female (74%), and the average age was 48 years old. The demographic characteristics by diagnosis were consistent with known characteristic distributions for these types of vasculitis. For example, the ratios between female and male participants in this study were characteristic of each disease(25–27).
Table 1.
Patient Characteristics
| All | |||||
|---|---|---|---|---|---|
| Patients | GCA | TAK | AAV | RP | |
| n = 196 | n = 47 | n = 47 | n = 46 | n = 56 | |
| Total number of visits | 454 | 113 | 90 | 172 | 79 |
| Age, mean years (SD) | 48 (20) | 68 (11) | 34 (14) | 53 (18) | 42 (17) |
| Sex, n (% female) | 145 (74) | 35 (74.5) | 40 (85.1) | 26 (56.5) | 44 (78.6) |
| Race, n (% Caucasian) | 148 (75.5) | 37 (78.7) | 32 (68.1) | 37 (80.4) | 42 (75.0) |
| Brief Illness Perception Questionnaire (median, range) | |||||
| Consequences | 7 (3–8) | 6 (3–8) | 6 (3–8) | 6 (2–9) | 8 (7–10) |
| Timeline | 9 (5–10) | 10 (2–10) | 9 (6–10) | 9 (5–10) | 10 (7–10) |
| Personal Control | 3 (2–5) | 5 (2–7) | 3 (0–5) | 5 (3–7) | 3 (1–4) |
| Treatment Control | 8 (5–10) | 8 (6–10) | 7 (5–10) | 9 (7–10) | 7 (5–8) |
| Identify | 5 (2–8) | 5 (2–7) | 4 (1–6) | 4 (1–8) | 8 (6–9) |
| Illness Concern | 8 (6–10) | 8 (7–10) | 7 (5–10) | 8 (5–10) | 10(8–10) |
| Coherence | 7 (5–9) | 8 (5–10) | 7 (5–9) | 7 (5–8) | 7 (5–8) |
| Emotional Representation | 5 (2–8) | 3 (2–6) | 6 (3–8) | 4 (2–7) | 7 (4–9) |
Abbreviations:GCA = giant cell arteritis; TAK = Takayasu’s arteritis; AAV = ANCA associated vasculitis; RP = relapsing polychondritis; n = number; SD = standard deviation
Validity of the Brief Illness Perception Questionnaire
Accuracy and precision of the BIPQ compared to the IPQ-R
Scores on each illness perception domain were compared between the BIPQ and the IPQ-R. There were no significant differences between the cohort of patients with vasculitis who completed the IPQ-R compared to the current cohort in terms of age, sex, and disease duration. Mean scores for each domain did not significantly differ between the IPQ-R and BIPQ (3.47 vs 3.28, p=0.22) (Figure 1A). Further, there were no differences in domain scores between the BIPQ and IPQ-R stratified by disease (data not shown). Although there was comparable accuracy between the BIPQ and IPQ-R, the BIPQ was less precise to measure responses across each domain with significantly lower mean standard deviation of responses compared to the IPQ-R (0.84 vs 1.21, p<0.0001) (Figure 1B).
Figure 1. Comparison of the BIPQ and IPQ-R domains mean and standard deviation to determine comparability of the two measures.
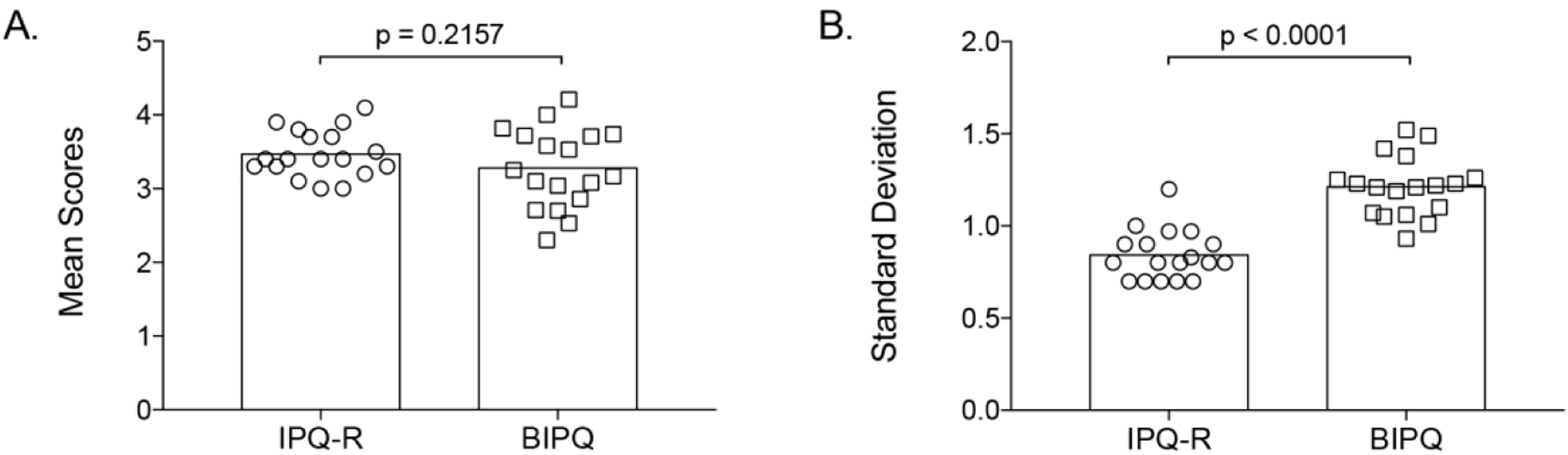
(A) Mean illness perception domains scores did not significantly differ between the BIPQ and the IPQ-R, indicating comparable accuracy between the two assessment tools. (B) Mean standard deviations for illness perception domain scores were significantly lower for the IPQ-R compared to the BIPQ, indicating that illness perceptions are measured with greater precision by the IPQ-R.
Validity of the BIPQ composite score
There was weak to moderate correlation between the different illness perception domains, and the only pairwise correlation >0.70 was between identity and consequences (r=0.80). Factor analysis using a 2–4 factor solution did not suggest data reduction was appropriate because only identity and consequences loaded onto the same factor with a loading >0.60. Therefore, use of a BIPQ composite score, derived by summation of all eight illness perception domains, was considered appropriate in this dataset. Distribution of BIPQ composite scores by type of vasculitis is shown in Figure 2. Significant differences in illness perceptions across the four types of vasculitis were observed (AAV: 31.13 (SD=12.16), GCA: 35.16 (SD=13.93); TAK:38.4 (SD=14.47); RP: 52.11 (SD=10.36); p<0.0001) with the highest composite score observed in patients with RP. Scores in the individual domains are listed by disease in Table 1. On average, patients with RP had the highest perceived burden of disease burden for consequences, identity, illness concern, and emotional representation.
Figure 2. Distribution of BIPQ composite scores by type of vasculitis.
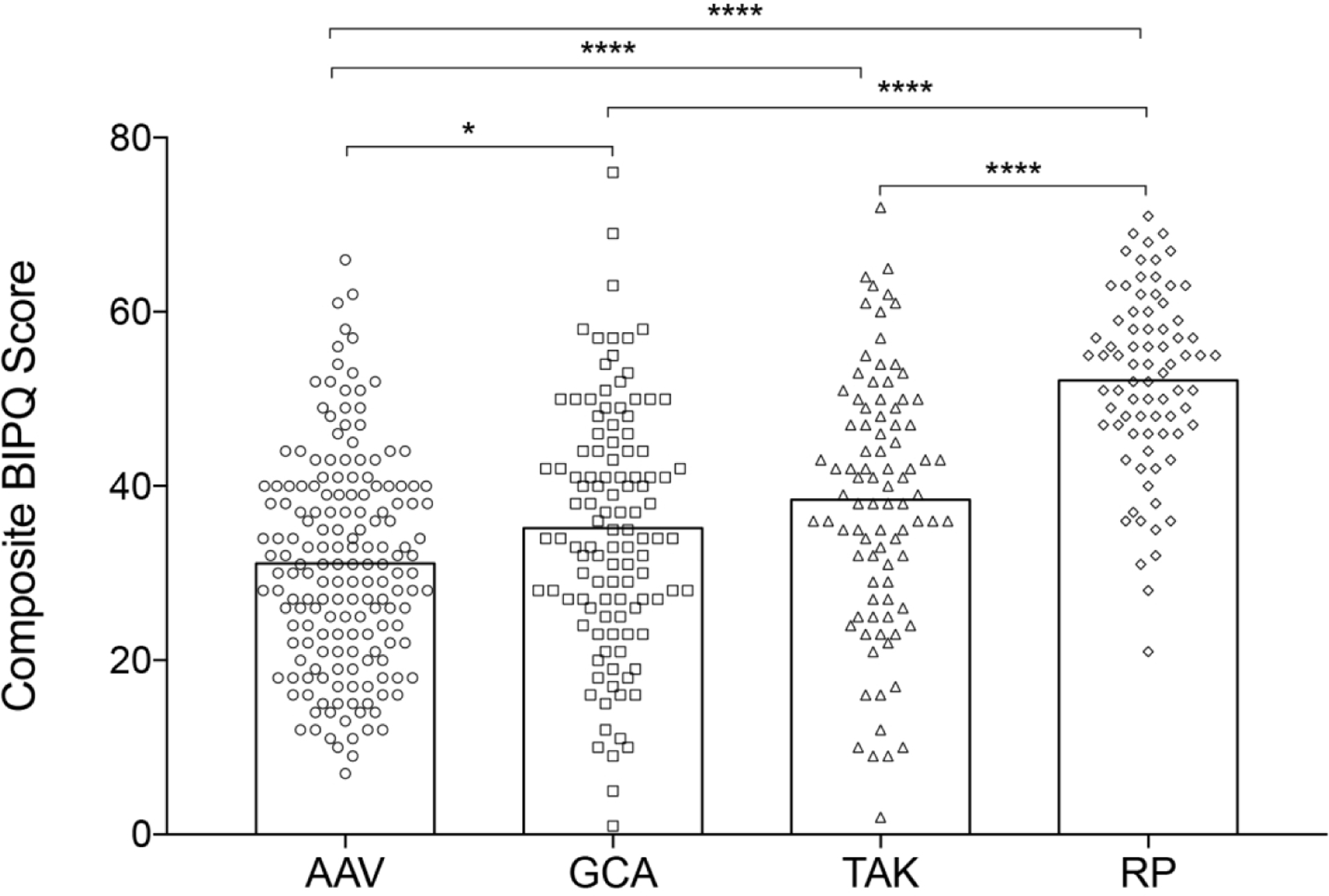
Perceived psychological burden of illness as assessed by the composite BIPQ score differed significantly across the four forms of vasculitis. Patients with relapsing polychondritis (RP) perceived the greatest psychological burden of illness. Analysis of variance test with post-hoc Tukey comparisons. *p<0.05 ****p<0.0001. GCA = giant cell arteritis; TAK = Takayasu’s arteritis; AAV = ANCA-associated vasculitis.
Clinical utility of the Brief Illness Perception Questionnaire
Comparison of BIPQ to patient- and physician-reported assessments of disease
Correlations between illness perceptions (BIPQ) and patient-reported measures of fatigue, disease activity, physical health and mental health (MFI, PtGA, SF-36 PCS and SF-36 MCS respectively) demonstrated strong associations between the various patient-reported outcomes (Figure 3A). BIPQ composite scores significantly correlated with PtGA (ρ=0.70, p<0.0001); fatigue (MFI) (ρ=0.63, p<0.0001); mental health (SF-36 MCS) (ρ= −0.50, p<0.0001); and physical health (SF-36 PCS) (ρ = −0.60, p<0.0001). In contrast, patient perception of physical health (SF-36 PCS) was the only patient-reported measure significantly associated with physician assessment of disease activity (PhGA) (ρ= −0.24, p=0.01) (Figure 3B), and BIPQ composite scores were not significantly associated with PhGA (Figure 3C).
Figure 3. BIPQ associations with patient- and physician-reported measures.
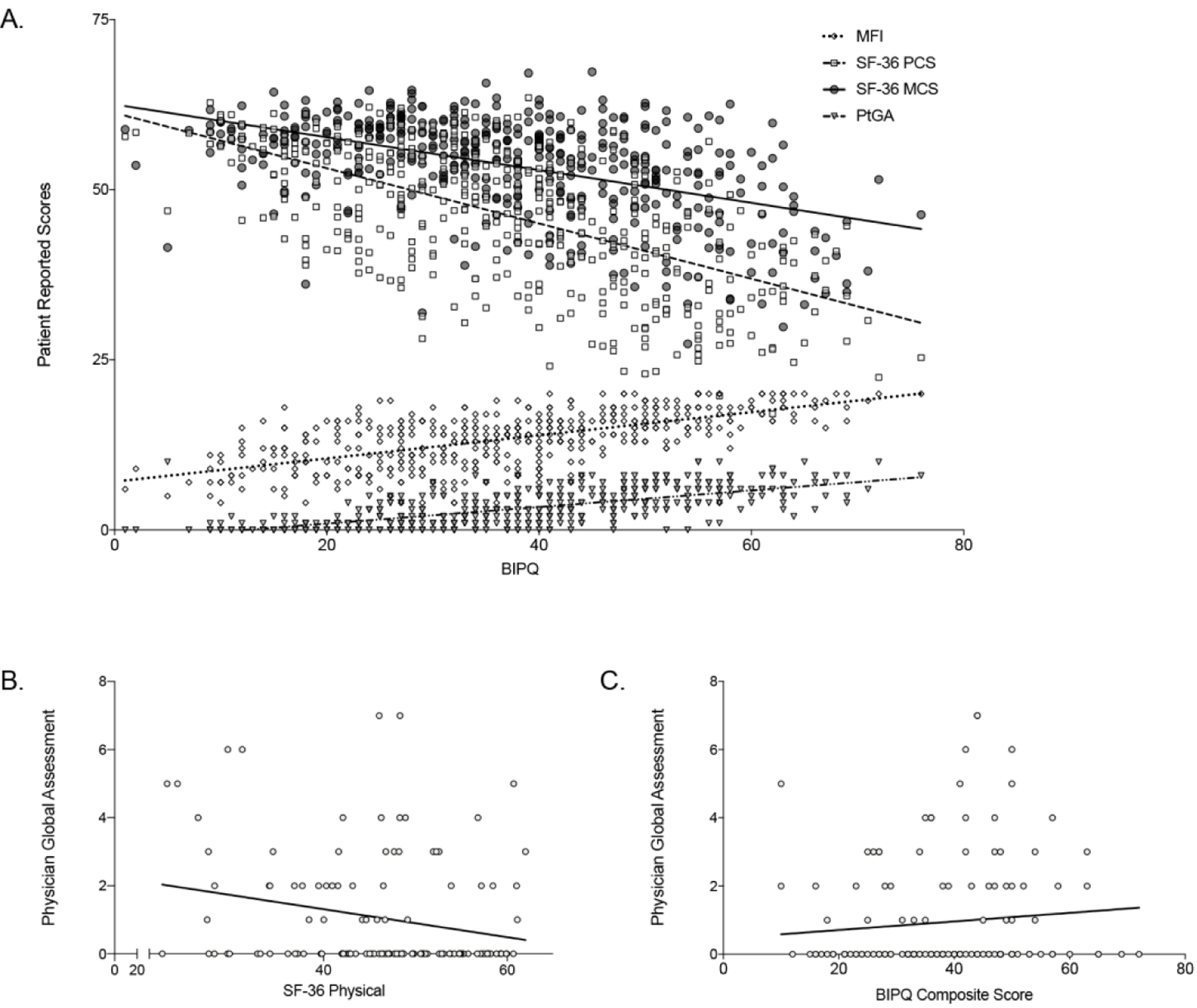
(A) Illness perceptions as measured by the composite Brief Illness Perception Questionnaire (BIPQ) were significantly correlated to other patient-reported outcome measures, including patient global assessment (PtGA: r = 0.70, p < 0.01), fatigue (MFI: r = 0.63, p < 0.01), metal health (SF-36 MCS: r = −0.50, p < 0.01), and physical health (SF-36 PCS: r = −0.60, p < 0.01). (B) SF-36 PCS was the only patient-reported outcome significantly associated with physcian assesment of disease activity (PhGA) (r = −0.24, p = 0.01). (C) Illness perceptions as measured by the BIPQ were not significantly correlated with PhGA (r = 0.13, p = 0.13).
Associations of specific domains of the BIPQ with patient- and physician-reported assessments of disease
The associations between specific illness perception domains and both patient- and physician-reported outcome measures are listed in Table 2. Consequences (extent to which life is negatively affected by disease) and Illness Concern (degree of concern about illness) were most significantly associated with fatigue. Identity (number of different symptoms attributed to illness) and Illness Concern were most significantly associated with PtGA. Timeline (how chronic the illness is perceived to be) and Identity were most significantly associated with PhGA. Consequences, Identity, and Coherence (how well illness is understood by the patient) were most significantly associated with the SF-36 PCS. Illness Concern, Coherence and Emotional Representation (extent of emotional effect from illness) were most significantly associated with the SF-36 MCS.
Table 2.
Multivariable linear regression models to assess the relationship between each BIPQ domain (predictor variables) and various patient and physician reported outcome measures
| SF-36 MCS | |||||
|---|---|---|---|---|---|
| Consequences (negative impact) | 0.69 (0.08) *** | 0.10(0.05)* | 0.08 (0.08) | −1.63(0.12)*** | −0.094(0.16) |
| Timeline (more chronic) | 0.11 (0.05)* | −0.01 (0.03) | −0.17(0.04)*** | −0.13 (0.10) | −0.04 (0.09) |
| Personal Control (more control)† | −0.11(0.06) | −0.06 (0.03) | 0.12(0.04)** | 0.20(0.13) | 0.20(0.10) |
| Treatment Control (more control)† | −0.03 (0.06) | −0.07 (0.04) | −0.09 (0.06) | −0.04(0.15) | 0.16(0.13) |
| Identity (more symptoms) | 0.12 (0.07) | 0.48 (0.04) *** | 0.20 (0.07) ** | −1.22(0.18)*** | 0.14(0.14) |
| Illness Concern (more concerned) | −0.18 (0.06) ** | 0.11 (0.04)** | −0.05 (0.06) | 0.30(0.14)* | 0.39(0.11)** |
| Coherence (more understanding)† | 0.03 (0.07) | 0.08 (0.04) * | −0.01 (0.06) | −0.41 (0.15)** | 0.32 (0.12) ** |
| Emotional Representation (negative impact) | 0.17 (0.07) * | −0.01 (0.04) | −0.03 (0.05) | 0.33 (0.15) * | −1.62 (0.12) *** |
| 0.44 |
Results are presented as beta coefficients (standard error). Abbreviations: BIPQ = brief illness perception questionnaire; MFI = multidimensional fatigue inventory; PtGA = patient global assessment; PhGA = physician global assessment; SFS-36 PCS = short form health survey physical composite score; SFS-36 MCS = short form health survey metal composite score;
p<0.05
p<0.01
p<0.0001
BIPQ domains that are scored (0-to-10, negative to positive)
Assessing the utility of the BIPQ for monitoring change in illness perceptions over time and relationship to changes in patient- and physician-reported assessments of disease
The average change in BIPQ composite score between visit intervals was 7.4 (SD=6.7). Using a threshold BIPQ composite score of 7 to define meaningful change, there were corresponding significant differences in change in PtGA over study visits (Figure 4A). When BIPQ scores increased by ≥7, corresponding PtGA scores were significantly higher than when BIPQ scores were unchanged or decreased by ≥7 (change in PtGA scores: worse 0.97 (SD=0.46), unchanged: −0.023 (SD=0.13), improved: −1.31 (SD=0.26); p=0.02). After iterative testing of different threshold scores, a change in the BIPQ composite score ≥7 remained most strongly associated with change in corresponding PtGA scores. In contrast to patient assessment, change in the BIPQ composite score by ≥7 was not significantly associated with corresponding change in PhGA (Figure 4B). Additionally, change in fatigue (MFI) significantly correlated with change in BIPQ composite scores over successive visit intervals (ρ = 0.38, p = 0.0008) (Figure 4C).
Figure 4. Change in illness perceptions over time and relationship to other patient- and physician- reported disease assessments.

(A) Composite BIPQ scores were categorized as worse (increased by 7 points or greater), improved (decreased by 7 point or greater) or unchanged. Using this threshold, change in BIPQ was significantly associated with concomitant change in patient global assessment scores over time. (B) In contrast, change in composite BIPQ scores by 7 or greater was not associated with concomitant change in physician global assessment scores over time. (C) Change in measures of fatigue (MFI) and illness perception (BIPQ) were significantly correlated over time.
Discussion
This study validates the use of the BIPQ in patients with various forms of systemic vasculitis. The BIPQ is considerably shorter and easier to administer than the full-length IPQ-R, making it an attractive option to measure illness perceptions. In patients with vasculitis, the BIPQ provides comparable information to the IPQ-R. Although test precision was shown to be greater in the IPQ-R, the accuracy of the BIPQ to measure the various illness perception domains was similar to the IPQ-R. Internal consistency metrics were calculated and showed that each domain of the BIPQ captures unique information on illness perception, supporting the use of a BIPQ composite score in vasculitis. The BIPQ composite score was used to track change in illness perceptions over time, and a minimum threshold change of ≥7 points was associated with corresponding significant change in patient assessment of disease activity. These analyses enable the use and interpretation of the BIPQ as an outcome measure in future studies in vasculitis.
The BIPQ composite score revealed disease-specific differences in illness perception among patients with different forms of vasculitis. Patients with RP expressed the highest level of psychological burden of illness, while patients with AAV endorsed the least perceived burden of disease. The differences between the degree of negative illness perceptions likely reflect differences in standards of care for each condition. Over the last few decades, well-conducted clinical trials have supported development of evidence-based guidelines to manage ANCA-associated vasculitis and have improved long term clinical outcomes for these patients(28). Conversely, RP remains an under-studied condition for which there has never been a randomized clinical trial to enable development of treatment guidelines(25, 29). Comparison of illness perceptions by type of vasculitis therefore can help identify unmet needs and research priorities from the patient perspective.
Illness perceptions strongly correlated with other patient-reported measures of disease activity but only weakly correlated with physician assessment. This finding aligns with prior work demonstrating a divide exists between patient- and physician-based assessments of disease activity in vasculitis(6). Associations between specific domains of the BIPQ and various outcome measures provided additional insight into how patients with vasculitis perceive their illness. Patients with vasculitis experience both physical and psychological connection to their illness, while physician-based assessment of disease activity is influenced more heavily by the physical rather than mental components of disease(6). Both physician (PhGA) and patient assessments of physical health (SF-36 PCS) were strongly associated with the reported burden of symptoms (identify domain) on the BIPQ. Several additional domains on the BIPQ, including emotional impact of disease (emotional representations domain), were not associated with physician-based assessment but were strongly linked to patient perceptions of mental health (SF-36 MCS) and fatigue (MFI).
This study has a number of strengths. Although the BIPQ has been used previously in vasculitis research (30), its value, validity, and interpretation have not been previously assessed systematically. Unlike prior studies that assessed illness perceptions in patients with vasculitis(4), this study includes both patient-reported and physician based assessments of disease and utilizes simultaneous, blinded patient and physician evaluations. Further, this study uniquely included data from patients with RP, and demonstrated a high level of patient-perceived burden of illness in these patients (2). Finally, multiple validated questionnaires were administered concurrently within a standardized protocol to comprehensively assess the relationship between illness perceptions and other measures of disease activity in vasculitis. A few study limitations should also be highlighted. This was a single center study that should be replicated in other cohorts. The same patients did not take both the IPQ-R and the BIPQ surveys; however, patient-level data was available to facilitate disease-specific comparisons.
In a chronic illness such as vasculitis, it is important for care providers to recognize that patients think about disease differently than their physician counterparts. In that context, the BIPQ is a useful assessment tool to identify and monitor patient-held beliefs about illness. Patients have emotional and psychological connections to their illness and conceptualize disease activity differently than physicians. Being mindful of illness perception is therefore important to understand the nuances of how patients think about vasculitis. Developing therapeutic strategies that address perceived psychological burdens of illness may improve overall patient care.
Acknowledgments
Funding and Conflict of Interest Disclosure: This research was supported by the Division of Intramural Research of the National Institute of Arthritis and Musculoskeletal and Skin Diseases.
Footnotes
The authors declare no conflicts of interest.
References
- 1.Jennette JC, Falk RJ, Bacon PA, Basu N, Cid MC, Ferrario F, et al. 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum 2013;65:1–11. [DOI] [PubMed] [Google Scholar]
- 2.Ferrada MA, Grayson PC, Banerjee S, K AS, R AC, Sinaii N, et al. Patient Perception of Disease-Related Symptoms and Complications in Relapsing Polychondritis. Arthritis Care Res (Hoboken) 2018;70:1124–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.File I, Trinn C, Matyus Z, Ujhelyi L, Balla J, Matyus J. Relapsing polychondritis with p-ANCA associated vasculitis: Which triggers the other? World J Clin Cases 2014;2:912–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Grayson PC, Amudala NA, McAlear CA, Leduc RL, Shereff D, Richesson R, et al. Illness perceptions and fatigue in systemic vasculitis. Arthritis Care Res (Hoboken) 2013;65:1835–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Leventhal H Illness representations: theoretical foundations In: Petrie KJ, Weinman JA, Perceptions of health and illness: Current research and applications. Amsterdam, Netherlands: Harwood Academic Publishers; 1997. p. 19–45. [Google Scholar]
- 6.Herlyn K, Hellmich B, Seo P, Merkel PA. Patient-reported outcome assessment in vasculitis may provide important data and a unique perspective. Arthritis Care Res (Hoboken) 2010;62:1639–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Figueiras MJ, Alves NC. Lay perceptions of serious illnesses: An adapted version of the Revised Illness Perception Questionnaire (IPQ-R) for healthy people. Psychology & Health 2007;22:143–58. [Google Scholar]
- 8.Moss-Morris R, Weinman J, Petrie K, Horne R, Cameron L, Buick D. The Revised Illness Perception Questionnaire (IPQ-R). Psychology & Health 2002;17:1–16. [Google Scholar]
- 9.Broadbent E, Petrie KJ, Main J, Weinman J. The brief illness perception questionnaire. J Psychosom Res 2006;60:631–7. [DOI] [PubMed] [Google Scholar]
- 10.Broadbent E, Wilkes C, Koschwanez H, Weinman J, Norton S, Petrie KJ. A systematic review and meta-analysis of the Brief Illness Perception Questionnaire. Psychol Health 2015;30:1361–85. [DOI] [PubMed] [Google Scholar]
- 11.Hunder GG, Bloch DA, Michel BA, Stevens MB, Arend WP, Calabrese LH, et al. The American College of Rheumatology 1990 criteria for the classification of giant cell arteritis. Arthritis Rheum 1990;33:1122–8. [DOI] [PubMed] [Google Scholar]
- 12.Arend WP, Michel BA, Bloch DA, Hunder GG, Calabrese LH, Edworthy SM, et al. The American College of Rheumatology 1990 criteria for the classification of Takayasu arteritis. Arthritis Rheum 1990;33:1129–34. [DOI] [PubMed] [Google Scholar]
- 13.Leavitt RY, Fauci AS, Bloch DA, Michel BA, Hunder GG, Arend WP, et al. The American College of Rheumatology 1990 criteria for the classification of Wegener’s granulomatosis. Arthritis Rheum 1990;33:1101–7. [DOI] [PubMed] [Google Scholar]
- 14.McAdam LP, O’Hanlan MA, Bluestone R, Pearson CM. Relapsing polychondritis: prospective study of 23 patients and a review of the literature. Medicine (Baltimore) 1976;55:193–215. [PubMed] [Google Scholar]
- 15.Damiani JM, Levine HL. Relapsing polychondritis--report of ten cases. Laryngoscope. 1979;89:929–46. [PubMed] [Google Scholar]
- 16.Smets EM, Garssen B, Bonke B, De Haes JC. The Multidimensional Fatigue Inventory (MFI) psychometric qualities of an instrument to assess fatigue J Psychosom Res. 1995;39:315–25. [DOI] [PubMed] [Google Scholar]
- 17.Tomasson G, Boers M, Walsh M, LaValley M, Cuthbertson D, Carette S, et al. Assessment of health-related quality of life as an outcome measure in granulomatosis with polyangiitis (Wegener’s). Arthritis Care Res (Hoboken) 2012;64:273–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Walsh M, Mukhtyar C, Mahr A, Herlyn K, Luqmani R, Merkel PA, et al. Health-related quality of life in patients with newly diagnosed antineutrophil cytoplasmic antibody-associated vasculitis. Arthritis Care Res (Hoboken) 2011;63:1055–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Tomasson G, Davis JC, Hoffman GS, McCune WJ, Specks U, Spiera R, et al. Brief report: The value of a patient global assessment of disease activity in granulomatosis with polyangiitis (Wegener’s). Arthritis Rheumatol 2014;66:428–32. [DOI] [PubMed] [Google Scholar]
- 20.Nikiphorou E, Radner H, Chatzidionysiou K, Desthieux C, Zabalan C, van Eijk-Hustings Y, et al. Patient global assessment in measuring disease activity in rheumatoid arthritis: a review of the literature. Arthritis Res Ther 2016;18:251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Turk M, Pope JE. Physician global assessments for disease activity in rheumatoid arthritis are all over the map! RMD Open 2018;4:e000578. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Broadbent E, Wilkes C, Koschwanez H, Weinman J, Norton S, Petrie KJ. A systematic review and meta-analysis of the Brief Illness Perception Questionnaire. Psychol Health. 2015;30:1361–85. [DOI] [PubMed] [Google Scholar]
- 23.MacCallum RC, Widaman KF, Preacher KJ, Hong S. Sample size in factor analysis: the role of model error. Multivariate Behav Res 2001;36:611–37. [DOI] [PubMed] [Google Scholar]
- 24.Copay AG, Subach BR, Glassman SD, Polly DW, Schuler TC. Understanding the minimum clinically important difference: a review of concepts and methods. Spine J 2007;7:541–6. [DOI] [PubMed] [Google Scholar]
- 25.Rednic S, Damian L, Talarico R, Scire CA, Tobias A, Costedoat-Chalumeau N, et al. Relapsing polychondritis: state of the art on clinical practice guidelines. RMD Open 2018;4:e000788. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Sait MR, Lepore M, Kwasnicki R, Allington J, Balasubramanian R, Somasundaram SK, et al. The 2016 revised ACR criteria for diagnosis of giant cell arteritis - Our case series: Can this avoid unnecessary temporal artery biopsy? International Journal of Surgery Open 2017;9:19–23. [Google Scholar]
- 27.Robson JC, Dawson J, Cronholm PF, Milman N, Kellom KS, Ashdown S, et al. Health-related quality of life in ANCA-associated vasculitis and item generation for a disease-specific patient-reported outcome measure. Patient Relat Outcome Meas 2018;9:17–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Yates M, Watts RA, Bajema IM, Cid MC, Crestani B, Hauser T, et al. EULAR/ERA-EDTA recommendations for the management of ANCA-associated vasculitis. Ann Rheum Dis 2016;75:1583–94. [DOI] [PubMed] [Google Scholar]
- 29.Misra DP, Naidu G, Agarwal V, Sharma A. Vasculitis research: Current trends and future perspectives. Int J Rheum Dis 2019;22 Suppl 1:10–20. [DOI] [PubMed] [Google Scholar]
- 30.Brezinova P, Englbrecht M, Lovric S, Samann A, Strauss B, Wolf G, et al. Coping strategies and depressiveness in primary systemic vasculitis--what is their impact on health-related quality of life? Rheumatology (Oxford) 2013;52:1856–64. [DOI] [PubMed] [Google Scholar]