

Abstract
Purpose
This study evaluated the medial joint stability after high tibial osteotomy (HTO) releasing the superficial medial collateral ligament (sMCL) without cutting and repairing.
Methods
Twenty-one patients who performed HTO were enrolled. After an L-shaped incision was made in the pes anserinus, the sMCL was released from the distal portion during surgery. After plate fixation, the sMCL was reattached and the pes anserinus was repaired underneath the plate. Plate removal was performed after 31.1 ± 14.2 months. Before HTO, a valgus force of 40 N was exerted at extension for reference values. Before and after plate removal, a valgus force of 40 N was exerted at extension and at a flexion position of 20°. Medial stability was evaluated by measuring the joint line convergence angle (JLCA).
Results
The JLCAs in the extension state before HTO and plate removal were 1.64° ± 1.15° and 1.83° ± 1.36°, respectively; there was no significant difference (p = 0.198). There was also no significant difference in JLCA before HTO and after plate removal (p = 0.835). There was also no significant difference in JLCA before and after plate removal both at a knee extension and flexion position of 20° (p = 0.348 and p = 0.456, respectively).
Conclusions
Releasing the sMCL without cutting and repairing the pes anserinus underneath the plate during medial open wedge HTO could facilitate the maintenance of medial joint stability.
Keywords: Pes anserinus, Medial laxity, High tibial osteotomy
Introduction
High tibial osteotomy (HTO) is a useful surgical option for medial osteoarthritis combined with varus deformity in young active patients [1, 2]. Several surgical options for HTO exist, including the lateral closed wedge and medial open wedge osteotomy [3, 4]. Recently, medial open wedge HTO with locking plates has become favored to avoid co-morbidity associated with fibular osteotomy, which is required for closed wedge osteotomy [5].
During medial open wedge HTO, the medial soft structures should be exposed for the osteotomy site and released for gap opening. Among these structures, the superficial medial collateral ligament (sMCL) is the primary restraint of valgus stress and the pes anserinus also stabilizes the medial side of the knee joint [6, 7]. During HTO, some surgeons prefer subperiosteal elevation and pull-aside without transection. This technique, however, has disadvantages, including narrower view and incomplete correction over 10 mm of osteotomy gap [8]. Other surgeons prefer complete cutting or transection of the sMCL because this provides a good view for surgery and prevents neurovascular damage [8–10]. Additionally, the pes anserinus could be repaired over the plate. After plate removal, severe medial laxity could occur during the conversion of HTO to total knee arthroplasty (TKA), owing to insufficient healing of the sMCL or recutting the pes anserinus over the plate [11].
It is assumed that medial stability could be maintained when the sMCL is released and reattached at the tibial attachment without cutting and the pes anserinus repaired underneath the plate. The aim of the present study was to evaluate medial joint stability before and after plate removal among patients who have undergone HTO with sMCL reattachment and pes anserinus repair under the plate.
Material and methods
Patients
This study was approved by the institutional review board (IRB) of the authors’ affiliated institution. This study retrospectively evaluated 21 patients (4 men and 17 women) who underwent medial open wedge HTO for varus deformity and medial osteoarthritis from July 2012 to March 2018. The mean patient age was 56.5 years (age range, 47–61 years). All patients underwent open wedge HTO with locking plates. Tomofix locking plates (Synthes GmbH, Solothurn, Switzerland) were used for five patients and OhtoFix locking plates (Ohtomedical Co. Ltd., Goyang, South Korea) were used for 16 patients.
Surgical procedure
All operations were performed by a single surgeon. During HTO, after an L-shaped incision of the pes anserinus was made, the sMCL was released from the distal portion using a periosteal elevator without cutting. Biplane osteotomy was performed and locking plates were used for fixation in addition to one screw for the fourth hole for pes anserinus passage under the plate. The gap was filled with allograft bone chips mixed with autologous bone marrow obtained from the anterior superior iliac spine. Then, the sMCL was reattached, the pes anserinus was repaired underneath the plate, and the final locking screw was fixated (Fig. 1).
Fig. 1.

a An L-shaped incision of the pes anserinus (arrow) was performed to approach the superficial medial collateral ligament and osteotomy site. b After the locking plate was fixed, the pes anserinus was passed under the plate using suture thread attached to the pes anserinus. c The thread of pes anserinus was sutured to the patellar tendon. Then repair under the plate was performed
Evaluation methods
Preoperatively, a valgus force of 40 N was exerted at extension. Medial stability was evaluated by measuring the joint line convergence angle (JLCA). After a mean period of 31.1 months, plate removal was performed and medial stability was also evaluated. Before and after plate removal, a valgus force of 40 N was exerted at extension and at a flexion position of 20°. Medial stability was evaluated and compared by measuring the JLCA (Fig. 2). The change of this angle at each position was compared for evaluating the medial stability. The preoperative JLCA at extension was also compared with the angle before and after plate removal. Clinical scores, including the Hospital for Special Surgery (HSS) score, Knee Society Knee Score (KS), function score (FS), and patellar score was also evaluated before HTO and before plate removal.
Fig. 2.
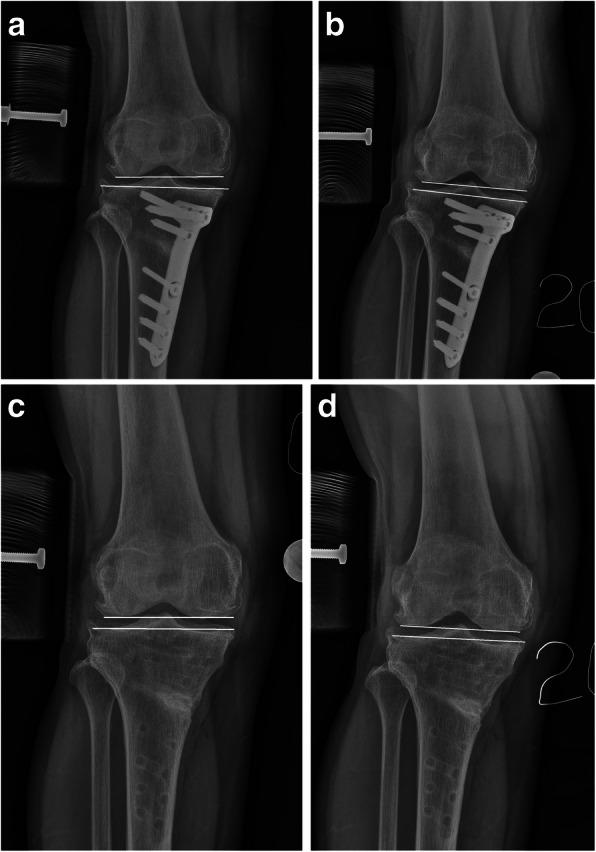
The joint line convergence angle was measured using radiographs. The angle between two lines is joint line convergence angle. a A valgus force of 40 N was exerted at extension before plate removal. b A valgus force of 40 N was exerted at a flexion position of 20° before plate removal. c A valgus force of 40 N was exerted at extension after plate removal. d A valgus force of 40 N was exerted at a flexion position of 20° after plate removal
Statistical analyses
The JLCAs at each period were compared using Wilcoxon’s signed-rank test. The clinical results before HTO and before plate removal were also compared using the same method. All statistical analyses were performed using SPSS Statistics version 21.0 (IBM Corp., Armonk, NY, USA). Statistical significance was assumed at a p value < 0.05.
Results
The mean mechanical femorotibial angle was changed from preoperative varus at 7.3° ± 1.7° to postoperative valgus at 3.4° ± 1.5°. The mean HSS score improved from 72.21 to 89.77 (p < 0.001). The mean KS and FS also improved from 62.71 to 91.38 (p < 0.001) and 61.05 to 89.52 (p < 0.001), respectively. The mean patellar score did not change significantly, from 24.62 to 25.00 (p = 1.000).
The JLCAs in the extension state before HTO and plate removal were 1.64° ± 1.15° and 1.83° ± 1.36°, respectively; there was no significant difference (p = 0.198). There was also no significant difference in JLCA before HTO and after plate removal (p = 0.835) (Table 1). There was also no significant difference in JLCA before and after plate removal both at a knee extension and flexion position of 20° (p = 0.348 and p = 0.456, respectively).
Table 1.
Joint line convergence angle measurements
| Before HTO operation (°) | Before plate removal (°) | After plate removal (°) | p value | |
|---|---|---|---|---|
| At extension | 1.64 ± 1.15 | 1.83 ± 1.35 | 0.198 | |
| 1.64 ± 1.15 | 1.80 ± 1.25 | 0.835 |
HTO high tibial osteotomy
Discussion
This study demonstrated that releasing the sMCL distally without cutting and repairing pes anserinus underneath the plate during medial open wedge HTO could maintain medial joint stability after HTO. It is thought that the released sMCL at the tibial site without transection heals after HTO. Medial stability was also maintained even after plate removal.
Between the two methods of HTO, medial open wedge HTO has the advantage of higher accuracy of correction [3]. Moreover, lateral closed wedge HTO is associated with complications, including peroneal nerve palsy, that can be prevented by performing medial open wedge HTO [12–14]. During medial open wedge HTO, the medial soft structures should be exposed for the osteotomy site and released for gap opening. Among these structures, the sMCL is the primary restraint of valgus stress and the pes anserinus also stabilizes the medial side of the knee joint [6, 7]. However, these structures can be injured during open wedge HTO and this may cause medial instability. For these reasons, several authors have reported that the release of the sMCL for open-wedge HTO should be kept to a minimum to decrease the potential of later valgus instability, because the partial release of sMCL had a similar effect with complete release [15].
A study by Kim et al. [11] demonstrated that medial instability can occur after plate removal during TKA conversion, even if the joint was stable before plate removal. The alignment after HTO was well corrected; however, the medial proximal tibial angle was overcorrected. This could be the result of medial soft-tissue injury during the process of plate removal. When the pes anserinus was repaired over the plate during HTO, pes anserinus dissection over the plate could cause medial instability after plate removal. After this experience, the importance of preserving the medial soft tissue—including by releasing the sMCL distally without cutting and repairing pes anserinus under the plate—became clear.
Cutting the sMCL completely without repair is a good method for approaching the osteotomy site and preventing neurovascular damage [8]; however, this technique could cause medial instability. Pes anserinus repair over the plate is also easier to accomplish than if attempted under the plate. However, soft-tissue irritation might occur and recutting the pes anserinus during plate removal could cause medial instability. Therefore, the present study, wherein the elevated distal portion of the MCL was placed in tissue on grafted bone and the pes anserinus was repaired during open wedge HTO, showed that this is a good method for preventing medial instability.
This study had several limitations, including the small sample size and retrospective study design. Additionally, we did not make comparisons with cases in which the sMCL was cut or in which the pes anserinus was not repaired. Future large, comparative, prospective studies should be performed.
Conclusions
Releasing the sMCL without cutting and repairing the pes anserinus underneath the plate during medial open wedge HTO could facilitate the maintenance of medial joint stability.
Acknowledgements
Not applicable.
Abbreviations
- HTO
High tibial osteotomy
- sMCL
Superficial medial collateral ligament
- TKA
Total knee arthroplasty
- JCLA
Joint line convergence angle
- KS
Knee Society knee score
- FS
Knee Society function score
- IRB
Institutional review board
Authors’ contributions
HJK and HSK designed the study and wrote the manuscript. JYS analyzed the data. HJL and CHJ wrote the manuscript. KHP wrote and revised the manuscript. The author(s) read and approved the final manuscript.
Funding
None.
Availability of data and materials
Not applicable.
Ethics approval and consent to participate
This study was approved by the IRB of Kyungpook National University Hospital (IRB no. KNUH 019–05–014-001).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Ryu SM, Park JW, Na HD, Shon OJ. High tibial osteotomy versus unicompartmental knee arthroplasty for medial compartment arthrosis with kissing lesions in relatively young patients. Knee Surg Relat Res. 2018;30(1):17–22. doi: 10.5792/ksrr.17.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Lee DC, Byun SJ. High tibial osteotomy. Knee Surg Relat Res. 2012;24(2):61. doi: 10.5792/ksrr.2012.24.2.61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sun H, Zhou L, Li F, Duan J. Comparison between closing-wedge and opening-wedge high tibial osteotomy in patients with medial knee osteoarthritis: a systematic review and meta-analysis. J Knee Surg. 2017;30(02):158–165. doi: 10.1055/s-0036-1584189. [DOI] [PubMed] [Google Scholar]
- 4.Brosset T, Pasquier G, Migaud H, Gougeon F. Opening wedge high tibial osteotomy performed without filling the defect but with locking plate fixation (TomoFix™) and early weight-bearing: prospective evaluation of bone union, precision and maintenance of correction in 51 cases. Orthop Traumatol Surg Res. 2011;97(7):705–711. doi: 10.1016/j.otsr.2011.06.011. [DOI] [PubMed] [Google Scholar]
- 5.Kyung HS, Lee BJ, Kim JW, Yoon SD. Biplanar open wedge high tibial osteotomy in the medial compartment osteoarthritis of the knee joint: comparison between the aescula and TomoFix plate. Clin Orthop Surg. 2015;7(2):185–190. doi: 10.4055/cios.2015.7.2.185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Mochizuki T, Akita K, Muneta T, Sato T. Pes anserinus: layered supportive structure on the medial side of the knee. Clin Anat. 2004;17(1):50–54. doi: 10.1002/ca.10142. [DOI] [PubMed] [Google Scholar]
- 7.Toor AS, Limpisvasti O, Ihn HE, McGarry MH, Banffy M, Lee TQ. The significant effect of the medial hamstrings on dynamic knee stability. Knee Surg Sports Traumatol Arthrosc. 2019;27(8):2608–2616. doi: 10.1007/s00167-018-5283-x. [DOI] [PubMed] [Google Scholar]
- 8.Nha KW. Current concepts in open-wedge high tibial osteotomy. Arthrosc Orthop Sports Med. 2015;2(1):12–22. doi: 10.14517/aosm14009. [DOI] [Google Scholar]
- 9.Agneskirchner JD, Hurschler C, Wrann CD, Lobenhoffer P. The effects of valgus medial opening wedge high tibial osteotomy on articular cartilage pressure of the knee: a biomechanical study. Arthroscopy. 2007;23(8):852–861. doi: 10.1016/j.arthro.2007.05.018. [DOI] [PubMed] [Google Scholar]
- 10.Nha KW, Oh SM, Ha YW, et al. A retrospective comparison of union rates after open wedge high tibial osteotomies with and without synthetic bone grafts (hydroxyapatite and β-tricalciumphosphate) at 2 years. Arthroscopy. 2018;34(9):2621–2630. doi: 10.1016/j.arthro.2018.03.008. [DOI] [PubMed] [Google Scholar]
- 11.Kim HJ, Kim YG, Min SG, Kyung HS. Total knee arthroplasty conversion after open-wedge high tibial osteotomy: a report of three cases. Knee. 2016;23(6):1164–1167. doi: 10.1016/j.knee.2016.06.010. [DOI] [PubMed] [Google Scholar]
- 12.Vena G, D’Adamio S, Amendola A. Complications of osteotomies about the knee. Sports Med Arthrosc. 2013;21(2):113–120. doi: 10.1097/JSA.0b013e3182900720. [DOI] [PubMed] [Google Scholar]
- 13.Wright JM, Crockett HC, Slawski DP, Madsen MW, Windsor RE. High tibial osteotomy. J Am Acad Orthop Surg. 2005;13(4):279–289. doi: 10.5435/00124635-200507000-00007. [DOI] [PubMed] [Google Scholar]
- 14.Tunggal JA, Higgins GA, Waddell JP. Complications of closing wedge high tibial osteotomy. Int Orthop. 2010;34(2):255–261. doi: 10.1007/s00264-009-0819-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Pape D, Duchow J, Rupp S, Seil R, Kohn D. Partial release of the superficial medial collateral ligament for open-wedge high tibial osteotomy. A human cadaver study evaluating medial joint opening by stress radiography. Knee Surg Sports Traumatol Arthrosc. 2006;14(2):141–148. doi: 10.1007/s00167-005-0649-2. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Not applicable.